DeepSeek NAPLEX Questions (Oncology)
1/294
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
295 Terms
Which parameter is most commonly used to dose chemotherapy drugs?
A) Body weight (kg)
B) Body mass index (BMI)
C) Body surface area (BSA)
D) Ideal body weight (IBW)
Solution: C) Body surface area (BSA)
Rationale: The underlined text states "Most chemotherapy is dosed using body surface area (BSA)."
Which chemotherapy drug is an exception to BSA-based dosing?
A) Cisplatin
B) Paclitaxel
C) Carboplatin
D) Doxorubicin
Solution: C) Carboplatin
Rationale: The underlined text specifically notes carboplatin as the exception, using the Calvert formula instead.
When calculating BSA for chemotherapy dosing, which weight should typically be used?
A) Ideal body weight
B) Adjusted body weight
C) Actual body weight
D) Lean body weight
Solution: C) Actual body weight
Rationale: The underlined instruction states to "use the patient's actual body weight for dose calculations, unless instructed otherwise."
A patient is 170 cm tall and weighs 75 kg. Using the Mosteller equation, what is their BSA?
A) 1.72 m²
B) 1.85 m²
C) 1.92 m²
D) 2.01 m²
Solution: B) 1.85 m²
Rationale: Using the Mosteller equation: √[(170 × 75)/3600] = 1.85 m².
Which of the following is the correct Mosteller equation for BSA calculation?
A) √(height in cm × weight in kg / 3600)
B) (height in cm + weight in kg) / 100
C) 0.007184 × (height in cm)^0.725 × (weight in kg)^0.425
D) Weight in kg / (height in m)²
Solution: A) √(height in cm × weight in kg / 3600)
Rationale: This matches the Mosteller equation shown in the image.
Besides Mosteller, which other BSA equation is commonly used in oncology?
A) Cockcroft-Gault
B) Du Bois and Du Bois
C) Schwartz
D) MDRD
Solution: B) Du Bois and Du Bois
Rationale: The underlined text mentions "Du Bois and Du Bois" as another commonly used equation.
A 60-year-old female (height 160 cm, weight 90 kg) is to receive cyclophosphamide. Which weight should be used for her BSA calculation?
A) 60 kg (ideal body weight)
B) 75 kg (adjusted body weight)
C) 90 kg (actual body weight)
D) 100 kg (dosing weight)
Solution: C) 90 kg (actual body weight)
Rationale: The underlined text specifies using actual body weight unless instructed otherwise.
What is required to calculate a carboplatin dose using the Calvert formula?
A) BSA and serum creatinine
B) Creatinine clearance and target AUC
C) Liver function tests
D) Platelet count
Solution: B) Creatinine clearance and target AUC
Rationale: While not shown, this tests knowledge that the Calvert formula uses CrCl and AUC (implied by the exception note).
For BSA calculation, how should a patient's height of 5 feet 7 inches be converted?
A) 57 cm
B) 157 cm
C) 170 cm
D) 175 cm
Solution: C) 170 cm
Rationale: 5'7" = 67 inches × 2.54 cm/inch = 170 cm (tests ability to convert units for the Mosteller equation).
Using the Mosteller equation, what is the BSA for a patient who is 180 cm and 72 kg?
A) 1.65 m²
B) 1.80 m²
C) 1.89 m²
D) 1.95 m²
Solution: C) 1.89 m²
Rationale: √[(180 × 72)/3600] = 1.89 m² (tests calculation skills).
A patient with a creatinine clearance (CrCl) of 80 mL/min is prescribed carboplatin with a target AUC of 5. What is the total dose (mg) using the Calvert formula?
A) 325 mg
B) 425 mg
C) 525 mg
D) 625 mg
Solution: C) 525 mg
Calculation:
Formula:
Dose (mg) = Target AUC × (GFR + 25)
5 × (80 + 25) = 5 × 105 = 525 mg
A patient with CrCl of 40 mL/min needs carboplatin with a target AUC of 4. Calculate the dose.
A) 180 mg
B) 260 mg
C) 340 mg
D) 420 mg
Solution: B) 260 mg
Calculation:
4 × (40 + 25) = 4 × 65 = 260 mg
For a patient with CrCl 120 mL/min and target AUC of 6, what is the carboplatin dose?
A) 720 mg
B) 870 mg
C) 960 mg
D) 1,020 mg
Solution: B) 870 mg
Calculation:
6 × (120 + 25) = 6 × 145 = 870 mg
A frail elderly patient has CrCl 30 mL/min and requires a reduced target AUC of 2. What is the appropriate carboplatin dose?
A) 55 mg
B) 110 mg
C) 165 mg
D) 220 mg
Solution: B) 110 mg
Calculation:
2 × (30 + 25) = 2 × 55 = 110 mg
A 65-year-old male (weight 70 kg, Scr 1.2 mg/dL) is prescribed carboplatin with AUC 5. Calculate his dose using the Calvert formula.
A) 385 mg
B) 429 mg
C) 512 mg
D) 575 mg
Solution: B) 429 mg
Calculation:
5 × (60.8 + 25) ≈ 5 × 85.8 = 429 mg
For CrCl 47 mL/min and AUC 4.5, what is the carboplatin dose (round to nearest 10 mg)?
A) 310 mg
B) 320 mg
C) 330 mg
D) 340 mg
Solution: B) 320 mg
Calculation:
4.5 × (47 + 25) = 4.5 × 72 = 324 → 320 mg (rounded)
A 12-year-old (CrCl 110 mL/min/1.73m², BSA 1.5 m²) needs carboplatin with AUC 5. What is the dose?
A) 575 mg
B) 675 mg
C) 750 mg
D) 825 mg
Solution: B) 675 mg
Calculation:
5 × (110 + 25) = 5 × 135 = 675 mg
If a patient’s calculated carboplatin dose is 1,200 mg but the institutional maximum is 1,000 mg, which action is appropriate?
A) Administer 1,200 mg
B) Administer 1,000 mg
C) Hold the dose
D) Switch to cisplatin
Solution: B) Administer 1,000 mg
Rationale: Institutional maximums override calculated doses to ensure safety.
Alkylating agents like cyclophosphamide exert their cytotoxic effects primarily by:
A) Inhibiting topoisomerase II
B) Cross-linking DNA strands
C) Blocking microtubule assembly
D) Interrupting RNA synthesis
Solution: B) Cross-linking DNA strands
Rationale: The underlined text states alkylating agents work by "cross-linking DNA strands," disrupting DNA replication.
Which toxic metabolite of cyclophosphamide causes hemorrhagic cystitis?
A) Acrolein
B) Phosphoramide mustard
C) 4-Hydroxycyclophosphamide
D) Carboxyphosphamide
Solution: A) Acrolein
Rationale: The table explicitly links "hemorrhagic cystitis" to "toxic metabolite acrolein."
A patient receiving high-dose cyclophosphamide should be monitored for hemorrhagic cystitis using:
A) Serum creatinine
B) Hematuria, Urinalysis for RBCs
C) Liver function tests
D) Platelet count
Solution: B) Hematuria, Urinalysis for RBCs
Rationale: The table lists "urinalysis (for RBCs)" and lower urinary tract symptoms as monitoring parameters.
Mesna is required for all doses of ifosfamide and cyclophosphamide doses above:
A) 0.5 g/m²
B) 1.0 g/m²
C) 1.8 g/m²
D) 2.5 g/m²
Solution: C) 1.8 g/m²
Rationale: The table specifies mesna is needed for cyclophosphamide doses ">1.8 g/m²" and all ifosfamide doses.
A patient on busulfan develops progressive dyspnea and dry cough. Which toxicity is most likely?
A) Pulmonary fibrosis
B) Hemorrhagic cystitis
C) Neurotoxicity
D) Hepatotoxicity
Solution: A) Pulmonary fibrosis
Rationale: The table lists "pulmonary toxicity (e.g., pulmonary fibrosis)" for busulfan.
The carmustine wafer implant is associated with which unique toxicity?
A) Hemorrhagic cystitis
B) Cerebral edema/seizures
C) Pancreatitis
D) Cardiotoxicity
Solution: B) Cerebral edema/seizures
Rationale: The table highlights "neurotoxicity (e.g., seizures, cerebral edema)" with the wafer implant.
Which intervention prevents cyclophosphamide-induced hemorrhagic cystitis?
A) Allopurinol
B) Adequate hydration
C) Potassium supplementation
D) Folic acid
Solution: B) Adequate hydration
Rationale: The table lists "adequate hydration" as a preventive measure under "Management."
Which toxicity is shared by both busulfan and carmustine?
A) Hemorrhagic cystitis
B) Pulmonary fibrosis
C) Neurotoxicity
D) Hepatotoxicity
Solution: B) Pulmonary fibrosis
Rationale: Both drugs list "pulmonary toxicity (e.g., pulmonary fibrosis)" in the table.
A patient on cyclophosphamide reports urinary urgency and dysuria. Which condition should be suspected?
A) UTI
B) Hemorrhagic cystitis
C) Nephrotoxicity
D) Hypercalcemia
Solution: B) Hemorrhagic cystitis
Rationale: The table lists "lower urinary tract symptoms (e.g., urinary urgency, dysuria)" as monitoring indicators.
Platinum-based compounds like cisplatin exert their cytotoxic effects primarily by:
A) Inhibiting topoisomerase I
B) Cross-linking DNA strands
C) Blocking purine synthesis
D) Disrupting microtubule function
Solution: B) Cross-linking DNA strands
Rationale: The underlined header states these agents "cross-link DNA," interfering with replication.
A patient develops dyspnea and urticaria during cisplatin infusion. Which is the most appropriate immediate action?
A) Slow the infusion rate
B) Administer diphenhydramine and continue infusion
C) Stop infusion and give epinephrine
D) Switch to carboplatin
Solution: C) Stop infusion and give epinephrine
Rationale: The table lists "dyspnea, angioedema, urticaria" as signs of hypersensitivity requiring emergency treatment.
Which intervention reduces cisplatin-induced cumulative renal toxicity?
A) Mesna
B) Amifostine (Ethyol)
C) Leucovorin
D) Dexrazoxane
Solution: B) Amifostine (Ethyol)
Rationale: The table specifies amifostine as a "chemoprotectant that reduces cumulative renal toxicity."
Which baseline assessment is critical before initiating cisplatin?
A) Audiogram
B) Echocardiogram
C) Pulmonary function test
D) Liver biopsy
Solution: A) Audiogram
Rationale: The table lists "audiogram at baseline" for ototoxicity monitoring.
Which electrolytes require monitoring with cisplatin? (Select ALL that apply.)
A) Magnesium
B) Calcium
C) Potassium
D) Phosphorus
Solution: A) Magnesium, B) Calcium, C) Potassium
Rationale: The table specifies monitoring "Mg, K, Na, Ca" (sodium not listed in options).
A patient starting oxaliplatin should avoid:
A) Hot beverages
B) Cold temperatures
C) High-fat meals
D) Sun exposure
Solution: B) Cold temperatures
Rationale: The underlined text states to "avoid cold exposure" to prevent acute sensory neuropathy.
What is the maximum recommended cisplatin dose per cycle to reduce toxicity?
A) 50 mg/m²
B) 75 mg/m²
C) 100 mg/m²
D) 120 mg/m²
Solution: C) 100 mg/m²
Rationale: The table specifies to "limit cisplatin dose per cycle to ≤100 mg/m²."
Which symptom suggests oxaliplatin-induced acute sensory neuropathy?
A) Abnormal sensations
B) Blurred vision
C) Hearing loss
D) Tremors
Solution: A) Abnormal sensations
Adequate hydration is essential with cisplatin primarily to prevent:
A) Neurotoxicity
B) Nephrotoxicity
C) Ototoxicity
D) Myelosuppression
Solution: B) Nephrotoxicity
Rationale: Hydration is listed under "Management" for nephrotoxicity prevention.
Which platinum agent is most associated with acute cold-induced neuropathy?
A) Cisplatin
B) Carboplatin
C) Oxaliplatin
D) Nedaplatin
Solution: C) Oxaliplatin
Rationale: The underlined text specifically links cold-induced neuropathy to oxaliplatin.
Which toxicity is unique to cisplatin compared to carboplatin?
A) Myelosuppression
B) Ototoxicity
C) Nausea/vomiting
D) Alopecia
Solution: B) Ototoxicity
Rationale: The table lists ototoxicity monitoring only for cisplatin.
Anthracyclines like doxorubicin exert their cytotoxic effects through which mechanisms? (Select ALL that apply.)
A) Intercalation into DNA
B) Inhibition of topoisomerase II
C) Creation of oxygen-free radicals
D) Blockade of microtubule assembly
Solution: A) Intercalation into DNA, B) Inhibition of topoisomerase II, C) Creation of oxygen-free radicals
Rationale: The underlined header lists all three mechanisms as key actions of anthracyclines.
Which monitoring parameter is essential for patients receiving doxorubicin?
A) Left ventricular ejection fraction (LVEF)
B) Forced expiratory volume (FEV1)
C) Intracranial pressure
D) Glomerular filtration rate (GFR)
Solution: A) Left ventricular ejection fraction (LVEF)
Rationale: The table specifies monitoring "LVEF" for anthracycline-induced cardiotoxicity.
What is the maximum recommended lifetime cumulative dose of doxorubicin to minimize cardiotoxicity?
A) 300-400 mg/m²
B) 450-550 mg/m²
C) 600-700 mg/m²
D) No maximum limit
Solution: B) 450-550 mg/m²
Rationale: The underlined text clearly states to "limit total lifetime cumulative dose to 450-550 mg/m²."
Which medication can be used to reduce anthracycline-induced cardiotoxicity in select patients?
A) Mesna
B) Dexrazoxane
C) Leucovorin
D) Amifostine
Solution: B) Dexrazoxane
Rationale: The table lists dexrazoxane as a "chemoprotectant" for this purpose.
A patient receiving doxorubicin develops peripheral edema and shortness of breath. Which toxicity should be suspected?
A) Pulmonary fibrosis
B) Heart failure
C) Nephrotic syndrome
D) Anaphylaxis
Solution: B) Heart failure
Rationale: The table lists "edema, shortness of breath" as symptoms of cardiotoxicity.
The generic name "-rubicin" (as in doxorubicin) is associated with which distinctive side effect?
A) Blue sclera
B) Red discoloration of bodily fluids
C) Green-colored urine
D) Yellow skin pigmentation
Solution: B) Red discoloration of bodily fluids
Rationale: The "NAME TIP" states the "-rubicin" suffix correlates with "ruby red body fluids."
What color change in bodily fluids is associated with mitoxantrone?
A) Red
B) Blue
C) Green
D) Orange
Solution: B) Blue
Rationale: The table specifies "blue discoloration of sclera and bodily fluids" for mitoxantrone.
A patient's urine turns red after doxorubicin administration. Which action is appropriate?
A) Hold next dose
B) Reassure the patient this is expected
C) Administer IV fluids
D) Check CK-MB levels
Solution: B) Reassure the patient this is expected
Rationale: The "ruby red body fluids" note indicates this is a benign, expected effect
Mitoxantrone is classified as:
A) An anthracycline
B) An anthracenedione
C) A platinum analog
D) An alkylating agent
Solution: B) An anthracenedione
Rationale: The table clearly identifies mitoxantrone as "an anthracenedione, related to the anthracyclines."
A patient asks why they need echocardiograms during doxorubicin treatment. How should the pharmacist respond?
A) "To monitor for potential heart damage"
B) "To assess kidney function"
C) "To check for lung toxicity"
D) "To evaluate liver enzymes"
Solution: A) "To monitor for potential heart damage"
Rationale: LVEF monitoring (via echocardiogram) is specifically for cardiotoxicity.
A patient receives 6 cycles of doxorubicin at 60 mg/m² per cycle. What is their cumulative dose?
A) 240 mg/m²
B) 300 mg/m²
C) 360 mg/m²
D) 420 mg/m²
Solution: C) 360 mg/m²
Rationale: 60 mg/m² × 6 cycles = 360 mg/m² (direct application of the underlined formula).
At what cumulative doxorubicin dose should dexrazoxane be considered?
A) 100 mg/m²
B) 200 mg/m²
C) 300 mg/m²
D) 400 mg/m²
Solution: C) 300 mg/m²
Rationale: The underlined guideline states to consider dexrazoxane at ≥300 mg/m².
A patient with prior mediastinal radiation reaches a doxorubicin cumulative dose of 400 mg/m². What action is required?
A) Continue treatment up to 550 mg/m²
B) Switch to liposomal doxorubicin
C) Discontinue doxorubicin
D) Reduce dose by 50%
Solution: C) Discontinue doxorubicin
Rationale: The lower end (400-450 mg/m²) applies for high-risk patients (e.g., prior radiation).
Which imaging modality is used to monitor LVEF for doxorubicin cardiotoxicity? (Select ALL that apply.)
A) Echocardiogram
B) MUGA scan
C) CT angiography
D) PET scan
Solution: A) Echocardiogram, B) MUGA scan
Rationale: The underlined text specifies both modalities for LVEF monitoring.
Dexrazoxane is initiated in a patient receiving doxorubicin primarily to:
A) Prevent myelosuppression
B) Reduce cardiotoxicity
C) Treat extravasation
D) Enhance efficacy
Solution: B) Reduce cardiotoxicity
Rationale: The underlined text links dexrazoxane to cardiotoxicity prevention at ≥300 mg/m².
What is the absolute maximum lifetime cumulative dose of doxorubicin for most patients?
A) 300 mg/m²
B) 450 mg/m²
C) 550 mg/m²
D) 600 mg/m²
Solution: C) 550 mg/m²
Rationale: The underlined range of 450-550 mg/m² establishes 550 mg/m² as the upper limit.
When should LVEF be assessed in patients receiving doxorubicin?
A) Only at treatment completion
B) Before treatment and every 2 cycles
C) Only if symptoms develop
D) Before and after treatment
Solution: D) Before and after treatment
Rationale: The guideline specifies monitoring "before and after treatment."
A patient has received 350 mg/m² of doxorubicin with 3 more planned cycles (50 mg/m² each). Which action is appropriate?
A) Continue without changes
B) Add dexrazoxane
C) Switch to epirubicin
D) Discontinue immediately
Solution: B) Add dexrazoxane
Rationale: At 350 mg/m² (≥300 mg/m²), dexrazoxane should be considered per guidelines.
A 65-year-old patient receiving irinotecan (Campiosa) for metastatic colon cancer develops acute diarrhea and abdominal cramping during the infusion. Which of the following is the most appropriate immediate treatment?
A. Loperamide
B. Atropine
C. Ondansetron
D. Diphenhydramine
Solution: B. Atropine
Rationale: Acute diarrhea during irinotecan infusion is due to cholinergic effects (e.g., abdominal cramping, lacrimation). Atropine (an anticholinergic) is used for prevention/treatment. Loperamide is reserved for delayed diarrhea (>24 hours post-infusion).
Which adverse effect of irinotecan is associated with the mnemonic "I run to the can"?
A. Neutropenia
B. Acute diarrhea
C. Peripheral neuropathy
D. Alopecia
Solution: B. Acute diarrhea
Rationale: The mnemonic refers to acute cholinergic diarrhea occurring during/after irinotecan infusion. Delayed diarrhea occurs later (>24 hours).
A patient experiences severe delayed diarrhea 48 hours after receiving irinotecan. Which of the following is the first-line treatment?
A. Atropine
B. Loperamide (high-dose)
C. Octreotide
D. Hydromorphone
Solution: B. Loperamide (high-dose)
Rationale: Delayed diarrhea (>24 hours post-infusion) is managed with antidiarrheals (e.g., loperamide). Atropine is for acute diarrhea. Octreotide is reserved for loperamide-refractory cases.
Which phase of the cell cycle is primarily targeted by topoisomerase I inhibitors like irinotecan?
A. G1 phase
B. S phase
C. G2 phase
D. M phase
Solution: B. S phase
Rationale: Topoisomerase I inhibitors act during the S phase by causing DNA strand breaks during replication. Topoisomerase II inhibitors (e.g., etoposide) target the G2 phase
A patient on irinotecan develops cholinergic symptoms (lacrimation, salivation). Which premedication could have prevented this?
A. Dexamethasone
B. Atropine
C. Granisetron
D. Leucovorin
Solution: B. Atropine
Rationale: Atropine premedication can prevent acute cholinergic symptoms caused by irinotecan.
What is the mechanism of action of topoisomerase I inhibitors?
A. Inhibit microtubule polymerization
B. Prevent DNA religation, causing strand breaks
C. Crosslink DNA strands
D. Block purine synthesis
Solution: B. Prevent DNA religation, causing strand breaks
Rationale: Topoisomerase I inhibitors prevent resealing of single-strand DNA breaks, leading to apoptosis.
Which supportive care measure is critical for a patient with irinotecan-induced delayed diarrhea?
A. IV bisphosphonates
B. Hydration and electrolyte replacement
C. Filgrastim
D. Potassium supplements
Solution: B. Hydration and electrolyte replacement
Rationale: Symptomatic care for delayed diarrhea includes hydration/electrolyte replacement to prevent dehydration.
Which drug is a topoisomerase II inhibitor?
A. Irinotecan
B. Topotecan
C. Etoposide
D. Fluorouracil
Solution: C. Etoposide
Rationale: Etoposide is a topoisomerase II inhibitor. Irinotecan and topotecan are topoisomerase I inhibitors.
A patient receiving etoposide for lung cancer asks how the drug works. The pharmacist explains it targets which cell cycle phase?
A. G1
B. S
C. G2
D. M
Solution: C. G2
Rationale: Topoisomerase II inhibitors (e.g., etoposide) act in the G2 phase by preventing DNA religation.
Which adverse effect is unique to irinotecan compared to other topoisomerase inhibitors?
A. Alopecia
B. Acute cholinergic diarrhea
C. Mucositis
D. Cardiotoxicity
Solution: B. Acute cholinergic diarrhea
Rationale: Irinotecan’s acute diarrhea (with cholinergic symptoms) is distinctive. Other topoisomerase inhibitors more commonly cause myelosuppression.
A 45-year-old patient receiving vincristine for non-Hodgkin’s lymphoma reports new-onset numbness and tingling in their fingers. Which adverse effect is most likely?
A. Myelosuppression
B. Peripheral neuropathy
C. Hepatotoxicity
D. Cardiotoxicity
Solution: B. Peripheral neuropathy
Rationale: Vinca alkaloids (e.g., vincristine) inhibit microtubule formation, disrupting axonal transport and causing peripheral neuropathy (numbness, paresthesia).
What is the maximum single dose of vincristine, regardless of body surface area (BSA) calculations?
A. 1 mg
B. 2 mg
C. 4 mg
D. No maximum dose
Solution: B. 2 mg
Rationale: To mitigate neurotoxicity, vincristine doses are capped at 2 mg per dose (per NCCN guidelines)
A pharmacist notices vincristine is prepared in a 50 mL IV bag. Which risk does this preparation method aim to prevent?
A. Extravasation
B. Intrathecal administration
C. Rapid infusion reaction
D. Hypersensitivity
Solution: B. Intrathecal administration
Rationale: Vincristine must be prepared in a small IV piggyback bag to avoid fatal intrathecal administration (boxed warning).
Which route must be used for vinca alkaloid to avoid toxicity described by the warning "FATAL IF GIVEN BY OTHER ROUTES"?
A. Oral administration
B. Intrathecal administration
C. Subcutaneous injection
D. Intramuscular injection
E. Intravenous injection
Solution: E. Intravenous injection
Rationale: It must only be given IV.
A patient on vincristine develops severe constipation. Which mechanism explains this?
A. Autonomic neuropathy
B. Electrolyte imbalance
C. Bowel obstruction
D. Opioid-induced effect
Solution: A. Autonomic neuropathy
Rationale: Vinca alkaloids disrupt autonomic nerves, leading to constipation (a form of autonomic neuropathy).
Which phase of the cell cycle is targeted by vinca alkaloids?
A. G1
B. S
C. G2
D. M
Solution: D. M phase
Rationale: Vinca alkaloids inhibit microtubule formation during mitosis (M phase), preventing spindle formation.
A patient with neuropathic pain from vincristine asks why it occurs. The pharmacist explains it is due to:
A. Demyelination of CNS neurons
B. Disrupted axonal transport in peripheral nerves
C. Calcium channel blockade
D. Serotonin syndrome
Solution: B. Disrupted axonal transport in peripheral nerves
Rationale: Vinca alkaloids impair microtubule-dependent axonal transport, causing peripheral neuropathy.
Which monitoring parameter is critical for patients receiving vincristine?
A. Liver function tests
B. Signs of neuropathy (e.g., numbness)
C. Serum creatinine
D. ECG
Solution: B. Signs of neuropathy (e.g., numbness)
Rationale: Neuropathy monitoring (e.g., pain, paresthesia) is essential due to dose-limiting toxicity.
A nurse asks why vincristine is never dispensed in a syringe. The pharmacist’s response should emphasize:
A. Risk of extravasation
B. Risk of accidental intrathecal use
C. Stability concerns
D. Compatibility issues
Solution: B. Risk of accidental intrathecal use
Rationale: Syringes increase risk of fatal intrathecal administration; vincristine must be diluted in an IV bag.
Which of the following is a boxed warning for vincristine?
A. Cardiogenic shock
B. Intrathecal administration is fatal
C. QT prolongation
D. Hemorrhagic cystitis
Solution: B. Intrathecal administration is fatal
Rationale: The boxed warning states vincristine is fatal if given intrathecally (causes ascending paralysis/death).
A 60-year-old patient with pre-existing diabetic neuropathy is prescribed vincristine. Which action is most appropriate?
A. Avoid vincristine due to contraindication
B. Reduce dose and monitor for worsening neuropathy
C. Administer with IV calcium gluconate
D. Premedicate with atropine
Solution: B. Reduce dose and monitor for worsening neuropathy
Rationale: Pre-existing neuropathy increases risk, but vincristine can be used cautiously with dose reduction and close monitoring.
A 58-year-old patient develops numbness and tingling in their hands after 3 cycles of paclitaxel for breast cancer. Which is the most likely cause?
A. Hypercalcemia
B. Peripheral neuropathy
C. Hypersensitivity reaction
D. Fluid retention
Solution: B. Peripheral neuropathy
Rationale: Paclitaxel stabilizes microtubules, disrupting axonal transport and causing dose-limiting peripheral neuropathy (numbness, paresthesia).
Which phase of the cell cycle do taxanes primarily target?
A. G1
B. S
C. G2
D. M
Solution: D. M phase
Rationale: Taxanes inhibit microtubule depolymerization during mitosis (M phase), preventing spindle breakdown.
A patient is scheduled to receive docetaxel. Which premedication regimen is most appropriate to prevent hypersensitivity reactions?
A. Dexamethasone alone
B. Dexamethasone + diphenhydramine + famotidine
C. Ondansetron + aprepitant
D. Atropine + loperamide
Solution: B. Dexamethasone + diphenhydramine + famotidine
Rationale: Docetaxel requires premedication with steroids (e.g., dexamethasone), antihistamines (diphenhydramine), and H2RAs (famotidine) to prevent solvent-related hypersensitivity.
Which taxane is most associated with severe fluid retention?
A. Paclitaxel
B. Docetaxel
C. Cabazitaxel
D. Nab-paclitaxel
Solution: B. Docetaxel
Rationale: Docetaxel carries a boxed warning for severe fluid retention (pleural effusion, ascites), mitigated by steroid premedication.
A nurse asks why docetaxel must be administered using non-PVC tubing. The pharmacist's response should cite:
A. Risk of leaching plasticizers into the solution
B. Incompatibility with 0.9% sodium chloride
C. Increased risk of extravasation
D. Reduced drug stability
Solution: A. Risk of leaching plasticizers into the solution
Rationale: Docetaxel’s solvent (polysorbate 80) leaches plasticizers from PVC tubing, requiring non-PVC bags/tubing.
A patient develops facial swelling and dyspnea 10 minutes into their first docetaxel infusion. Which is the immediate action?
A. Administer IV calcium gluconate
B. Stop infusion and give epinephrine
C. Increase infusion rate to complete dose faster
D. Add diphenhydramine to the IV bag
Solution: B. Stop infusion and give epinephrine
Rationale: This describes anaphylaxis (angioedema, dyspnea). Stop infusion and treat with epinephrine (per ASCO guidelines).
Which monitoring parameter is critical for patients receiving docetaxel?
A. Serum potassium
B. Signs of fluid retention (e.g., weight gain, edema)
C. Platelet count
D. Liver enzymes
Solution: B. Signs of fluid retention (e.g., weight gain, edema)
Rationale: Docetaxel requires monitoring for fluid retention (boxed warning), which steroids may mitigate.
A pharmacist reviews an order for paclitaxel in a patient with pre-existing diabetic neuropathy. Which action is most appropriate?
A. Discontinue paclitaxel due to contraindication
B. Reduce dose and monitor neuropathy symptoms
C. Substitute with docetaxel
D. Premedicate with IV magnesium
Solution: B. Reduce dose and monitor neuropathy symptoms
Rationale: Pre-existing neuropathy increases risk, but paclitaxel can be used with dose adjustments and close monitoring.
What is the mechanism of action of taxanes?
A. Inhibit tubulin polymerization
B. Stabilize microtubules to prevent depolymerization
C. Crosslink DNA strands
D. Block topoisomerase II
Solution: B. Stabilize microtubules to prevent depolymerization
Rationale: Taxanes hyperstabilize microtubules, disrupting mitosis (contrast with vinca alkaloids, which inhibit polymerization).
Which taxane requires non-PVC infusion sets due to its solvent system?
A. Paclitaxel
B. Docetaxel
C. Both A and B
D. Neither A nor B
Solution: C. Both A and B
Rationale: Both paclitaxel (Cremophor EL) and docetaxel (polysorbate 80) require non-PVC bags/tubing to prevent leaching.
Which of the following taxanes requires administration using non-PVC tubing and containers due to the risk of leaching plasticizers?
A. Nab-paclitaxel
B. Cabazitaxel
C. Docetaxel
D. Both B and C
Solution: D. Both B and C
Rationale:
Docetaxel (polysorbate 80 solvent) and cabazitaxel (polysorbate 80) must be administered with non-PVC tubing/bags to prevent leaching of plasticizers (e.g., DEHP).
Nab-paclitaxel (Abraxane) is albumin-bound and does not require special tubing.
A nurse prepares to administer paclitaxel and notices the order specifies "use 0.22 micron in-line filter." Which of the following explains this requirement?
A. To prevent microbial contamination
B. To remove precipitate formed by the Cremophor EL solvent
C. To reduce the risk of hypersensitivity reactions
D. To stabilize the drug during prolonged infusions
Solution: B. To remove precipitate formed by the Cremophor EL solvent
Rationale:
Paclitaxel’s Cremophor EL solvent can form micelles or precipitates, requiring a 0.22 micron filter to trap particles.
Cabazitaxel (Jevtana) also requires a 0.22 micron filter for the same reason (per prescribing information).
Filters do not prevent hypersensitivity (premedication does) or microbial contamination (handling sterility does).
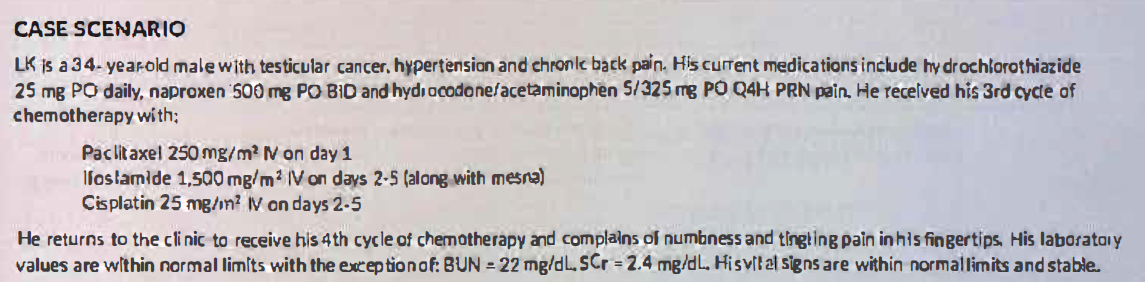
How would you characterize the type of pain LK describes?
It is consistent with sensory peripheral neuropathy
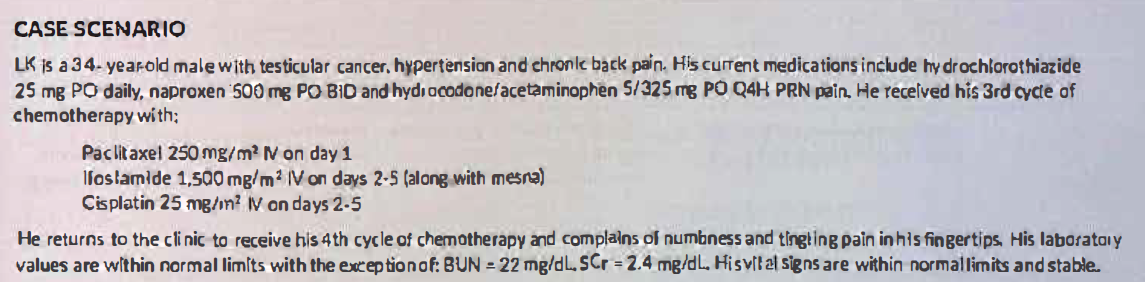
What could be causing his new pain symptoms?
Paclitaxel and cisplatin are assoicated with sensory peripheral neuropathy.
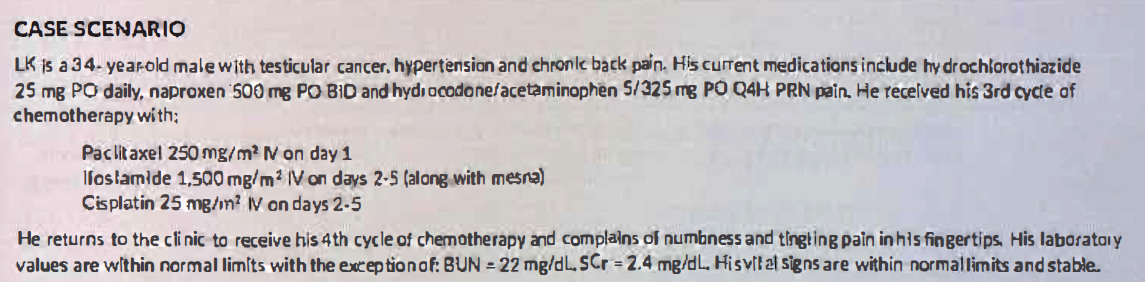
Dehydration is ruled outbased on the BUN/SCr ratio and normal vital signs. What is the likely cause of LK’s elevated SCr?
Cisplatin-induced nephrotoxicity should be suspected. No further cisplatin should be given at this time. Naproxen and hydrochlorothiazide should be held, as NSAIDs can decrease renal blood flow and diuretics can cause dehydration and potentiate further kidney damage. An alternative medication can be chosen for BP control.
A 62-year-old patient receiving capecitabine (Xeloda) for colon cancer develops painful erythema and peeling skin on their palms and soles. Which adverse effect is this?
A. Stevens-Johnson syndrome
B. Hand-foot syndrome
C. Allergic dermatitis
D. Photosensitivity
Solution: B. Hand-foot syndrome (palmar-plantar erythrodysesthesia)
Rationale: Capillary leakage of fluorouracil metabolites causes painful erythema and desquamation on palms/soles, a hallmark toxicity of fluoropyrimidines.
Which enzyme deficiency increases the risk of severe fluorouracil toxicity (e.g., myelosuppression, GI necrosis)?
A. Thiopurine methyltransferase (TPMT)
B. Dihydropyrimidine dehydrogenase (DPD)
C. CYP2D6
D. UDP-glucuronosyltransferase (UGT1A1)
Solution: B. Dihydropyrimidine dehydrogenase (DPD)
Rationale: DPD deficiency impairs fluorouracil metabolism, leading to life-threatening toxicity (per FDA warnings). Testing is recommended pre-treatment.
A patient on fluorouracil develops painful oral ulcers and thrush. Which toxicity is this?
A. Neuropathy
B. Mucositis
C. Hand-foot syndrome
D. Cardiotoxicity
Solution: B. Mucositis
Rationale: Fluorouracil targets rapidly dividing cells, including oral/GI mucosa, causing ulcerations and secondary infections (e.g., thrush).
Which drug is an oral prodrug of fluorouracil?
A. Tegafur
B. Capecitabine
C. Gemcitabine
D. Cytarabine
Solution: B. Capecitabine (Xeloda)
Rationale: Capecitabine is converted to fluorouracil by thymidine phosphorylase in tumors.
A patient’s INR rises to 6.5 after starting fluorouracil while on warfarin. Which mechanism explains this interaction?
A. Fluorouracil inhibits CYP2C9
B. Fluorouracil displaces warfarin from albumin
C. Fluorouracil reduces vitamin K absorption
D. Fluorouracil enhances warfarin’s anticoagulant effect
Solution: A. Fluorouracil inhibits CYP2C9
Rationale: Fluorouracil inhibits CYP2C9, the enzyme that metabolizes S-warfarin, increasing INR. Close INR monitoring is required.
Which phase of the cell cycle do pyrimidine analogs primarily target?
A. G1
B. S
C. G2
D. M
Solution: B. S phase
Rationale: Pyrimidine analogs (e.g., fluorouracil) inhibit DNA synthesis during the S phase by incorporating into DNA/RNA.
Which antidote should be given within 96 hours for fluorouracil overdose or early severe toxicity due to DPD deficiency?
A. Leucovorin
B. Uridine triacetate (Vistogard)
C. N-acetylcysteine
D. Methylene blue
Solution: B. Uridine triacetate (Vistogard)
Rationale: Uridine triacetate is the FDA-approved antidote for fluorouracil overdose, displacing fluorouracil from RNA/DNA.
Which adjuvant therapy enhances fluorouracil’s efficacy in colorectal cancer?
A. Levoleucovorin
B. Mesna
C. Dexrazoxane
D. Allopurinol
Solution: A. Levoleucovorin (or leucovorin)
Rationale: Leucovorin prolongs inhibition of thymidylate synthase by stabilizing fluorouracil’s active metabolite (FdUMP).