Pain Mechanisms
1/19
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
20 Terms
inputs to the system
processing of inputs
outputs from the CNS
Mature Organism Model – Review
what is inputs to the system?
– Include sensory afferents and environmental context
– Nociceptive inputs from body tissues
– Peripheral nerve-related pain
what is processing of inputs?
– Occurs from the dorsal horn to cortical centers
– Involves central pain mechanisms
– Influencing factors:
Past experiences, Social and cultural context, Pain beliefs and knowledge, Expectations and fear, Other psychosocial elements
what is output from the CNS?
– Construction of the pain experience
– Other physiological and behavioral responses
what is three types of pain?
nociceptive
peripheral neuropathic
central (nociplastic)

what is nociceptive pain?
Proportionate Pain
Aggravating and easing factors
Intermittent sharp, dull ache, or throb at rest
No night pain, dysesthesia, burning, shooting or electric pain
what is Peripheral Neuropathic Pain?
• Pain in dermatomal or cutaneous distribution
• Positive neurodynamic tension testing and palpation
• History of nerve pathology or compromise
Disproportionate pain
Disproportionate aggravating factors
No easing factors
Diffuse tenderness to palpation
Psychosocial Issues
– Fear avoidance
– Pain catastrophizing
– Depression
Central Sensitization (Nociplastic Pain)
pain referred in a dermatomal or cutaneous distribution
history of nerve injury, pathology, or mechanical compromise
pain/symptom provocation mechanical testing which moves, loads, or compresses neural tissue
peripheral neuropathic
pain localized to area of injury or dysfunction +/- somatic referral
clear proprotionate mechanical or anotomical nature to agg/eases
usually intermittent and sharp with movement or mechanical provocation
absence of:
pain with other dysesthesias
night pain or disturbed sleep
burning, shooting, or electrical pain
nociceptive
disproportionate, non-mechanical unpredictable pain pattern in response to multiple or non specific aggs/eases
pain disproportionate to the nature and extent of injury or pathology
diffuse/non anatomic area of pain/ tenderness on palpation
strong association with maladaptive psychosocial factors
central nocioplastic
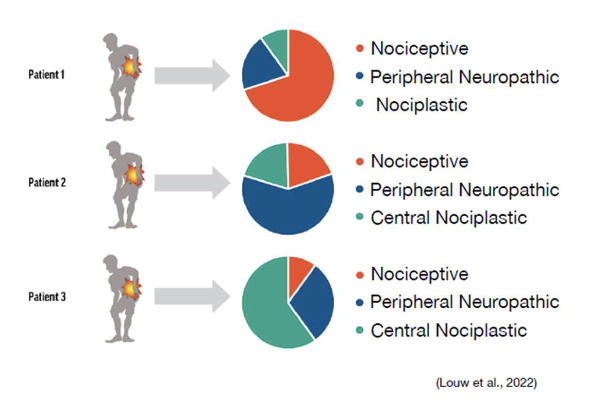
shows the relative contributions of different pain mechanisms in a patient’s experience
dynamic
size of each “slice” can change over time based on biological, psychological, and social factors
help understand the dominant pain mechanism
tailor assessment and treatment strategies
pain pies
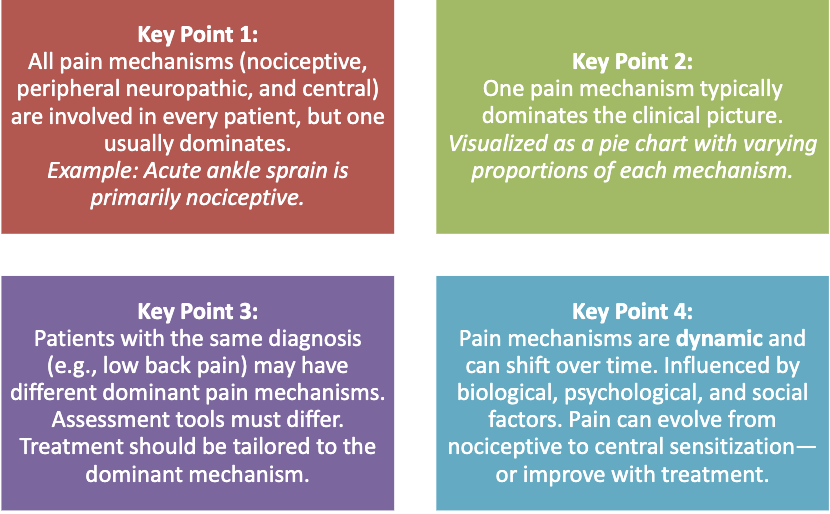
Pain Mechanisms - Key Points
Patient 1 – Nociceptive-Dominant
Presentation: Acute low back pain after lifting a heavy object.
Pain Pie:
Red (Nociceptive): Large portion – tissue damage, inflammation.
Blue (Peripheral Neuropathic): Small – mild nerve irritation.
Green (Nociplastic): Small – minimal central sensitization.
Clinical Focus: Address tissue healing, inflammation, and movement education
Case Example 1
Patient 2 – Peripheral Neuropathic- Dominant
Presentation: Radiating leg pain with numbness and tingling.
Pain Pie:
Blue (Peripheral Neuropathic): Large portion – nerve root involvement.
Red (Nociceptive): Small – some mechanical irritation.
Green (Central Nociplastic): Small – early signs of central involvement.
Clinical Focus: Nerve mobility, reduce mechanical compression, education on nerve pain.
Case Example 2
Patient 3 – Central Nociplastic-Dominant
Presentation: Chronic low back pain for over a year, widespread sensitivity, poor sleep, and fear of movement.
Pain Pie:
Green (Central Nociplastic): Large portion – central sensitization, altered pain processing.
Red (Nociceptive): Small – minimal tissue damage.
Blue (Peripheral Neuropathic): Small – no clear nerve involvement.
Clinical Focus: Pain neuroscience education, graded exposure, cognitive-behavioral strategies.
Case Example 3
Traditional Time-Based Categories:
Updated Understanding
Clinical Implication:
Acute, Sub-Acute and Chronic Pain
Traditional Time-Based Categories:
– Acute Pain: Present for less than 3 months.
– Subacute Pain: Lasts between 6 weeks and 3 months.
– Chronic Pain: Persists for more than 3 months.
what is Updated Understanding?
– Central sensitization/nociplastic pain can develop within days after injury.
– Time alone is not a reliable indicator of pain mechanism.
acute, sub-acute and chronic pain Clinical Implication:
– Therapists must recognize that persistent pain can begin early.
– Early identification of central mechanisms is crucial for effective treatment.