Adult III: Exam 4 Study Guide
1/104
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
105 Terms
What is the Monroe-Kelly Doctrine?
There are 3 rigid cranial vaults, or the rigid cranial vault contains 3 non-compressible contents—brain matter 80%, blood 10%, CSF 10%
The Sum of the brain, the CSF (cerebrospinal fluid), and the intracranial blood volumes is consistent.
An increase in one should cause a decrease in one or both of the remaining two —>Due to the limited space, an increase in one equals a decrease in the others, so this means that if CSF increases, the intracranial blood volumes and brain volumes should decrease
Intracranial pressure is the sum of the pressures of the brain, cerebrospinal fluid, and intracranial blood.
What is normal adult ICP?
5-15 mmHG
How is cerebral perfusion pressure calculated?
What is normal cerebral perfusion pressure?
MAP - ICP = cerebral perfusion pressure
Ex: So, if MAP is 65 and ICP is 10, cerebral perfusion pressure is 55
Normal: 70 - 80 mmHg, so in the example above, that cerebral perfusion pressure is not sufficient
—>So when a patient is having neurological issues, a MAP of 65 is not good enough to perfuse the brain = if the patient has a neuro problem, they will likely have increased ICP, so MAP needs to be kept at higher to maintain a cerebral perfusion pressure of 70-80 mmHg
What is normal cerebral perfusion pressure?
What happens if cerebral perfusion pressure equals MAP?
70 - 80 mmHg
If cerebral perfusion pressure = MAP, then cerebral circulation stops
What is cerebral perfusion pressure?
The pressure required to maintain adequate blood flow to the brain
You are given a question where you need to find out if a patient’s MAP is sufficient to maintain cerebral perfusion pressure, how do you do this?
Take the MAP and subtract ICP from it, then see if it is at least 70-80, if it is, MAP is sufficient
Verbalize the Glasgow coma scale
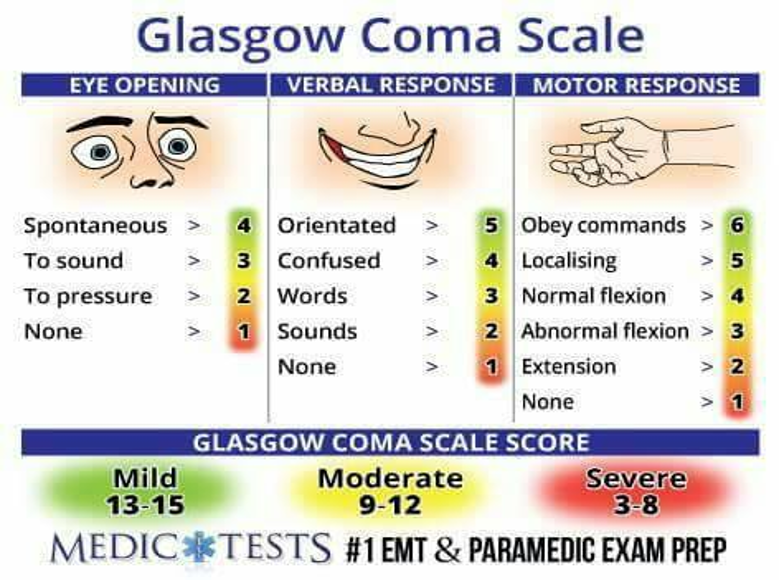
Verbal
4 = confused—i.e., know name, but not where they are at
3 = words—i.e., you ask them where they are and they say “brown cow”
2 = sounds—i.e., garbled, incomprehensible sounds
Motor
6 = obeys commands—i.e., squeezes your fingers or moves feet on command
5 = localizing—The patient purposefully moves toward the site of the painful stimulus (e.g., reaching up to grasp the examiner's hand and removing it from the supraorbital ridge)
4 = normal flexion (withdrawal)—the patient pulls away from the painful stimulus
3 = abnormal flexion (decorticate =)—the patient has rigid flexion of the arms, clenched fists, and adducted arms to the chest, with legs internally rotated and extended
2 = abnormal extension (decerebrate)—The patient exhibits rigid extension of the arms, adduction, and internal rotation of the shoulders, with pronation of the forearms and extended legs
1 = none (flaccid/no movement in response to painful stimuli)
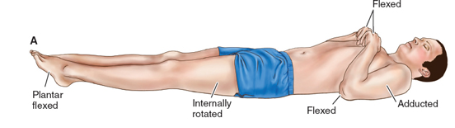
What is decorticate posturing?
Decorticate posturing = an abnormal posture associated with severe brain injury, characterized by abnormal flexion of the upper extremities and extension of the lower extremities (flexion and internal rotation of forearms and hands)
Decorticate = flexion of upper extremities to the core—Think “core”; they are protecting their core
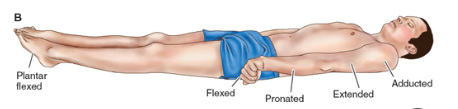
What is decerebrate posturing?
Decerebrate posture: Extension and external rotation of upper extremities with plantar flexion of the feet; an abnormal body posture associated with severe brain injury, characterized by extreme extension of the upper and lower extremities
Decerebrate posturing indicates deeper and more severe dysfunction than does decorticate posturing; implies brain pathology; poor prognostic sign
A patient has a GCS of 3-8. What will likely be required to maintain life?
Intubation
A GCS of 3-8 is severe
A GCS of 3 in particular indicates severe impairment of neuro function, brain death, or pharmacologic intervention (i.e., w/ admin of pharmacologic paralyzing agents like neuromuscular-blocking agents)
List common conditions that affect GCS
Blood glucose
Electrolytes
Liver function
BUN/creatinine
Drugs/alcohol
Resp function alteration (Based on ABGs)
Calcium levels
When performing a neurological exam, what should you assess regarding language?
Assess fluency and spontaneity of speech, word finding ability and comprehendion; if intubated, cannot speak to you , so have them write on a white board or blink eyes
Expressive aphasia = broca’s aphasia—hard time word finding/completing verbal or written skills
Wernicke’s aphasia—response does not follow cntesxt on situation = receptive issue; ____
What is expressive aphasia?
Expressive aphasia = Broca’s aphasia—hard time word finding/completing verbal or written skills
What is Wernicke’s aphasia?
Wernicke’s aphasia—response does not follow context of the situation = receptive issue
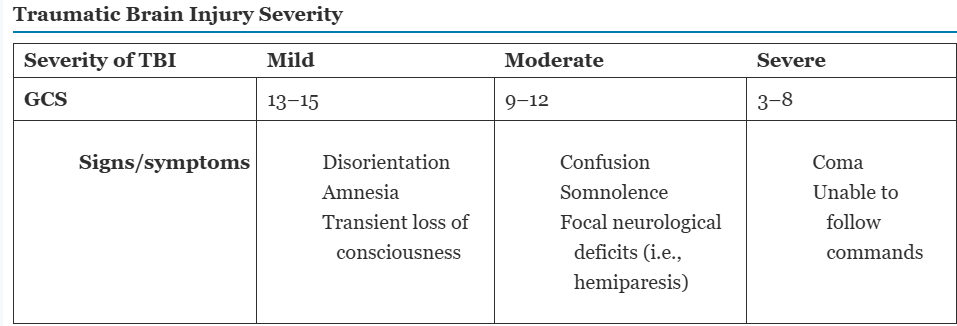
List s/s of TBI of the following GCS ranges:
Mild (13-15)
Moderate (9-12)
Severe (3-8)
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?What is the major function of the ___ nerve? How do you assess its function?
What is the major function of the ___ nerve? How do you assess its function?