Physical Assesment
1/59
Earn XP
Description and Tags
Physical Assessment
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
During a health history, a client reports drinking alcoholic beverages several mornings a week before going to work. In which part of the CAGE questionnaire should the nurse document this information?
Eye-openers
What are true statements regarding oral cancer?
Oral cancer occurs more frequently in males.,
Risk factors for oral cancer includes oral sex.,
Smoking is a risk factor for oral cancer.
What is an example of comprehensive assessment?
Health history and physical examination upon admission to a hospital
What describes an aspect of the nursing assessment process?
'The assessment process is ongoing and is not linear.'
A client on the orthopedic unit is being discharged home. The client is elderly and has a broken right humerus; the client is right handed. The client's closest family member lives 50 miles away. What should the nurse consider before discharging the client?
Who will be there to help the client with ADLs?
How will the client get home from the hospital?
How will the client cook and eat?
Purposeful hourly rounding by the nurse should include which assessments?
pain
personal needs
position'
fall prevention
The nurse prepares to analyze a list of a client's health problems. List the steps in the order the nurse completes critical thinking of these problems.
Identify abnormal data and strengths
Cluster the data
Draw inferences and identify problems
Propose possible nursing diagnoses
Check for defining characteristics of the diagnoses
Confirm or rule out nursing diagnoses
The usual order for performing assessment is:
Inspection, palpation, percussion, auscultation
Which assessment findings may result from inspection?
Respiratory rate 12 breaths per minute,
Gait unsteady,
Speech slurred
The correct depth for light palpation is:
1 cm
Which part of the hand is best for assessing temperature?
Dorsa/back of the hand
You are preparing to palpate a patient's abdomen during a comprehensive assessment. You will likely use which part of your hand?
Palm
For which assessment would the nurse plan to use deep palpation?
Size of liver
Deep palpation is used to assess the size, shape, and consistency of abdominal organs.
what is an example of palpation?
The nurse detects a small mass in the epigastric area.,
The nurse detects crepitus over the individual's thorax.,
The nurse detects increased warmth surrounding an abdominal incision.
For which of the following assessments would the nurse plan to use light palpation?
Skin temperature, Skin texture, Skin rash
Light palpation is used to assess surface characteristics, such as a papular rash. Deep palpation is used to assess the size, shape, and consistency of abdominal organs.
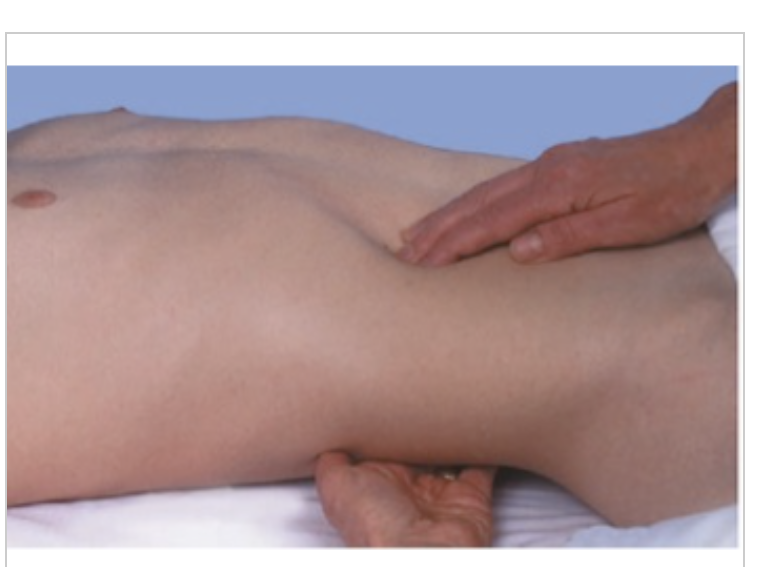
The nurse is assessing the client and performs the assessment shown. What is the nurse assessing?
Right kidney
A nurse, new to the hospital, is attending orientation with the nurse educator. The educator is discussing the use of deep palpation when assessing a patient. The nurse should be aware of what risk when using this assessment technique?
Risk for injury
When performing blunt percussion during an assessment, you should begin by:
Placing your palm flat against the patient's skin
You perform percussion during an assessment, and the procedure causes the patient pain. What is the most likely indication of this finding?
There is inflammation in an underlying structure.
The most commonly used type of percussion is:
Indirect percussion is used to assess the size and density of the organs in the chest and abdomen. It is used more commonly than direct percussion or blunt percussion. There is no such thing as deep percussion.
Diana wants to demonstrate normal findings so the new nurses have a foundation on which to build their knowledge. Asking the patient’s permission, which of the following patients would she choose to start with?
Enid Smith, a healthy 60 y/o admitted for a fractured femur due to a fall at a local skating rink.
A new nurse asks if areas of the body sound different when percussing. The instructor says yes and provides which example?
Normal percussion tones are quiet through areas such as the bones.
What are examples of percussion?
The nurse notes dullness over the patient's liver.,
The nurse notes resonance over the patient's thorax.,
The nurse notes tympany over the patient's lower abdomen.
What are examples of auscultation?
The nurse notes gurgling sounds over the individual's abdomen.,
The nurse notes crackling over the individual's thorax.,
The nurse notes a rhythmic lub-dub over the patient's anterior thorax.
The nurse wants to elicit a sound from a client's abdomen. Which technique should the nurse use?
Indirect percussion ensures that the client does not receive direct strikes to the body part being examined.
As the density of tissue decreases, the percussion note becomes which of the following?
Lower pitched
During assessment of the patient's abdomen, you should auscultate immediately after performing palpation.
False
Abdominal assessment deviates from the IPPA format. Auscultation precedes palpation and percussion so that abdominal sounds are not produced by the nurse's manipulation of the abdomen.
The bell of the stethoscope is best used to hear:
Low-pitched sounds
the bell of the stethoscope is used to auscultate low-pitched sounds, while the diaphragm is used to auscultate higher pitched sounds.
When auscultating the patient's respiratory system, which action should you perform?
Listen to one full breath in each location where you place your stethoscope.
Auscultation
Using the stethoscope to listen to sounds within organs i.e heart & lungs
is performed 2nd during an abdominal assessment, but 4th step in physical assessment as a whole
When assessing the patients radial pulse, what data does the nurse focus on obtaining?
pulse rate
pulse rhythm
pulse amplitude and contour
elasticity of the vessel
While observing respirations, what do nurses look for?
Rate
rhythm
depth
The nurse is preparing to auscultate the posterior thorax of an adult female client. The nurse should do what?
Ask the client to breathe deeply through her mouth.
The nurse's auscultation of a client's lung fields reveals the presence of a wheeze. The nurse should recognize that this adventitious sound results from what pathophysiological process?
Air passing through constricted passageways
The consistent use of gloves and gowns is known to be the most effective means of breaking the chain of infection and preventing nosocomial infections.
False
Rationale: Hand hygiene is the priority infection control measure. Gloves and gowns are often necessary, but hand hygiene is the foundation of all infection control measures and applies in each and every situation.
The nurse positions the client for auscultation of heart sounds. What does the nurse do first?
Clean the stethoscope
Universal precautions are primarily designed to protect the health care worker from what?
Blood-borne pathogens
A client asks why gloves are being worn during the physical examination. What should the nurse respond to this client?
They make sure that any microorganisms on my hands do not touch your skin.'
A nurse is preparing to perform intubation on a client. Which pieces of equipment are needed to prevent the transmission of infectious agents during this procedure?
Gloves,
Gown,
Face shield
True of False: The general survey begins at the moment the nurse meets the patient.
True
When conducting a general survey, you are performing what?
Observing the patient's overall appearance, dress, and approximate age
Rationale: The patient's overall characteristics are the focus of the general survey. Vital signs and review of specific body systems are not normally considered to be within the scope of a general survey. A general survey forms the beginning of the nursing process and does not include the later steps of nursing diagnosis and goal setting.
The general survey uses which assessment technique?
Inspection portion of IPPA
what would the nurse consider to be an abnormal finding during the general survey?
Unable to identify the day of the week
Before completing the physical examination, the nurse determines that the patient is awake, alert, and oriented. This information would be important for which part of the general survey?
Level of consciousness

The nurse observes the client sitting at the side of the bed in the position shown. What health problem should the nurse suspect the client is experiencing?
Chronic obstructive pulmonary disease
Rationale: The tripod position is when the client leans forward and uses the arms to support weight and lift the chest to increase breathing capacity. This position is not routinely assessed in a client with asthma, heart failure, or tuberculosis.
The nurse is assessing a client's gait. Which finding would alert the nurse to the need for a referral for further evaluation.
Shuffling of the feet suggest a problem that would most likely require a referral for further evaluation. Evenly distributed weight, ability to stand on heels and toes, and arms swinging in opposition are considered normal findings.
A nurse in the surgical daycare department has called a client in from the waiting room and is meeting the client for the first time. The nurse immediately observes that the client has a noticeably 'stooped' posture. How should the nurse best follow up this abnormal assessment finding?
Rationale: If you observe abnormalities during the first meeting, you may need to perform an in- depth assessment of the body area that appears to be affected. Abnormal posture would warrant musculoskeletal assessment. Referral would be premature, and there is no pressing need to inform the anesthesiologist. The family history is unlikely to be relevant to an abnormality in posture.
A nurse has completed the general survey of a client who has been transferred to the unit. The information gathered during the general survey primarily provides the nurse with which of the following?
An indication of the level of physical distress experienced by the client,
Clues about the overall health of the client,
Indications about normal variations in the status of body systems
A patient's blood pressure (BP) is 124/80 mm Hg, and they ask you what this means. What should you tell them?
The top number is the systolic BP and reflects the pressure when the heart contracts.
True or False: Critical thinking is especially applicable when the nurse is collecting and analyzing objective data from a patient.
True
A 65-year-old male patient has a blood pressure of 150/90 mm Hg in a lying position, 132/80 mm Hg in a sitting position, and 104/64 mm Hg in a standing position. How should you best interpret these assessment findings?
The change in blood pressure readings is consistent with orthostatic hypotension.
Rationale: Orthostatic hypotension is characterized by significant drops in blood pressure when the patient transitions from lying to standing. This is not considered to be an expected finding in patients of any age. Orthostatic hypotension is not a risk factor for hypertension.
A nurse auscultates a client's carotid arteries, finding the strength of the pulse to be bounding. Which score should the nurse record?
4 +
Rationale:The strength of the pulse is evaluated on a scale from 0 to 4 as follows: 0 = Absent, 1+ = Weak, 2+ = Normal, 3+ = Increased, and 4+ = Bounding.
The nurse measures the height and body weight of a female client with high muscle mass. The client weighs 175 pounds (79.4 kg) and is 68 inches (173 cm) tall. In which of these categories does the client's body mass index (BMI) fit best?
Normal
Rationale:Although a BMI of 26.6 for a female client would normally be categorized as overweight, this client has higher muscle mass. This needs to be considered when providing recommendations for a healthy body weight. Given the factors involved, this client should be categorized with a normal BMI. The client would be best suited to the overweight category if muscle mass was deemed low. A BMI of less than 18.5 is best suited to the underweight category. A BMI of 30 or greater is considered obese.
Upon assessing a patient who is hemorrhaging, the nurse is most likely to assess which compensatory change in vital signs?
Increased pulse rate
A client's radial artery pulse rate is 42 beats in 30 seconds with occasional pauses. What action should the nurse take?
Auscultate the heart rate for a full minute
Rationale:If the radial pulse is irregular, the apical heart rate should be auscultated for a full minute. There is no need to palpate the carotid artery. Documenting that the pulse is 84 and irregular cannot be validated unless the heart rate is auscultated for a full minute. Palpating the radial pulse for a full minute will not necessarily provide the client's correct pulse rate since pauses are occurring.
The nurse assesses the urine output (UOP) of several assigned clients. Which finding is priority for the nurse to address?
UOP 50 mL in 5 hours
The nurse is assessing the quality of the patient's pain. To obtain this information, the nurse should ask:
What does the pain feel like?
True or False: The physiology of pain is best explained by the gate control theory, which describes the passage of pain stimuli from peripheral nerves to the cerebral cortex.
True
What is the best way to take an oral temperature?
By the molars, under the tongue