Key terms in Human factors
1/21
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
22 Terms
Medication error
Is any preventable event that may cause or lead to inappropriate medication use or patient harm while in the control of the health care professional, patient, or consumer.
-”Prescribe, advise on, or provide medicines or treatment, including repeat prescriptions (only if you are suitably qualified) if you have enough knowledge of that person’s health and are satisfied that the medicines or treatment serve that person’s health needs”
Types of medication errors
professional practice, health care products, procedures and systems, including prescribing, order communication, product labelling, packaging, nomenclature, compounding, dispensing, distribution, administration, education, monitoring and use
Human factors
enhancing clinical performance through an understanding of the effects of teamwork, task, equipment, workspace, culture and organisation on human behaviour and abilities and application of that knowledge in clinical settings
Human factors and cognition
Flaws are inherent in human cognitive processes. There are different modes of cognitions: skill based, rule based and knowledge based
Skills based- automatic mode
Inattention bias- when you are focusing on something while missing things that are right in front of you
Rule based- problem solving mode
apply a rule
pattern matching
Confirmation bias
Knowledge based
Analysis synthesis
Human factors and errors
Systems and human errors, mental workload, staffing levels, physical demands, tiredness, hunger, stress, distractions and interruptions, physical working environment, clutter, overstocking, lack of stock, device or product design
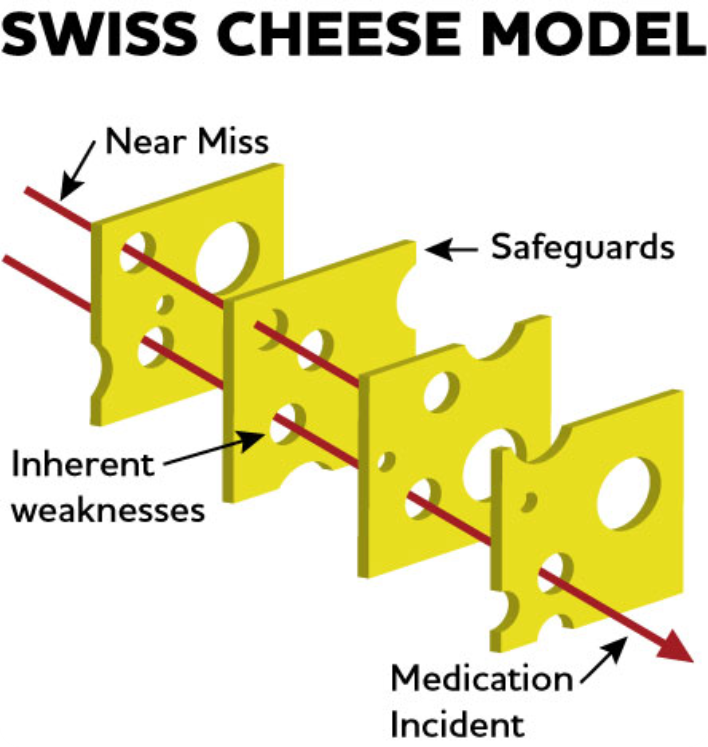
What is in place to help us avoid errors
Policies and guidelines, independent checking , 6R’s, BNF and monographs, scanning of wristband, labelling of medications- tall man lettering, compatible syringes, training and education, electronic prescribing (reduces medication errors), flagging allergies and drug interactions, default frequencies and doses
The NMC code (2018) says…
In Section 18 it says “Advise on, prescribe, supply, dispense or administer medicines within the limits of your training and competence, the law, our guidance and other relevant policies, guidance and regulations”
-"prescribe, advise on, or provide medicines or treatment, including repeat prescriptions (only if you are suitably qualified) if you have enough knowledge of that person’s health and are satisfied that the medicines or treatment serve that person’s health needs”
Never events
is a serious, largely preventable patient safety incident involving a medication error that should not happen if existing safety guidelines and procedures are followed.
Medication never events
•Mis-selection of a strong potassium solution
•Administration of medication by the wrong route
•Overdose of insulin due to abbreviations or incorrect device
•Overdose of methotrexate for non-cancer treatment
•Mis-selection of high strength midazolam during conscious sedation
Never event – administration of medication by the wrong route (2001)
The patient is given one of the following:
•intravenous chemotherapy by the intrathecal route
•oral/enteral medication or feed/flush by any parenteral route
•intravenous administration of an epidural medication that was not intended to be administered by the intravenous route
Never event – Overdose of insulin due to abbreviations or incorrect device
A patient is given a 10-fold or greater overdose of insulin because the words ‘unit’ or ‘international units’ are abbreviated; such an overdose was given in a care setting with an electronic prescribing system
•A healthcare professional fails to use a specific insulin administration device – that is, an insulin syringe or pen is not used to measure the insulin
•A healthcare professional withdraws insulin from an insulin pen or pen refill and then administers this using a syringe and needle
Near miss
It is a prevented patient safety incident, an event not causing harm but has the potential to cause injury or ill health. Reviewing near misses can provide useful learning and areas for improvement.
What do we when we make a medication error?
monitor patient for side effects
inform the doctors
incident report
duty of candour
Duty of candour
it is a general duty to be open and transparent with people receiving care from you. Nurses have both statutory and professional duty of candour. Its is also of the fundamental standards , below which care should never fall
Examples of duty of candour
offer an apology in person
act in an open and transparent way about the care and treatment provided
Provide an accurate account of what happened. This must include all the facts, to the best of your knowledge, at the time
tell them in person what further inquires you will need to make
Tell them in person as soon as possible after finding out about the incident. Support them around the incident, including when you tell them what happened
Follow this by giving the same information in writing. Give an update on the enquiries
Keep a written record of all communication with the relevant person.
Positive safety culture
education and training
supporting staff who make mistakes
National patient safety alerts
The NHS patient safety strategy
Patient safety incident response framework (PSIRF)
Sets out the NHS,s approach to developing and maintaining effective systems and processes for responding to patient safety incidents for the purpose of learning and improving patient safety
PSIRF key aims
compassionate engagement and involvement of those affected by patient safety incidents
Application of a range of system-based approached to learning from patient safety incidents
considered and proportionate responses to patient safety incidents
supportive oversight focused on strengthening response system functioning and improvement
Saying sorry
Saying sorry:
•always the right thing to do
•not an admission of liability
•acknowledges that something could have gone better
•the first step to learning from what happened and preventing it recurring
It is also statutory, regulation and professional requirement
(NHS resolution 2023)