2130 unit 4
1/151
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
152 Terms
parts of cardiovascular system
1) Heart → pump & makes pressure to move blood thru CV system
2) Blood vessels → tubes blood flows through (diff types & structures)
3) Blood → fluid carry gases, nutrients, hormones, immune cells, proteins, waste
What are the 4 primary functions of the cardiovascular system?
1) Distribution of blood to meet metabolic demands
2) Exchange/delivery of substances (nutrients, wastes, and hormones)
3) Heat regulation
4) Hemostasis (blood clotting)
5) Modulating inflamatory responses
what are the circuits of the CV system?
(1) pulmonary
blood leave heart w pulmonary artery
send blood to lungs (pick up O2, deliver CO2 waste pxd → return back to heart vis pulmonary veins)
(2) systemic
blood leave heart w aorta & aortic branches
send blood to organs & tissues in body EXCEPT lungs
GOAL = pick up waste to deliver to lungs, deliver O2 from lungs
What is the path of the pulmonary circuit?
Heart (deoxygenated) --> lungs --> heart (oxygenated)
What is the path of the systemic circuit?
Aorta (oxygenated) --> all organs and tissues --> veins (deoxygenated) --> heart
deliver blood back to R heart side w/ superior & inferior vena cava
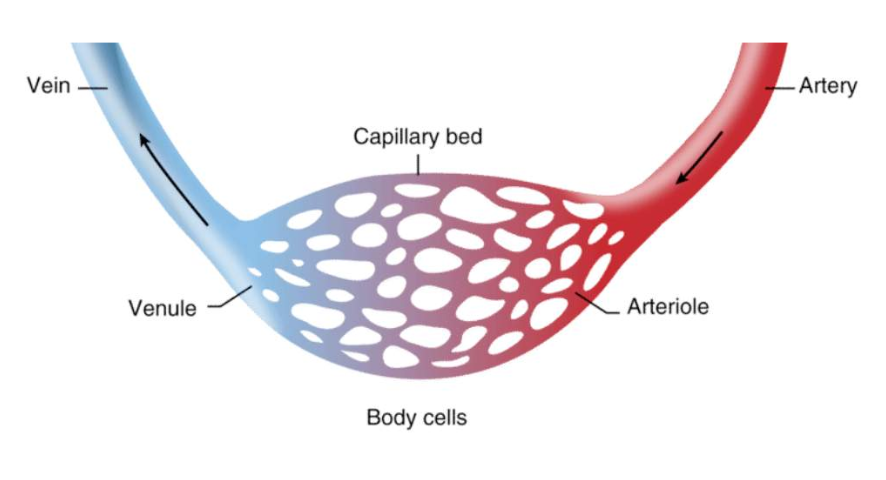
How are the blood vessels organized?
Heart → arteries (break into…) → arterioles → capillaries
capillaries (combine to…) → venules → veins → heart
arteries vs veins
A → carry blood AWAY from heart
V → carry blood TOWARDS heart
capillaries
exchange occurs
EX → glucose, AAs, CO2 + O2 move in/out blood
how does blood move through the heart?
deliver blood to heart via superior & inferior vena cava (via systemic circuit)
blood enter R atrium (returned from all organs & tissue EXCEPT lungs)
blood enter R ventricle via RIGHT AV valve
R ventricle blood sends thru pulmonary arteries
go towards lungs w pulmonary circuit (L & R pulmonary arteries)
blood = DEC O2, INC CO2 (collected from systemic organs, O2 dropped & CO2 picked up)
uses pulmonary valve
pulmonary arteries deliver CO2 (exhaled) & O2 added (inhale) back to blood
pulmonary veins (2R, 2L) collect blood from diff areas on lungs & enter L side of heart
blood enter L atrium via pulmonary circuit
blood enter L ventricle via LEFT AV valve
L ventricle sends blood thru aorta
send blood to all organs but lungs w systemic circuit
blood =INC O2, DEC CO2 (collected blood from lungs, pick up O2 & drop CO2)
uses aortic valve
blood sent out to rest of body tissue/organs via systemic capillaries
ventricles move blood to aorta & pulmonary arteries starting from apex → tip of heart & cascade contractions up towards atria
anatomy of the heart/organization of CV system
interventricular septum → wall divide L & R side prevent blood mix
left ventricular myocardium = L wall thicker bc INC pressure made to move blood thru systemic circuit bc gravity
atria → 2 top chambers
R = get blood from all organs/tissue except lungs via vena cava
L = get blood from lungs via pulmonary veins
ventricles → 2 bottom chambers
below atria
R = send blood via pulmonary arteries to lungs (DEC O2, INC CO2)
L = get blood via L atrium to aorta (INC O2, DEC CO2)
vena cava
#1 biggest vein
on R side
deliver blood back to heart from SYSM circulation
superior = blood from head/neck/chest/arms
inferior = blood from
pulmonary artery → deliver blood to lungs
pulmonary vein → 2L 2R collect blood from lungs & send to heart
aorta → blood sent to all tissues/organs except lungs
apex → bottom & start of where ventricles contract (send waves to top ventricles)
What are the 4 valves of the heart?
2 exits of ventricles → (1) aortic + (2) pulmonary valve
2 exits of atria → (3) R atrioventricular + (4) L atrioventricular (AV) valve
R atrioventricular (AV) valve
prevent blood backflow from R ventricle → R atrium
AKA tricuspid
L atrioventricular (AV) valve
prevent blood backflow from L ventricle → L atrium
AKA mitral
pulmonary valve (semilunar)
has 3 cusps that fill, expand & close to prevent blood backflow into R ventricles from pulmonary arteries
pass blood thru R ventricle → blood to pulmonary arteries → pulmonary circulation
aortic valve (semilunar)
has cusps that fill, expand & close to prevent blood backflow into L ventricles from aorta
pass blood thru L ventricle → blood to aorta → systemic circulation
what does a heart sound like?
valves closing = change blood flow dynamic & make sound
normal heart = lub (AV valve close, ventricle contract, blood go to atria) + dub (aortic & pulmonary valves close to send blood to ventricles)
heart murmur = valve regurgitation, X close properly
heart arrhythmia = irregualr heart contract
cardiomyocytes
cardiac muscle cells
allow for contraction & relaxation of heart
diff types have diff APs
(1) contractile cells
(2) nodal/conducting cells
How are cardiomyocytes similar to skeletal myofibers?
both striated (has myofibrils)
need Ca++ to contract
need mitochondria for ATP
need AP
How are cardiomyocytes different from skeletal myofibers?
for cardiomyocytes:
INC mitochondria
make own AP from nodal cells (X motor neurons)
branched (X cylindrical)
has 1 nucleus
Ca induced Ca release → extracellular fluid (via ion channels, down [] gradient to help SR release) + sarcoplasmic reticulum (store & release when AP occur
electrical connected w gap junctions → cell comm. bc coupled together & shares info w gap junctions (channels let ions pass from 1 cell to another)
intercalated discs → lock cells together w desmosomes proteins (hold cardiomyocytes together) & hold gap junctions
![<p>for cardiomyocytes: </p><ul><li><p>INC mitochondria</p></li><li><p>make own AP from nodal cells (X motor neurons)</p></li><li><p>branched (X cylindrical)</p></li><li><p>has 1 nucleus</p></li><li><p>Ca induced Ca release → extracellular fluid (via ion channels, down [] gradient to help SR release) + sarcoplasmic reticulum (store & release when AP occur </p></li><li><p>electrical connected w gap junctions → cell comm. bc coupled together & shares info w gap junctions (channels let ions pass from 1 cell to another)</p></li><li><p>intercalated discs → lock cells together w desmosomes proteins (hold cardiomyocytes together) & hold gap junctions </p></li></ul><p></p>](https://assets.knowt.com/user-attachments/c6c6535f-3a7f-4efe-bd3b-fa9a5d204a2d.png)
What are contractile cells?
contract & relax to pump blood through the heart
What are nodal/conducting cells?
Self-excitable cells by making own AP
X contact → limited actin & myosin
generate APs and spread electrical activity throughout heart
EX → sinoatrial node. AV node, AV bundle, subendocardial branches
What is calcium-induced-calcium release in cardiomyocytes?
Calcium coming from extracellular fluid down its concentration gradient helps the release of intracellular calcium from the SR
w/o = DEC Ca in cell from SR so Ca from outside induce Ca inside
normal muscle cell only w SR = store Ca & release when AP
cardiomyocyte = Ca from ECF + SR
Why are gap junctions important for normal heart functions?
allow ions to pass between cells so that contractile cells can communicate APs directly with each other
electrically connect cells w special channels to let ions/Ca/Na thru
What are intercalated discs?
Connections that lock two cells together via desmosomes (glue proteins) where gap junctions are found
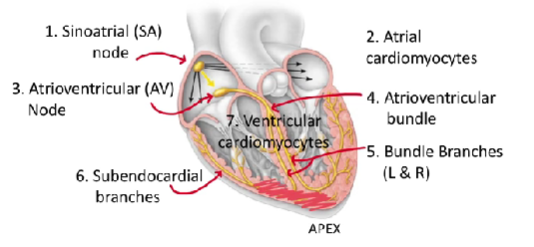
sinoatrial (SA) node
in upper R side of R atrium
move AP thru out heart so all of atria & contractile muscle of ventricle contract
AKA pacemaker of heart → sets heart rate
RMP unstable → self-excitable so contracts often (-60 lowest & -40 threshold)
F(x) =
has APs w/ → pacemaker potential, depolarize & repolarize
depolarization = Ca2+ voltage gated channels open @ threshold, move down [gradient] & INC (+) cell
repolarization = potassium (K+) leaking out, INC (-) cell
pacemaker potential
aka a graded potential to reach threshold
Na+ & Ca2+ move into own ion channels & prevent K+ leave
GOAL = cell INC (+) to make cell reach threshold
THUS → INC Na+ Ca2+ in cell & DEC K+ out of cell
What are 5 ways the SA node AP differs from a neuron AP?
SA node has =
1. unstable RMP
2. higher threshold (~40 mV)
3. depolarization caused by influx of Ca++
4. X hyperpolarization
5. slower than a neuron
Why is the SA node AP slower than a neuron AP?
SA node w/o fast sodium-gated channels
THUS → depolarization mainly b/c rapid influx of Ca
ALSO good bc neurons fire INC often & X need heartbeat that fast
How is the SA node related to heart rate?
1 AP = 1 beat
Heart rate = # of AP conducted by SA Node
intrinsic = 100 bpm
resting = 70 bpm
what is resting heart rate?
bio M = 70 bpm
bio W = 80 bpm → smaller hearts
trained athlete = 40-60 bmp b/c INC efficient pump blood w muscle contract INC force & need DEC often occur
Why is nodal/conducting cardiomyocytes pathway important?
contractile cells in atria & ventricles need AP to move Ca from ECF inside & release SR Ca → then if enough [] in cytoplasm, contracts
atria & ventricle CANNOT CONTRACT SIMOTANSEOUSLY
(1) atria contract = push blood into ventricles
(2) ventricle contract = push blood to lungs/body
atria & ventricles X direct contact w gap junction → use R/L AV valve
How does an AP generated at the SA node spread throughout the heart?
SA node creates AP & send to neighboring cells w gap junctions
Ca come into nodal cells = cell INC (+), threshold hit, make own AP
AP travel to atrial cardiomyocytes
AKA contractile muscle cells & neighbor cells
atria depolarize = contract, move blood into AV node
AV node gets AP → send AP btwn atria & ventricle
AP slows down (let atria finish contract) & pass to ventricles to contract
conduction starts in the interventricular septum
AV bundle gets AP & send to bundle branches
in the interventricular septum
AV bundle split into bundle branches
L & R bundle branches get AP & travel as branches contract same time to L & R ventricles
AP then travel subendocardial branches
under surface of heart in ventricular muscle
send AP from apex of ventricles → top of ventricles
AP travel fast at apex → quick move w wave to walls of both ventricles
ventricular cardiomyocytes get AP
contractile & contract bottom up
send AP w gap junctions
contract when AP @ apex
can the SA node fail?
intrinsic rate of SA node AP = fastest of all nodal/conducting cells
THUS → depolarizes & spreads AP before rest can fire AP
SA node fail = AV node takes over (2nd fastest)
What is the maximum heart rate?
220 - age
how does the autonomic nervous system affect the SA node?
get input from both branches
PSYN = heart rate DEC 100 bpm (rest, relax)
SYN = heart rate INC 100 bpm (fight, flight)
What system keeps the heart rate below 100 bpm?
parasympathetic system (PSYN of ANS)
ACh bind to MUSCARINIC receptors on SA node
THUS → DEC permeability of Na+ & Ca2+, INC permeability of K+
THEN → DEC slope of pacemaker potential = INC time reach threshold = DEC heart rate
What system raises the heart rate above 100 bpm?
sympathetic nervous system (SYN of ANS)
Norepinephrine binds to ADRENERGIC receptors on SA node
THUS → INC permeability to Na+ & Ca++ ions
THEN → slope of pacemaker potential INC = INC frequent fire = threshold reach faster = INC heart rate
SYN also releases epinephrine (adrenal gland) → hormone act of SA node, bind to adrenergic receptor & INC heart rate
what causes a change in the heart rate?
ANS innervates =
AV node → cause change in heart rate & keep coordinated heart contraction
ventricular cardiomyocytes → change force of ventricular contraction
Why does an AP slow down at the AV node?
To allow the atria to finish contracting before excitement is sent to the ventricles.
Why does an AP speed up at the subendocardial branches?
To allow the AP to spread throughout the heart and have a quick contraction of the ventricles.
What is bradycardia?
heart rate is too low
X enough blood & O2 delivered to tissue
need pacemaker in surgery maybe
dizzy, faint, tired
What is arrhythmia?
irregular heart rate
need pacemaker
How does a pacemaker work?
Acts as an SA node to stimulate heart to contract
THEN kick in when the heart starts beating irregularly
electrocardiogram (ECG/EKG)
AKA 12 lead ECG
give info abt electrical activity of the heart & how AP spread in heart
help diagnose heart issues → arrhythmia, heart attack, conduction issues
how does a ECG work?
waves = P, T, QRS
sums up all electrical events in heart b/c body fluids conduct APs
from surface of skin → 10 sticky electrode disks placed on diff chest/arm/legs
THUS → give 12 views of heart electrical activity from diff areas
has 3 waves →
P wave = depolarization ARTIA
QRS wave = depolarization VENTRICLES
T wave = REPOLARIZATION ventricles
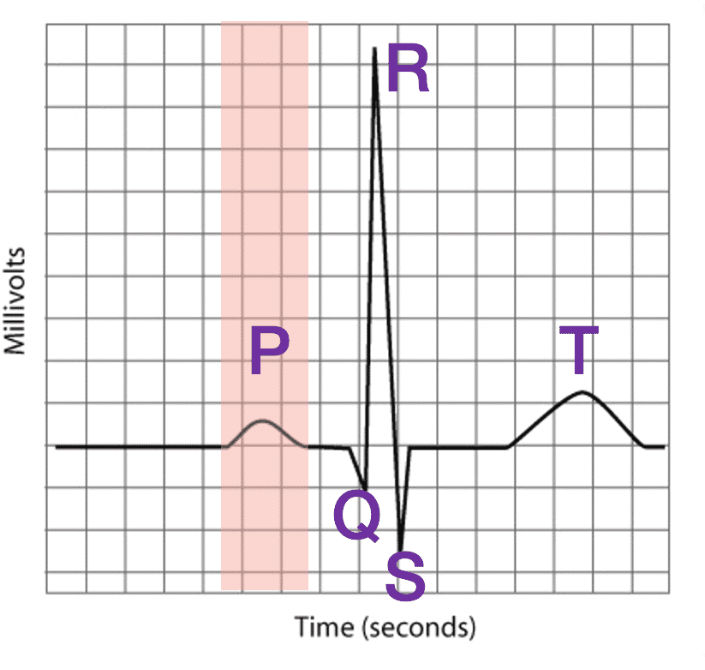
What does the P wave of an ECG indicate?
Atrial depolarization
measure TOTAL SUM of all AP occurs in atria
find heart rate if measure time from 1 P wave to next
RESULT = contraction
atria contract & pump blood to ventricles
PR interval
time from P wave to start of QRS wave
tell if electrical conduction normal btw atria & ventricles
QT interval
tell cardiac conditions
What does the QRS wave of an ECG indicate?
Ventricular depolarization & atria repolarization
atrial repolarization masked by larger QRS activity w ventricle depolarization
bigger wave than P wave → ventricles w INC mass = INC cells
RESULT = contraction
ventricles contract, pump blood out of heart
What does the T wave of an ECG indicate?
Ventricular repolarization
“up” phase → during AP
Why is repolarization represented as a 'positive' wave in an ECG?
direction of waves in an ECG based on direction of electrical activity towards a particular electrode
heading TOWARDS electrode = increase in voltage = INC wave
heading AWAY from electrode = DEC voltage = DEC wave
Why is the QRS wave much larger than the P wave?
The ventricles are much larger in mass than the atria and therefore have more cells depolarizing
What is systole?
measure of force exerted by cardiomyocytes on vessels when heart is contracting
top # on BP measurement
What is diastole?
measure of force exerted by cardiomyocytes on vessels in btwn heartbeats when heart is relaxing
bottom # on BP measurement
cardiac cycle
sequence of events occur in EVERY SINGLE heartbeat
go thru 5 phases of systole (contract) & diastole (relax) during 1 heart beat
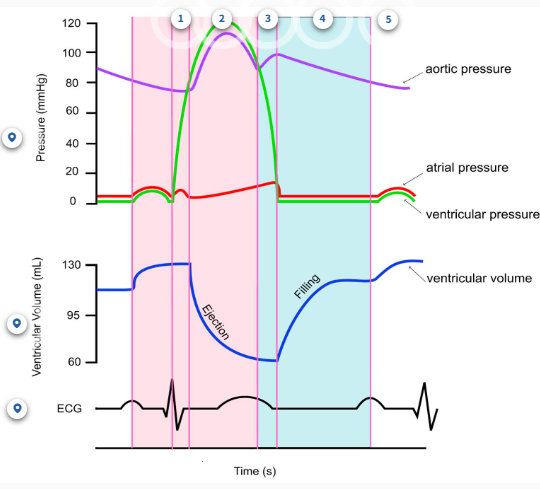
isovolumetric ventricular systole
ventricles start contraction BUT X pump blood out of heart yet
muscle → contraction
ECG → QRS wave (starting during atrial contraction)
Volume → X change
Valves → all closed
Pressure → ventricular INC dramatically BUT < aortic
ventricular systole
ventricles contract & move blood out of heart → aorta (L ventricle) + pulmonary arteries (R ventricle)
muscle → contraction
ECG → X new event
Volume → DEC ventricular volume
Valves → semilunar valves (pulmonary & aortic) open, AV valves closed
Pressure → ventricular > aortic
isovolumetric ventricular diastole
ventricles relax BUT X fill w/ blood
Muscles → relaxation
ECG → T wave (starting during ventricular systole)
Volume → X change
Valves → all closed
Pressure → DEC ventricular pressure, aortic > ventricular
late ventricular diastole
ventricles relax & fill w/ blood from atria
X fully filled & cont till atrial systole phase (little top up)
Muscles → relaxation
ECG → X new event takes place
Volume → INC ventricular volume
Valves → AV valves open, semilunar valves closed
Pressure → arial pressure > ventricular pressure
atrial systole
atria contract = move blood to ventricles
Muscles → contraction
ECG → P wave (starting during late ventricular contraction)
Volume → INC ventricular volume
Valves → AV valves open, semilunar valves closed
Pressure → atrial pressure > ventricular pressure
does the atria relax/atrial diastole occur?
YES → when ventricles contract & overpowered so X distinct phase
end systolic volume (ESV)
V of blood remain in ventricles at end of systole AFTER ventricles contracted
tells efficiency of the heart's pumping ability
What does a lower ESV indicated?
INC effective contraction
What does a higher ESV indicate?
DEC effective contraction
Heart dysfunction
end diastolic volume (EDV)
volume of blood in ventricles RIGHT BEFORE ventricular contraction
What is stroke volume (SV)?
volume of blood pumped out by the ventricles in each heartbeat
influences cardiac output
What is the formula for stroke volume?
SV = EDV - ESV
INC stroke V = INC EDV
INC stroke V = DEC ESV
What is cardiac output (CO)?
volume of blood the heart pumps per minute
measures heart f(x) + overall CV health
typical CO = 5-6 L/min
INC CO when exercise → INC demand tissue to pump blood to meet INC metabolic demands & deliver O2 to exercise
What is the formula for cardiac output?
CO = HR x SV
CO = heart rate x stroke volume
Why is cardiac output important?
essential 4 adequate blood flow to all tissues & organs
ensures proper O2 & nutrients delivered to cell & waste products remove
what can INC cardiac output?
INC # AP on SA node = INC heart rate
INC activation of sympathetic activity on SA node → release norepinephrine, bind to adrenergic receptors, INC SA node pacemaker = INC depolarization = INC heat rate
INC stroke V
INC EDV, DEC ESV
what affects stroke volume?
any factors affecting EDV & ESV
ANS innervation → affect Ca2+ permeability
preload on heart w/ EDV → affect contraction size
What is the distribution of muscarinic and adrenergic receptors on the ventricular muscles?
stroke volume based on contractile ventricle cardiomyocytes
INC adrenergic receptors → for SYN
DEC muscarinic receptors → for PSYN
UNLIKE →
SA node/pacemaker = muscarine & adrenergic receptors
AV node = muscarine & adrenergic receptors (control to speed/slow for coordinated heart contraction)
How is SV affected by activation of the SYN ANS?
SYN NS neurons innervate to ventricular cardiomyocytes
has adrenergic receptors on these contractile cardiomyocytes
able to bind norepinephrine (NTM) OR epinephrine (hormone)
activate adrenergic receptor on ventricular cardiomyocytes = INC Ca++ permeability
RESULT → INC Ca2+ in cytoplasm from SR = INC contraction strength
THUS → INC SV = INC pump blood each beat = INC CO
How is SV affected by the activation of the PYN ANS?
PSYN NS neurons innervate SOME contractile cardiomyocytes
PSYN release ACh when activated & binds to muscarinic receptors
RESULT → DEC Ca++ permeability = DEC Ca2+ into cytoplasm from SR = DEC contraction strength
THUS → DEC SV modestly = DEC CO
What is preload?
load on heart before contraction
load = volume of blood in ventricles (aka just EDV)
How does preload affect the SV?
INC EDV (INC full heart) = INC stretch of contractile cells of ventricle = INC contraction force of cells upon systole
THUS → INC amount of blood ejected from heart = INC SV
protective mechanism (frank starling’s law)
What is Frank Starling's Law of the heart?
INC preload (INC full heart & INC EDV) = INC cardiac output
w/o this, cause INC full heart w each beat
THUS → INC SV maintain regular ESV
How can you increase EDV and preload?
VENOUS RETURN
squeezing veins to force more blood back into heart (venous return)
What is the general pathway of blood flow through the systemic circuit?
Aorta --> arteries --> arterioles --> capillaries/body cells --> venules --> veins
DEC venules than capillaries → capillaries combine to make venules
Which circulatory system contains most of the blood?
Systemic circuit (85%)
each organ & tissue supplied by one of major arteries & smaller arteries/arterioles/capillaries/venules/smaller veins
blood move back to heart w major vein & empty to R atrium w vena cavas
what is the distribution of blood in the body?
total blood V = 4-6 → heart circulates entire blood V in 1 min
most blood in systemic circuit (85%)
veins > arteries > capillaries
little blood in heart & pulmonary circuit (15%)
What are the 3 layers of blood vessels?
Tunica externa, tunica media, and tunica interna.
What is the tunica externa?
Fibrous connective tissue: protects vessel, adheres it to surrounding tissues, and maintains its appropriate structure. Neurons and blood vessels are found here.
What is the tunica media?
Smooth muscle: contract or relax to various stimuli.
Elastin: allows vessels to stretch and recoil back to their resting shape.
Collagen: protein common in connective tissue.
What is the tunica interna?
Endothelial cells: important for normal vessel function.
How does the tunica media differ between arteries, arterioles, and veins?
Arteries: elastin is much more abundant than smooth muscle
Arterioles: smooth muscle is much more abundant than elastin
Veins: have some smooth muscle and elastin
How do the diameters of the different blood vessels compare?
Veins > arteries > arterioles = venules > capillaries
How do the wall thicknesses compared to diameters of the different blood vessels compare?
Arterioles > arteries > capillaries > venules = veins
What kind of vessels are arteries?
Distribution vessels: carry blood away from the heart.
What kind of vessels are arterioles?
Resistance vessels: carry blood from arteries to capillaries.
What kind of vessels are capillaries?
Exchange vessels: oxygen, nutrients, and ions are exchanged into cells while CO2 enters the blood.
What is the function of venules?
Carry blood from capillaries to veins.
What kind of vessels are veins?
Capacitance vessels: carry blood back to the heart.
How do the blood pressures of the different vessels compare?
Arteries > arterioles > capillaries > venules > veins
What is the main mechanism behind increasing EDV?
Exercising causes flight or fight response --> SNS innervates blood vessels and contraction of smooth muscle --> decreases diameter of vessels and forces blood forward
What is the skeletal muscle pump?
Veins squeezed by surrounding skeletal muscle --> muscle contracts and bulges --> squeezes vein and narrows diameter --> more blood returns to heart --> increases EDV, SV, and CO
Why is blood flow regulation important?
Ensures that different organs receive the appropriate amount of blood based on their needs. Maintains blood pressure. Increases or decreases heat loss from the body by redistributing blood.
Which organ receives the most blood?
Liver (25%).
Which two organs receive the least blood?
Heart and skin (5% each).