2.2.2 SOCIAL: Health Behaviour and the COM-B. Model
1/106
Earn XP
Description and Tags
1-40: Define what we mean by ‘health’ and ‘health behaviour 41-62 Demonstrate examples of behaviour in determining health status 63-77: Explain some of the determinants of health behaviour 78-88: Discuss how the COM-B model can explain behaviour (real world issues) 89-107: Discuss how the Behaviour Change Wheel can be used to develop behaviour change interventions
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
107 Terms
WHO (1964): health definition
a state of complete physical, mental and social wellbeing and not merely the absence of disease or infirmity
criticism of WHO (1964) health definition
out of date and not fit for purpose due to ageing population and ability to manage chronic health conditions (CHCs)
what is health? (how do you quantify it)
not a binary state, but on a spectrum
Huber et al., (2011): what do they propose?
shift the emphasis of health towards the ability to adapt and self-manage in the face of social, physical, and emotional challenges
causes of death in 1900s
Pneumonia/flu
TB
Diarrhoea
Heart disease
Intracranial lesions (vasc.)
Nephritis
Accidents
Cancer
Senility
Diphtheria
Allender et al. (2008): categories of major causes of death in 2006 (COD)
all cardiovascular diseases (CVDs)
all cancers
respiratory disease
accidents and injuries
other causes
% of deaths from all CVDs in UK in 2006 (Allender et al., 2008)
m - 35%
w - 34%
% of deaths from all cancers in UK in 2006 (Allender et al., 2008)
m - 29%
w - 26%
% of deaths from respiratory disease in UK in 2006 (Allender et al., 2008)
m - 13%
w -14%
% of deaths from accidents and injuries in UK in 2006 (Allender et al., 2008)
m - 5%
w - 3%
% of deaths from “other causes” in UK in 2006 (Allender et al., 2008)
m - 18%
w - 23%
Defra (2008)
study examining % of deaths due to major causes like CVDs and cancer across lifespan, against age and sex
Defra (2008): % of deaths due to CVD across lifespan- findings
increase overlifespan
25-34: m and f around the same, higher for f
35-64 - see drastic increase in men dying from CVDs, from 44yo almost double men compared to women
women gradually increase across lifepspan, biggest jumps between 55-64 and 65-74, and then 64-74 and 75-84.
elderly population (75+), similar between men and women (slightly more women 85+ slightly more men 75-84)
risk for women appears more associated w old age , for men, anything above 45 seems high
Defra (2008): % of deaths due to cancer across lifespan- findings
not associated w old age, peaks middle age for both sexes
women much higher, over double in young adults - 25-34
mild increase for men linearly under 55-64 and same at 65-74 and then gradual decrease
women, increase to 55-64
well over double men for 35-44
gap between men and women closes 65-74
in elderly population, men higher than women
men double women 75-84
smaller gap but men slightly more 85+
what does Defra (2008) findings highlight?
significant sex differences in causes of deaths and differing dispersion of and relationship between
middle age women at highest risk for death by cancer
biggest gap between deaths by cvd in men vs women in the 35-64 age group (men more)
biggest gap between deaths by cancer in women vs men in 25-34, 35-44 and 45-54 (women more), and then large/double 75-84 (men more)
Adler et al. 1999: explaining health outcomes
behaviours like smoking, dietary choice, alcohol consumption, regular physical activity
play important role in HOs
Gruman + Follick, 1998: health outcomes
behavioural factors account for around 50% of premature deatths from the 10 leading causes
what % of premature deaths from the 10 leading causes can be accounted to behavioural factors
50
what marks the start of the modern concept of health behaviour
Doll and Hill (1964): studied british docs in 1950s and found smoking was a major precursor of premature mortality
health behaviour (Conner & Norman, 1996) definition
any activity undertaken for the purpose of preventing or detecting disease or disease or for improving health/wellbeing
Steptoe, Gardner, & Wardle, 2010: health behaviours
can have positive and negative health effects
what effects do health behaviours have?
positive and negative (Steptoe.. 2010)
types of health behaviour (HB)
protective
risky
term for negative health behaviour
risky health behaviour
term for positive health behaviour
protective health behaviour
protective health behaviour (PHB): definition
activities that may help to:
(and/or)
prevent disease
detect disease and disability at an early stage
promote and enhance health
project from risk of injury
risky health behaviour (RHB): definition
activities undertaken by people with a frequency of intensity that increases risk of injury or disease
health behaviours (broadest/ Steptoe, Gardner, & Wardle, 2010) definition:
behaviours individuals engage in that affect their health
difference in Conner & Norman 1996 and Steptoe, Gardner, & Wardle, 2010
CN1996- define HB as any activity undertaken for purpose of preventing or detecting disease or for improving health and wellbeing
their definition of HB is what SGC2010 define as the definition of protective HB
SGC2010 highlight two types of HBs- protective vs risky, and so define HB broadly as behaviours individuals engage w that affect (non directional bc can be good or bad) their health
measuring health behaviours: what is often the dv + why
behaviour
bc the currency of research into health behaviours
challenge with measuring HBs
dv behaviour
behaviour notoriously hard to measure
how are health behaviours typically measured?
self report questionnaires using categorical or continuous measures
smoking: two main types of self report qs, format example
categorical: do you smoke- yes/no
continuous: how many cigarrettes do you smoke a day?
issues with measuring health behaviours via self report questionnaires
social desirability bias → over/under repporting
subject to recall bias
measures of health behaviours
self report questionnaire (typically categorical or continuous)
observation
proxy measures
what is CCTV cameras to observe mask wearing in supermarkets an example of
an observational measure of health behaviours
what are some examples of proxy measures of HBs
blood tests
step counters
pill counters
what are blood tests, step counters, pill counters, etc examples of?
proxy measures of HBs
issue w proxy measures of HBs
not always accurate
accuracy issues w proxy measures of HBs (examples)
blood test results can depend on metabolic rate
pill counters rely on pills actually being taken out of a bottle
step counters- errors in measurement, can be falsified
also: (my thghts): positive health behaviours do not always equal positive health outcomes, underlying conditions can perservere regardless of behaviour, blood tests cld be perfect in someone who eats poorly, doesnt diet, and cld show nutrient deficiencies in someone who eats well, takes supplements etc. plus possibly issues w measures being geared towards male levels/ white ppl/ miscalculated or wrongly balanced for Black ppl and other poc. so may not acc indicate health behaviours always.
Alameda country study (Belloc, 1973): procedure/participants
around 7000 adults
baseline postal questionnaire in 1965 followed by regular surveys of death and illness
Alameda country study (Belloc, 1973): findings
7 negative health behaviours predicted mortality:
lack of exercise
snacking between meals
smoking
sleep (more than 8 hrs, less than 7),
skipping breakfast
regularly drinking more than 5 units of alcohol
over/underweight
negative health behaviours predicting mortality in Belloc, 1973 study + study name
Alameda country study
lack of exercise
snacking between meals
smoking
sleep (more than 8 hrs, less than 7),
skipping breakfast
regularly drinking more than 5 units of alcohol
over/underweight
Belloc (1973): features of a healthy lifestyle
7 negative health behaviours predicted mortality
highlighted then 7 features of a healthy lifestyle
non smoking
moderate alcohol intake
7-8hrs sleep nightly
exercise regularly
maintain a healthy body weight
avoid high cal snacks
eat breakfast regularly
7 features of a healthy lifestyle (Belloc 1973): relationship strength
very strong
relationship between the 7 health behaviours + death/illness lead Belloc (1973) to propose that…
people aged 75+yo who carried out all 7 of the positive behaviours had health comparable to those aged 35-44 who did less than 3
Belloc (1973) proposed
people aged 75+yo who carried out all 7 of the positive health behaviours (‘features of a healthy lifestyle’) had health comparable to those aged 35-44 who did less than 3
Khaw et al., (2008): procedure
analysed data from the EPIC Norfolk longitudinal study of 20,000 men and women
baseline - no known cvd/cancer, aged 45-79
followed up over 14 years
looked at association between cumulative survival and health behaviours
Khaw et al., (2008): findings
survival was associated with 4 health behaviours:
not smoking
being physically active
drinking moderately
eating 5 or more servings of fruit and veg per day
the fewer of these behaviours performed → the greater the risk of death
number of health behaviours- studies
Belloc (1973): Alameda country study
Khaw et al., (2008): analysed data from EPIC Norfolk longitudinal study
preventable causes of death by health behaviour- study
Danaei et al., (2009)- investigation of deaths in USA
Danaei et al., 2009
investigation of deaths in USA
health behaviours can be linked to range of different causes of deaths - CV, cancer, diabetes, respiratory, other NCD, injury
e.g. smoking attributable to CVD, cancer, diabetes, and resp diseases
health behaviours in the modern world: points emerging from definitons of HB and its study
concept of health behaviour is fluid and behaviours included can change as medical knowledge develops
health behaviours not uniformly important, but vary in their influence across time and different populations
strength of evidence relating behaviours w health outcomes is variable
behaviours may be done for non health purposes- e.g. motivated for appearance over health
key point:
health psychologists need to view behaviour in a broad context and recognise that health motivations and cognitions are a part of a wider set of influences on health behaviour
what perspective shld health psychologists take
view behaviour in a broad context and recognise that health motivations and cognitions are a part of a wider set of influences on health behaviour
strength of evidence relating behaviours with health outcomes
variable
case control, prospective, experiemtnal, cross sectional (but association =/= causation)
consistent results w diff samples and study desgins, and a clear biological mechanism → stronger evidence
case- control study
type of observational study commonly used to look at factors associated w disease or outcomes
two existing groups differing in outcome/condition are identified and compared on the basis of supposed causal attribute/s
important health behaviours in the modern world
diet
physical activity
smoking
sexual behaviour
alcohol
diet (NHS, 2020)
in 2018 only 28% adults eating 5+ servings fruit/veg per day
physical activity (WHO, 2022)
more than 80% adolescents and 27% adults do not meet their recommended levels
smoking (ONS, 2021)
rates declined over last decade but still 8ish million adults in uk who do
highest rates 25-34yos
sexual behaviour (YouGov poll, 2017)
47% of sexually active young ppl do not use a condom when sleeping with sm1 for the first time
alchohol (ONS, 2017)
25-28% adult drinkers in UK binge on alc on their heaviest drinking day
types of behaviour change
initating a new behaviour
stopping an existing behaviour
how a behaviour is performed (changing frequency, intensity, duration)
changing behaviour: what do we need to consider?
biopsychosocial approach to health
primary motivational concerns in life same for humans as are for most animals- food,water,air,reproduction,etc
challenging behaviours motivated by these systems can be difficult (e.g.: sexual behaviour-condom usage; energy seeking behaviour- eating habits; energy conservation behaviour- exercise levels)
appreciation of evolutionary/biological, psychological, social contexts in which behaviour takes place to understand and then attempt to change
determinants of health behaviour: biopsychosocial approach
biology x psychology x social context
overlap of all = health
biological determinants of health behaviour
gender
physical illness
disability
genetic vulnerability
immune function
neurochemistry
stress reactivity
medication effects
psychological determinants of health behaviour
learning/memory
attitudes/beliefs
personality
behaviours
emotions
coping skills
past trauma
social context determinants of health behaviour
social supports
family background
cultural traditions
social/economic status
education
Plomin et al., 2000: biological determinants
twin studies evidence suggesting heritable component to smoking initiation, nicotine addiction, as well as body weight and obesity
biological determinants of health behaviours- physiology
some HBs have physiological response (smoking, drinking, ating, exercising) → releasing dopamine, endorphins which can reinforce the behaviour
biological determinants of health behaviours- ability
ability to carry out many HBs is affected by personal health
disabilities may impact ability to carry out physical activity
symptoms can act as cues to change or stop behaviour (e.g. smoking, adherence to meds, etc)
social determinants of health behaviours (Baranowski, 1997)
HBs strongly affected by peer group influences, family habits, and social networks
early socialisation- observational learning → health habits e.g. brushing teeth, smoking
culturally valued or discouraged behaviour → e.g. alc consumption in some religions
peer pressure in adolescence → contributor/origin of many risk behaviours
social determinants of health behaviour (Pampel, Kreuger, Denney, 2010)
socioeconomic status (SES)
financial barriers to health behaviours, lack of available resource, lower education
social determinants of health behaviour (DeJong & Hingson, 1998)
legislative laws
e.g seat belt use, drink driving
psychological determinants of health behaviour: two core components
emotion
cognition
psychological determinants of health behaviour (Ferrer and Mendes, 2018)
emotion
stress - smoking, overeating, drinking, and exercise
fear - avoidance of healthcare (e.g. dental- delay in response to symptoms, screening etc)
disgust → fear avoidance - blood test, cervical screening
psychological determinants of health behaviour (Armitage and Conner, 2000)
cognition
attitudes/beliefs
social cognition models (e.g. ToPB, Azjen, 1991)
interventions based on ToPB to improve HB
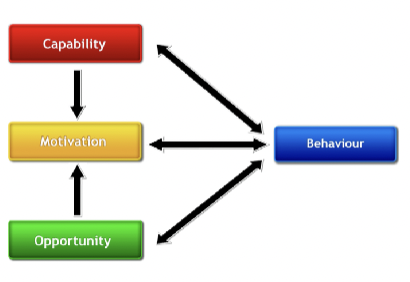
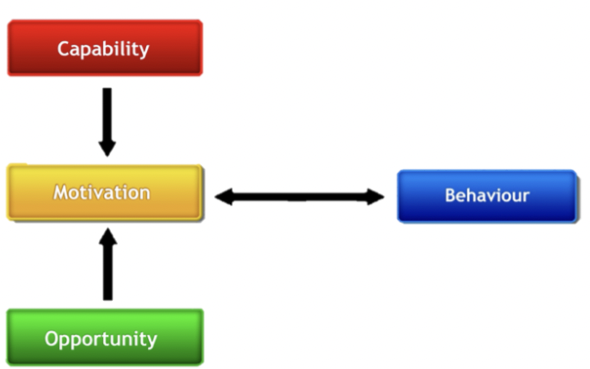
COM-B Model (Michie et al., 2011)
C = capability
O = opportunity
M = motivation
B = behaviour
COM-B: C
capability
the ability to enact behaviour
capability = physical + psychology capability
COM-B: O
opportunity
environment that enables behaviour
opportunity = physical + social opportunity
physical- afforded by environment
social- afforded by social/cultural norms
COM-B: M
motivation
mechanisms that activate or inhibit behaviour
motivation = reflective + automatic motivation
reflective- evaluations (beliefs about what is good/bad), plans (intentions)
automatic- emotional reactions, desires (wants and needs), impulses, inhibitions. e.g. anticipated pleasure
methods to collect data using COM-B
questionnaires
interviews/ focus groups
observation
questionnaire method to collect data using COM-B
specific Qs about their C/O/M
reach larger groups of ppl
interview/ focus group method to collect data using COM-B
in depth qualitative data
ask open ended Qs about C/O/M/ barriers/ facilitators of engaging in desired behaviour
smaller samples
observation method to collect data using COM-B
self report data from questionnaires/interviews may be far from the truth
observations useful tool to see what acc happens
how well can the COM-B explain behaviour? study
Willmott et al., (2021) COM-B and physical activity
Willmott et al., (2021): design
COM-B and physical activity
cross sectional survey
used validated measures to capture COM constructs and physical activity behaviour
administered online to sample of young adults 18-35yo
N = 582, mean age 22.8, 80.3% female
Willmott et al., (2021): findings
the COM-B model explained 31% of variance in physical activity
C and O found to be associated with B through mediating effect of M
increased C + increased O → increased M → increase physical activity (B)
Michie et al., (2011): designing interventions for behaviour change
developed a synthesis of 19 frameworks of behaviour change interventions
the Behaviour Change Wheel (BCW)
BCW:
comprehensive
coherent
linked to a model of behaviour- the COM-B
identified 9 intervention functions and 7 policy categories that cld enable/support these interventions to occur
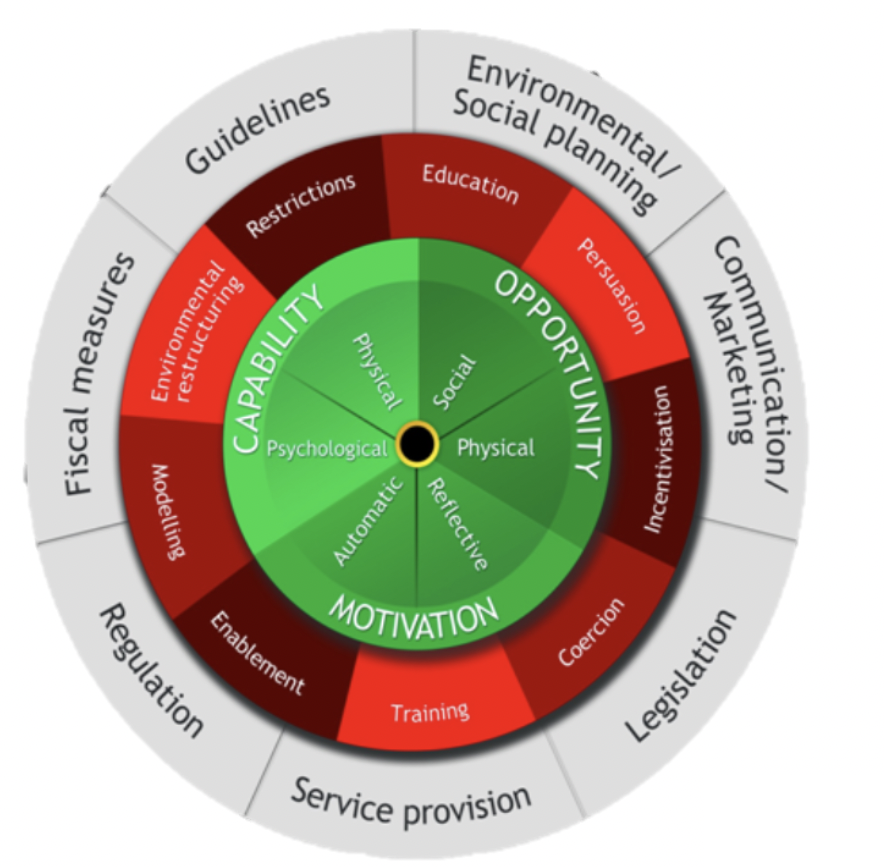
what do the colours correspond to on the BCW?
grey
red
green
policy categories
intervention functions
sources of behaviour
describe the BCW
a wheel made by Michie et al., 2011 to aid behave change/intervention development
behavioural diagnosis → aspects of COM-B that need addressing → intervention functions to change the behaviour + policies aiding that
centre circle- sources of behaviour:
motivation (automatic, reflective)
capability (physical, psychological)
opportunity (social, physical)
inner circle- intervention functions:
enablement
training
coercion
incentivisation
persuasion
education
restrictions
environmental restructuring
modelling
outer circle- policy categories:
service provision
legislation
communication/marketing
environmental/social planning
guidelines
fiscal measures
regulation
BCW: intervention functions
= activities designed to change behaviour
enablement
training
coercion
incentivisation
persuasion
education
restrictions
environmental restructuring
modelling
can be matched to COM-B
capability- physical → effective intervention functions
training
enablement
capability- psychological → effective intervention functions
education
training
enablement
opportunity- physical → effective intervention functions
restriction
environmental restructuring
enablement
opportunity- social → effective intervention functions
restriction
environmental restructuring
enablement
motivation- automatic → effective intervention functions
persuasion
incentivisation
coercion
environmental restructuring
modelling
enablement
motivation- reflective → effective intervention functions
education
persuasion
incentivisation
coercion
intervention function definitions
Education: increasing people’s knowledge
Persuasion: using communication to induce positive or negative feelings
Incentivisation: creating an expectation of reward
Coercion: creating an expectation of cost or punishment
Training: helping people to develop skills
Enablement: giving people means to engage in behaviour or reduce barriers
Modelling: providing an example for people to aspire to or emulate
Environmental restructuring: changing the physical or social context
Restrictions: using rules to reduce opportunity to engage in target behaviours
BCW: policy categories
policies = decisions made by authorities concerning interventions
policy categories are:
service provision
legislation
communication/marketing
environmental/social planning
guidelines
fiscal measures
regulation