NPTE: SCI
1/45
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
46 Terms
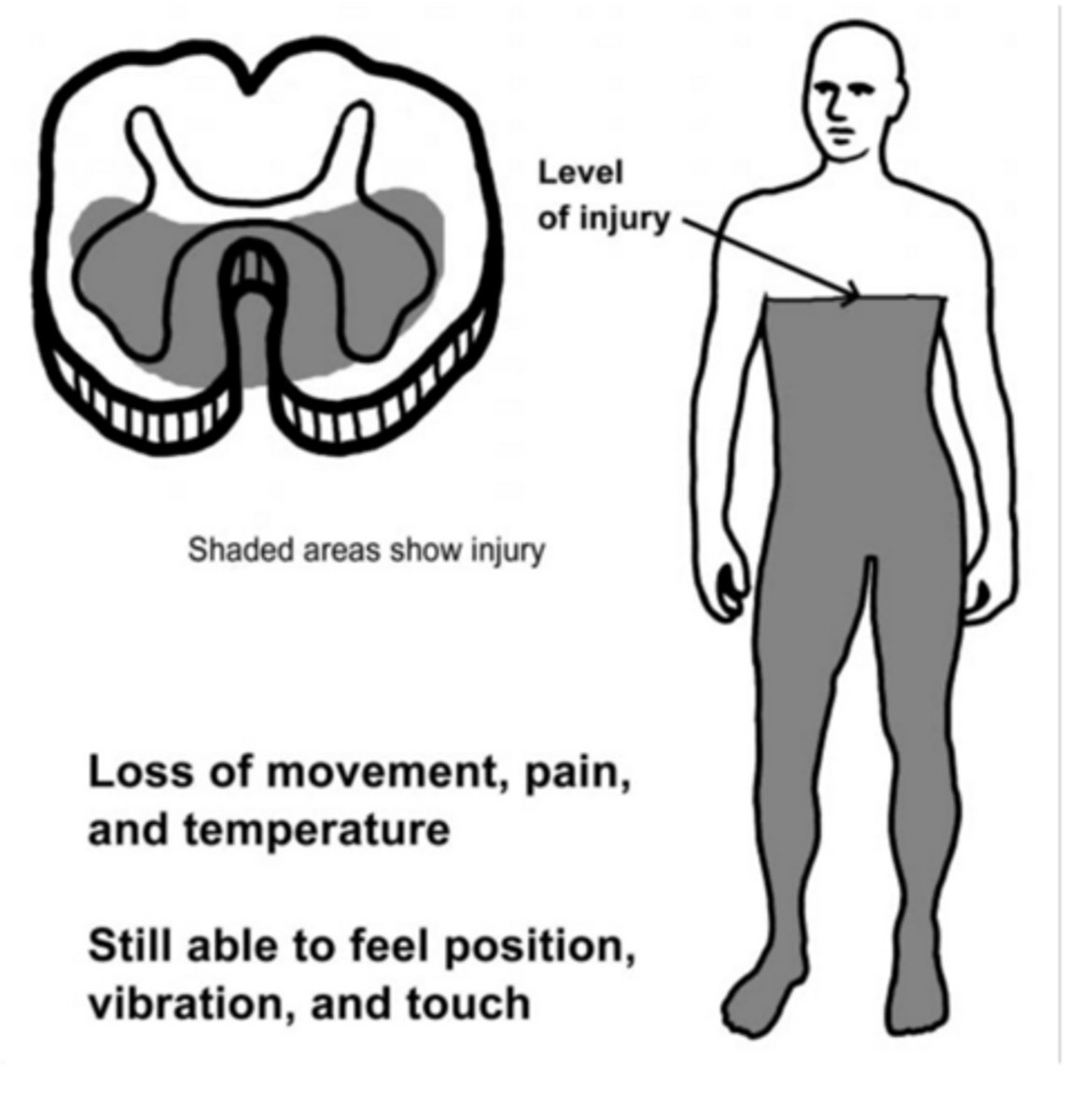
Anterior cord syndrome
hyperflexion injury
-loss of pain and temperture bilaterally
-loss of motor bilaterally
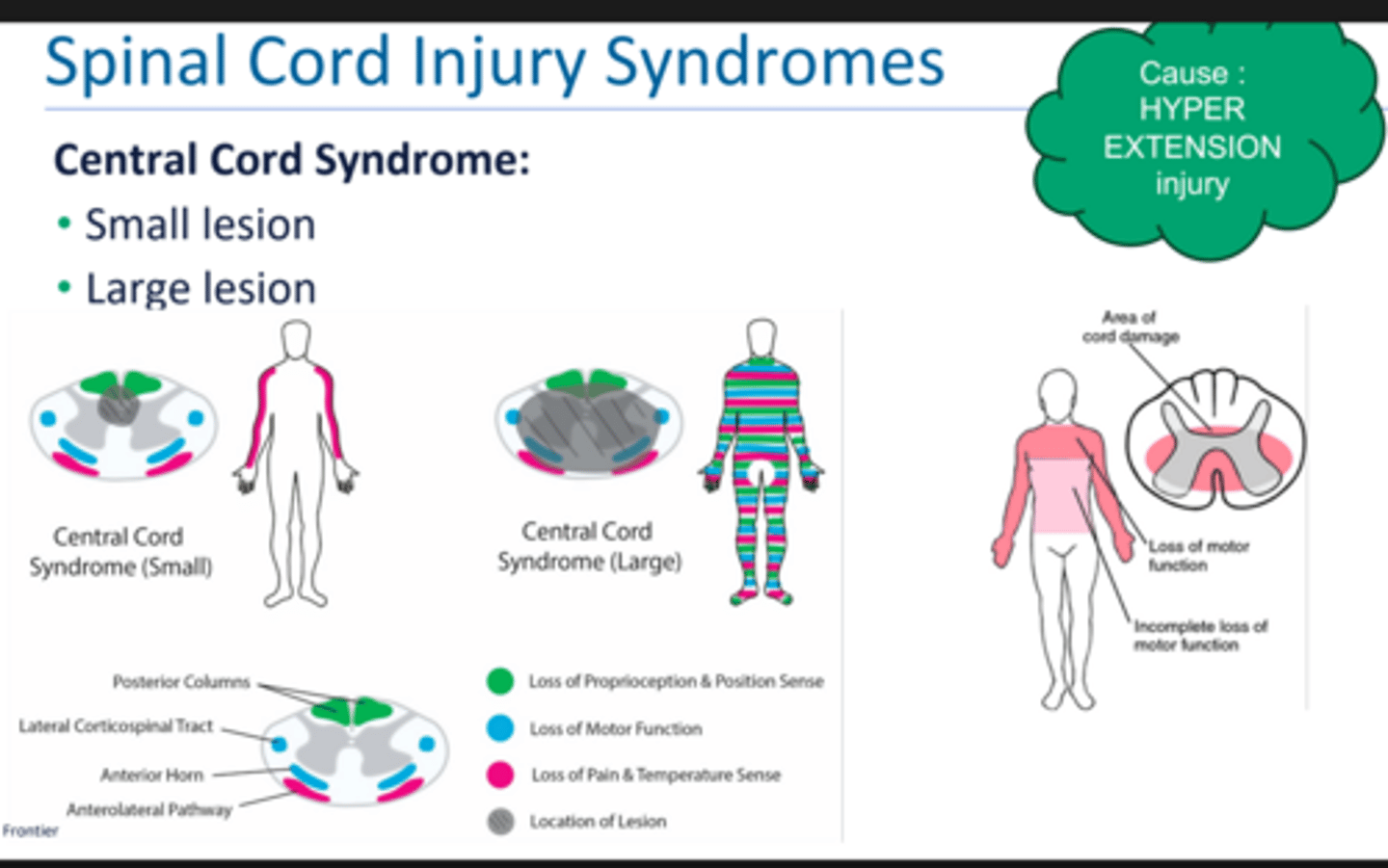
Central cord syndrome
aka walking SCI
hyperextension injury
if small lesion: bilateral pain and temp
if large lesion:
-loss of motor and sensory function
-affects motor > sensory
-affects UE > LE and proximal > distal
SAFETY RISKS BUT USUALLY CAN AMBULATE
affected tracts: spinothalamic, corticospinal, dorsal column
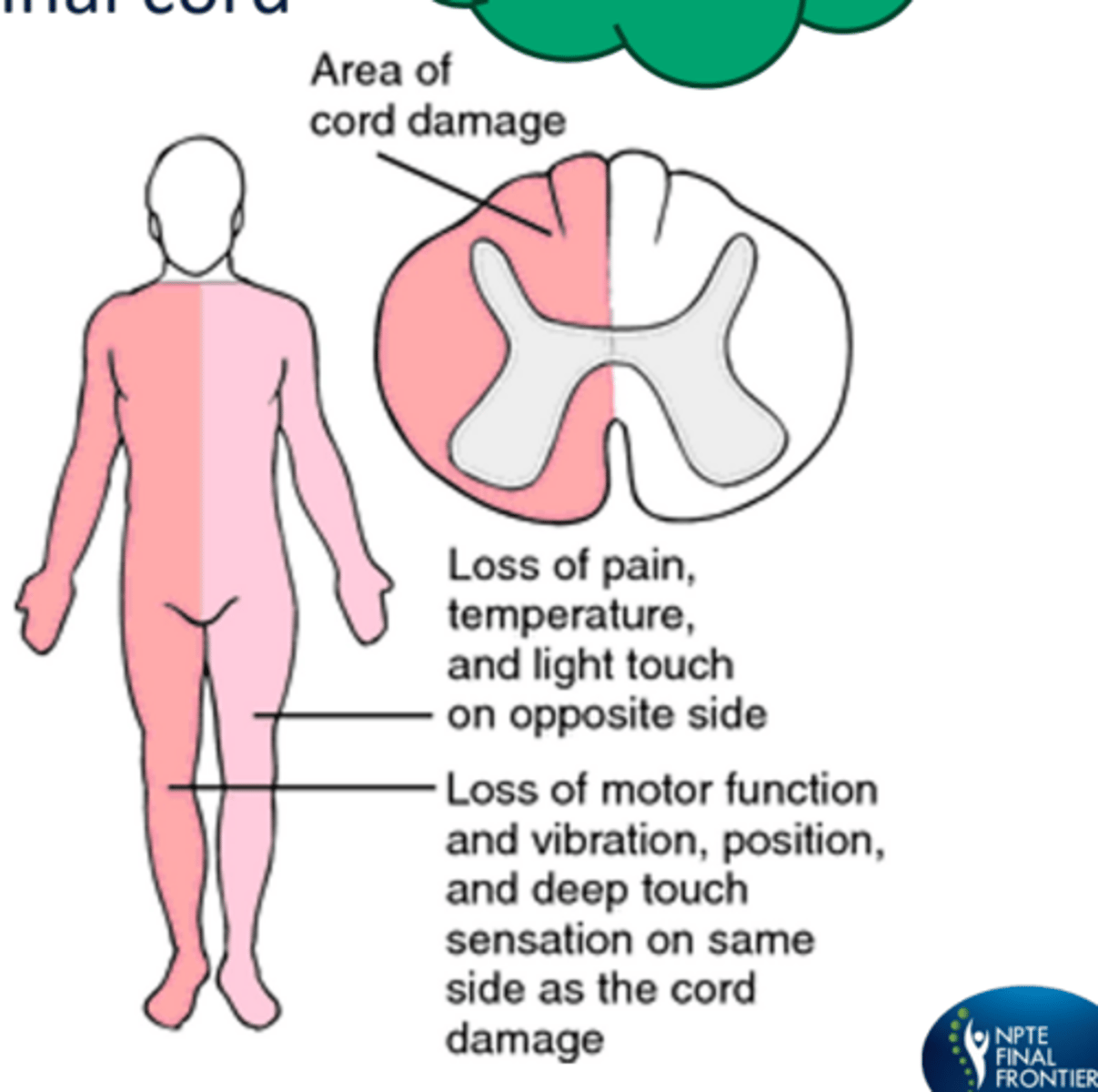
Brown-Sequard Syndrome
stab gunshot wound
-ipsilateral motor loss (corticospinal)
-ipsilateral proprioception, light touch, vibration loss (dorsal column)
-contralateral loss of pain and temperature sensation (spinothalamic)
nemonic: brown pott
Cauda equina syndrome
injury below L1
-lower extremity motor and sensory loss
-areflexic bowel and bladder and saddle anesthesia
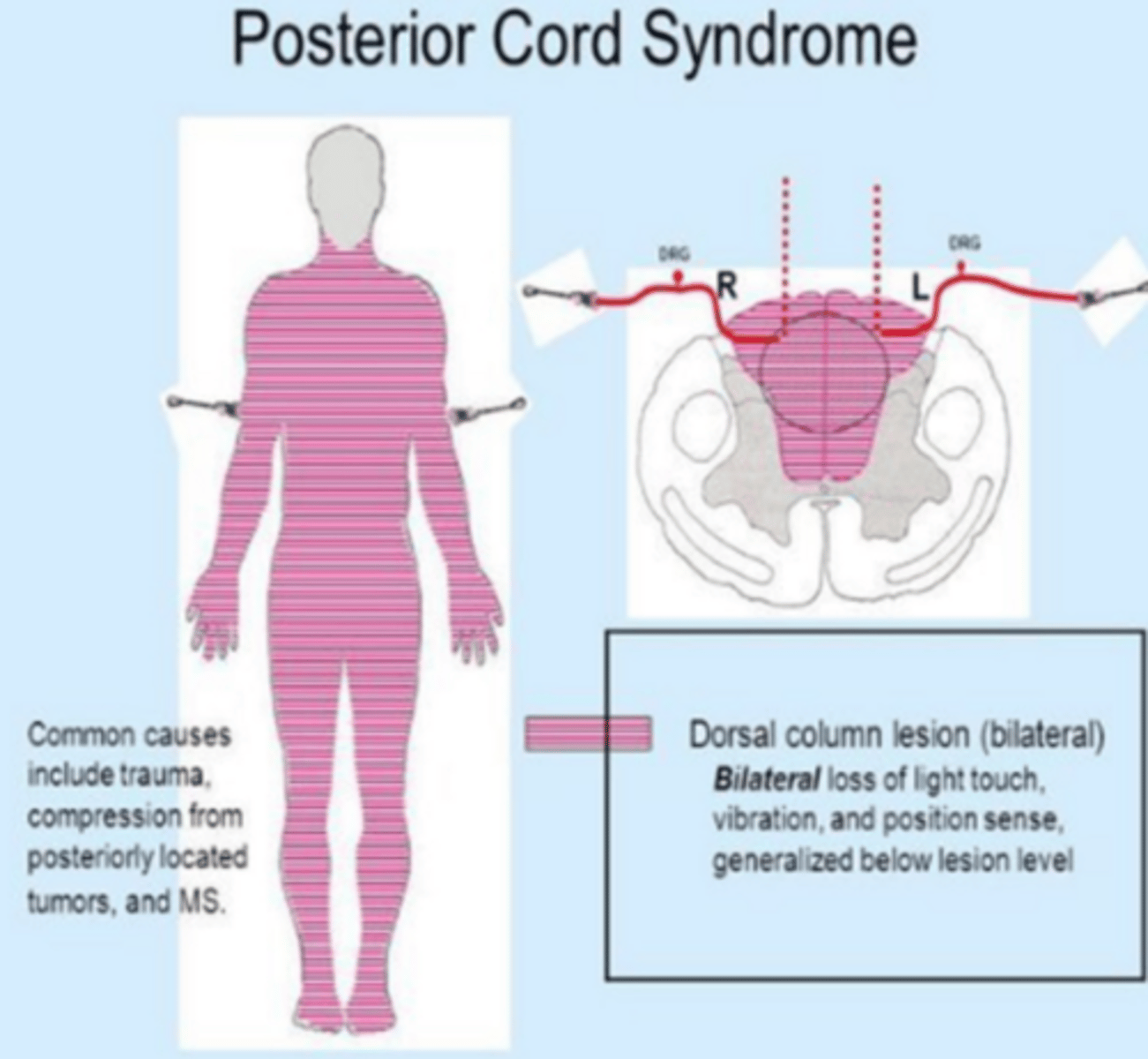
Posterior Cord Syndrome
causes: RARE iatrogenic aka medical error; compression of posterior spinal artery or (NPTE focuses on medical error) hyperextension injury
-DCML affected ... loss of vibration, proprioception, 2 point discrimination, sterognosis
-motor function is preserved
-sensory ataxia due to DCML involvement
Dorsal vs ventral horns vs intermediate
dorsal (posterior): sensory
ventral (anterior): motor
Spinal shock
transient period of reflex depression and flaccidity; can last several hours to 6. months or more
S/S: flaccid paralysis, areflexia, vasodilation, decreased cardiac output and venous pooling
-abscence of reflex activity impairs autonomic regulation, which results in hypotension and loss of ability to sweat
What reflex indicates the body is out of spinal shock?
bulbocavernosus S2-4
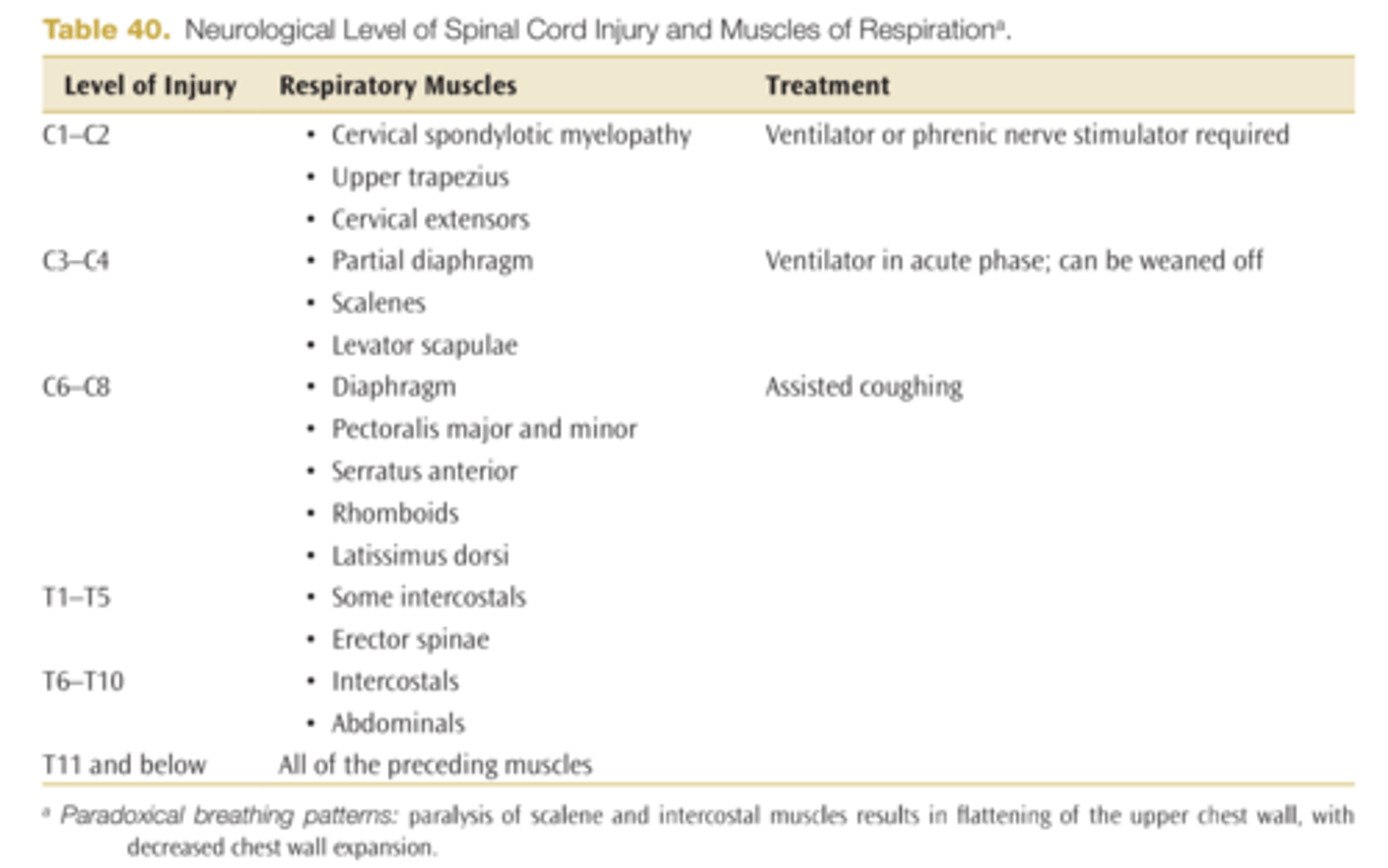
What level do you start to see respiratory function issues?
above C4
-above C3-C5 need ventilator because supplies phrenic nerve and assist diaphragm control
Below ___ patient can normally be weaned from ventilator
C4 (must teach assistive coughing to help; glossopharngeal breathing is used when diaphragm is denervated)
At ___ and below patient can learn self assisted coughing techniques
C5
Below ___ patient is likely to have near normal ventilatory respiratory functions
T10
Respiratory muscles C1-T11
Autonomic dysreflexia
occurs with injuries at or above T6 --> disruption of sympathetic response
-MEDICAL EMERGENCY
-vasoconstriction occurs leading to hypertension and decreased HR
-increased BP, decreased HR, headache, flushing, profuse sweating, anxiety, constricted pupils, blurred vision, piloerection
-systolic increases by 20-30
-vasoconstriction below level of injury and vasodilation above
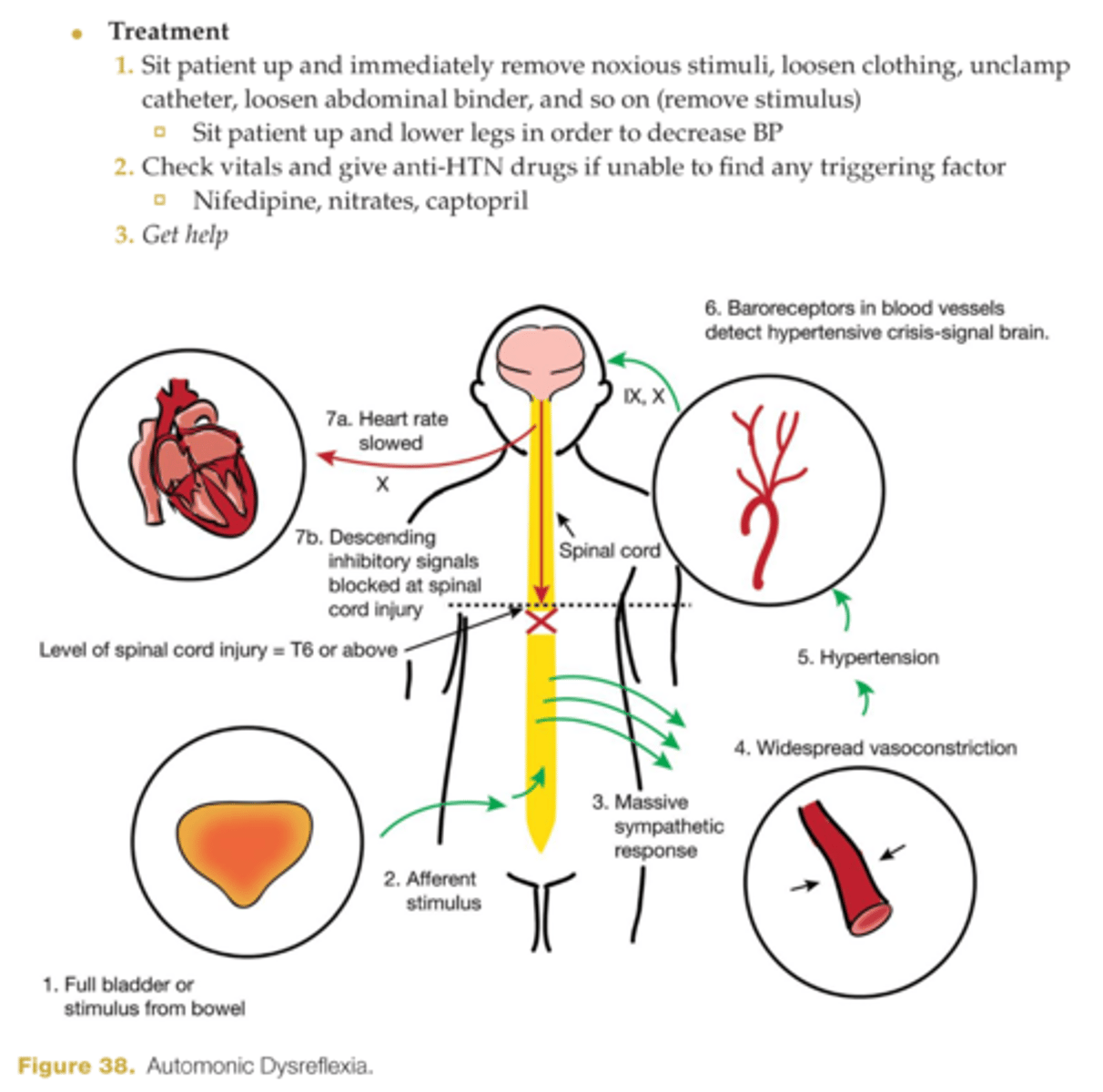
Factors that cause autonomic dysreflexia
-bowel and bladder distension, infection, impaction, catheterization blocked, abdominal binder
-skin breakdown, pressure sores, ingrown toenail, and similar stimuli
neurogenic shock
occurs with SCI above T6
-S/S: decreased BP, decreased HR, cyanosis, warm and dry extremities, decreased CO, peripheral vasodilation and venous pooling
Orthostatic hypotension seen with SCI above
T6
Spastic bladder
seen in injury above S2 sacral segment
-bladder contracts and reflexively empties in response to certain level of filling pressure
-reflex action present
-treat with intermittent cauterization every 3-6 hours
-bladder can be emptied by: manual stimulation or timed voiding schedule
Flaccid bladder
seen in injury below S2
-no reflex present
-can be emptied by: crede maneuver (manual compression of lower abdomen; valsalva; timed voiding schedule
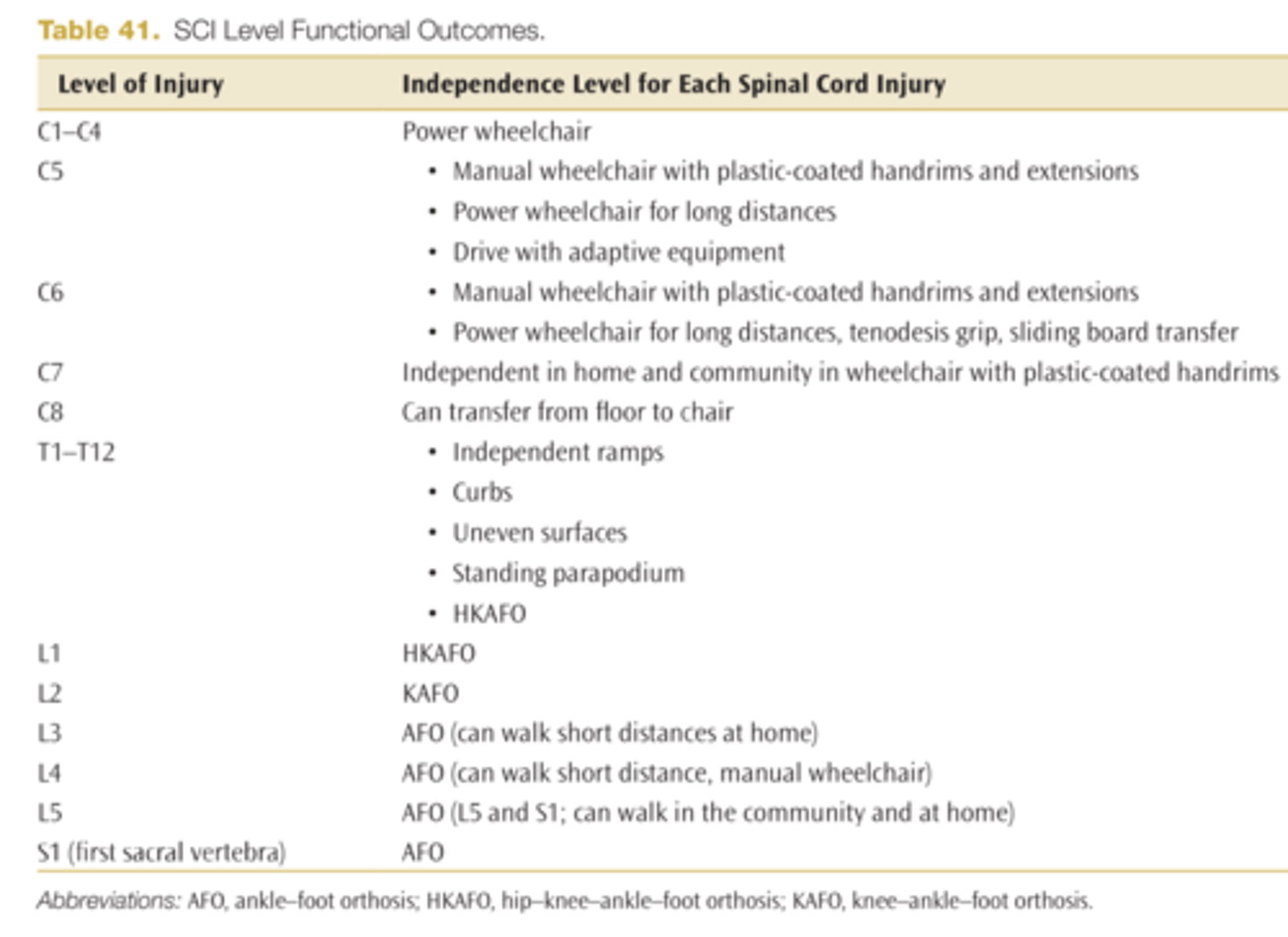
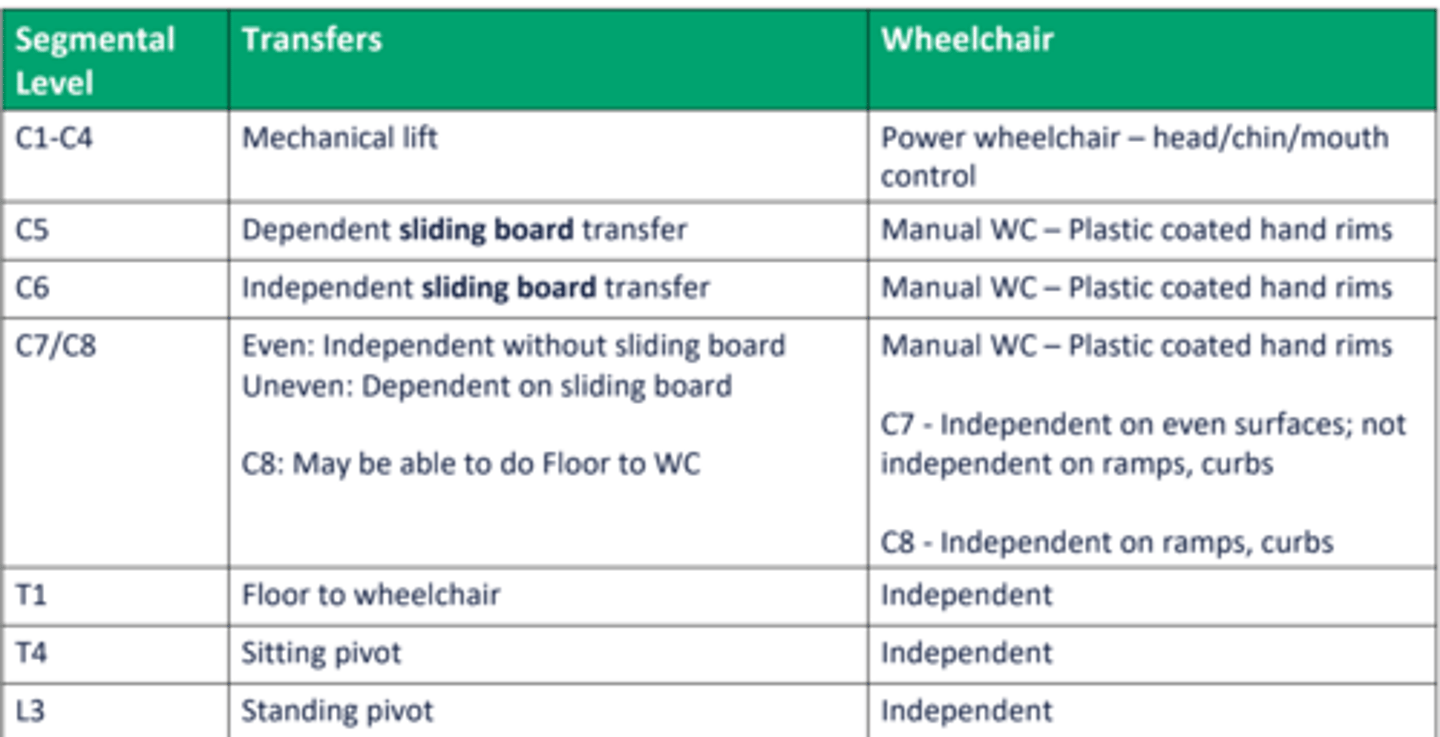
Independence level for each spinal cord injury
Heterotopic ossifications
- Common
- Generally near large joints
- No aggressive stretching!
Fasciculus cuneatus
ascending tract; sensory tract for trunk, neck, and UE proprioception, vibration, two-point discrimination, and graphesthesia
Fasciculus gracilis
ascending tract; sensory tract for trunk and LE proprioception, vibration, two-point discrimination, and graphesthesia
Spinocerebellar tract (dorsal)
ascending tract; sensory tract that ascends to the cerebellum for ipsilateral (I/L) subconscious proprioception, tension in muscles, joint sense, posture of the trunk and LEs
Spinocerebellar tract (ventral)
ascending Tract; sensory tract that ascends to the cerebellum, with some fibers crossing and subsequently recrossing at the level of the pons for I/L subconscious proprioception; tension in muscles; joint sense; and posture of trunk, UEs, and LEs
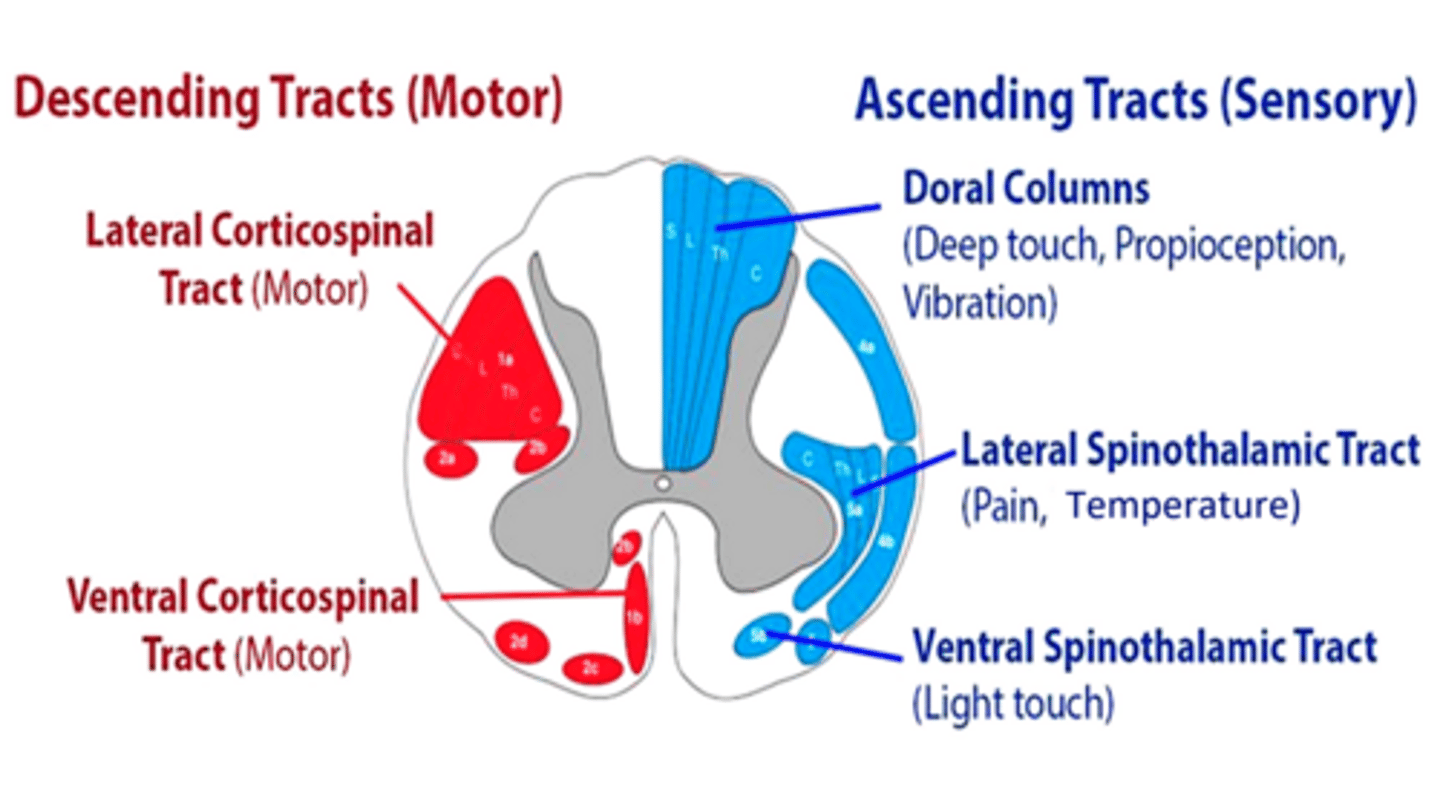
Spinothalamic tract anterior
ascending tract; sensory tract for light touch and pressure
Spinothalamic tract (lateral)
ascending tract; sensory tract for pain and temperature sensation
Corticospinal tract anterior
descending tract; pyramidal motor tract responsible for I/L voluntary, discrete, and skilled movements
Note: Damage to corticospinal (pyramidal) tracts results in a positive Babinski sign, absent superficial abdominal and cremasteric reflexes, and the loss of fine motor or skilled voluntary movement
Corticospinal tract lateral
descending tract; pyramidal motor tract responsible for C/L voluntary fine movement
Note: Damage to corticospinal (pyramidal) tracts results in a positive Babinski sign, absent superficial abdominal and cremasteric reflexes, and the loss of fine motor or skilled voluntary movement
Where does the spinal cord end?
L1 and then goes into conus medullaris then to cauda equina (we do lumbar punctures at L3-4 to avoid spinal cord injury)
Dorsal column medial leminscus (DCML)
-Proprioception
-vibration
-graphesthesia
-barognosis
-stereognosis
-2-pt discrimination
-kinesthesia
-fine touch
(poor val got GBS 2x, keep fighting)
Anterolateral system
Anterior STT: Crude touch ("did you feel it")
Lateral STT: Pain and temperature
Corticospinal tract
movements
Which tracts are ascending vs descending tracts
ascending: sensory tracts (DCML and anterolateral system)
descending: corticospinal
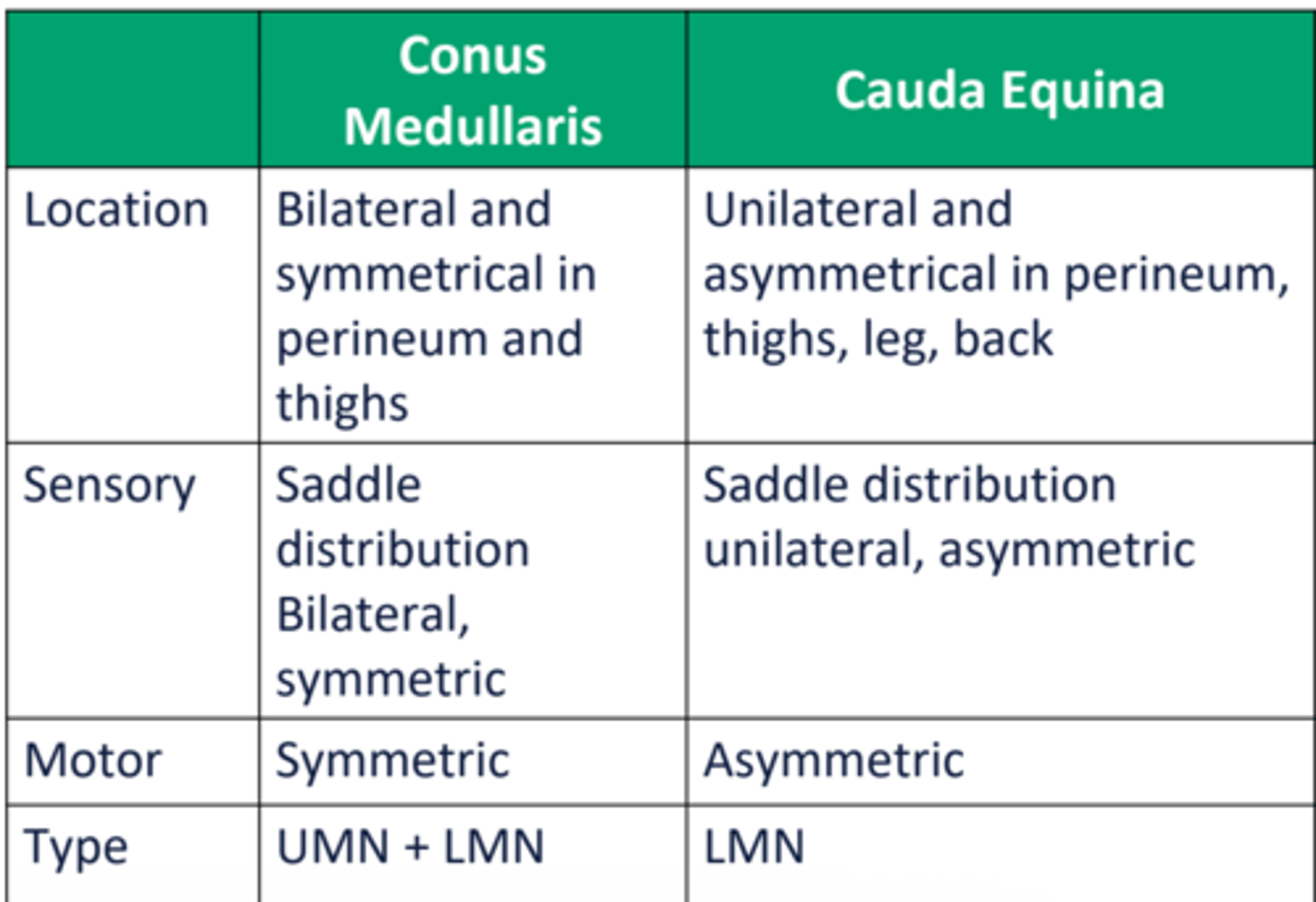
Conus medullaris vs cauda equina
conus medullariS = symmetrical
cauda equinA = asymmetrical
Complete vs incomplete SCI
complete: No sensory or motor function in the lowest sacral segments (S4 and S5)
Incomplete: Motor and/or sensory function below the neurological level including sensory and/or motor function at S4 and S5
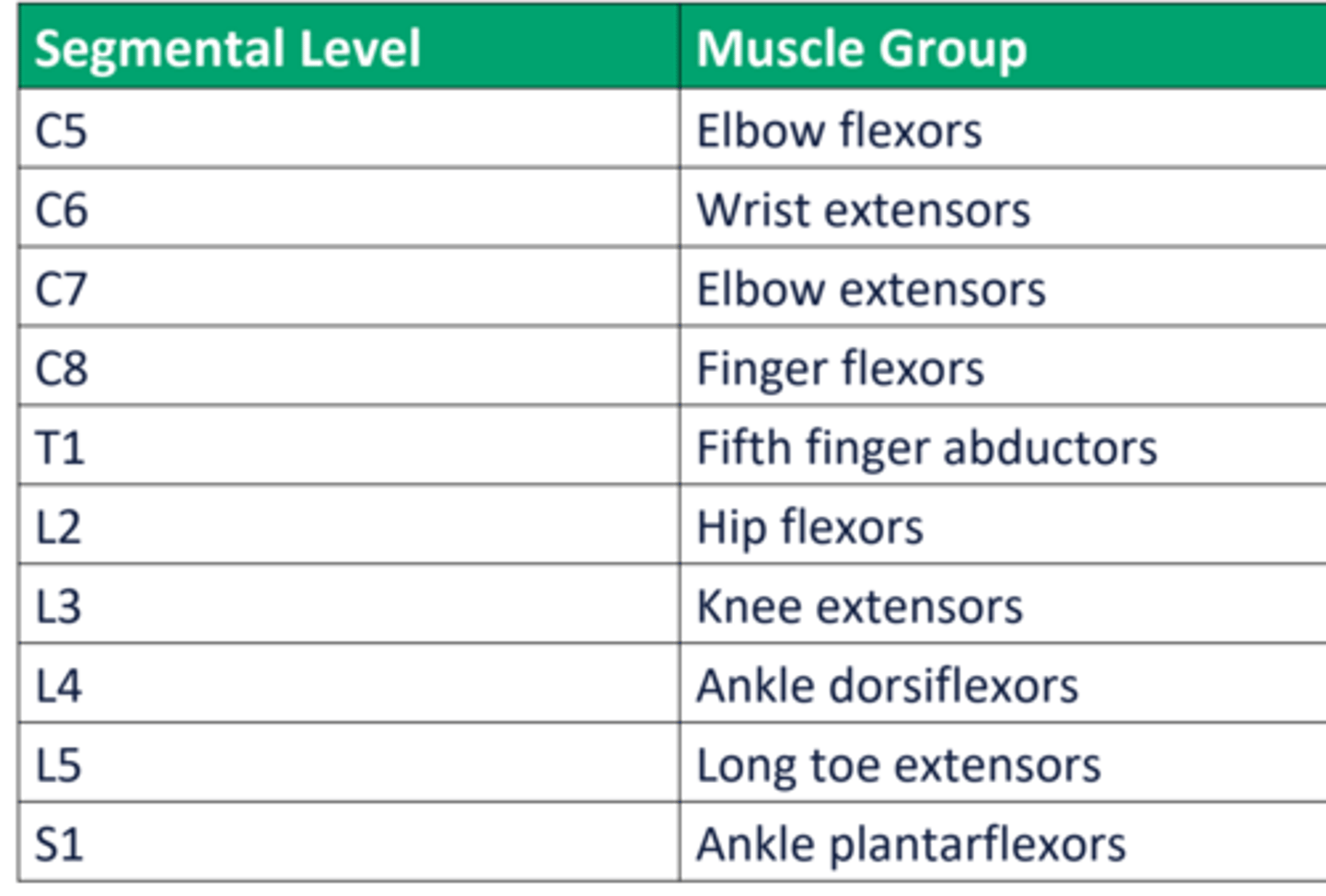
ASIA SCI assessment segmental level muscle groups C5-S1
Motor level steps
1. Lowest Level at which strength is at least
3/5
2. All levels above being 5/5
Scored for each side, overall score is last
normal for both
Sensory level steps
Defined as the level where sensory
function is normal on both sides of the
body.
Easy Steps:
1. Lowest level where you have "2's"
2. All above levels being "2's"
(0 is no sensation; 1 is present/impaired, 2 is normal)
Neurological level
CAUDAL most level with NORMAL
sensory and motor function on
BOTH sides of the body.
Easy Steps:
1. Find Motor and Sensory level
2. Pick the higher one
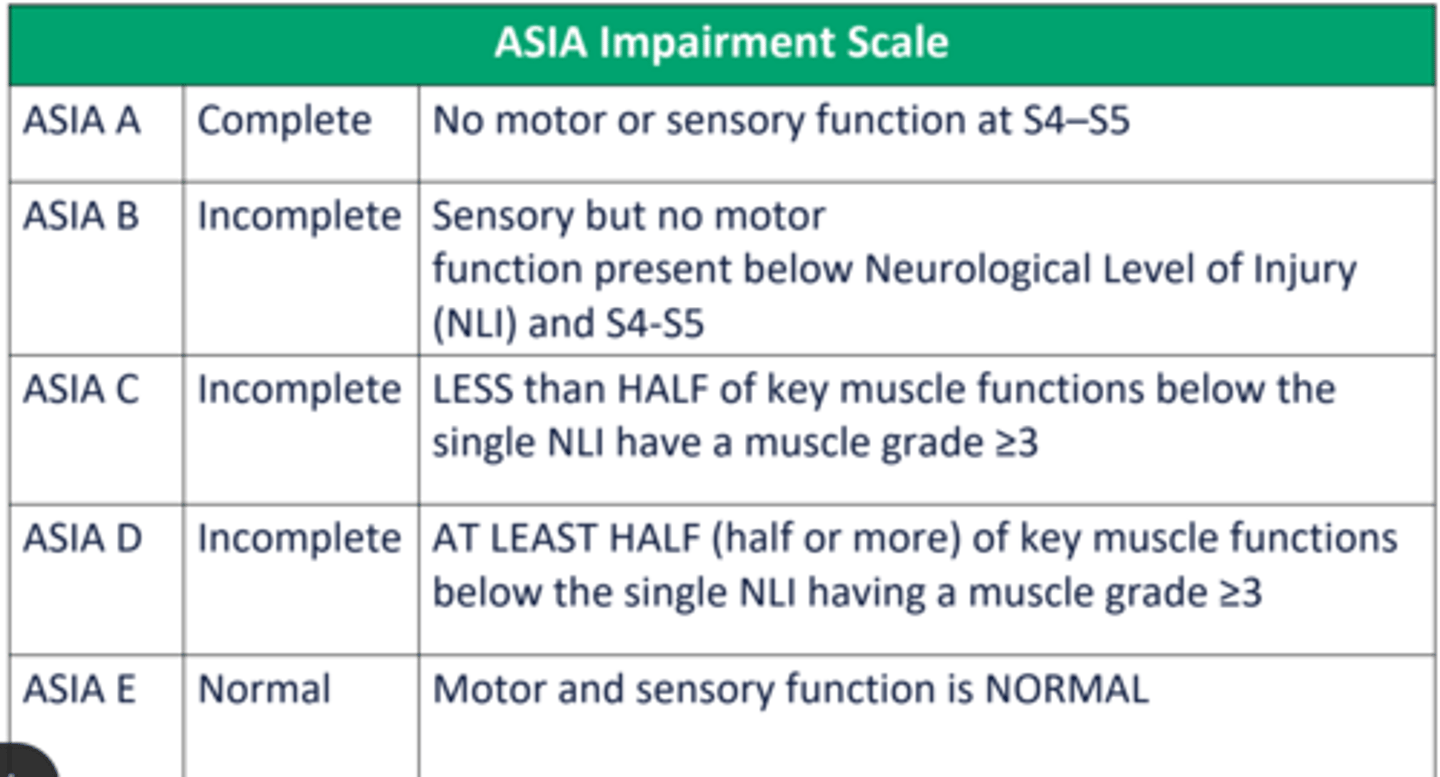
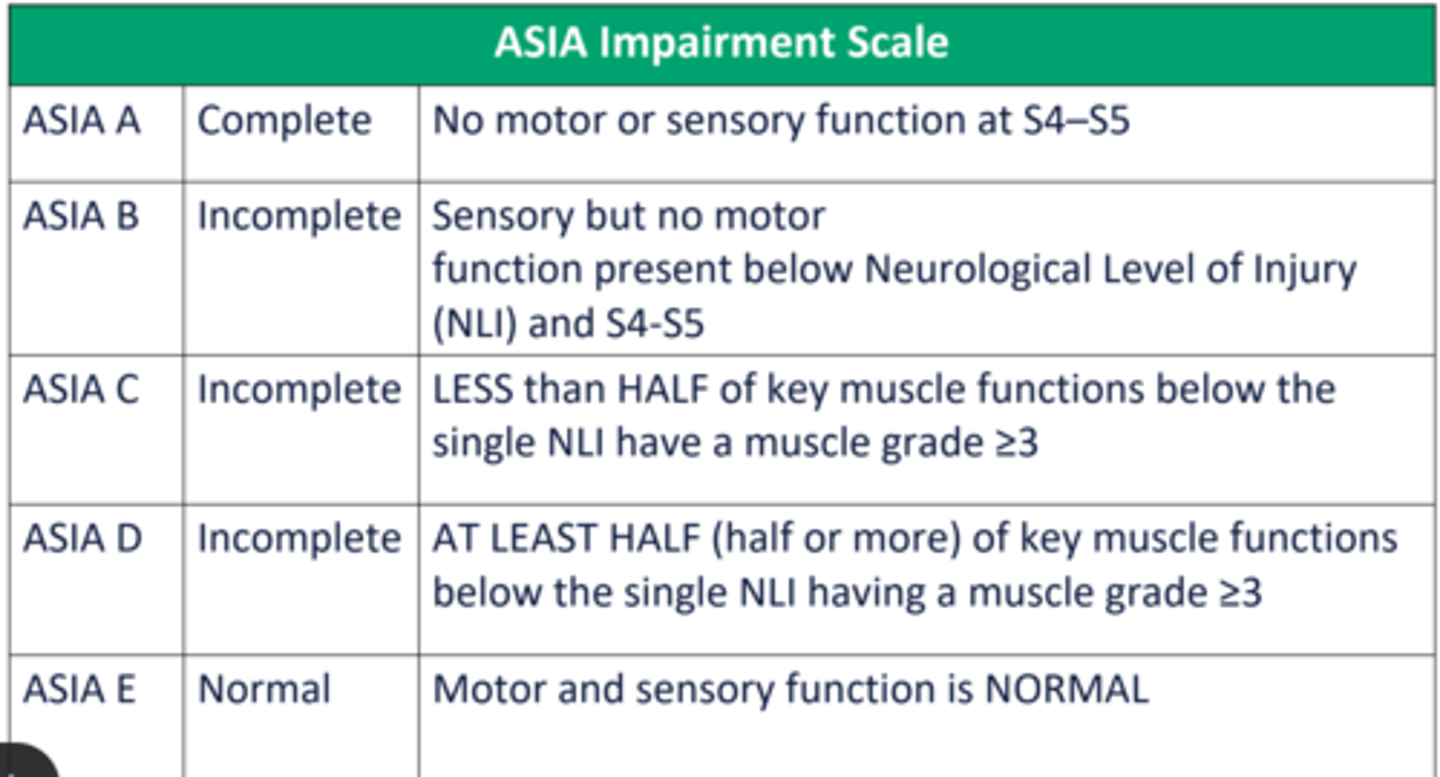
ASIA A-E scale
ASIA C: more than half have a grade less than 3/5
Autonomic dysreflexia/hyperreflexia causes and signs/symptoms
• At or above T6
• Noxious stimuli below level of lesion
• Rise in systolic blood pressure of 20 to 30 mmHg is diagnostic of an episode of autonomic dysreflexia
• More common in chronic stage (3-6 months after injury); can be seen in acute too
• More common with complete SCI
What to do with autonomic dysreflexia
• SIT UP and LOWER LEGS
• Remove painful stimuli:
̶Loosen clothing, abdominal binder
̶CHECK BLADDER distension: Unclamp catheter, drain it
• Monitor vitals throughout: If still no change, medical/nursing
assistance > meds to lower BP (Nifedipine, nitrates, and captopril)
Functional level C1-L3 transfers vs WC/ambulation ability
look at chart with spinal cord injury functions
Diaphragm innervation
C3,4,5 keep the diaphragm alive
C4 can be off ventilator if they do
glossopharyngeal breathing