Clinical Psychology Master Set
1/124
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
125 Terms
What is statistical infrequency (SI)?
The fewer times we see something, the less normal we perceive them to be ∴ uncommon is seen as abnormal.
AO3 of statistical infrequency
Strengths:
RWA: Useful part of clinical assessment
Weaknesses:
Unusual characteristics can be positive
Labelling can be harmful. If someone is living happily, labelling them as abnormal won’t help them, regardless of how abnormal they are.
Deviation from social/cultural norms
When a person strays from acceptable behaviour, and is therefore labelled as abnormal
What is the DSM-V ASA?
Diagnostic and Statistical Manual of Mental Disorders- Fifth Edition, The American Psychological Association
What is failure to function adequately? (FFA)
Circumstances where a person can no longer face the demands of everyday life
Signs of FFA (Rosenhan & Seligman 1989)
No longer conforming to standard interpersonal rules
Severe personal distress
Behaviour becomes irrational/dangerous to themselves or others
AO3 of FFA
Strengths:
Acknowledges the patient’s perspective, also captures the experience of many people who need help- suggesting it’s useful in assessing abnormality
Weaknesses:
Is it simply a deviation from social norms?
Subjective. Someone has make a judgement on whether or not the patient is functioning adequately.
Criteria for Ideal mental health (Marie Jahoda 1958)
No symptoms of distress
Rational and able to perceive ourselves accurately
We self-actualise
We can cope with stress
We have a realistic view of the world
We have good self-esteem and lack of guilt
We are independent of other people
We can successfully work, love, and enjoy our leisure time
AO3 of Criteria for ideal mental health
Strengths:
It’s a comprehensive definition: Covers a broad range of criteria for mental health, likely covers most of the criteria someone would seek mental health for
Weaknesses:
Cultural relativism
Subjective
Sets an unrealistically high standards for mental health
What is a phobia?
An irrational fear of an object or situation that evokes a biological response.
What categories of phobia and related anxiety disorders are recognised in the DSM-V?
Specific Phobia: Object, animal, body part, situation
Social Anxiety: Social situations
Agoraphobia: Outside, public places
DSM-V Diagnostic features of phobias
Intense, persistent, irrational fear of a particular object, event, or situation
Response is disproportionate and leads to avoidance
Fear is severe enough to interfere with functioning
Condition may or may not be accompanied by panic attacks
Behavioural characteristics of phobias
Panic: Crying, screaming, running away
Endurance: stays, but with very high levels of anxiety
Avoidance: Limit on what they can do, often involves changing routine/action
Emotional Characteristics of phobias
Anxiety: Unpleasant state of high arousal. Prevents relaxation and positive emotion.
Fear: Immediate, extremely unpleasant response we feel.
Cognitive Characteristics of phobias
Selective attention: PS is hard to look away from
Irrational beliefs: Will hold irrational beliefs in relation to PS
Cognitive distortion: The sufferer’s perception of the stimulus is distorted (bigger than reality)
Behaviourist Approach to explaining phobias
Emphasises role of learning in the acquisition and maintenance of behaviour- PEA
Mowrer’s Two-Process Model (TPM) (1960)
Phobias are acquired via classical conditioning (Neutral Stimulus + Fear) and maintained through operant conditioning (Negative Reinforcement through Avoidance)
AO3 of Mowrer’s TPM
Strengths:
Real World Application: The model led to effective behavioural therapies, such as SD and flooding
Internal Validity: CC and OC’s mechanisms are easily observable and testable in controlled conditions.
Weaknesses:
Ignores Cognition: Only focuses on behaviour, ignoring cognitive aspects like irrational thoughts or cognitive distortions that contribute to phobias, which Cognitive Behavioural Therapy (CBT) often addresses better.
Reductionist/Deterministic: Reduces complex human behaviour to simple stimulus-response mechanisms and assumes all, or at least many, traumatic events lead to phobias, which is not true
What are the two behavioural treatments of phobias?
Systemic Desensitisation (SD)
Flooding
What is Systemic Desensitisation?
Counter-Conditioning to unlearn the maladaptive response to the phobia
What are the 3 components of SD?
Fear Hierarchy
Relaxation Training
Exposure
What are the DETAILS of the components/steps in SD?
Establish Anxiety Hierarchy
C+T (Client and Therapist) rank phobic situations from least to most terrifying/anxious
Relaxation Techniques
C taught relaxation techniques, such as breathing exercises and mental imaging techniques.
Can also use drugs such as Valium
According to SD, you cannot be both relaxed and anxious at once, so the relaxation will eventually take over.
Exposure
C is exposed to phobic stimulus while in relaxed state
Takes place over several sessions
Finished when relaxed in all stages
AO3 of SD
Strengths:
Gilroy et al Arachnophobia study (ADD MORE DETAIL)
SD is suitable for a diverse range of participants. Alts aren’t always suitable, e.g, if a C has a learning disability and can’t rationalise flooding
Less traumatic than flooding. Relaxation techniques can be enjoyable
Weaknesses:
Time consuming and costly
What is flooding?
Patient cannot escape their phobia through continuous exposure, wait until anxiety decreases. More extreme than SD. (Shove someone in a room full of clowns and hope for the best- Don’t write that, though)
What are the two types of flooding?
In Vivo- Actual, real life exposure
In Vitro- Imaginary Exposure
What is a phobia?
An irrational fear of an object or situation that evokes a biological response. It is also severe enough to interfere with functioning.
What categories of phobia and related anxiety disorders are recognised in the DSM-V?
Specific Phobia: Object, animal, body part, situation
Social Anxiety: Social situations
Agoraphobia: Outside, public places
DSM-V Diagnostic features of phobias
Intense, persistent, irrational fear of a particular object, event, or situation
Response is disproportionate and leads to avoidance
Fear is severe enough to interfere with functioning
Condition may or may not be accompanied by panic attacks
Behavioural characteristics of phobias
Panic: Crying, screaming, running away
Endurance: stays, but with very high levels of anxiety
Avoidance: Limit on what they can do, often involves changing routine/action
Emotional Characteristics of phobias
Anxiety: Unpleasant state of high arousal. Prevents relaxation and positive emotion.
Fear: Immediate, extremely unpleasant response we feel.
Cognitive Characteristics of phobias
Selective attention: PS is hard to look away from
Irrational beliefs: Will hold irrational beliefs in relation to PS
Cognitive distortion: The sufferer’s perception of the stimulus is distorted (bigger than reality)
Behaviourist Approach to explaining phobias
Emphasises role of learning in the acquisition and maintenance of behaviour- PEA
Mowrer’s Two-Process Model (TPM) (1960)
Phobias are acquired via classical conditioning (Neutral Stimulus + Fear) and maintained through operant conditioning (Negative Reinforcement through Avoidance)
AO3 of Mowrer’s TPM
Strengths:
Real World Application: The model led to effective behavioural therapies, such as SD and flooding
Internal Validity: CC and OC’s mechanisms are easily observable and testable in controlled conditions.
Weaknesses:
Ignores Cognition: Only focuses on behaviour, ignoring cognitive aspects like irrational thoughts or cognitive distortions that contribute to phobias, which Cognitive Behavioural Therapy (CBT) often addresses better.
Reductionist/Deterministic: Reduces complex human behaviour to simple stimulus-response mechanisms and assumes all, or at least many, traumatic events lead to phobias, which is not true
What are the two behavioural treatments of phobias?
Systemic Desensitisation (SD)
Flooding
What is Systemic Desensitisation?
Counter-Conditioning to unlearn the maladaptive response to the phobia
What are the 3 components of SD?
Fear Hierarchy
Relaxation Training
Exposure
What are the DETAILS of the components/steps in SD?
Establish Anxiety Hierarchy
C+T (Client and Therapist) rank phobic situations from least to most terrifying/anxious
Relaxation Techniques
C taught relaxation techniques, such as breathing exercises and mental imaging techniques.
Can also use drugs such as Valium
According to SD, you cannot be both relaxed and anxious at once, so the relaxation will eventually take over.
Exposure
C is exposed to phobic stimulus while in relaxed state
Takes place over several sessions
Finished when relaxed in all stages
AO3 of SD
Strengths:
Gilroy et al (2003) Arachnophobia study
Found that those who underwent 3×45 min SD sessions were more relaxed than those who were only taught relaxation techniques when faced with a spider/ spider questionnaire.
SD is suitable for a diverse range of participants. Alts aren’t always suitable, e.g, if a C has a learning disability and can’t rationalise flooding
Less traumatic than flooding. Relaxation techniques can be enjoyable
Weaknesses:
Time consuming and costly
What is flooding?
Patient cannot escape their phobia through continuous exposure, wait until anxiety decreases. More extreme than SD. (Shove someone in a room full of clowns and hope for the best- Don’t write that, though)
What are the two types of flooding?
In Vivo- Actual, real life exposure
In Vitro- Imaginary Exposure
What is OCD?
A condition characterised by obsessions and/or compulsions.
Obsessions= cognitive
Compulsions= behavioural
Symptoms of OCD
Repetitive intrusive thoughts, anxiety reducing behaviours.
How common is OCD?
2% of population
DSM-V OCD
The DSM-V recognises OCD and a range of related disorders. What the disorders all have in common is repetitive behaviour accompanied by obsessive thinking:
Related disorders:
Trichotillomania
Hoarding Disorder
Excoriation disorder
What is Trichotillomania
When someone can't resist the urge to pull out their hair.
Hoarding Disorder
A persistent difficulty discarding or parting with possessions because of a perceived need to save them. A person with hoarding disorder experiences distress at the thought of getting rid of the items. Excessive accumulation of items, regardless of actual value, occurs.
What is Excoriation disorder
A mental illness related to obsessive-compulsive disorder. It is characterized by repeated picking at one's own skin which results in skin lesions and causes significant disruption in one's life (also referred to as chronic skin-picking or dermatillomania)
OCD Cycle
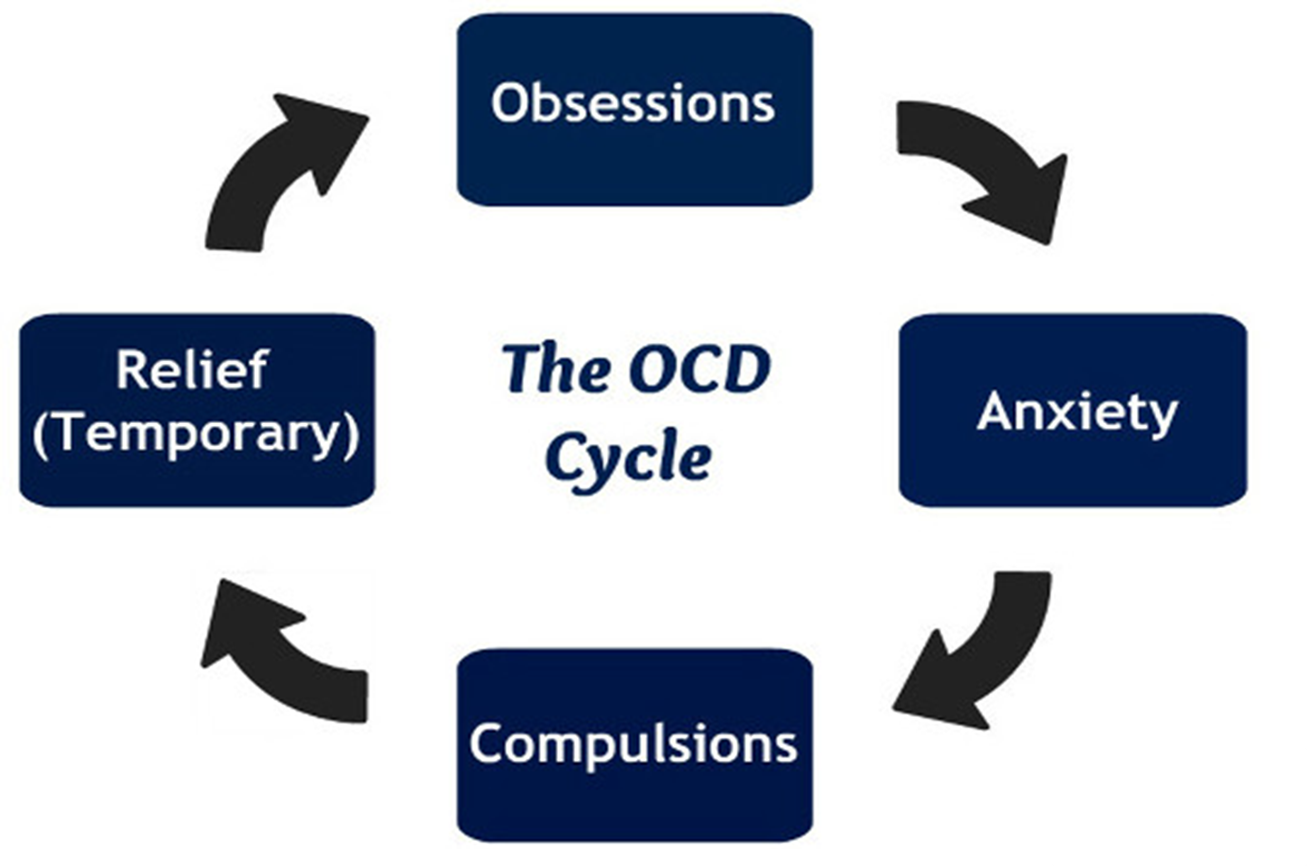
What are compulsions?
Unwelcome thoughts, images, urges, worries or doubts that repeatedly appear in your mind. They can make sufferers feel very anxious or uncomfortable.
Behavioural Characteristics of OCD
Compulsions are repetitive: Suffers feel compelled to repeat behaviours e.g. handwashing, praying, tidying, ordering items.
Compulsions reduce anxiety: Compulsive handwashing is carried out as a response to an obsessive fear of germs. Therefore compulsions are seen to manage to sufferers’ anxiety.
Emotional Characteristics of OCD
Anxiety and Distress: The urge to repeat a behaviour creates overwhelming anxiety. Obsessive thoughts are unpleasant and frightening.
Accompanying Depression: OCD is often comorbid with depression so there is also likely to be low mood and anhedonia.
Guilt and Disgust: Sometimes OCD involves emotions such as irrational guilt e.g. for example over minor moral issues, or disgust which may be directed against something external like dirt or at the self.
Cognitive Characteristics
Obsessive thoughts: Thoughts that recur over and over again. They vary from the person to person but are always unpleasant and maladaptive. e.g. the door was left unlocked.
Cognitive strategies to deal with obsessions: For example, a religious person tormented by guilty may respond to praying or meditating. This may help the person but will look abnormal to others.
Insight into excessive anxiety: OCD sufferers are aware their obsessions and compulsions are irrational. OCD sufferers experience catastrophic thoughts about the worse case scenarios that might occur if their anxieties were justified.
Family Studies of OCD
Lewis (1936) found that 37% of OCD patients had parents with OCD and 21% had Siblings with OCD.
This suggests OCD is passed on in genetic vulnerability, not certainly
According to the diathesis-stress model, Certain gever leave Some people more villnerable to Supper a mental disorder, but it's not certain - some environmental stressor is recassary. to trigger it.
Candidate genes (Lewis 1936)
Researchers have identified genes, which reale vulnerability for OCD, called candidate genes.
Some of these genes are involved in regulating the development of the seratonin systemic.
OCD is Polygenic
This means that OCD is not caused by one sole gene, but several genes are involved
Taylor (2013) analysed the findings of previous studies and found evidence that of may up to 230 genes involved. These genes related to the the action of dopamine and serotonin- both have roles in regulating mood
Different types of OCD Explanation
OCD is aetiologically heterogenous, meaning the origin (aetiology) of OCD has different causes (heterogenous)
There is also some evidence to suggest that different types of OCD variations may be the result of particular genetic variations
The role of Serotonin
Low levels of serotonin impact the normal transmission of mood-relevant information, leading to difficulties in emotional regulation and cognitive processes such as memory and decision-making.
Decision-making systems
Some cases of OCD seem to be associated with impaired decision making.
This may be associated with the with abnormal functioning on the lateral of samtal lobe in the brain.
There is also evidence that an area called the left parahippocampal gyrus functions abnormally in OCD.
Twin Studies
Nestadt et al. (2010) reviewed previous studies. and found that 68% of Identical twins shared OCD as opposed to 31% of non-identical twins
Limitation of candidate genes
For many candidate genes Carnot fin down all genes involved (atm) Only increase OCD risk fractionally
Environmental risk factors.
Cromer et al. 2007 found that over half the OCD patients in their sample had a traumatic event in their past, and that OCD was more severe in these with multiple traumas.
Limitations of environmental risk factors
Not a full explanation, not entirely genetic in nature
Supporting evidence of the biological explanation
Some anti-depressants are effective in reducing OCD symptoms, suggesting Serotonin is involved:
Also, OCD symptoms form a part of a number of other conditions are biological in nature e.g Parkinson’s (Nestadt et al 2010)
Limitations of the biological explanation
Not clear exactly what neural mechanisms are involved. (Should not assume neural conditions cause OCD)
The serotonin OCD link may simply be Co- morbidity with depression.
Strengths of the biological explanations
One of the best sources of evidence for the importance of genes is twin studies. Nestadt et al. (2010) reviewed previous studies and found that 68% of identical twins shared OCD as opposed to 31% of non-identical twins.
Limitations of the biological explanation
Although twin studies strongly suggest that OCD is largely under genetic control, psychologists have been much less successful at pining down all the genes involved. One reason for this is because it appears that several genes are involved and that each genetic variation only increases the risk of OCD by a fraction.
It seems that environmental factors can also trigger or increase the risk of developing OCD (the diathesis-stress model). For example, Cromer et al. (2007) found that over half the OCD patients in their sample had a traumatic event in their past, and that OCD was more sever in those with more than one trauma.
Strengths of the neural explanations
There is evidence to support the role of some neural mechanisms in OCD. For example, some antidepressants work purely on the serotonin system, increasing levels of this neurotransmitter. Such drugs are effective in reducing OCD symptoms and this suggests that the serotonin system is involved in OCD. Also, OCD symptoms form part of a number of others conditions are biological in nature Parkinson's Disease (Nestasdt et al., 2010).
Limitations of the neural explanation
Studies of decision making have shown that these neural systems are the same systems that function abnormally in OCD (Cavedini et al. 2002). However, research has also identified other brain systems that may be involved sometimes but no system has been found that always plays a part in OCD.
There is evidence to suggest that various neurotransmitters and structures of the brain do not function normally in patients with OCD. However, this is not the same as saying that this abnormal functioning causes the OCD.
Drug Therapy
Drug therapy aims to increase or decrease, levels of neurotransmitters, which increase or decrease certain behaviours. Low levels of serotonin are associated with OCD.
Drug treatments work to increase serotonin levels
What does SSRI stand for?
Selective Serotonin Reuptake Inhibitor
SSRIs
Most commonly used antidepressants to treat OCD
SSRI's work by Mocking (or inhibiting) reuptake.. meaning more serotonin is available to pass wee angers between nearby neurons.
Prevents it from being reabsorbed into the sending cell
Can take 3-4 months to have any real impact on symptoms
Fluoxetine is a key SSRI
Combining SSRIS & other treatments
Often used alongside CBT
Drugs help reduce symptoms, increasing engagement with CBT
Some patients respond best to CBT alone, whilst others benefit more from drug like Fluoxetine
Ocaissonally, other dogs are prescribed alongside SSRIS
Alternatives to SSRIS
If SSRIs aren't working, it can be combined with Tricyclics & & Clomipramine. e.g. Clomipramine
These have more severe side effects
SNRIs aka Serotonin-noradrenaline reuptake Inhibitors
New, Same effects as SSRI
Strengths
Soomro et al. (2009) reviewed studies which compared SSRIs to placebos when treating OCD. All 17 studies showed better results for the SSRIs than the placebos. Effects are even greater when the SSRIS are combined with other forms of treatment like CBT. Typically symptoms decline for 70% of those taking SSRIS. Of remaining 30%, alt drugs and psych. treatments are likely to be effective.
Drug treatments are cheaper than other psychological treatments. Using drugs to treat OCD is therefore good value for a public health system. + when compared to other drugs, SSRIs are also non-disruptive to patients' lives. For some patients, they can take drugs until they feel better without the need to engage with the hard work needed for other forms of therapy like CBT.
Limitations
Although drugs can be helpful, a significant minority will get no benefit. Some also suffer side-effects. For example, those taking Clomipramine, side-effects are more common and can be more serious. More than 1- in-10 patients suffer erection problems, tremors and weight gain. More than 1-in- 100 become aggressive and suffer disruption to blood pressure and heart rhythm.
OCD is widely believed to be biological in origin therefore it makes sense that treatments are biological. However, some forms of OCD can have a range of other causes i.e. whereby OCD is a response to a traumatic life event.
Although, SSRIs are fairly effective and any side-effects will probably be short term, like all drug treatments they have some controversy attached. For example, some psychologists believe the evidence favouring drug treatments is biased because the research is sponsored by drug companies who do not report all the evidence (Goldacre, 2012).
Assumptions of Cognitive Treatments
Faulty thinking and thought processes make a person vulnerable to depression.
Steps in CBT
Initial assessment
Goal setting
Identifying negative/irrational thoughts and challenging these using either:
Using Beck’s cognitive therapy
Ellis’s REBT
Homework e.g. record how they feel about a given situation
CBT Cycle

Initial Assessment and Goal Setting
Starts with assessment in which client and therapist work together to clarify the patient’s problems, identify goals for the therapy create a plan to achieve them.
One of the central tasks of CBT is to identify negative or irrational thoughts that will benefit from being challenged.
CBT involves working to change negative and irrational thoughts and finally put more effective behaviours into place. Some CBT therapists do this using techniques purely from Beck’s cognitive therapy, or some rely exclusively on Ellis’s rational emotive behaviour therapy. Most draw on both.
Beck’s Negative Triad
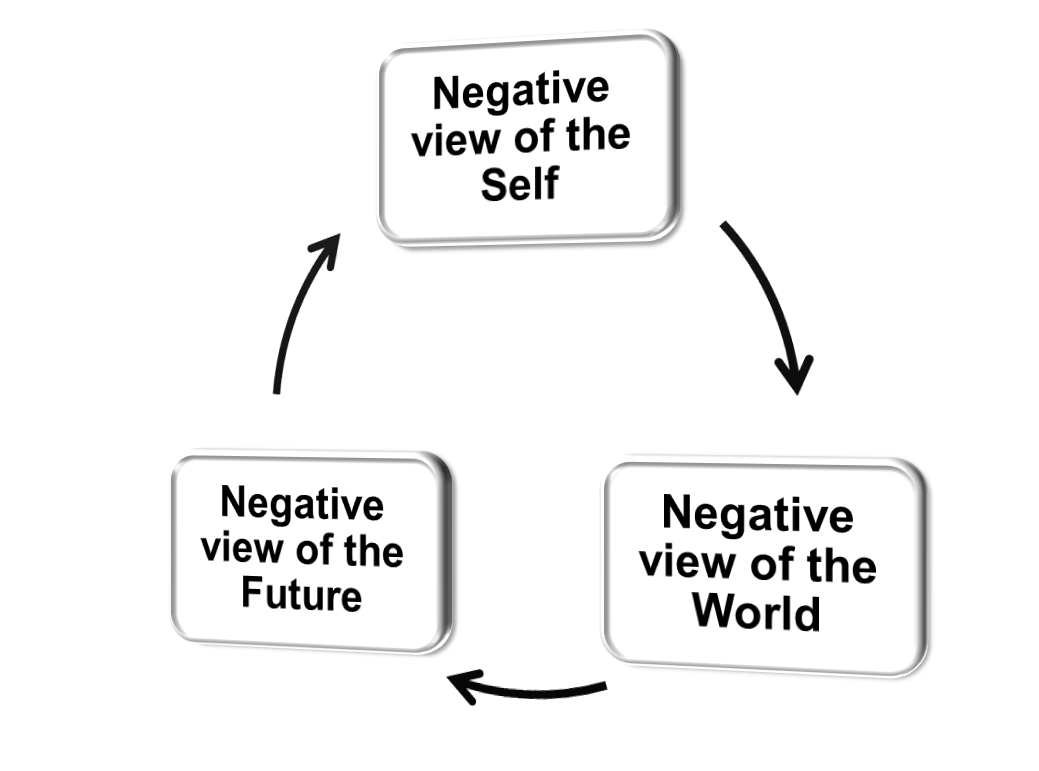
Beck’s cognitive triad can be used to test the reality of their negative beliefs.
Negative Triad in CBT
The therapist will help the patient to identify negative thoughts in relation to themselves, their world and their future, using Beck’s negative triad.
The patient and therapist will then work together to challenge these irrational thoughts, by discussing evidence for and against them.
Ellis’ REBT
Based on idea that many problems are the result of faulty thinking.
Self defeating habits → faulty beliefs about themselves and the world around them.
The method can be said to be more confrontational than Beck’s by challenging the clients self defeating beliefs in intense debates.
Ellis’ ABC Model (1962)
A = Activating Agent
B = Belief
C = Consequence (rational- healthy emotions)-(irrational-unhealthy emotions)
Strengths of Ellis’ ABC Model
Recognises Complexity also important.
Effective in treatment.
Individual Control.
Limitations of Ellis’ ABC Model
Narrow explanations.
Blames the patient rather than Situational factors.
Unclear Cause & effect
Not all rational beliefs are irrational
Alloy & Abrahamson: depressive realists see things for what they are, and aren’t necessarily irrational
Extension of REBT
ABCDE Model:
D= Dispute. Such as an empirical or logical debate.
E= Effect. New beliefs replace irrational ones.
Supporting Case study for Beck’s CBT
March et al. (2007) compared CBT, antidepressants and a combination of the two for treating depression in 327 teenagers with a main diagnosis of depression.
After 36 weeks:
81% of the CBT group were significantly improved
81% of the antidepressants group were significantly improved
86% of the CBT + antidepressants group were significantly improved.
Limitations of CBT
Depression can be so severe that patients can’t motivate themselves to engage with the hard cognitive work of CBT. A better alternative- antidepressant medication then start CBT when they are more alert and motivated.
Success may be due to the CT Relationship. Rozenweig (1936) suggested that differences methods of psychotherapy, such as between CBT and systematic desensitisation might actually be quite small. It may actually be the quality of this relationship that determines success rather than any particular technique that is used.
CBT Doesn’t focus on past experiences: Some who experienced a traumatic event could benefit from exploring their past therefore therapies like psychotherapy where past experiences are discussed and there aim to resolve such trauma may be more effective in such cases.
Overemphasis on cognition: Reductionist as it doesn’t consider alternative explanations i.e. bio explanations such as genetic or chemical imbalances in the brain would give a more holistic understanding of the disorder.
Strengths of Cognitive Treatments
Grazioli and Terry (2000) assessed 65 pregnant women for cognitive vulnerability and depression before they gave birth. Found that those with high cog. vulnerability were more likely to suffer from post natal depression.
Similarly, Clark and Beck (1999) reviewed research on this topic and found that there was solid support for all these cognitive vulnerability factors. Critically, these cognitions can be seen before depression develops.
Increased understanding of the cognitive basis of depression leads to more effective treatments. E.g. elements of the cog. triad can be identified by a therapist and challenged as an irrational thoughts. Shows that it translates well into a successful therapy.
Limitations of Cognitive Treatments
Some depressed patients are deeply angry and Beck can not easily explain this extreme emotion.
Some sufferers of depression suffer from hallucinations and bizarre beliefs - e.g Cotard's syndrome (Jarrett, 2013).
They cannot explain all aspects of depression e.g. hallucinations, anger, Cotard’s. This poses a particularly difficult practical issue in that patients may become frustrated that their symptoms cannot be explained according to this theory and therefore cannot be addressed in therapy.
Cognitive explanations for depression share the idea that cognition causes depression. This is closely tied up with the concept of cognitive primacy, the idea that emotions are influenced by cognition. This is certainly the case sometimes, but not necessarily always.
What is depression?
A mental disorder characterised by low mood and energy levels
Diagnostic features of Depression
Can affect thoughts, feelings, behaviour and, physical well-being. Clinical depression is not just feeling sad (but this is part of it), its a set of complex symptoms. The symptoms must be causing distress or impaired functioning in social and/or occupational roles.
How are forms of depression and depressive disorders characterised?
All forms of depression and depressive disorders are characterised by changes to mood.
Categories of depression:
Major depressive disorder – severe but short term.
Persistent depressive disorder – long term and recurring.
Disruptive mood dysregulation disorder – childhood temper tantrums.
Premenstrual dysphoric disorder – prior to menstrual cycle
Behavioural Characteristics of Depression
Activity Levels
Disruption to sleep and eating
Aggression and self-harm
Activity Levels and depression
Sufferers have reduced energy levels (lethargy). Leads to withdrawal from work, education and social situations.
It can result in sufferers not getting out of bed. (Extreme)
There can be an opposite effect – psychomotor agitation, where individuals struggle to relax and may continuously pace.
Disruption to sleep and eating
May experience insomnia, premature waking, or hypersomnia.
Also, appetite and eating may increase or decrease (with weight gain or loss). Key point: These behaviour are disrupted by depression.
Aggression and self-harm
Sufferers of depression are often irritable, and can become verbally or physically aggressive.
This can have a serious knock-off effects on different aspects of their life e.g. someone experiencing depression might display verbal aggression by ending a relationship or quitting a job.
Depression can also lead to physical directed against the self. This includes self-harm or suicide attempts.
Emotional Characteristics
Lowered mood
Anger
Lowered self-esteem