Lecture 7: Gender Identity and Sexuality in Neurodevelopmental Conditions
1/49
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No study sessions yet.
50 Terms
historical view (gender, sexuality & neurodevelopmental conditions)
-individuals with neurodevelopmental conditions seen as childlike or asexual
-led to a lack of research and clinical attention
-ethical concerns limited research
-biases hindered early studies e.g., focus on victimisation
moving past historical view (gender, sexuality & neurodevelopmental conditions)
-focus on sexual education, consent and healthy relationships
-studies on the impact of neurodevelopmental conditions on sexual development and expression
-research on gender identity and sexual orientation within neurodivergent populations
-emphasis on need for tailored support
sexual attraction (sexuality)
-who a person is physically attracted to
-can involve romantic and emotional involvement
sexual identity (sexuality)
-how a person identifies their sexual attraction and orientation
sexuality
-includes sexual attraction and sexual identity
-diverse and can be fluid
-cultural and societal norms play a role shaping how sexuality is understood and expressed
childhood sexual development
-0-12
-body awareness
-gender role exploration
-early understanding of relationships
adolescence sexual development
-13-19
-puberty
-sexual identity formation
-early romantic experiences
adult sexual development
-continued exploration
-intimacy and relationship development
-lifelong learning about sexual health and expression
Weir - autism and sexuality
-autistic people 8x more likely to identify as asexual and ‘other’ sexuality than their non-autistic peers
-sex differences in sexual orientation:
autistic men 3.5x more likely to identify as bisexual than non-autistic men
autistic women 3x more likely to identify as homosexual than non-autistic women
ADHD and sexuality
-women with ADHD are more likely to have had homosexual experiences
-generally, individuals with ADHD do not differ from neurotypical peers in their self-reported sexual orientation
-potential to show more hypersexual behaviours
ADHD features and sexuality
inattention → difficulty engaging in sex and maintaining relationships
impulsivity → linked to risky sexual behaviours
sensory sensitivities → can find sex uncomfy or repelling due to sensation → hyposexuality
dopamine → reduction in dopamine in ADHD so may seek out stimulation → hypersexuality
medication for ADHD can lead to reduction in sex drive
sex
-typically refers to biological attributes
-chromosomes, hormones and anatomy
gender
-social construct
-the norms and expectations that societies create around what it means to be a ‘man’, ‘woman’ or other gender identities
-norms vary across cultures and change over time
Kohlberg’s stages of gender identity
gender identity based on appearance
gender stability over time, still appearance based
gender constancy across changes
biological factors (sex and gender)
-hormones influence development
-intersex conditions and transgender/twin studies are relevant
social cognitive theory (sex and gender)
-gender development involves personal, environmental and behavioural factors
gender similarity hypothesis (sex and gender)
-genders are more alike than different in most variables
gender-typing and gender expression
-as children develop, they learn to perform behaviours associated with their gender
-processes by which adopt observable behaviours in line with our construction of gender
gender-typed preferences
-results from the combined influence of biological, psychological and sociocultural processes
gender identity
-individual’s internal sense of their own gender
-deeply personal experience that may or may not align with assigned sex at birth
-exists on a spectrum, people may identify as male, female, non-binary, etc.,
gender diversity (gender identity)
-experiencing aspects of gender as different from assigned sex at birth
-can result in gender incongruence where a person’s gender identity differs from their assigned sex
general population (gender identity)
-as many as, 1-2% identify as gender diverse
-UK Census found 0.5% of the population indicated gender identity differed to their assigned sex
Harrison
-so many different ways of identifying:
non-binary
pangender
transgender
androgyne
genderfluid
agender
demigender
genderqueer
bigender
gender dysphoria
-people may experience discomfort or distress when their assigned sex is different from the gender they identify with
-transgender people must be assessed for gender dysphoria before gender affirming care
DSM-5-TR - children
-marked incongruence between one’s experienced gender and assigned gender
desire to be of the other gender or an insistence that one is the other gender
preference for cross-gender roles in fantasy play
preference for the toys, games or activities stereotypically used by other gender
preference for playmates of the other gender
dislike of one’s sexual anatomy
desire for physical sex characteristics that match one’s experienced gender
DSM-5-TR - girls (children)
-preference for wearing only typical masculine clothing and strong resistance to wearing of typical feminine clothing
-rejection of typically feminine toys, games and activities
DSM-5-TR - boys (children)
-preference for cross-dressing or simulating female attire
-rejection of typically masculine toys, games and activities
-avoidance of rough and tumble play
DSM-5-TR - adolescents and adults
-marked incongruence between one’s experienced/expressed gender and their assigned gender
marked incongruence between one’s experienced/expressed gender and primary and/or secondary sex characteristics
desire to be rid of one’s primary and/or secondary sex characteristics because of a marked incongruence with one’s experienced gender
desire for primary and/or secondary sex characteristics of the other gender
desire to be of the other gender
desire to be treated as the other gender
conviction that one has the typical feelings and reactions of the other gender
de Vries (gender diversity in autism)
-incidence of autism in children and adolescents referred for gender diversity services
-7.8% of the sample met strict diagnostic criteria for autism
-10 times higher than prevalence of autism in the general population
Strang (gender diversity in autism)
-identified studies of gender diverse and transgender youth that included only clinical autism diagnoses
-rates of clinical diagnoses were significantly greater than the general population
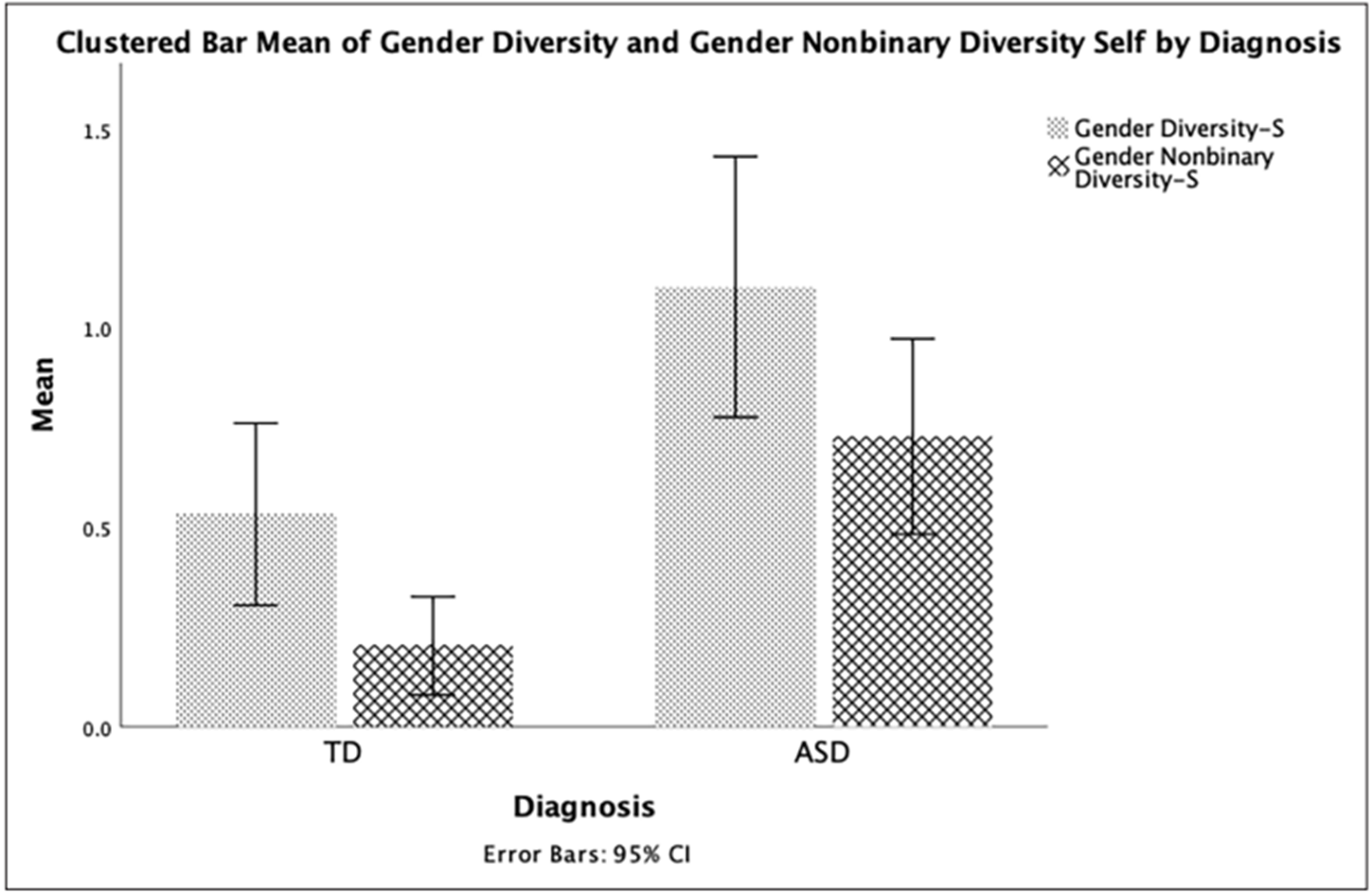
Corbett (gender diversity in autism)
-research typically relied on parent-report based on a single question
-this research used the Gender Diversity Screening Questionnaire with two domains:
binary gender diversity
nonbinary gender diversity
-self report → autistic children showed higher gender diversity
-parent report → significance difference in gender diversity between the groups on body incongruence
-need to better understand and support the unique and complex needs of autistic children who experience gender diversity
gender diversity and ADHD
-very limited, few studies
-transgender and gender diverse individuals had elevated rates of ADHD
-prevalence rate of 8.3% in children and adolescents referred for gender care
-prevalence rate of 4.3% in TGD adults
Ignatova (gender diversity and ADHD)
-ADHD and transgender adolescents
-longitudinal Adolescent Brain Cognitive Development study
-methods:
are you transgender → yes/no/maybe
-gender diverse individuals showed higher levels of ADHD traits
-results reduced when controlling for stress
Cooper (lived experience - autistic and transgender)
-semi-structured interview with autistic adults who identified as transgender and/or non-binary
-distress due to their bodies not matching their gender identities, while managing complex intersecting needs
-societal acceptance of gender and neurodiversity → barriers in accessing healthcare for their gender needs
-tension between need to undergo a physical gender transition vs a need for sameness and routine
Cooper - positive experiences (lived experience - autistic and transgender)
-being autistic allows one to step outside societal norms and follow own path
-do not care for fitting into societal boundaries about gender
-autism diagnosis made experiences come to light and comforting → allows for new coping strategies
DSM-5-TR - autism (dysphoria and sensory activities)
-hyper or hypo reactivity to sensory input or unusual interests in sensory aspects of the environment
dysphoria and sensory activities
-sensory dysphoria → distress linked to sensory experiences
-wearing uncomfortable fabrics and shapes associated with girls’ clothes
-sensory challenges of puberty e.g., facial hair, periods
explanations for dysphoria and autism
biological explanations
increased self-identification
cognitive and sensory differences
biological theories (dysphoria)
prenatal hormone exposure
brain structure and function
prenatal hormone exposure (biological theories)
-variations could contribute to differences in how individuals perceive and experience gender
-not a simple cause and effect relationship
brain structure and function (biological theories)
-differences in structure and function could influence how individuals process and internalise social constructs
-differences in brain regions involved in social cognition and self-perception might play a role
increased self-identification (dysphoria)
-autistic individuals may be less influenced by societal norms and expectations surrounding gender and sexuality
-leading to greater likelihood of expressing their authentic gender or sexual identities, even if it deviates from societal norms
-may be less likely to supress or conform to traditional gender roles due to social pressures
differences in social cognition and sensory processing (dysphoria)
systemising pattern recognition
intense focus and special interests
sensory sensitivities/sensation seeking
systemising and pattern recognition (differences in social cognition and sensory processing)
-more analytical approach to gender
-breaking down its components and questioning traditional norms
intense focus and special interests (differences in social cognition and sensory processing)
-increased depth
-leading to more profound understanding of their own identify
-less influence from outside sources
sensory sensitivities/sensation seeking (differences in social cognition and sensory processing)
-certain clothing textures or social environments associated with specific genders might be intensely uncomfortable
-preferences for certain gendered presentations due to the sensory input it provides
down syndrome (gender identity, sexuality and DS)
-limited to no studies investigating gender diversity in DS
-parent-report regarding more general views of sexuality in DS
-no studies directly speaking to individuals with DS
-focus on the need for and improvement of sexual education for individuals with DS
sexual education in DS
-adolescents and young adults with intellectual or developmental disabilities frequently excluded
-often focuses on safety and abuse prevention rather than a holistic approach → healthy relationships, consent and sexual fulfilment
-need to work with these individuals to develop and implement more accessible and effective SE programs
Schmidt (SE for DS)
-improving the accessibility of SE for individuals with intellectual or developmental disabilities
-qualitative data collection through interviews and focus groups
modalities → educational guides, visuals, videos, universal design for learning, direct/explicit instruction
settings → 1:1, small groups, combination
additional → role-playing and modelling, open communication, importance of parental support and education
universal design for learning (UDL)
-adapts education to fit diverse learner needs
-3 principles:
representation → other information in varied formats
action/expression → provide different ways for learners to interact and express themselves
engagement → increase motivation through choice, relevance and collaboration
-can make SE accessible and engaging for all