Psych 261 Midterm 2
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
Neuroplasticity
Modification of the tissues of the brain throughout the lifespan
Neurogenesis
Formation of new neurons in the NS
Neurogenesis Locations
1) Subventricular zone by the lateral ventricles
2) Denate gyrus of the hippocampus
3) Striatum (likely via. adjacent subventricular zone)
Neurogenesis Process in the denate gyrus of the hippocampus
Type 1 Radial Stem Cells (astrocytes) divide
Type 2 Non-Radial Stem Cells formed
Type 2 cells multiply and give rise to immature neurons
Immature neurons differentiate to form mature neurons that are integrated into the neural architecture
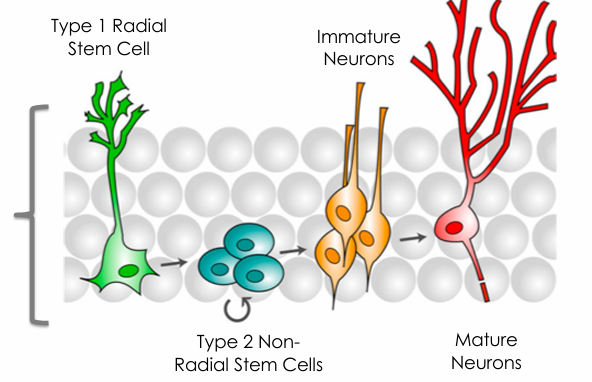
% turnover + # of neurons generated in the adult hippocampus
1.75% turnover (~700)
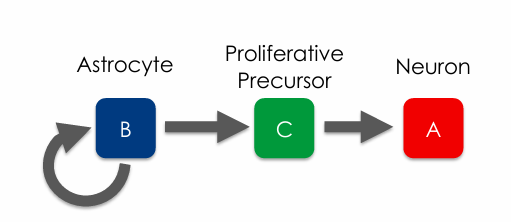
Neurogenesis Process in the subventricular zone by the lateral ventricles
Ependymal cells form the ventricular zone.
Beside the ependymal cells, there are 3 types of cells (B, C, A)
Type B cells (astrocyte) can self-renew and also give rise to Type C cell
Type C cells are proliferative precursors that form type A cells which are new neurons.
Difference & similarity b/w neurogenesis in denate gyrus vs. SVZ
1st step for both involves glia
DG - Type 2 non-radial stem cells (2nd step) can either multiply or give rise to immature neurons
SVZ - Type B (astrocyte) (1st step) can self-renew or give rise to neurons
Where do type A cells (neurons) go after being formed in the SVZ
In rodents & other mammals, Astrocytes bundle up the new neurons and migrate them to the olfactory bulb via the rostral migratory stream
In humans, they make their way to areas close to the SVZ, such as the striatum.
Evidence that neurogenesis occurs in the SVZ in humans
Astrocytes w/ neural stem cell characteristics identified
SVZ has the ability to produce neuroblasts (stem cells)
3 Ways to increase neural plasticity
Exercise
Diet
Learning
How does exercise influence neural plasticity
Increases neurogenesis + growth/complexity of existing neurons by triggering the release of brain-derived neurotrophic factor(BDNF)
Brain-derived neurotrophic factor (BDNF) functions (4) + how is it transported
Major neuron growth molecule (supports the growth of neurons and synapses)
Transported retrogradely & anterogradely
Potentiates synaptic transmission
Involved in gene transcription
Modifies synaptic morphology
Enhances neuronal resilience
(PIME)
What happens when BDNF binds to their TrkB receptors?
Presynaptically - Modify transmitter release
Postsynaptically - Modify postsynaptic sensitivity (ex. w/ NMDA receptors)
What does exercise enhance in addition to neural plasticity?
Cognitive performance (executive control, controlled processing, visuo-spatial ability, response speed)
(EC VR)
Does decreasing your energy intake increase neuronal growth?
Yes.
mRNA for growth factors of BDNF increased w/ energy intake reduction. Additionally, higher neurogenesis is observed.
Dietary restriction increases (4)
Neurotrophins (ex. BDNF), antioxidants, removal of damaged molecules, and reduction of inflammation/oxidative stress
(NADIO)
What phenomenon allows dietary restriction to have positive effects?
Hormesis/preconditioning - exposure of cells/organisms to a mild stress results in adaptive responses that protect against more severe stress
(think of going to the gym - body builds back stronger after a stressor)
Types of dietary protocols (4) & which are the most effective?
Western (3 large meals w/ snacks interspersed)
Caloric restriction (CR) (eating smaller meals - cutting caloric intake by ~30%)
Time Restricted Feeding (TRF) (eating a normal amount, but restricting that to a 4-8 hour period)
Intermittent Energy Restriction (IER) (interspersing days of normal eating w/ days of energy restriction)
Beneficial effects on the brain even when the overall # of calories remains the same as a normal diet (TRF/IER)
Including periods of fasting might have greater benefits than simply reducing caloric intake.
HFS vs LFCC diets influence on brain plasticity
(High saturated fat/refined sugar vs low saturated fat + complex carb)
Inc BDNF & performance
What brain change occurred when squirrel monkeys trained a dexterous grasping task?
The motor cortex finger‑representation area enlarged after ~12 days of training.
What neural changes occur after 3 months of juggling training?
Increased gray matter in the left posterior intraparietal sulcus and mid‑temporal motion‑processing areas.
How does long‑term violin training change somatosensory cortex?
Enlarged representation of LEFT‑hand digits in RIGHT S1 (the hand used).
Stroke/cerebrovascular accident def’n
Disruption of normal blood delivery to brain tissue
Two types of strokes & which is more common
Ischemic (more common) & Hemorrhagic (10-20%)
Ischemic strokes
Arteries/capillaries blocked by either:
Floating debris
Buildup of material inside the blood vessels
Constriction of the blood vessels
Prevents nutrients from getting to brain cells, ultimately resulting in death of the cells in the region supplied by the blocked blood vessels.
Hemorrhagic strokes
a.k.a Intracerebral hemorrhage (ICH)
Involves a RUPTURE of a blood vessel in the brain
Occurs due to either a traumatic brain injury or other factors, including high blood pressure.
Severity depends on the amount of blood lost. (>150 mL) results in blood pressure in cerebral vessels that is insufficient to supply the remainder of the brain, leading to death.
Hematoma
A large blood mass in the brain, which can put pressure on critical parts of the brain, can lead to death (just as blood loss from the arteries/capillaries can at the same time).
What % of hemorrhagic strokes result in death soon after
40%
Death caused by ischemic stroke reason
Exitotoxicity - over-activity of nutrient-starved cells
Exitotoxicity mechanisms mechanism #1
Cerebral blood flow drops b/w critical lvl
Energy demands outweigh nutrient availability
Energy-dependent ion channels (ex. Na+/k+ pump) work less efficiently, causing Na+ buildup in the cells
Cells are depolarized and inc NT release into the synaptic cleft
Exitotoxicity mechanisms mechanism #2
Astrocyte (involved in tripartite synapse) have transporter proteins (some are also present on neurons) responsible for clearing glutamate
As the levels of glutamate increase - they can’t keep up
Additionally, transporters begin to malfunction & can even reverse (ejecting more glutamate into the synaptic cleft) as a result of insufficient energy supply
Exitotoxicity mechanisms mechanism #3
An increase in glutamate - even 100x (caused by inc Na+ in cells & less being cleared by transporters on astrocytes) leads to more positive ion influx into local cells
Furthers the problem - even more glutamate is release
Glutamate receptors let what ions into the cell - what effect does this have?
In addition to Na+, NMDA receptors allow Ca2+ into the cell (glutamate gated calcium channels)
Calcium enters in large amounts due to excess stimulation of these receptors (from elevated lvls of glutamate)
Impact of excess calcium influx on cells
Impairs mitochondrial function, disrupting the production of ATP
Further compromising energy supply to active mechanisms (ex. Na+/K+ pump)
A series of chemical reactions occur that lead to the production dangerous free radicals such as nitric oxide (NO), which causes dmg to nearby cells
Problematic roles of nitric oxide (3)
Destroy organelles inside the cell (ex. proteins, nucleic acids, and liquid membranes)
Triggers more glutamate release
Precursor to a molecule involved in triggering apoptosis
Main NT of interest in stroke pathology
Glutamate (excitatory)
Cytotoxic Edema Mechanism & Impact
Positive ions accumulate in BOTH neurons & glia - water is osmotically drawn in from extracellular regions. Leads to swelling.
Disrupts protein function & physically stresses cells
Ultimate result of ischemic stroke (2)
Necrosis - ishcemic cells rupture, spilling their contents into intercellular space.
Apoptosis - dissolution of the contents of the cell
Necrosis seems to occur first
Summary of the effects of ischemic stroke
Decreased nutrient supply
Increased Na+ in cell
Increased glutamate release (due to elevated Na+ & astrocyte transporters being overwhelmed by glutamate to pick up & reversing when they do not have sufficient nutrient supply)
Calcium lvls elevate as glutamate binds to NMDA receptors (which allow Na+ to enter the cell but also calcium when there is sufficient glutamate)
Calcium results in NO (free radicals) - which destroy organelles, release more glutamate, & release precursors to apoptosis.
Ultimately necrosis &/or apoptosis
Hemorrhagic Stroke Additional Counterintuitive mechanisms
Blood pools outside of the ruptured blood vessels, creating a hematoma which mechanically puts pressure on the surrounding cells, disrupting their function.
Lower blood flow in the surviving arteries leads to similar events seem w/ ischemic stroke
Can cytotoxic edema be caused by both ischemic & hemorrhagic strokes?
Yes
Dmg from a hematoma as well as ischemia caused by vasoconstriction can lead to cytotoxic edema
What enzyme does a hemorrhage produce - why & what effects does this have
Surrounding cells produce thrombin (criticial to clotting)
Helps stop bleeds via coagulation
High concentrations - make NMDA more responsive to glutamate, leading to excitotoxicity - often can cause apoptosis in glia + neurons
Thrombin triggers inflammatory responses from microglia, release pro-inflammatory markers & free radicals
Cell Dmg as a result of hemorrhagic stroke (from hematomes)
The immune system (microglia) considers blood spill an invader - inadvertently damaging local brain cells
Iron is released from hemoglobin from RBCs - creates free radicals that cause oxidative stress, damaging surrounding tissue
Plasma flows into interstitial space, causing vasogenic edema (water enters), putting further pressure on the cells, disrupting their function
Traumatic Brain Injury Unifying Factor
Brain dmg results from external forces (direct impact, rapid acceleration/deceleration, penetrating objects, blast waves, etc.)
The nature/intensity/direction/duration determine the dmg
Which type of TBI is most common w/ athletes & effect(2)
Impact deceleration injuries (head is moving and come into contact w/ stationary object)
Results in coup or countercoup (dmg is site directly adjacent to point of impact - skull is driven into brain OR dmg is on the opp side of the head where the brain and skull again make contact on the rebound)
Impact to the head Primary Damage (3)
Hematoma formation in the cerebrum or around the meninges
Contusion (local area of brusing involving small tears in blood vessels)
Diffuse axonal injury from general axonal shearing
Lead to various lvls of ischemia b/c of impaired blood flow caused by the injury
Primary Damage from TBI effect
PD (causes ischemia) - Contributes to swelling (edema).
Cytotoxic edema and/or vasogenic edema
Locally or throughout (diffuse traumatic brain edema) the brain
Swelling inc intracranial pressure & dec cerebral perfusion pressure, inc the likelihood of ischemia (reduced nutrient availability)
Ischemia, swelling, & bleeding big 3 effects
Inflammation
Exitotoxicity
Oxidative Dmg
Brain dmg associated w/ an acute traumatic brain injury is referred to as a
Concussion
Symptoms - headache, nausea, dizziness, and memory/attention problems (DHMAN)
May resolve w/i a week or two
Chronic traumatic brain injury Cause & Effect
Repeated impacts to the head
Associated w/ Alzheimer’s, Parkinsons, mood disturbances (impulsiviiy), and impaired cognition (memory/attention) (AP MC)
Dmg can effect cytoarchitecture of neurons, cerebral blood loss, and white matter atrophy
Following focal damage caused by an ischemic stroke, what occurs?
Necrotic (dead) tissue in the main area of the dmg is surrounded by a penumbra of live, but struggling cells.
Denervation - Cells in the penumbra that were connected to now dead cells lose axonal input
Spine collapse - dendrites of survive cells shrink b/c there is reduced input
What immediately happens to the surviving cells follow an ischemic stroke?
Decreased activity
Axons that are damaged by the stroke are prevented from re-growing by inhibitory signals
Spontaneous Recovery: Initial Events
Weeks 1-4 post-stroke
Brain kicks in adaptive plasticity mechanisms -
Considerable synaptogenesis
Dendritic spines reappear (potentially in diff locations/shapes)
Local axons begin to sprout axon collaterals that connect to denervated dendritic regions (even long-range axons)
Inc growth factors (ex. BNDF) - upregulated
Inhibitory GABA receptor activity dec
Excitatory NMDA receptor activity inc
Spontaneous Recovery: Network Reorganization
Weeks 4-8 post-stroke
Reorganization of cortical networks is already underway.
Network Reorganization Example (stroke to part of the somatosensory cortex previously represented by the forelimb)
Initial Effects & 1-4 weeks after
Some of the neurons representing the forelimb die + the surviving tissue is affected by dendritic spine collapse and less efficient neuronal functioning
One to four weeks after the stroke, more neurons are responsive to both fore- and hind-limbs.
Increased growth factors, dendritic spine remodeling & axonal spouting, and excitability. Reduced sensory specificity.
Increase in connections b/w the various limb regions of the somatosensory cortex.
Network Reorganization Example (stroke to part of the somatosensory cortex previously represented by the forelimb)
4-8 weeks after
A drop in the number of neurons responding to both limbs
Region of the cortex responsive to forelimb has expanded and taken over some of the territory of the hindlimb
Topographic reorganization of the somatosensory cortex after a stroke
Large Scale Network Reorganization
It can cross hemispheres
For example, people who experience a stroke to their subcortical motor pathway in one hemisphere might end up with increased connectivity between the ipsilesional motor areas and the motor areas in contralesional hemisphere.
At the same time they might show reduced connectivity between the thalamus of the ipselisional hemisphere and motor areas in the contralesional hemispheres.
Connectional Diaschisis
The reduced connectivity among areas distant from a stroke (that is beyond the penumbra)
Functional Diaschisis
Some brain areas further away from the stroke focal point might experience less activity in response to a stimulus or when they are involved in a given behavior.
Diaschisis General Meaning
Reduced activity in or reduced connectivity with areas that are relatively distant from the focal lesion, that is, those that are beyond the penumbral region.
Reorganization as a result of deprived input occurs when?
Somatosensory cortex/motor areas may be derived of their regular input.
May involve the loss of a limb)
Phantom Limb Syndrome
Continued sensations coming from the lost limb
Feeling like the limb is touched is rare - pain is common
Phantom Pain Mechanisms
Peripheral - injured nerve endings, altered activity in the dorsal root ganglion (contains sensory nerve bodies)
Can also occur due to the reorganization of the sensory & motor areas of cortex.
Ex. When amputees with phantom limb pain move their lips, activity appears not only in the face area of the motor and somatosensory cortex but also in the cortical region that previously represented the now‑amputated hand, showing expansion of the lip area into denervated hand territory. Brain doesn’t know that the sensations are now coming from the face and not the hand.
(amputees without phantom limb pain do not show activation of the hand area when moving their lips)
Spontaneous Recovery: Neurogenesis & Gliogenesis
In addition to network reorganization, the mammalian brain attempts to recover function after a brain injury by increasing the production of new cell
In rodent models of stroke, the source of new neurons that migrate to ischemic brain areas appears to be the subventricular zone.
One possibility is that newborn neurons migrate from elsewhere (such as the subventricular zone), using blood vessels as scaffolds for migration or as destination markers. Alternatively, these neurons could arise locally,
Neurogenesis after TBI
Neurogenesis mainly occurs in the peri-damaged brain regions after TBI in humans. However, it remains unclear whether these cells are born locally or from neurogenic regions.
Drug Therapies
Might mitigate the damage associated with brain injury and to speed recovery.
Would have to consider the timeline of brain injury and spontaneous recovery
(during and right after the injury, it would be helpful if the patient could take a drug that reduces neuronal overactivity. In contrast, after the initial damage, the problem is one of underactivity of the remaining neurons. Thus, some time after the injury, it would be useful to have a drug that increased the activity of underactive neurons.)
Injury = acute hyperactivity → you’d want to calm neurons.
Damage = chronic underactivity → you’d want to boost neurons.
The one drug therapy that has been shown to be useful
Ued as an early intervention during ischemic strokes
Tissue plasminogen activator (tPA) . . . tPA works by dissolving the clot and improving blood flow to the part of the brain being deprived of blood flow.
Administer w/i 3hrs
Training-Induced Recovery
Deficits associated with brain-injury can be ameliorated for up to a year post injury by applying rehabilitative training technique
Enriched environment and training induced dendritic growth in the spared tissue.
Stem Cell Therapy
Involves the introduction of stem cells into the post-stroke brain
Shown to improve behavior and brain function
Stem cells from monkey embryos, intravenous injection from bone marrow stem cells… lead to formation of new glia & neurons.
Intravenous injection of peoples’ own bone marrow stem cells (harvested under local anesthesia) led to better recovery after ischemic strokes when compared to control stroke patients who did not receive the treatment.
Brain Stimulation For Motor Recovery Post-Stroke
After stroke, motor cortex activity becomes imbalanced across hemispheres: the lesioned hemisphere is underactive while the contralesional hemisphere over‑inhibits it.
Anodal tDCS over the lesioned motor cortex boosts activity and promotes neural growth, while rTMS or cathodal tDCS over the contralesional cortex reduces its over‑inhibition, allowing the damaged hemisphere to regain function.