Developmental Psychopathology
1/95
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
96 Terms
what is a mental disorder?
distressing to self or others
dysfunctional for person or society
deviates from social norms
this all equals judgement of abornormality
what can classification also be called?
nosology
what are examples of contemporary classifications?
DSM-5
ICD-10
what are the features of contemporary classifications?
uses operational definitions
criteria is research based
atheoretical an aetiologically agnostic
what does the term “uses operational definitions” mean?
instead of sayng “typical features of the disorder are A, B, C and D” opertaionla definitions specofy how much of A,B, C and D must be present to diagnose the disorder
what does the term “ criteria are research based” mean?
research is reviewed in expert working groups
what does the term “ atheoretical” mean?
classification does not rely on or endorse any specfic theory about how or why a condition develops
what does the term “aetiologically agnositic” mean?
this means it does not make assumptions about the cause (aetiology) of the disorder
it does not claim to know what causes the disorder
what are the criticisms of contemporary classifications? (7)
high rates of comorbidity
questions the validity of this idea of distinct disorders
inconsistent with dimensionality of psychopathology
criticising the idea that mental disorders are clear cut categories
dsm-5 says you can be diagnosed with MDD if you have symptoms that last for 14 days which means if you have symptoms for 13 days you do not qualify for the diagnosis
seems arbitrary.
causes and treatments often transdiagnostic
CBT is the primary treatment that works well for most disorders
if cases and treatments are very similar does that not mean there is maybe just one big class of disorder rather than all these individual
conflicts of interests
70% of members had a conflict on interest when coming up with DSM-5
pharmaceutical companies were involved in the creation
cross-sectional “one point in time” focus
ignores the longitudinal nature of mental health, including changes, remission, recurrences
overlooks the developmental trajectory of mental illness
medicalisation - over diagnosis
everyday problems or distress may be increasingly labeled as mental disorders
expanding diagnostic criteria risks pathologizing normal human experiences like grief, shyness, etc
most research based on WEIRD samples - not representative of the world
many cultural differences.
what is epidemiology?
it is the study of how diseases or health-related conditions are distributed in populations and the factors that influence them or determine that distribution
in simple terms
who gets sick?
how often?
where and when does it happen?
why does it happen?
and what can be done to prevent or control?
looks at patterns of health and ilness across groups of people - not just individuals
it examines risk factors, causes and protective factors
uses data and statitiscal methods to make sense of trends and test hypotheses
what is prevalence?
how common are mental disorder
what is point prevalence?
proportion of indviduals in a specfied population who the disease of interest at one point in time
what is period prevalence ? (life time or last year prevalence)
proportion of individuals in a specfied population who have the disease of interest over a specfied period of time
what did the longitudinal cohort study investigate?
asessed 1037 people born in dunedin in new zealand repeatedly over 4 decased
conducted clinical interviews for common mental disorders
what is the source for the dunedin study?
(Caspi et al., 2020)
what does this graph from the dunedin study depict?
each person = one line
green = absence of disorder
yellow = indvidual met the criteria for disorder at a given assessment
orange/brown = greater number of concurrent disorders
gray/black = missing/death
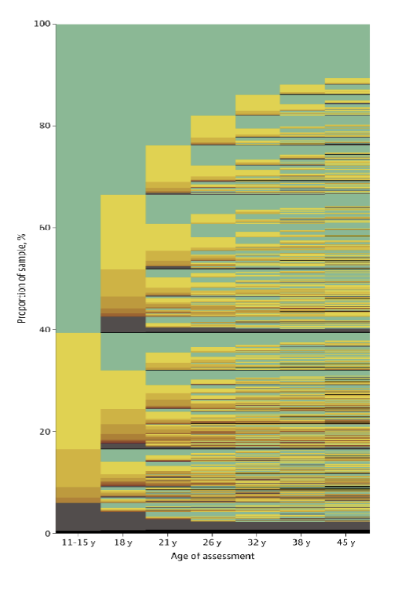
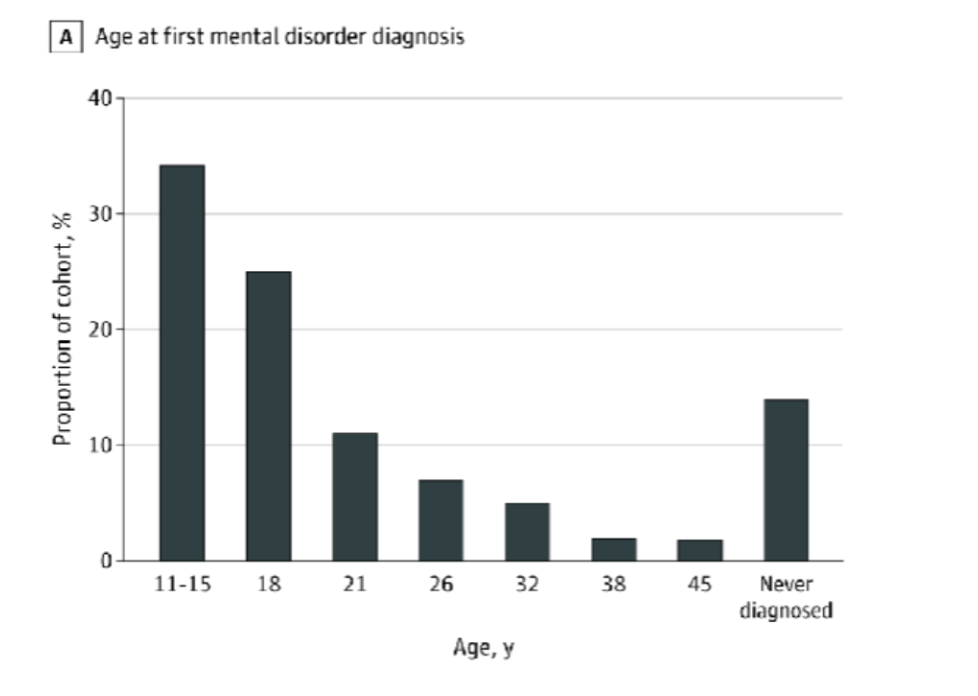
what were the findings for proportions of participants meeting the criteria?
already by age 11-15 a third of particpnats had a mental disorder
by 45 years old, 86% peopple had experienced at least one mental disorder
people who had a disorder once did not necessarily have one again
lifetime prevalance is not unique to this cohort and matched prevalnce reported for mutliple psychitric epidemology studies around the world
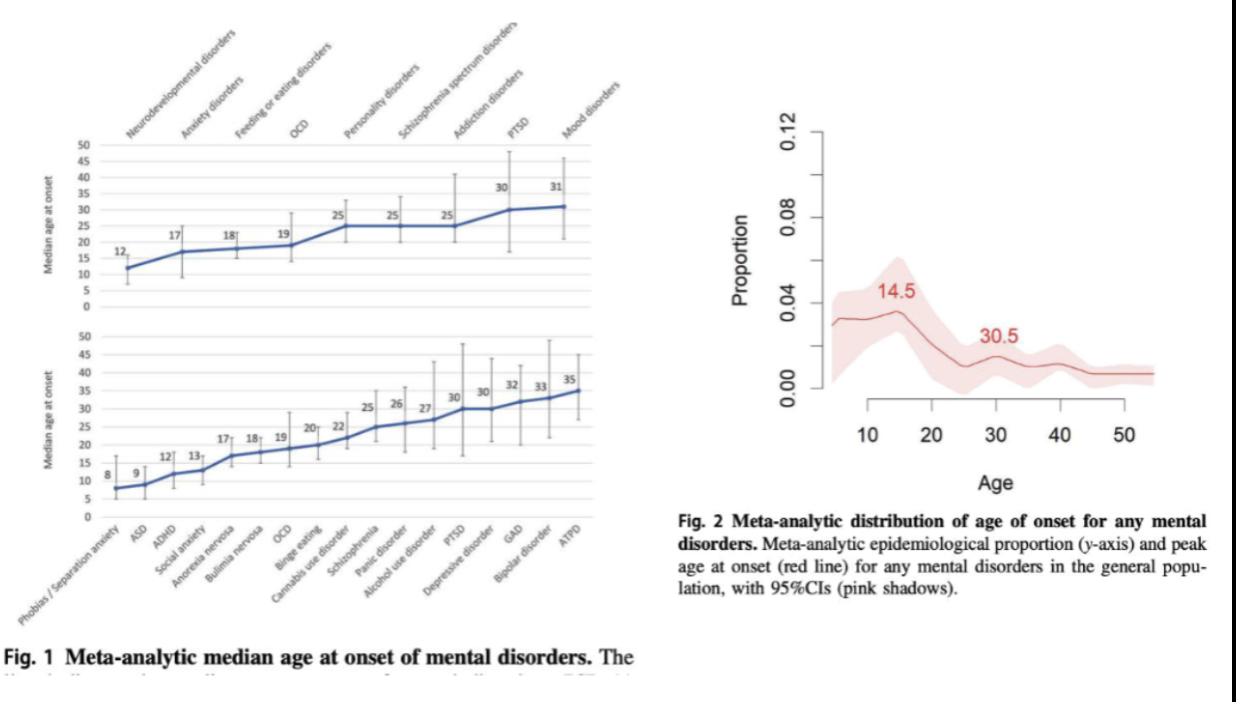
what were the main findings of age of onset from the dunedin study?
most participants received a diagnosis as. ateenaged
virtually no participants received a diagnosis at age 45 years
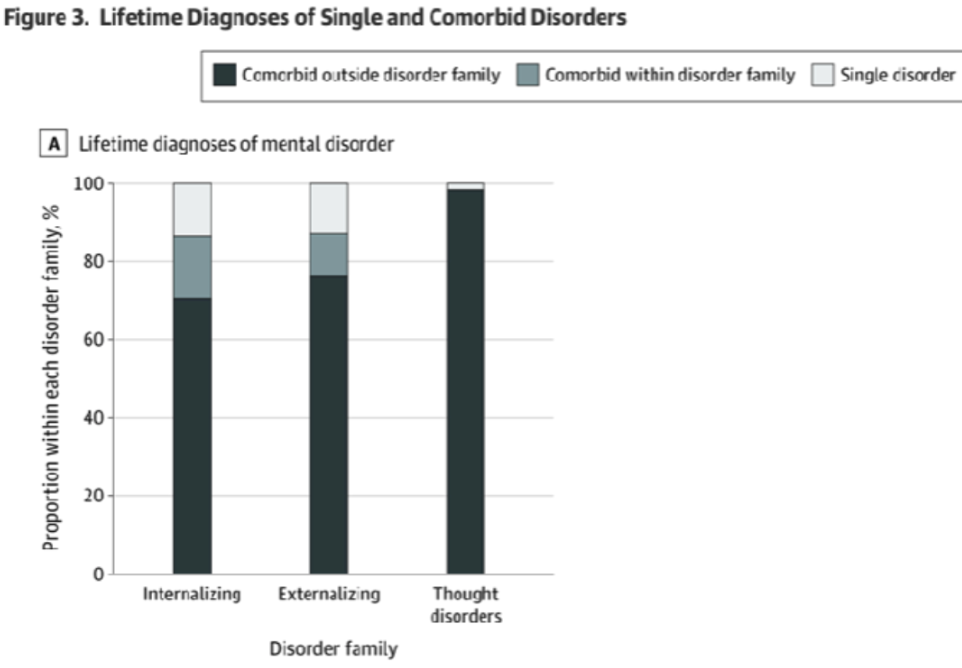
what were the findings regarding comorbidity from the dunedin study?
participants with early onset disorders subsquently met diagnostic criteria for more diverse disorder types
among particpants ever diagnosed with an internalisng disorder, 70% also experienced externalising or thought disorders
by age 45 years, 85% of participnats with a disorder had accumulated comomorbid diagnoses.
what are the typical findings for age of onset of mental disorders?
most mental disorders have their diagnosable onset by ealry adulthood
it is relatively unusual to have a first disorder onset in adulthood
there are differences across disorders
schizophrenia usually onsets in early twenties unless drug induced
what are the general findings of comorbidity across disorders?
rare for people to have just one pure single disorder
people with thought disorders will almost never only have one disorder
comorbidity across disorders is extensive
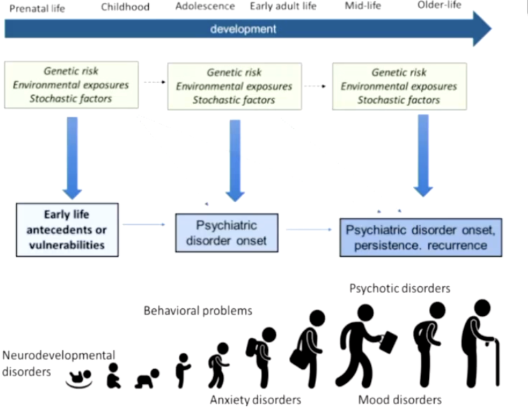
what does the life- course perspective on psychopathology focus on? (8)
to what extent are mental disorders continuing or discontinuing across development?
why do some people have a chronic course? why do some people recover?
homotypical and hetereotypical comorbidities
homo - within disorders
hetero - across different categories
longer term effects of earlier experiences
sensitive periods
cumulative effects
gene-enviroment interplay overtime
age/period/cohort effects
for example , to what extent does your risk of getting a mental disorder influenced by the broader effect of the period of histiry that you’re living in
important to look at asessment of comorbidity when asessing a person with depression you must look at them and decide if they are a person who will have depression once and then recover or have it until adult life
the image shows that some of causes of mental disorders start prenatally
stochastic factors/random factors - someone might get into a car accident and develop PTSD but this could interact with already pre-existing enviormental or genertic risk factors
what are externalising disorders?
attention deficit/hyperactivity disorder
conduct disorder
alcohol dependence
cannabis dependence
other drug dependence
tobacco dependence
what are internalising disorders?
depression
generalised anxiety disorders
fears
social phobia
simple phobia
agoraphobia
panic disorder
post traumatic stress disorder
eating disorders
bulimia
anorexia
what are thought disorders?
obsessive compulsive dirorder
mania
schizophrenia
why should we consider different developmental phases? (4)
prevalence of disorders may differ across age
differences and similarities in presentation
differences in assessment
differences in treatment
what are the reasons for age differences in prevalence?
pragmatic reasons
age retsirctions
sample drop out
genuine age differences
explain the age restrictions for diagnosis?
in the DSM-5 disorders are defined as one that can only occur at a certain age
for example, anti social disorder can only be diagnosed in 18+ years older (even if symptoms had to be present for 15+)
this is because you have to know if these symptoms have been a stable and pervasive pattern
before age 18, people can be diagnosed with conduct disorders
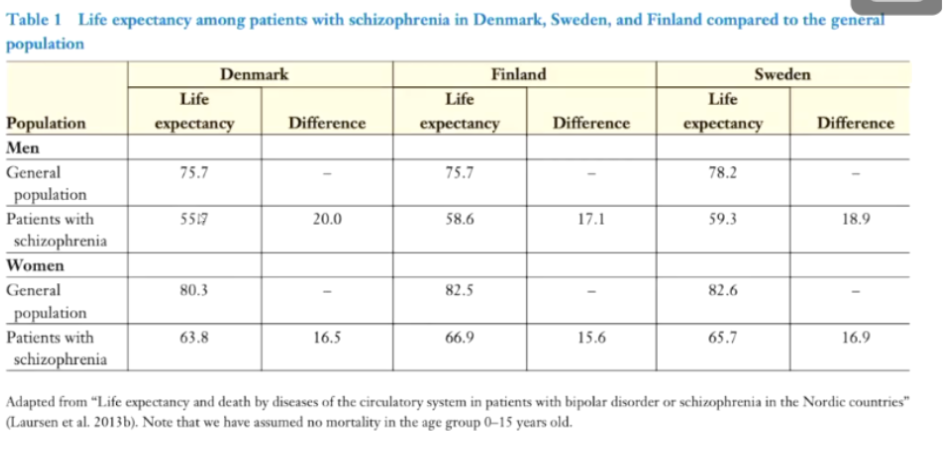
explain sample dropout?
people with disorder die earlier than the general population so are not included in older samples
the graph shows the difference in life expectancy across patients with schizophrenia
majority of the shortened life expectanacy is due to age related diseased not always suicide
there is alos a gap in treatment for people schizophrenia
there is a difference in life expectancy of about 20 years in males and 15/16 years in females across europe
explain the genuine age differences?
anti social behaviour peaks in adolescence
rewiring of the brain cause difficulties of brain processing
adolescents are less able to regulate their behaviour
prevalence of antisocial behvaiour follows a characteristic curve across life
veyr few people have antosicla behaviour that is stable
schizophrenia usually had a peak age of onset in early adulthood
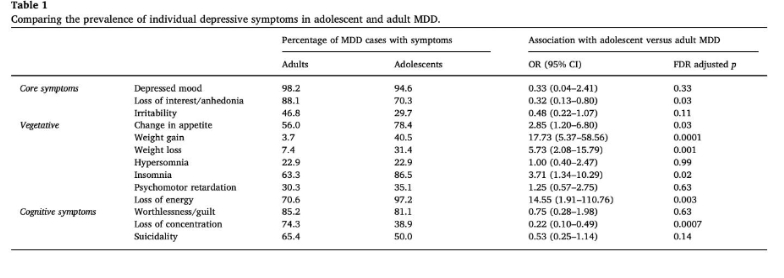
explain the differences and similarities in presentation?
from a paper on adolescent and adult differences in major depressive symptoms profiles
weight loss and weight gain is much more common in adolescents than in adults
vegetative things seems to show most variation
insomnia is much more common in adolescents than in adults
physical symptoms seem to vary quite a bit
what are the differences in asessment, particulary asessment in childhood ?
observe behaviours and interactions throuugh observations and play asessments
interested in how they intercat with others
do they play well with strangers?
follow development carefully over 6, 12, and 24 months
persistence of not making eye contact with childre - something that you see on avarege in autistic childre
rely heavily on caregiver reports
as children get older, play asessemnt becomes more independent rather than guided
berkley puppet interview
helps elicit information on whether there is domestic violence going on at home
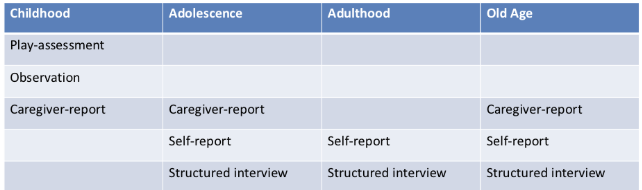
what are the differences in asessment, particulary asessment in adulthood ?
SCID asessment
sometimes you can ask spouses to help understand/ recognise the problem
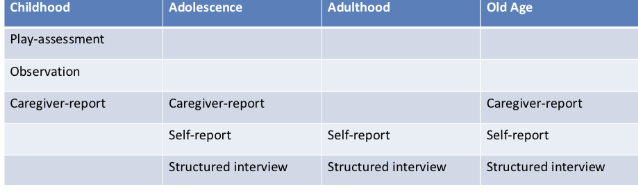
what are the differences in assessment, particularly assessment in old age?
you can also rely on caregiver reports, not from parents but of whoever is looking after the old person as they may not be able to explain what is happening
what are the differences in treatment?
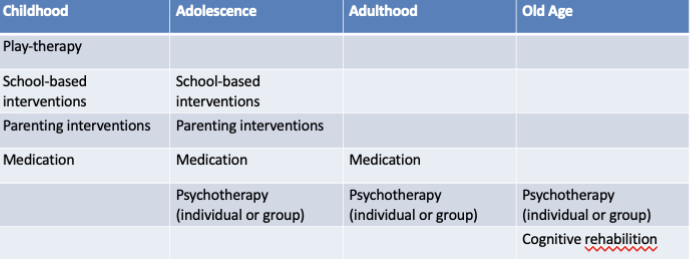
important to note that old people can also get medication
what does mental health in infancy/early childhood look like?
young children can be diagnosed with mental disorders
however it is hard to assess especially when very young
this is because assessment methods need to be age appropriate
there is lots of variation in normal development
children may catch up in development
there can be worries about labelling a child
wuetsions about stability of diagnoses
stability of infant diagnoses
when we just focus on diagnostic criteria for autism, the largets group does not meet the criteria for any of these ages
if a child does not meet the criteria at 18 months, there is a chance they could meet the criteria later
what does mental health in childhood look like?
common externalising problems: neurodevelopmental disorders, anxiety disorders
rare/non existent in childhood : schizophrenia , bipoalr disoder, personaloty disorders
difficulty to distinguish between normal and problemati behvaiour?,m
how to distinguish between normal and problematic behaviour/
lots of children have temper trantrums but do not meet the criteria for diagnosis
severity
persistence
pervasiveness
type of behaviour
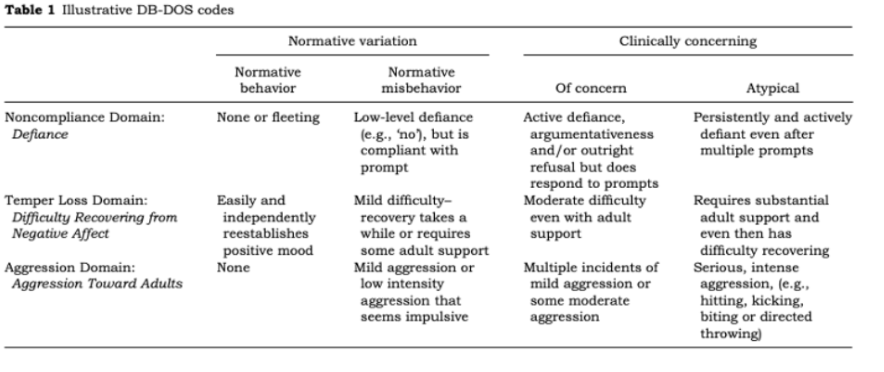
what did researchers come up with to help distingish? and who was it ?
they came up with the DB-DOS
looked at non compliace (defiance )
temper loss domain (difficulty recovering from negative affect)
agression domain (agression toward adult)
within each of these three measures, they distingusiged what a normal child would show and what a atypical child would show
e.g - normative behaviour should be able to move on from tantrums independently but atypical behvaiour finds it hard to struggle with transitions
Wakschlag et al. (2007)
what does mental health in adolescence look like?
this is the key age of onset of many disorders
adolescents face ,any developmental challenges such as integrating with peers, school, puberty, sexual experimces and relationships
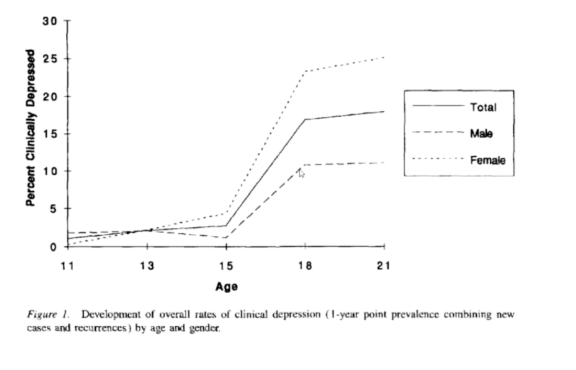
sex differences in some disorders emerge
however no difference before the age of 15v
what does mental health in early adulthood look like?
simialr to adolescence - many disorders first onset here ( schizophrenia)
face developmental challenges of leaving home, beginning college or entering the workforce, little stability/ lots of change
use of drugs and alcohol may become more common during this time
what does mental helath in adulthood/mid - age look like?
relatively rare for disorder to first onset at mid-age
with age, mental disorders can become comobird with physical health problems
diabetes and depression
menopause is currently receiving a lot of research attention for its potential association with new-onset or escalation of mental health problems
drop in antisocial behaviour even in people with antisocial personality disorder
what does mental health in old age look like ?
severe menyal disorders, esp new onset, in older age is relatively more rare than in developmental periods
because of earlier mortality
can be harder to identify symptoms in older people
there may be some growing out of symptoms (but it is rare)
mental disorders can sometimes develope secondary to other problems e.g dementai
what can be used to detect ADHD in very young children?
the DC: 0-5 is more inclusive, offering clinicians the ability to use the nosology to characterise the clinical presentation of veyr young children
some children under 36 months of agre present with extremes of hyperactivity or inattention and/or impulsivity
parent reports of hyperactvity/impulsivness at age 19 months were signficantly associated with teacher reports at 72-84 months
does mental illness often run in families ?
yes
if both biological parents have a condition your chnaces of getting the disorder are greatly increased
this could be explained through envrioment and genetics and how these both combine instead of one or the other
what is an example of mental illness running in families?
the galvin family
based in the US and there were 12 children, 8 out of the 12 children developed schizophrenia
what is the liftime chance of getting schizophrenia and bipolar disorder?
1 in 100
what is the chance of getting SZ or BPD if one of your biologicla parents have the condition?
6 in 100
what is the chance of getting SZ or BPD if both your biological parents have the condition?
45 in 100 sz
40 in 100 bpd
what is the chance of getting SZ or BPD if your brother or sister has the condition?
9 in 100 sz
13 in 100 bpd
what is the chance of getting SZ or BPD if your identical twin has the condition
40-50 in 100 sz
40-70 in 100 bpd
what is the chance of getting SZ or BPD if your non identical twin has the condition?
17 in 100 sz
20 in 100 bpd
nature vs nurture?
think about how they combine rather than one or the other
what are some goals of psychiatric genetic research?
quantifying overall genetic influence
how much genetic influence is there on ADHD
identifying specific genetic variants
is there a particular genetic variant associated with schizophrenia
proven to be quite tricky
studying gene-environment interplay
how does genetic liability and parenting combine to influence risk of antisocial behaviour?
what are tools of psychiatric genetics?
quantative-genetic approaches
inferring genetic influences
twins, adoptees
molecular genetic approaches
measuring genetic variation directly
genome wide association studies (GWAS)
what are twin studies and what are the three components that make up twins?
twin studies allow us to estimate how much a trait comes from our genes and how much of that is influenced by environment
genetic influences, shared environments, non-shared environments
what are shared enviroments ?
these make identical twins and non identical twins alike
they are often thought of as family wide influences because they affect members of a family equally. e.g - SES or neigbourhood
if there was differences between identical twins what would this be due to ?
non shared enviromental influences
what percentage of genes do twins share? identical/ non identical ?
identical twins share 100% of their genes
non identical twins share 50% of their genes
if they share some of their other characteristics then this could come from families as they are both brought up in the same enviorment
what are the statistics for genetic infleunces of different traits/behaviours/disorders?
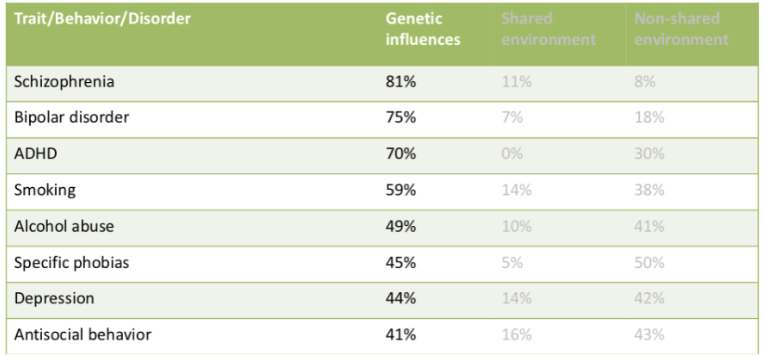
these estimated are based on a meta analysis and all are approximate
important to consider that if you expose 100 people to the exact same event, not all people are going to develop PTSD
some of these rely on the environment, if there is no alcohol in the environment, then there will be no alcohol abuse
what is a gene enviroment interaction interplay?
where all of these people may experience the same event or they may all be exposed to alcohol at univeirtsy and some will emerge from these experiemces without any issues with alcohol but thse may have genetics that are slightly different coudl develop issues
MYTH: heritability refers to individuals . TRUE OR FALSE?
FALSE
refers to populations not indviduals
40% of differences between people in depression are due to genetic differences between them
not 40% of ones depressiom
MYTH: heritability is fixed, it does not change. TRUE or FALSE?
FALSE
heritability can change and vary across history and in different cohorts
in more recently born cohorts, heritability of women’s alcohol has increased which could be due to alcohol use becoming more socially acceptable
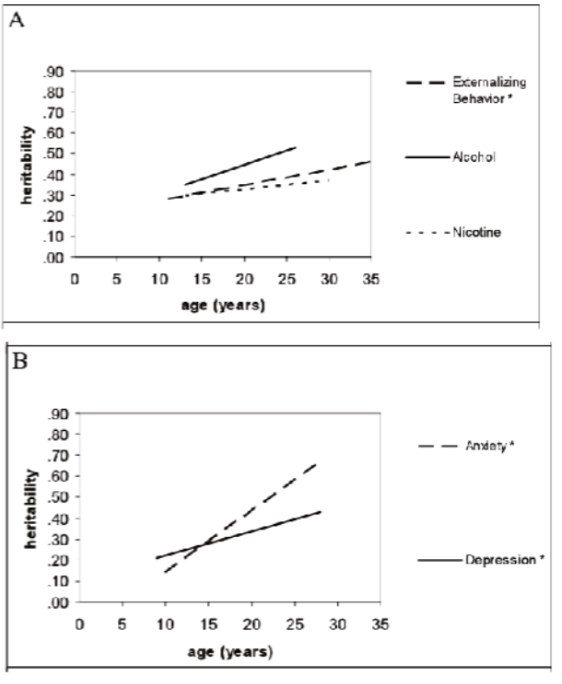
can change across age/development
as children grow older heritability tends to increase for some mental health problems
can change across environments
in neighborhoods where there are more alcohol outles and more opportunities for buying and presumably also consuming alcohol. there is greater heritabiloty of alcohol use
MYTH: high heritability means non malleability, i.e that a mental health problem cannot be changed - TRUE OR FALSE?
FALSE
there are ways of how environmental influences can modify to what extent a genetic disposition can manifest itself
short sightedness is very highly genetically influenced yet ome can wear glasses to soften the impact
someone who inherits a geentic risk of alcohol abuse decides to expose themsleves to alcohol
can you describe the molecular - genetic methods?
an entire set of 23 human chromosones is called a genome
human genome is composed of 3 billion base pairs
variation at a single base pair is called a SNP
there are around 10 million SNPS in the human genome which account for many of the genetic differences between you and everyone else
some SNPS account for differences in appearances, other can affect how we develop diseases or respond to drugs
direclty measure genomic variation
most currect research focuses on relativley common variants
what are candidate gene studies?
popular approach from approx 2003-2016
selected specific genetic variants a priori ( serotonin transporter gene 5-5HTT)
tested association between these outcomes either individually or in interaction with emvriorment
very poorly replicable
what replaces candidate gene studies?
genome wide association studies (GWAS)
what are GWAS studies ?
they do not just look at one particular genetic variant. they look at the whole genome
there is no prior selection of specific variants, they test thousands of variants
statistically much more sop
they calculate polygenic scores across many variants
higher scores - higher risk
what have we learned from psychiatric genetics research?
there is no single gene for mental disorders
for the most part mental disorders appear to be infleunced by many common genetic variants that each have a tiny effect
in other words mental disorders are polygenic not monogenic
there is shared heritability across disorders
higher genetic risk for one mental disorder is often associated with higher genetic risk for other disorders too
could partly explain high comorbidity across disorders
there is gene-envrioemntal interplay
what is the evidence for the gene enviorment interplay ?
stress vulnerability model
idea the more stressors in ones environment increases their vulnerability
e.g - person may carry a genetic vulnerability for SZ but they may never develop it unless they experience significant stress such as drug use, trauma, or social isolation
what is gene-environmnet correlation? implications? examples?
this is when environments don’t always happen to people randomly
example- children’s peer groups, often parents say “ my child fell in with the wrong crowd”. unfortunately it does seem to be the case that children often select their peers. children who are more prone to risk taking choose peers who are the same.
implications:
can be highly controversial, risk of victim blaming
but important tp consider when studying why mental illness develops
can guide us towards interventions
examples
a lot of policy effeort and interest in the legalistaion of cannabis
idea that if teenages or young adults have more access to cannabis because its legal, more likely to get schizophrenia
reserach suggests that if you have a genetic risk to dveelop schizophrenia, you are more likely to smoke cannabis
what are examples of microenvironmental influences? (6)
parenting
maltreatment
peer relationships
built environments
neighbourhoods
socioeconomic status
what is one way you can categorise environmental influences?
bronfrenners ecological systems
explain bronfenners ecological system?
microsystem - immediate environment
families, parents, schools.
immediate interactions individuals has with the environment
exosystem - friends families. neighbours, legal services
meso system - the way in which micro system intercats with the exosystem
macrosystem - things that are properties of country, culture and society that the individual lives in
chronosystem - particualr point in time that someone lives in
for example, pandemic or war
what are the three challenges for studying effect of enviornmental influences?
they can be difficult to measure
parents don’t report
child isn’t aware that what they are experience is abuse
they might not have immediate effects
longitudinal follow up studies might be better however these are expensive and harder to do
they cannot be easily studied using casually informative research designs
what is the hierarchy of evidence?
how good the quality of evidence is and how high the risk of bias is
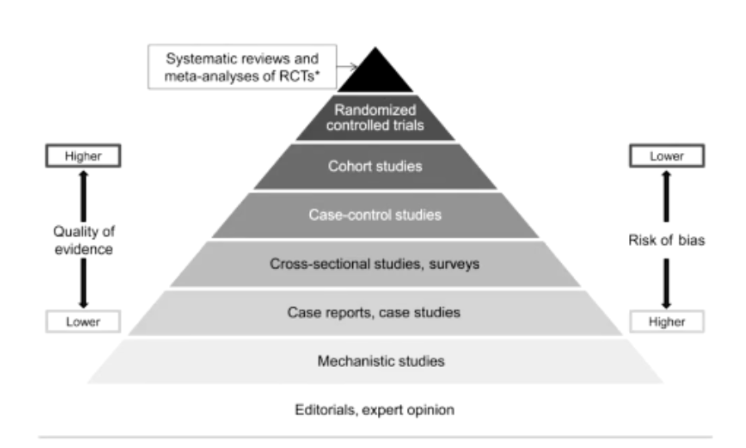
randomised controlled trials/ systematic rviews and meta-analyses of RCTs are highest quality and lowest of bias
editorials, experts opion are low quality and high bias
what is a problem of for mosy hypothesised risk factors randomised controlled trials?
they are typically unethical/ impractical
cannot assign someone to experience maltreatment, peer victimisation, war or diseased
what 4 biasses are introduced due to a lack of casually informative designs?
reporting biases
reverse causality
environmental confounding
genetic confounding
how do you measure parenting?
observational measures
unstructured tasks - play with your child for 10 mins
structure tasks - parents fill out form while child is playing next to them
home observation - wander around, see how many toys there are, focus on specfic aspects of parental behaviours and measure something like langauge development
voice recordings
informant reports
from child
from parent
what do you measure when parenting?
positive and negative parenting
what are examples of positive and negative parenting?
positive parenting
high warmth, affection
effective discipline
parental monitoring
negative parenting
dissatisfaction
shouting,hitting
chaotic home enviorment
what is a common measure of parent child relatinships and what is common finding from this measure ?
Robert C. Pianta scale
you see a skew in the questions that ask/ state “ i act warm to my child”
what are 4 challenges in interpreting association from parenting?
reporting biases
reverse causality
environmental confounding
genetic confounding
what is reporting bias in parenting?
in this study it explains that the child behaviour was completed by the primary caregiver at each time point to assist presence of child internalising and externalising symptoms
research suggests that mother who are depressed are more attuned to negative behaviours
therefore mothers with depression may rate their child’s internalising problems higher than mothers without
if completed by the same informant for predictor and outcome
could lead to a possible distortion by maternla depression

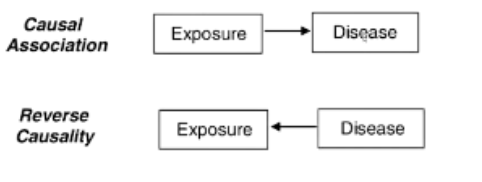
what is reverse causality in parenting?
this is when instead of poor parenting leading to internalising disorders it means that internalising problems cause the parents to perform poorly or act in a neglectful way
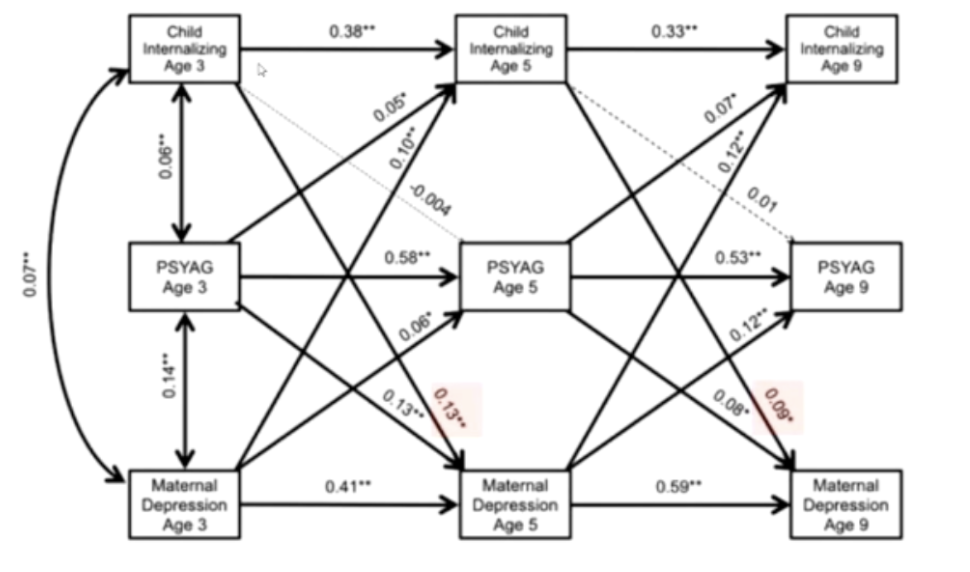
this graph shows that internalising at age 3 predicts maternal depression at age 5
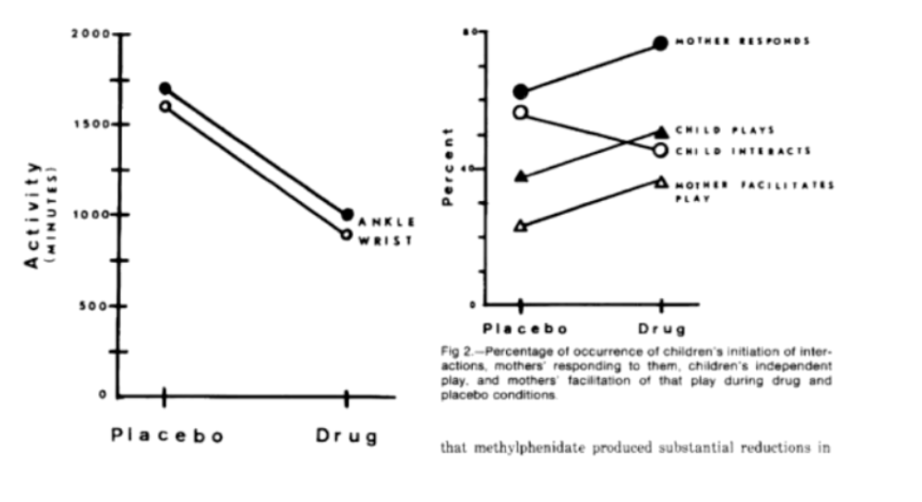
another study was done where mothers reacted more positively towards their hyperactive children when they were on medication
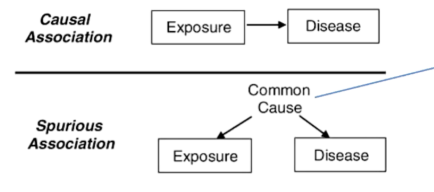
what are the enviormental confounds in parenting?
the common cause could be things such as;
family socioeconomic status
antisocial father
neigbourhood
these factors could have a direct impact on parenting
what are the genetic confounds in parenting (3)?
passive gene-environment correlation
evocative gene-environment correlation
active gene-environment correlation
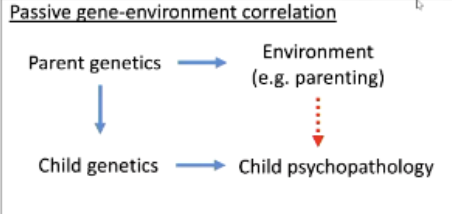
what is passive gene-enviornment correlation?
where genetic influences in parents might affcet the envrioment they provide for their children
example - parent at risk for depression may pass these genes to their child (increasing risk of depression) but also parent in less warm or more negative eays whihc may impact the child
what is evocative gene-enviornment correlation?
parent behaves differentlt toward the child based on their genetic disposition
example - a child with a genetic tendency toward ADHD might be more impulsive or difficulty which could cause their parent to be more harsh, frustarted or controlling
what is active gene-environemm correlation?
young perosn’s genetics lead them to select themselves into certain environments
example - a teenager with a genetic risk for risk-taking might seek out peers who drink or engabge in delinquent behavior
therefore experienced more conflict with parents as a result
what can we do about the challenges in interpreting association of parenting?
run RCT for parenting interventions
quasi experiments for treatments for maternal depression
genetically - sensitive designs, adoption design, twin differenes designs
high quality observational data
longitudinal
multiple informants
what is the example of the twin differences deisgn?
NASA did an expeirment where a set of twins provided lots of measurements including heart rate and various other forms of biological functions
one brother went into space and one styaed behind
when the brother came back, they comapred them on all the indicators
another examples was mesuring twins with differences in parening
the twin who revived more warm parenting from their mother dispayed fewer externlasing problems
effects were small