Esophagus Disorders
1/25
Earn XP
Description and Tags
These flashcards cover the anatomy and evaluation of esophageal diseases, focusing on key concepts such as layers of the esophagus, innervation, clinical signs, diagnostic methods, and complications.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
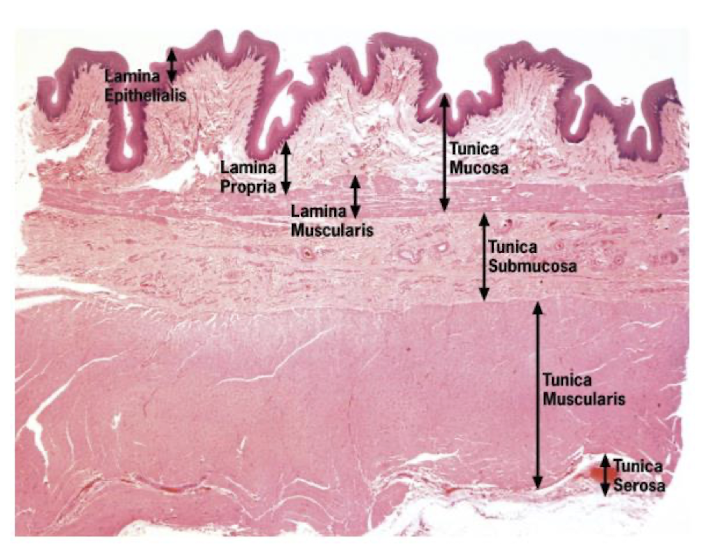
What are the four layers that compose the wall of the esophagus?
Tunica mucosa
Tunica submucosa
Tunica muscularis
Tunica adventitia/serosa
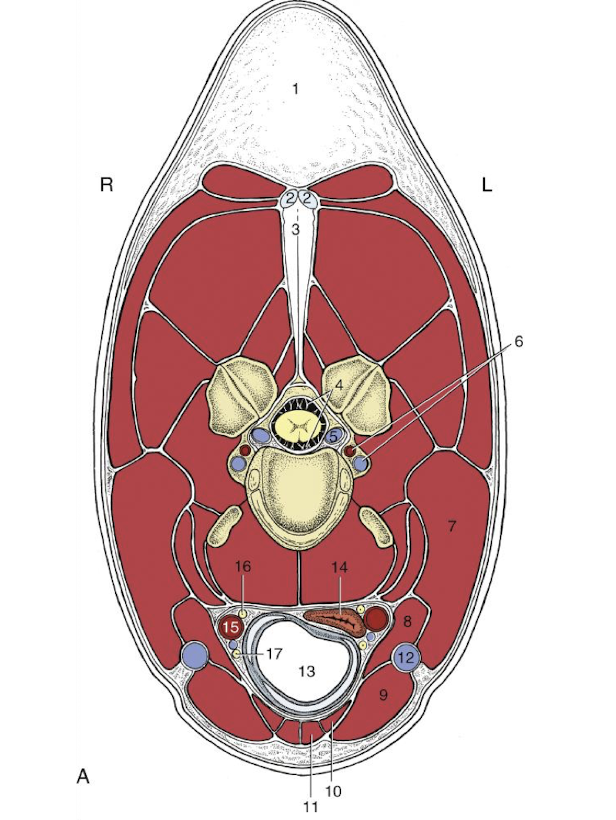
Important anatomical structures in the neck
jugular vein
trachea
common carotid artery
vago-sympathetic trunk
recurrent laryngeal nerve
Which cranial nerves are involved in the innervation of the esophagus? blood supply?
Cranial nerves IX and X, sympathetic trunk. mesenteric ganglion cells
Cervical corotid a, thoracic/abdominal part of bronchoesophageal and gastric a
What clinical sign indicates the potential for esophageal disease during a physical examination?
Ptyalism, dysphagia, coughing, or regurgitation of food.
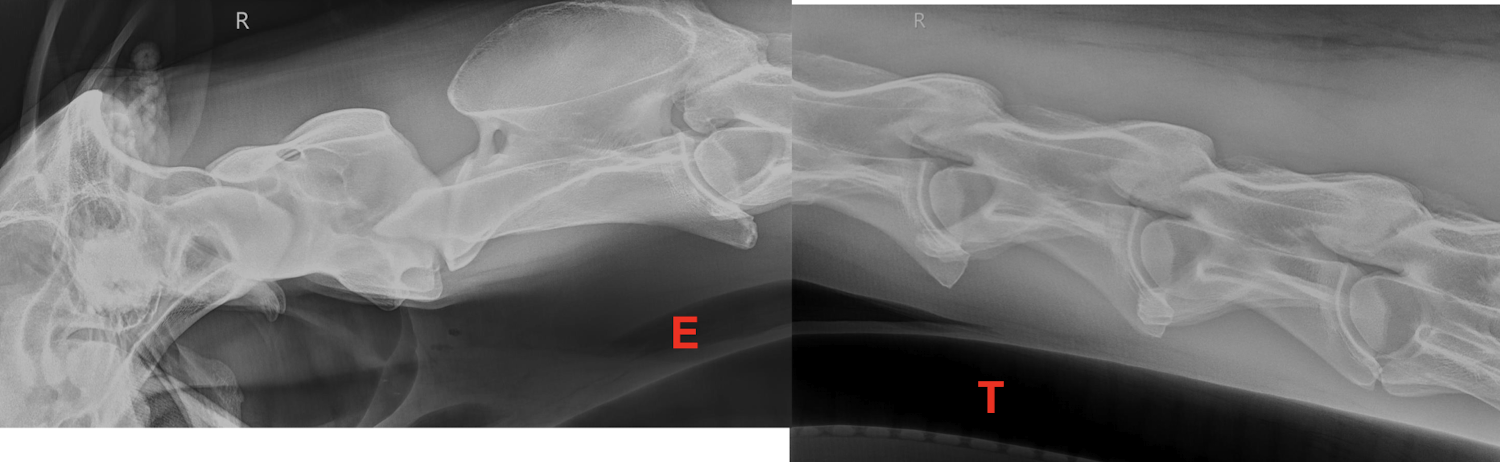
Normal imaging of the neck
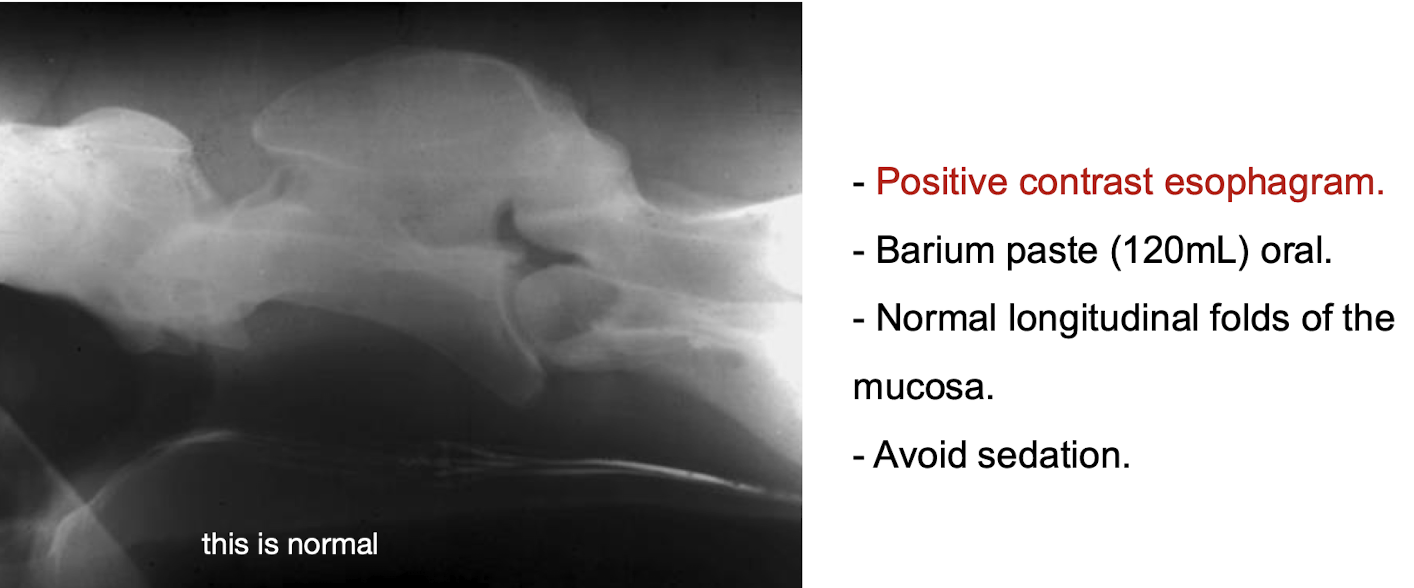
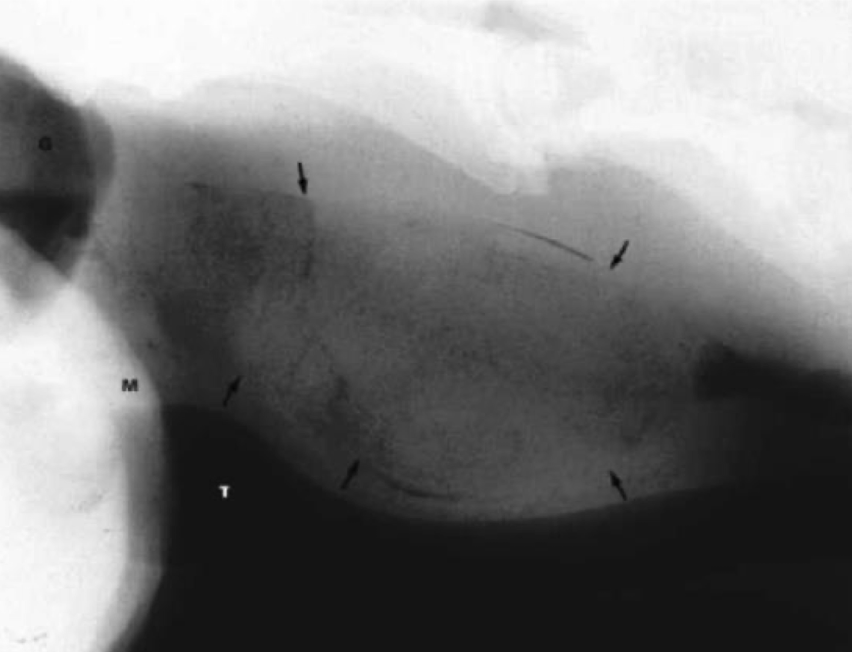
What is the purpose of performing a positive contrast esophagram?
To evaluate for esophageal obstructions, strictures, and other lesions.
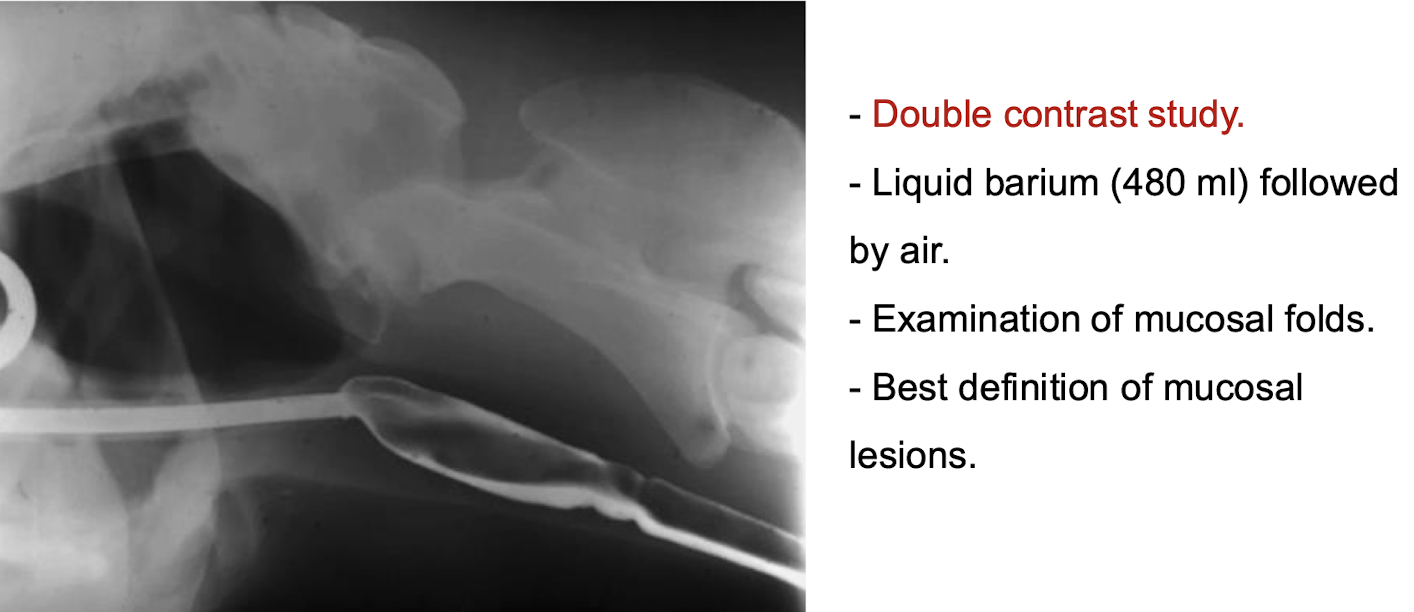
Double contrast study
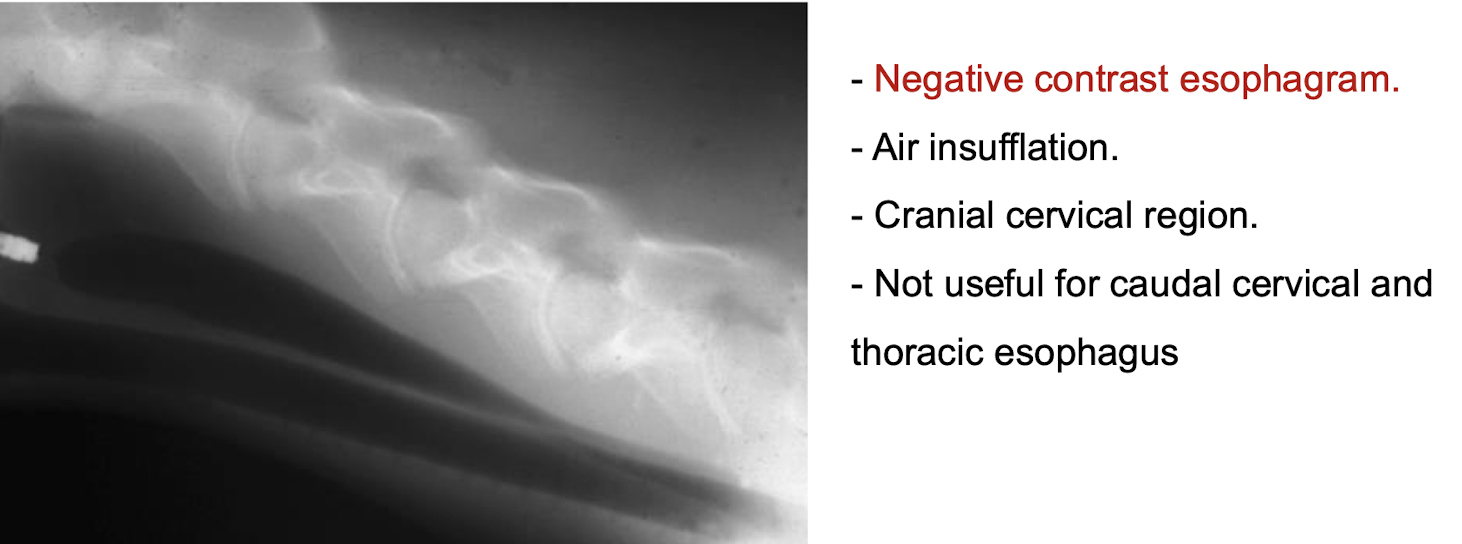
Negative contrast study
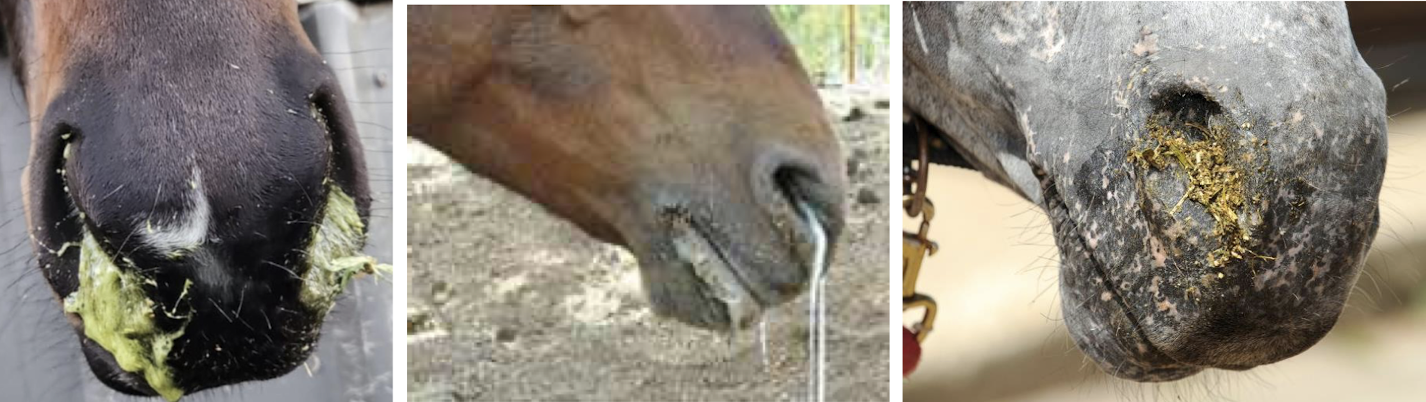
What is the primary clinical sign of impaction or choke in horses?
Ptyalism or excessive salivation.
Where do we start the endoscopy procedure?
Start all the way down in the stomach and look cranially

What part of the esophagus is this?
Proximal

What part of the esophagus is this?
Cervical
What is choke in horses?
Food becomes lodged in the esophagus, causing obstruction and discomfort leads to ptyalism, dysphagia, coughing, regurge of food, water and saliva from mouth and nostrils
odynohphagis → painful swallowing
repeated extension of the head and neck
distress, agitation
can lead to anorexia, electrolyte imbalance, dehydration, aspiration pneumonia (clinical signs occur 1 day after the choke)
Treatment for choke in horses
often involves sedation to keep head down, passing a nasogastric tube to relieve the obstruction DO NOT PUSH, and providing supportive care such as fluids and monitoring for complications
others
cuffed endotracheal tube → lavage under pressure → external massage → endoscopic basket
muzzle the horse → stall without bedding → off feed/water
surgical treatment with esophagotomy
ace, oxytocin, n-butylscopolammonium bromide, esophageal instillation of lidocaine for esophageal relaxation
Treatments for issues that arise from choke: Dehydration, Hyponatremia, Hypochloremia, Hypopotassemia, Metabolic alkalosis
polyionic fluids
broad spectrum antibiotics
NSAIDs be careful
Sucralfate
keep off food for 24-48h → slowly introduce pelleted mash food, hay can be given after 21 days
Prognosis for choke
Rate of reobstruction – 37%
Prognosis for survival – 78-88%
- Horses may require permanent diet changes
What damages can we see from chronic choke?
pharyngeal inflammation
mucosal bruising
mucosa stripped off submucosa
stricture
ruptured esophagus
periesophageal abscess
fistula
esophageal diverticulum
What are the three types of esophageal strictures based on anatomical location?
Type I - mural lesions → adventitia and muscularis
Type II - esophageal rings or webs → mucosa and submucosa
Type III - annular stenosis → all layers
Medical management for esophageal stricture
Balloon dilation → not so common in LA
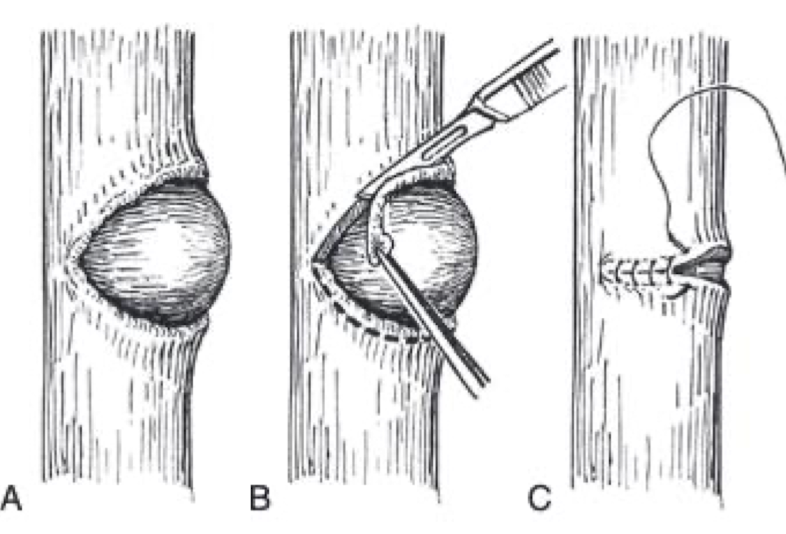
Surgical treatment for esophageal stricture
- Esophagomyotomy → for type 1
- Partial/complete resection and anastomosis
- Creation of a traction diverticulum
- Patch grafting
- Esophagostomy
What is one complication that can follow esophageal obstruction?
Aspiration pneumonia → make sure to sedate the horse so they drop their head to prevent further aspiration
Clinical signs of esophageal rupture
- Discomfort, depressed
- Head/Cervical swelling
- Subcutaneous emphysema – swallowed air escapes
- Cellulitis
Treatment for esophageal rupture
establish drainage
surgical repair within 12 hrs
drain needs to be place
second intension healing
antibiotics, anti-inflammatories, fluid therapy
What can esophageal rupture lead to?
- Mediastinitis, pleuritis, septicemia
- Horner’s syndrome, laryngeal hemiplegia
- Jugular thrombosis, carotid rupture
What are the two types of diverticula mentioned in the notes?
A. Traction (true) diverticulum → acquired from contraction of the periesophageal scar tissue, causes outward rotation and tenting of all layers. develops from esophagostomy, second intention healing sites. thicker neck
B. Pulsion (false) diverticulum → protrusion of mucosa and submucosa through a defect in the esophageal muscularis. has a thinner neck. poorer prognosis and will require surgery
What is the recommended treatment in cases of pulsing diverticulum?
Surgery is indicated due to the risk of obstruction and rupture → diverticulectomy, mucosa inversion preferred