CSD 318 Craniofacial Anomalies
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
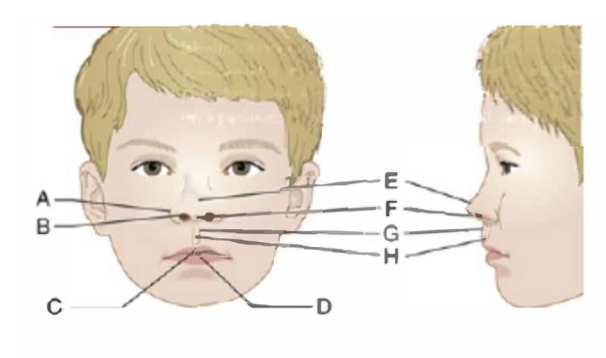
label a, b, c, d in order
ala base, ala rim, cupid’s bow, tubercle
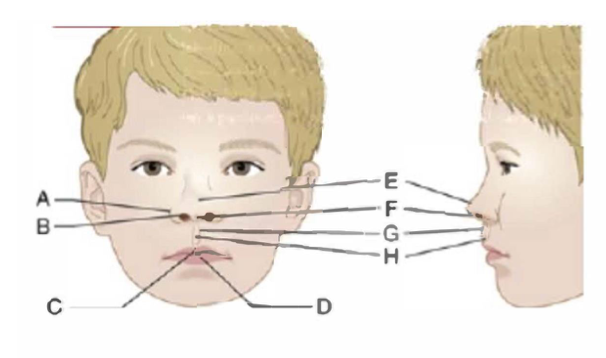
label e, f, g, h in order
nasal tip, columella, philtral ridges, philtrum
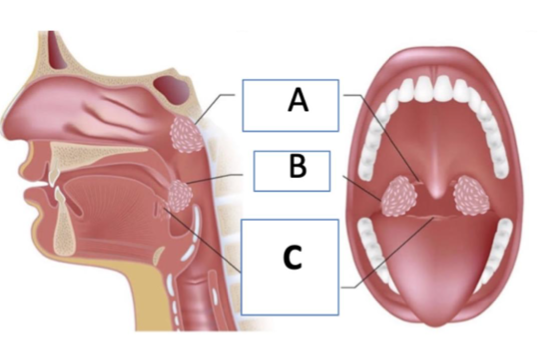
label a, b, c in order
adenoid/pharyngeal tonsil, palatine tonsil, lingual tonsil
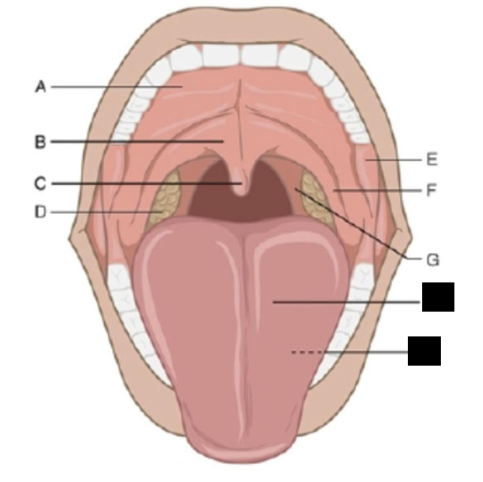
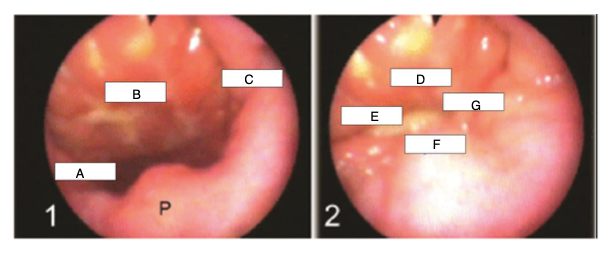
label a, b, c, d in order
hard palate, velum, uvula, palatine tonsil
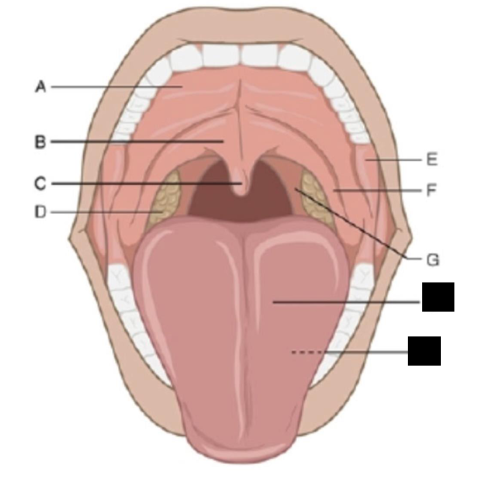
label e, f, g in order
alveolar ridge, anterior faucial pillar, posterior faucial pillar
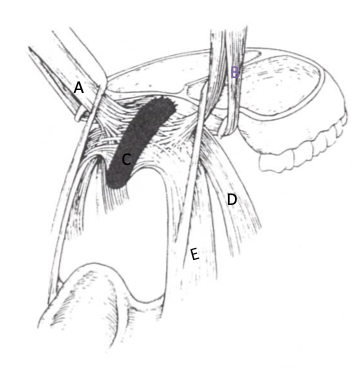
label a, b, c in order
levator veli palatine (LVP)
tensor veli palatine
musculus uvulae
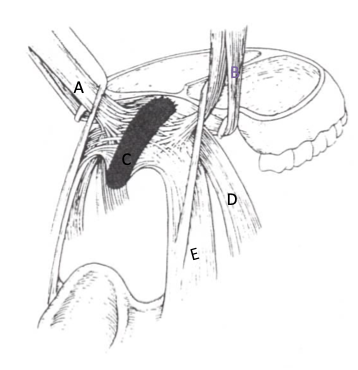
label d, e
palatoglossus
palatopharyngeus
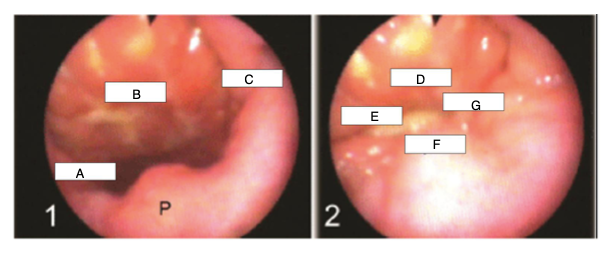
label a, b, c in order
lateral pharyngeal wall
posterior pharyngeal wall
lateral pharyngeal wall
label d, e, f, g in order
posterior pharyngeal wall
lateral pharyngeal wall
velum
lateral pharyngeal wall
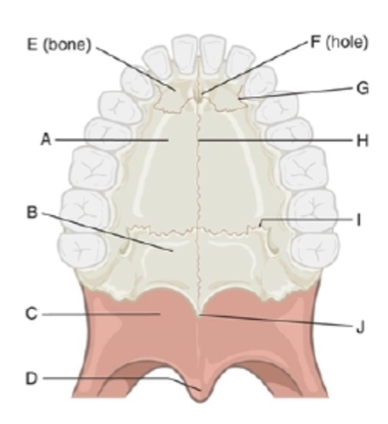
label a, b, c, d, e in order
palatine process of maxilla
palatine bone
velum
uvula
premaxilla
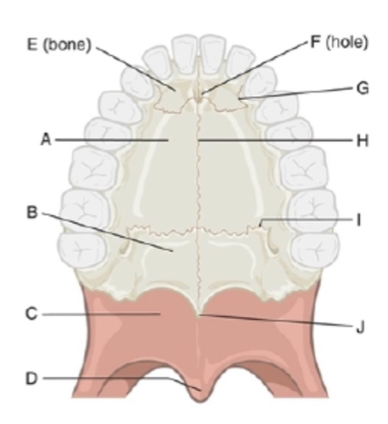
label f, g, h, i, j in order
incisive foramen
incisive suture
median palatine suture
transverse palatine suture
posterior nasal spine

label blue, yellow, and green areas in order
nasal cavity
pharynx
oral cavity
velar aponeurosis
insertion point for velar muscles
adenoids
pharyngeal tonsils
assist with VP closure due to location on posterior pharyngeal wall
apraxia
can cause velopharyngeal incompetence because it is a neurological disorder
mixed resonance can result from this
palatine tonsil
contain lymphoid tissue and assist in fighting infection particularly from 0-2
prone to hypertrophy in young children
atrophy almost completely by age 16
teratogen
any agent that can cause birth defects or developmental abnormalities
primary palate
upper lip, premaxilla, and front of hard palate
secondary palate
hard and soft palate
obligatory errors
child is using incorrect placement, attempting VP closure, and otherwise doing things correctly but the sound is not right
an unrepaired cleft can cause hypernasality, weak oral pressure, nasal emissions, /s/ distortions
speech therapy will not help, surgery is needed
compensatory errors
due to compensation for abnormal VP oral structure
if the structure has been repaired, therapy can help. if surgery is delayed, treatment can help with placement but surgery is recommended
hypernasality
too much resonance in the nasal cavity
hyponasality
too little resonance in nasal cavity due to a nasal blockage or inability to open VP on nasal sounds
cul-de-sac resonance (oral, nasal, & pharyngeal)
a “blocked” sound, as if something is taking up too much of the oral/nasal cavity or pharynx (often related to large tonsils)
mixed resonance
a combination of two or more other types of resonances
velopharyngeal mislearning
VP has appropriate structure and ability to function typically, but speaker is using VP in an atypical way
compensatory errors become this after a repair
therapy can help
direct instrumental procedures
provide direct visualization of the structures of the velopharyngeal valve during speech
includes videofluoroscopy and nasopharyngoscopy
important to determine the cause and location of VPI
indirect instrumental procedures
give objective information regarding physical correlates of velopharyngeal function (acoustics, airflow, and air pressure)
includes nasometry and aerodynamics
important for pre and post objective measures of resonance and speech
nasometry
measures acoustic correlates of resonance and nasal emission to infer VP function
nasalance score = nasal acoustic energy/total acoustic energy
fiberoptic endoscopy evaluation of swallowing (FEES)
like a nasopharyngoscopy but instead of speech you are viewing swallowing
videofluoroscopy
radiological technique used to obtain real-time moving images of internal structures
to visualize speech and/or swallowing
can see entire length of velum and depth of pharyngeal wall
speech aerodynamics
use equipment to measure airflow and air pressure through nose during speech
infer VP opening size or obstruction (more pressure = smaller opening)
nasopharyngoscopy
direct visual observation and analysis of the velopharyngeal mechanism during speech
only view that can see the nasal surface of the velum
same thing as a laryngoscopy (light source, flexible fiberoptic endoscope)
auditory feedback/biofeedback
motor learning
acquisition of motor skills to execute complex motor movements and sequences
results in development or change or refinement of speech sound production
(playing an instrument, sport, performing dance steps)
motor memory
develops automaticity of newly learned movements
dependent on constant repetition
makes new learning relatively permanent
torus palatinus
prominent longitudinal ride on oral surface along median palatine raphe/suture
normal variation and usually does not cause problems
passavant’s ridge
bulge or ride that can form on the PPW during speech and swalloging
describe the jobs of the main muscles of velopharyngeal opening/closure as well as the tensor veli palatini
levator veli palatini: velar sling, primary muscle of velar elevation, pulls velum up and back to seal off nasopharynx
superior constrictor: constricts lateral and posterior pharyngeal walls against velum to close VP complex
palatopharyngeus: pull LPWs medially and upward for VP closure/narrowing
palatoglossus: main antagonist to LVP, depresses velum for nasal consonants and can elevate tongue
musculus uvulae: bulges to assist with closure of nasopharynx
tensor veli palatini: opens eustachian tube for middle ear drainage
describe the pneumatic vs nonpneumatic activities of the VP
pneumatic involve actions that create air pressure (blowing or whistling)
non-pneumatic activities do not create pressure (sucking or swallowing)
describe how timing, height, and firmness of VP closure varies according to activity and why
valve closes before phonation begins or sound will be hypernasal; closure is maintained until nasal consonant or utterance is ended
closure contact may vary with different sounds; closure is higher and tighter with high pressure consonants, especially voiceless consonants; closure can be affected by rate and change
varies with consonant; gap of 5 mm is threshold for hypernasality; even very small gaps can cause audible nasal air emission
describe and define resonance and articulation
sound quality is affected by changes in sizes of the pharynx and oral cavity which is caused by velopharyngeal opening/closure (vowels)
moving of the articulators to produce different speech sounds (consonants)
describe VP function for nasal vs non-nasal sounds (be able to hypothesize different speech sounds from pictures of the pharynx, oral, and nasal cavities)
closes off the nasal cavity from the oral cavity to regulate and direct transmission of sound energy and airflow in the oral and nasal cavities
oral sounds: valve is closed, allowing acoustic energy to enter oral cavity. important for most consonants and all vowels
nasal sounds: valve is open, allowing most acoustic energy to enter nasal cavity, important for n, m, and ng
main endogenous and exogenous factors that can cause clefts
endogenous: syndromes, chromosomal disorders, genetic disorders
exogenous: drugs, viruses, teratogens, nutritional deficiencies, mechanical interference
when do the primary and secondary palate begin to develop and close
primary: 6-8 weeks
secondary: 9-12 weeks
describe the pattern of closure of the primary and secondary palate
primary: forward to form the alveolar ridge and then the lip
secondary: backward to form the hard palate and the velum
state the structural and functional effects of clefts of the primary palate
gap in the lip/upper gum
can cause difficulties with feeding, speech, hearing, and dental development
compare an overt vs occult submucous cleft
overt clefts are visible, often presenting with a bifid uvula, notch, and zona pellucida
occult submucuous clefts lack readily observable signs
describe the functional consequences of a submucous cleft
underlying muscles do not fully fuse even though surface looks normal
impacts speech, feeding, and hearing
describe the prevalence of cleft lip/palate generally
about 1 in 700
describe the unique characteristics of infant feeding anatomy
tongue fills the mouth, sucking pads, smaller mandible, epiglottis and velum touch, higher larynx, narrow vertical epiglottis
indicate the importance of suck-swallow-breathe coordination in feeding
this coordination is important so they can feed continuously
disrupted coordination can cause fatigue, poor intake, airway compromise, oxygen desaturation, negative feeding experiences, and distress
how are breast and bottle feeding impacted by cleft palate and why it’s less likely to be impacted by cleft lip
cleft palate causes difficulty with creating negative pressure which is needed for sucking
cleft lip may cause difficulty creating a seal, but this is more easily remedied through angles and types of bottles
describe resonance and articulation and how they interact with airflow
resonance refers to the amplification and modification of sound waves by the vocal tract
articulation involves shaping the sound waves into specific sounds
how is resonance typically adjusted or changed
compare velopharyngeal insufficiency, dysfunction, incompetence, and mislearning
dysfunction is any abnormal function of the velum
insufficiency is an anatomical or structural defect that prevents adequate VP closure by causing the velum to be short relative to the PPW
incompetence is a neuromotor problem resulting in poor movement of VP structure
mislearning is inadequate VP closure due to faulty learning of appropriate articulation patterns
describe the effects of VPI on resonance and speech
disrupts normal speech resonance and articulation by causing an opening between the nasal and oral cavity
list and describe the types of nasal emissions
inaudible: large VP gap, short utterance length, weak or omitted consonants
audible: small VP gap, air burst through nose on unvoiced pressure consonant sounds (consistent)
nasal rustle: small/tiny VP gap, rustling sound through nose on unvoiced pressure consonant sounds (inconsistent)
phoneme specific: mislearning
justify why an orofacial examination is important to an evaluation
determine if there are structural anomalies that could indicate a craniofacial syndrome
determine the cause of what you hear (obligatory, compensatory, or mislearning)
determine whether further assessment is needed if you are unsure about the cause
describe the basic components of an orofacial examination
examine the tongue, palatine tonsils, velum/uvula, alveolar ridge, hard palate, teeth
evaluating for hypertrophic tonsils, clefting of the hard palate, fistulas, missing teeth, malocclusions, median raphe, consistent pinkish color of the velum
how does surgery for VPI differ from palate and lip repairs? when does each take place?
lip (2-6 months) and palate repair (10-12 months): goal is to optimize facial, oral, and palate structures to facilitate feeding, speech, dentition, facial profile, and aesthetics
describe VP function: velum
moves in a superior and posterior direction
has a type of “knee action”
moves toward the posterior pharyngeal wall
describe vp function: lateral pharyngeal wall
moves medially
usually close against the velum
sometimes close in midline behind velum
describe VP function: posterior pharyngeal walls
moves anteriorly toward the velum
Passavant’s ridge is a bulge of muscle seen here
describe the connection between eustachian tube and velopharynx and differences in kids vs adults
connect middle ear to pharynx and is horizontal in children under 6
(45 degree angle in adults)
Pierre Robin Sequence
caused by genetic factors, in utero constriction leads to mechanical changes to the orofacial structure, medication exposures
associated with difficulty breathing and feeding, cleft palate, hearing probelms, and orthodontic difficulties (small lower jaw and overcrowding teeth)
Treacher Collin’s Syndrome
due to gene alteration
associated with unique facial features (bones of skull join together prematurely), cleft palate, hearing loss, breathing difficulties