UNIT 3 AVSD Anomalies
1/54
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
55 Terms
What is an atrioventricular septal defect, and list the 4 other names used for it.
An atrioventricular septal defect is characterized by what? with abnormalities where?
An atrioventricular septal defect is characterized by a deficiency in the AV septum with abnormalities of the inflow valves.
AVSD
Atrioventricular defect
AV canal defect
Endocardial cushion defect
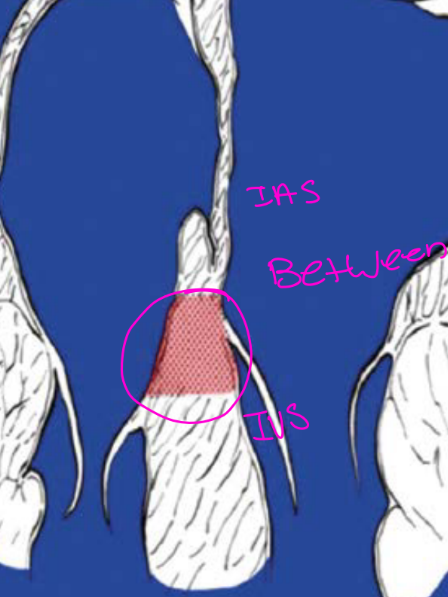
(AV septal defects are between the IAS and Ventricular septum, its still more of the muscular portion of the ventricular septum will be in the inlet area and also the primum area of the Atrial spetum b/c of the location it causes inflow anomalies)
The pic shows the nob of tissue / button of the AVSD
List the 6 factors that determine the severity of an AVSD.
The severity of the defects are characterized by the involvement of:
Involvement of the atrial septum
Involvement of the ventricular septum
Extent of the inflow-valve abnormalities
Presence of a common annulus or 2 separate valve openings
Associated cardiac anomalies
Differences in ventricular size
List the 4 incidence and association facts about AVSDs.
Has a high association with what disease?
what % of children with what chromosomal abnormalities have AV canal defect***
They are associated with what abdominal situs?
what gender are they more common?
High associated with congenital heart disease
About 45% of children with trisomy 21 have an AV canal defect**
They are associated with heterotaxy, including asplenia (bilateral Right siedness)
They are more common in females
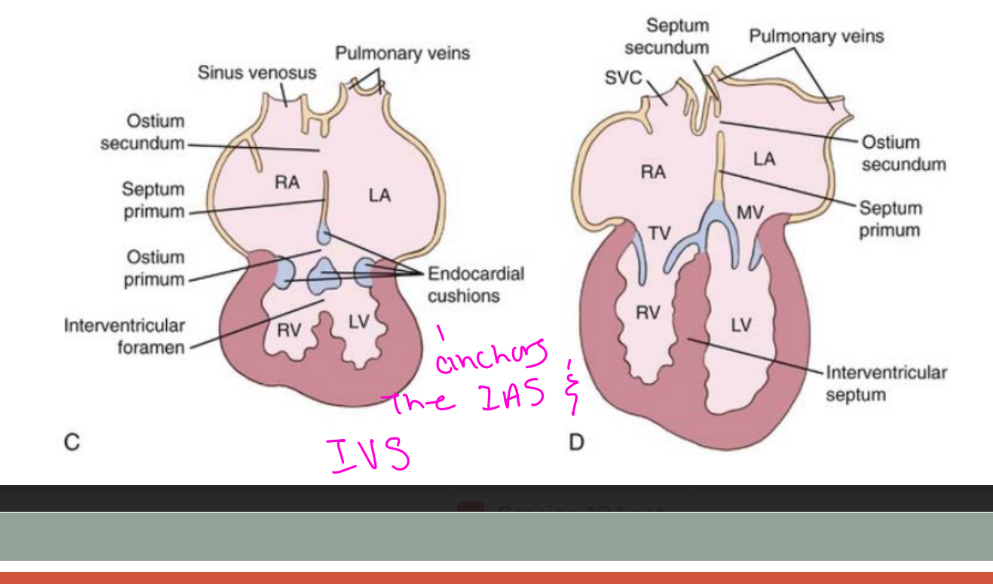
What embryologic abnormality causes an AVSD, and list the 4 structures normally formed with help from them^?
AVSDs result from abnormal development of the endocardial cushions.
The endocardial cushions help form:
Atrial septum
Ventricular septum
Septal leaflet of the tricuspid valve
Anterior leaflet of the mitral valve
List the 4 AVSD forms or subtypes.
Partial AVSD
Transitional AVSD
Complete AVSD
Incomplete AVSD

What structures are present in a partial AVSD? List 3
A partial AVSD consists of:
Primum ASD
Cleft mitral valve
It may also include a common atrium.
List the 3 main features of a transitional AVSD.
Two separate AV valve annuli
Primum ASD
Inlet VSD
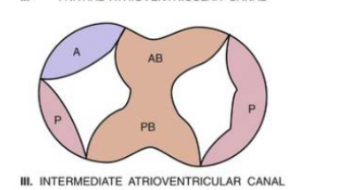
List the 4 main features of an intermediate AVSD.
A single /one AV valve annulus
The annulus is divided by tissue into right and left orifices / openings
Primum ASD
Large inlet VSD
Chat: It has one common AV valve annulus, but tissue divides it into two openings/right and left orifices.
Basically: one shared valve structure, two holes for blood to pass through.
List the 3 main components of a complete AVSD.
Primum ASD
Inlet VSD
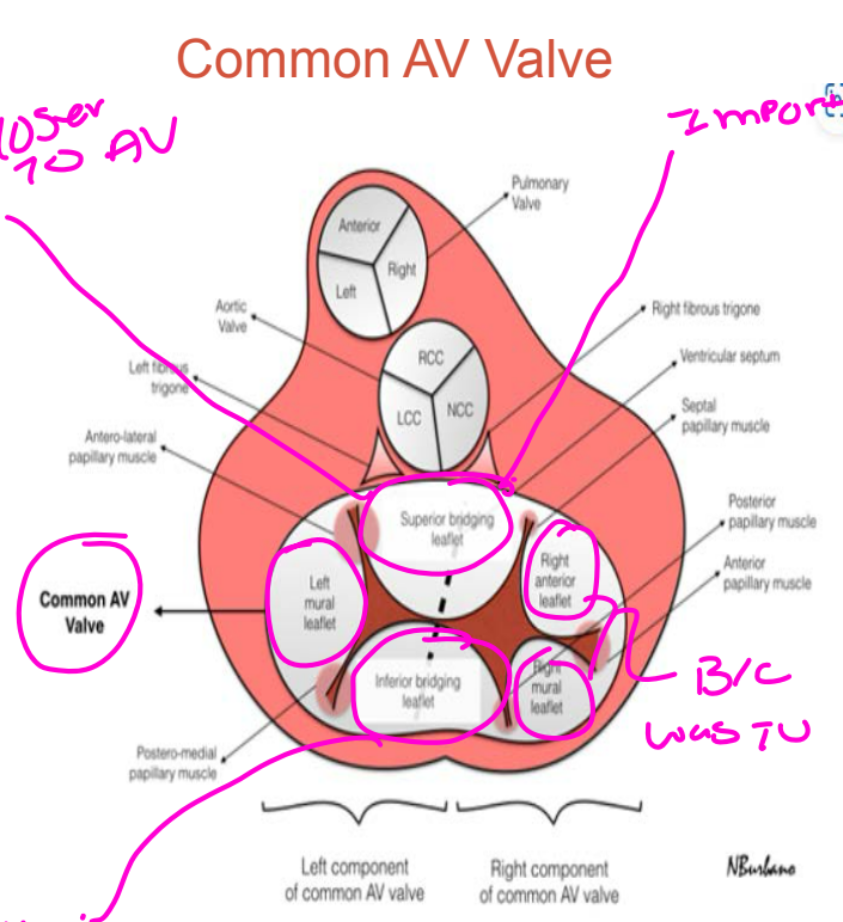
One common AV valve with 5 leaflets
List the 5 leaflets of the common AV valve.
Superior bridging leaflet
Inferior bridging leaflet
Anterior leaflet on the right side
Right lateral leaflet
Left lateral leaflet
List the 5 anatomical features shared by AVSDs.
what Level are the AV valves for all types? - what is the best view to see this?
How is the aortic valve placed?
what is the appearance of the LVOT?
How are the LV papillary muscles are rotated?
The (right ot left?) AV valve has a what component directed toward where?
The right and left AV valves insert at the same level at the cardiac crux - A4C is the best view
The aortic valve is unwedged and displaced anteriorly
The LVOT is elongated
The LV papillary muscles are rotated counterclockwise
The left AV valve component has a cleft directed toward the ventricular septum
Why do the right and left inflow-valve components insert at the same level in AVSD?
The AV septal deficiency removes the normal offset between the valves, causing both inflow-valve components to insert at the same level.

How does an AVSD produce an elongated LVOT, and what appearance does it create? Name 3 views you can see this in?
The aortic valve is unwedged and displaced anteriorly. This lengthens the LV outflow tract and produces the gooseneck appearance.
(views PLAX, LVOT, A5C) (pic A is normal, B gooseneck appearance.
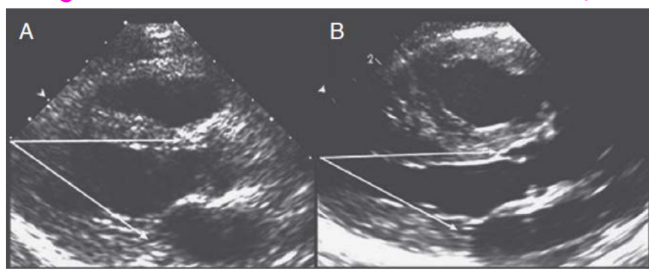
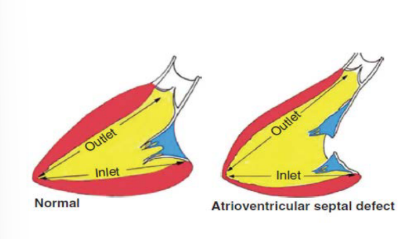
How does the relationship between the ventricular inlet and outlet differ in a normal heart versus AVSD?
In a normal heart, the inlet and outlet distances are equal. In an AVSD, the distance from the apex to the outflow tract is longer because the LVOT is elongated.
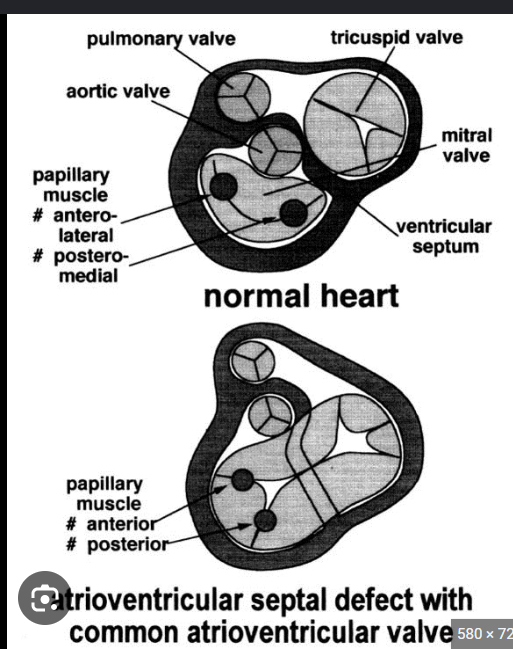
What papillary-muscle position occurs in all forms of AVSD, and what complication can it cause? what view can you see this in?
The LV papillary muscles rotate counterclockwise to approximately the 3-o’clock and 7-o’clock positions. This rotation may contribute to LVOT obstruction.
(in PSAX can see this)
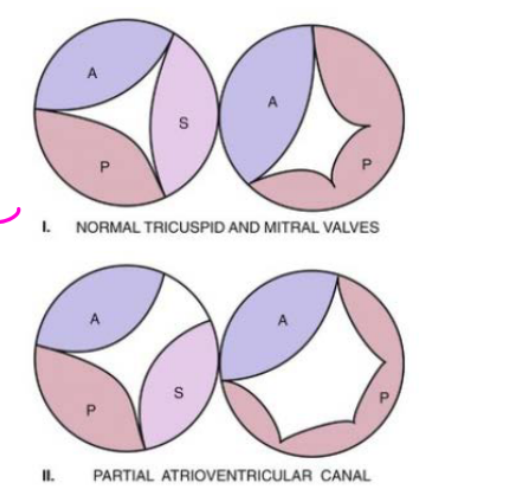
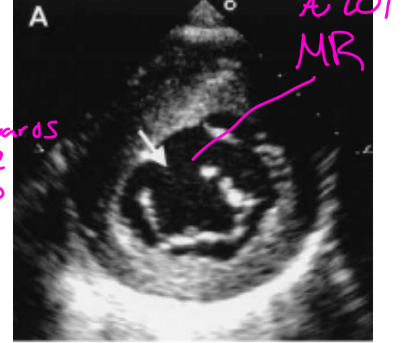
What valve abnormality is found in a partial AV canal defect, and where is the opening directed?
A cleft of the anterior mitral valve leaflet is present, and the opening is directed toward the ventricular septum.
Common Valve - Rastelli Classifications:
What do the superior bridging leaflet corresponds to?
What does the inferior bridging leaflets represent? List 2
How many leaflets does the common valve have?
The superior bridging leaflet corresponds to the anterior mitral leaflet.
The inferior bridging leaflet represents fusion of the septal tricuspid leaflet with the inferior part of the anterior mitral leaflet.
TV has 3 leaflets and MV 2 leafelts = 5 leafelts
What does the Rastelli classification evaluate?
It evaluates the superior bridging leaflet and how it attaches to the ventricular septum.
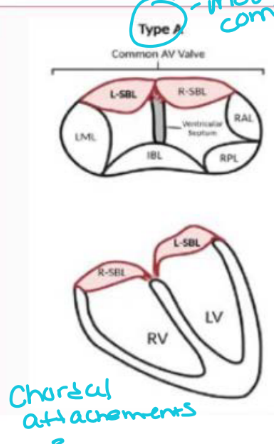
What is the best view for identifying the Rastelli classification? And which Type is the most common?
The subcostal short-axis view.
Type A is the most common
Describe Rastelli Type A.
The superior bridging leaflet is: Divided & Attached to the ventricular septum crest
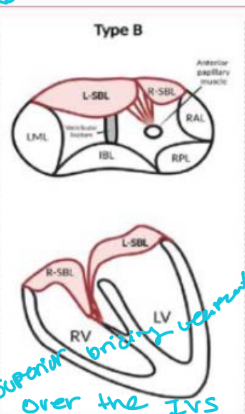
Describe Rastelli Type B.
The superior bridging leaflet is:
Partially divided
Not attached directly to the septum
Connected by chordae from superior bridging leaflet to an RV papillary muscle near the septum
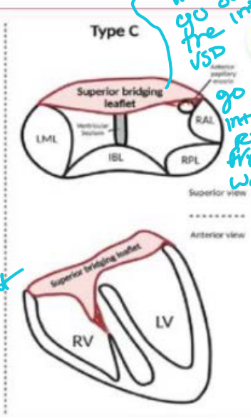
Describe Rastelli Type C.
The superior bridging leaflet is:
Undivided
Not attached to the ventricular septum
Free floating over the bridging leafelt
Attached to an RV free-wall papillary muscle
What papillary-muscle abnormality should be checked for, and with which AVSD type is it more common?
Look for a single papillary muscle, which is more common with a partial AVSD.
Why must atrial and ventricular balance be determined in AVSD?
Balance determines how what is distributed and helps decide whether the patient needs a _____-ventricle or __ - ventricular surgical repair.
Balance determines how blood flow is distributed and helps decide whether the patient needs a single-ventricle or biventricular surgical repair.
In unbalanced AVSDs which dominance is most common?
two-thirds are right dominant.
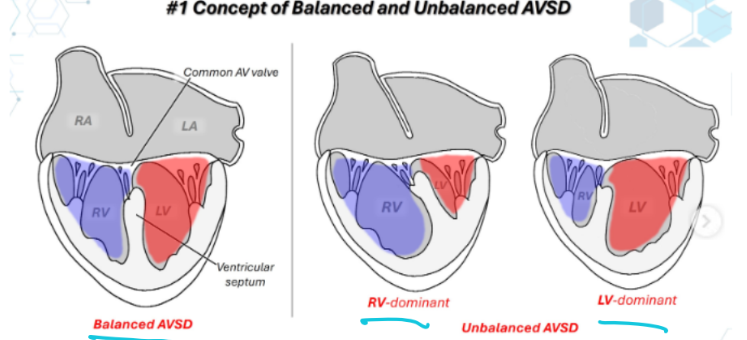
What does ventricular dominance mean in an AVSD?
The larger ventricle is called the dominant ventricle, while the opposite ventricle may be hypoplastic.
Describe an unbalanced AVSD with right-ventricular dominance.
The LV is hypoplastic, and more than half of the AV junction is committed to the RV.
List the 4 conditions commonly associated with partial and transitional AVSDs.
Persistent left superior vena cava
Pulmonary stenosis
Ellis–van Creveld syndrome
DiGeorge syndrome
List the 5 conditions commonly associated with complete and intermediate AVSDs.
LVOT obstruction
******Patent ductus arteriosus*********
Tetralogy of Fallot
Down syndrome (complete AVSD, Trisomy 21)
Double-orifice mitral valve
Explain the pathophysiology of a partial AVSD.
The cleft in the mitral valve prevents what and produces varing degrees of what?
The primum ASD causes what direction of atrial shunting?
The cleft in the mitral valve prevents complete closure and produces varying degrees of MR.
The primum ASD causes left-to-right atrial shunting.
Pathophysiology of a partial AVSD:
Together, the MR and ASD shunt create what? List 4
The combination of MR and ASD flow lead to a volume overload of
the right sided chambers
This increases the amount pulmonary blood flow and overtime
increases pulmonary vascular resistance and causes PHTN
(Dirctotic Notch flying W of pulmonary valve)
Pathophysiology for Transitional AV canal defects:
Why does a transitional AVSD behave similarly to a partial AVSD?
The inlet VSD is restrictive (small hole), so most of the shunting occurs between the atria through the primum ASD.
Explain the pathophysiology of an intermediate AVSD.
where does blood shunt across? what increases the amount of blood flow? what does the Inlet VSD add to what side of the heart causing what?
Blood shunts across the primum ASD, and MR increases the amount of blood flow. The inlet VSD also adds to the right-sided volume overload, causing dilation of the right heart.
Explain the pathophysiology of a complete AVSD.
The what valve is malformed and creating a what valve which results in varying degrees of what?
The MV is malformed and creating a common valve which results in varying degrees of MR
Explain the pathophysiology of a complete AVSD:
The primum ASD shunts blood in what direction?
The inlet VSD shunts blood from what direction?
The primum ASD shunts blood flow from left to right atrium
The inlet VSD shunts blood from the left to right ventricle
Explain the pathophysiology of a complete AVSD.
The combination of what (list 3) lead to a ____overload of the which chamber?
The combination of MR, VSD and ASD flow lead to a volume overload of the right and left chambers
Explain the pathophysiology of a complete AVSD.
What quickly leads to symptoms of congestive heart failure in early infancy?
The heavy workload on the heart and lungs to manage the excess pulmonary blood flow quickly leads to symptoms of congestive heart failure in early infancy
When do partial and transitional AVSDs usually present, and what are their symptoms similar to?
They may not present until early childhood, and their symptoms are similar to those of an ASD.
What finding can cause early congestive heart failure in partial or transitional AVSD?
Severe mitral valve regurgitation.
List the 6 clinical findings associated with intermediate and complete AVSDs.
Holosystolic murmur, Split wide Fixed S2
Congestive heart failure
Frequent respiratory infections
Poor growth and poor feeding
Tachycardia or AV block
Volume overload with pressure overload
What chest X-ray finding may occur with AVSD?
Cardiomegaly.
What ECG conduction abnormality may occur?
AV block.
How should the atrial septum, ventricular septum, and inflow valves be examined? List 4
Use careful, slow sweeps from posterior to anterior to evaluate:
Atrial septum
Ventricular septum
Inflow-valve morphology
Whether the AVSD is partial or complete
List the 5 things evaluated from the subcostal views.
and From subcostal sax determine 7
Size of the ASD and VSD
Location of the defects
Shape of the defects
Number of defects using 2D and color Doppler
IVC for estimation of RAP
From subcostal sax determine:
Number of valve leaflets and whether there is a cleft or common valve
Rastelli classification and ventricular balance
Papillary-muscle rotation, number, and attachments
List the 4 findings assessed from PLAX.
RV size and volume-overload pattern
Gooseneck deformity of the LVOT
Assess for MR
LVOTO
List the 8 findings assessed from PSAX of the ventricle level
Sweep from the base to apex to determine VSD size
Determine whether the VSD is restrictive or nonrestrictive
Evaluate inflow-valve morphology
Identify the valve cleft and its attachment to the septum
Assess mitral or left AV valve regurgitation
Determine ventricular balance
Identify papillary-muscle rotation
Evaluate the Rastelli type
List the 3 additional findings assessed at the PSAX great-vessel level.
PDA
RVOT obstruction
Tricuspid regurgitation
List the 11 assessment points from the apical four-chamber view.
Size of the ASDs
Location of the ASDs
Shape of the ASDs
Number of ASDs with 2D and color Doppler
Peak velocities and gradients
AV valve annuli inserting at the same level
Left and right inflow-valve regurgitation or stenosis
Regurgitant-volume and stenosis quantification
Pulmonary-vein PW Doppler
Balance of the atria and ventricles
RVSP & QP/QS
List the 4 findings assessed from the apical five-chamber view.
Gooseneck deformity of the LVOT
RVOT obstruction
LVOT obstruction
Peak velocities and gradients across the LVOT - to get the TVI for the QP/QS
List the 2 main differential considerations for an AV canal defect.
Single-ventricle anatomy
Other types of AV canal defects (like Partial, transitional, intermediate or complete AVSD)
List the 3 Medical Management approaches for AVSD.
Medications for heart failure
Endocarditis prophylaxis
Palliative pulmonary artery banding to reduce symptoms
What are the 2 main goals of AVSD surgery?
Close all atrial and ventricular septal defects
Create functional right and left AV valves
List the 5 surgical procedures that may be used to repair an AVSD.
Patch repair of the ASD and VSD with either 1 or 2 patches
Suture repair of the valve
Division of the common leaflet
Inflow-valve replacement when severe stenosis or regurgitation is present
Resection of a subaortic obstruction
Post OP Echo Investigation:
List the 6 things that should be evaluated after AVSD repair.
Residual ASD shunting
Residual VSD shunting, including direction and gradients
AV valve function and regurgitation
AV valve stenosis
Systolic and diastolic ventricular function
RVSP and possible subaortic stenosis
Compare the 4 AVSD types by their main anatomical components.
Partial: Primum ASD and cleft mitral valve
Transitional: Primum ASD, restrictive inlet VSD, and 2 separate AV valve annuli
Intermediate: Primum ASD, large inlet VSD, and one annulus divided into right and left openings
Complete: Primum ASD, inlet VSD, and one common 5-leaflet AV valve