Neurology
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Grey matter vs. white matter
Grey matter = Cell-rich part of the CNS consisting of a neuron’s cell body, dendrite and synapse
White matter = Axons supporting neurons which link neurons to their targets within the brain, spinal cord or receptor/target organ
Myelin = Fatty substance produced by oligodendrocytes (CNS) and Schwann cells (PNS) that coats axons in concentric layers
Different sections of myelin formed by different oligodendrocytes/Schwann cells
Nodes of Ranvier = Unmyelinated gaps between the myelin
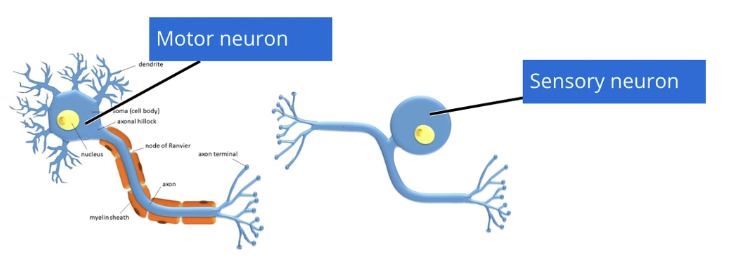
Sensory vs. motor neurons
Sensory Neuron = Cell body partway along axon → 2 axon terminals
Proximal terminal synapses with neurons
Distal terminal associated with receptor
Neuronal cell bodies in CNS (nucleus) OR PNS (ganglion)
Motor Neuron = Cell body at one end → 1 axon terminal synapsing onto effector organ
Myelinated vs. unmyelinated axons
Larger and myelinated axons transmit information faster than smaller and unmyelinated axons
Large/Myelinated Axons = Convey reflexes → Sharp pain to avoid further damage
eg. High temperature, withdrawal reflex, gag reflex, palpebral reflex
Shorter pathway → Reduced reaction time
Small/Unmyelinated Axons = Convey dull throbbing pain
Caused by existing tissue damage and inflammation
eg. C-fibres and A-delta fibres
What is the difference between a response vs. reflex
Response = Conscious reaction to stimulus (processed by forebrain)
Must be learned and can be suppressed with anxiety/stress
Reflex = Unconscious reaction to stimulus (processed by local brainstem/spinal cord)
NOT learned, but protective mechanisms
List the common DDx using VITAMIN D:
Forebrain (22)
Cerebellum (7)
Vestibular C/P (7)
Forebrain:
Inflammatory
Meningoencephalomyelitis of unknown origin (MUO)
Infectious
Bacterial
Viral
Fungal
Parasitic
Traumatic
Penetrating injury
Blunt trauma
Anomalous
Hydrocephalus
Porencephaly and hydranencephaly
Meningoencephalocele
Metabolic
Electrolyte imbalances
Mitochondrial encephalopathy
Hypoglycaemic encephalopathy
Acid-base related
Hepatic/renal encephalopathy
Endocrine-associated
Idiopathic
Epilepsy
Dyskinesia
Neoplasia
Meningioma, glioma, lymphoma, pituitary tumour, metastasis
Nutritional
Paroxysmal gluten-sensitive dyskinesia
Vitamin deficiency
Degenerative
Lafora disease
Cerebellum:
Vascular
Ischaemic infarction
Haemorrhage
Hypertension
Inflammatory
Idiopathic generalised tremour syndrome
Infectious
Protozoal (neosporosis)
Degenerative
Spinocerebellar ataxia
Cerebellar cortical degeneration
Vestibular:
Inflammatory
Nasopharyngeal polyp (primary secretory OM) (P)
Central (as for forebrain)
Infectious
Otitis media-interna (P)
Feline infectious peritonitis (C)
Toxin
Metronidazole (C)
Idiopathic
Idiopathic vestibular disease (P)
Nutritional
Thiamine deficiency (C)
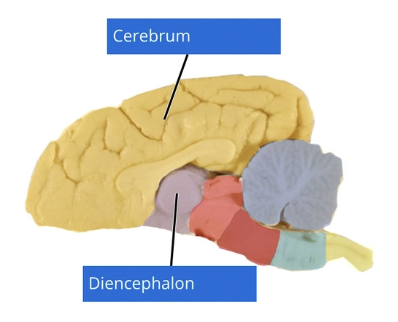
Describe the structure of the forebrain
Forebrain aka. prosencephalon =
Telencephalon = Cerebral hemispheres
Diencephalon =
Epithalamus
Hypothalamus
Subthalamus
Thalamus
Consists of:
Grey matter located in the superficial cortex AND deeper structures (eg. hippocampi, basal and septal nuclei)
White matter located deeper within the forebrain to link different parts of the brain together (+ brain to spinal cord)

List 7 functions of the forebrain
Responsible for thought, behaviour and cognition
Processes sensory input to provide conscious recognition (eg. vision, hearing, tactile sensation, proprioception)
Includes the limbic system responsible for emotions, behaviour and long-term memory
Includes the thalamus = Gateway for information between brainstem and cerebrum, sorting into correct location
Includes the hypothalamus responsible for homeostasis (eg. thirst, sleep and body temperature) and synthesis of hormones to trigger trophic hormone release from the pituitary gland
Includes the subthalamus responsible for management of body movement
Includes the epithalamus associated with the limbic system and contributes to the maintenance of circadian rhythm
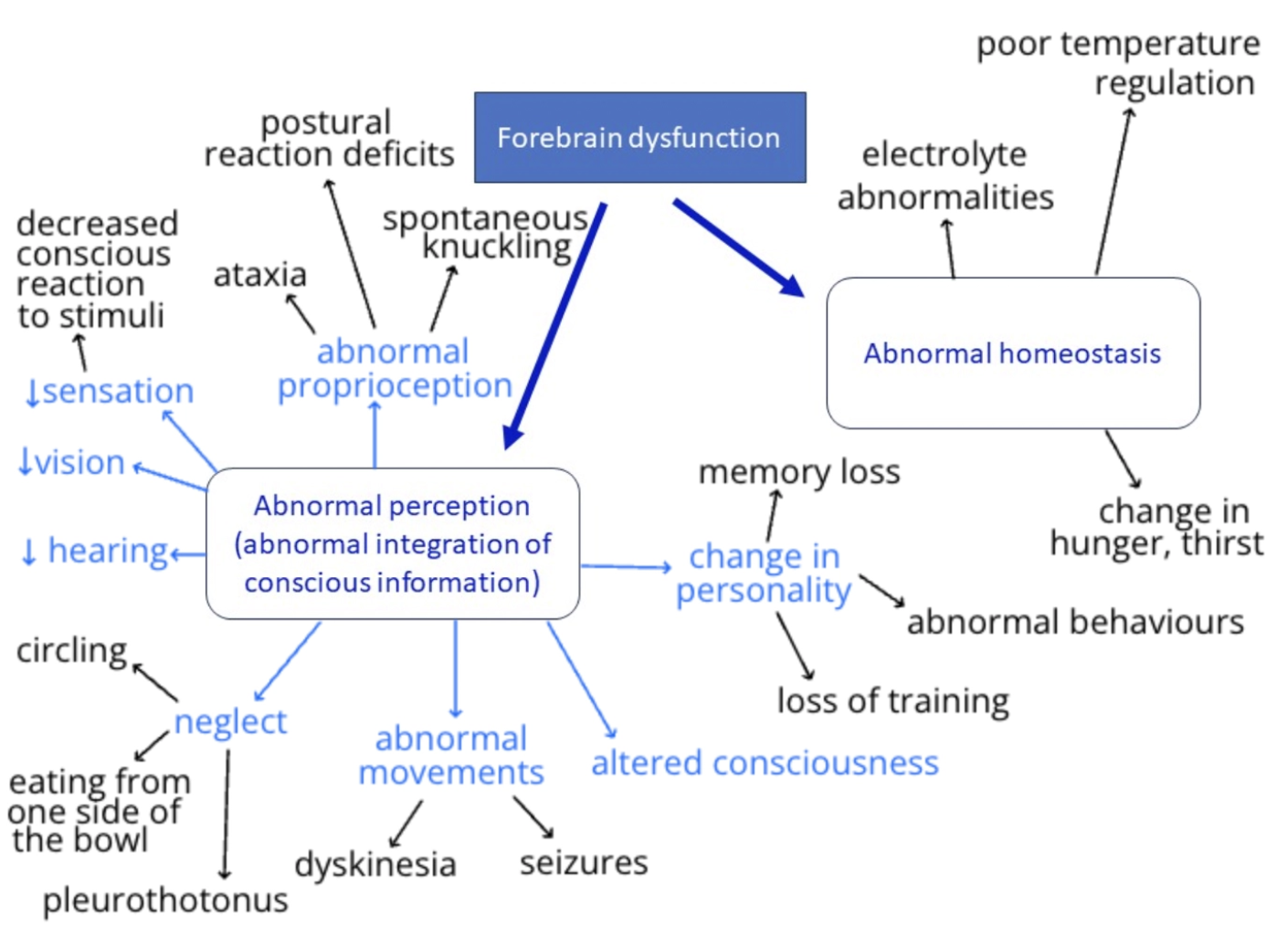
Describe 9 clinical manifestations of forebrain dysfunction (+ normal)
Abnormal Mentation
Abnormal level
Obtunded = Drowsy but rousable with reduced responsiveness (aka. depressed)
Stuporous = Sleeping but can be roused with painful stimulus
Comatose = Unconscious and cannot be roused with painful stimulus BUT still retains withdrawal reflex
Abnormal quality
Disoriented = Alert but inappropriate responses to stimuli
Delirium = Confusion and disrupted attention often accompanied by hallucinations
Abnormal Behaviour
eg. Wandering, lethargy, vocalisation, loss of learned behaviour, lack of recognition, aggression, loss of circadian rhythm
Hemi-neglect = Animal ignores all information from one side of the body (eg. only eating food from one half of the food bowl)
Abnormal Gait
Proprioceptive ataxia
Aimless wandering or compulsive pacing
WIDE circling towards side of brain with lesion: Cerebral hemisphere receives/sends instructions to CONTRALATERAL side
eg. L forebrain pathology → Information on R body is not being sent to forebrain → Animal circles to L as R does not exist in their brain
Abnormal Posture
Head turn OR pleurothotonus (head AND body turn) towards side of lesion
Head-pressing
Horizontal/low head carriage due to “headache” ± neck pain 2˚ to increased ICP
Contralateral Postural Reaction Deficits
Requires conscious realisation of need to correct posture
eg. Contralateral hemiparesis and delayed paw positioning response
Abnormal Movements = Epileptic seizure and dyskinesia
Hyperaesthesia = Excessive sensitivity and pain over calvarium on palpation (also cranial cervical spine with increased ICP)
Headache → Photophobia or head-pressing
Inappropriate Micturition = Loss of house-training or involuntary urination during seizure
Homeostatic Disorders = Endocrine dysfunction, loss of regulating water/food intake, loss of thermoregulation, abnormal growth
Normal:
Cranial nerve reflexes (processed in brainstem)
Spinal nerve reflexes (processed in spinal cord)
Nociception
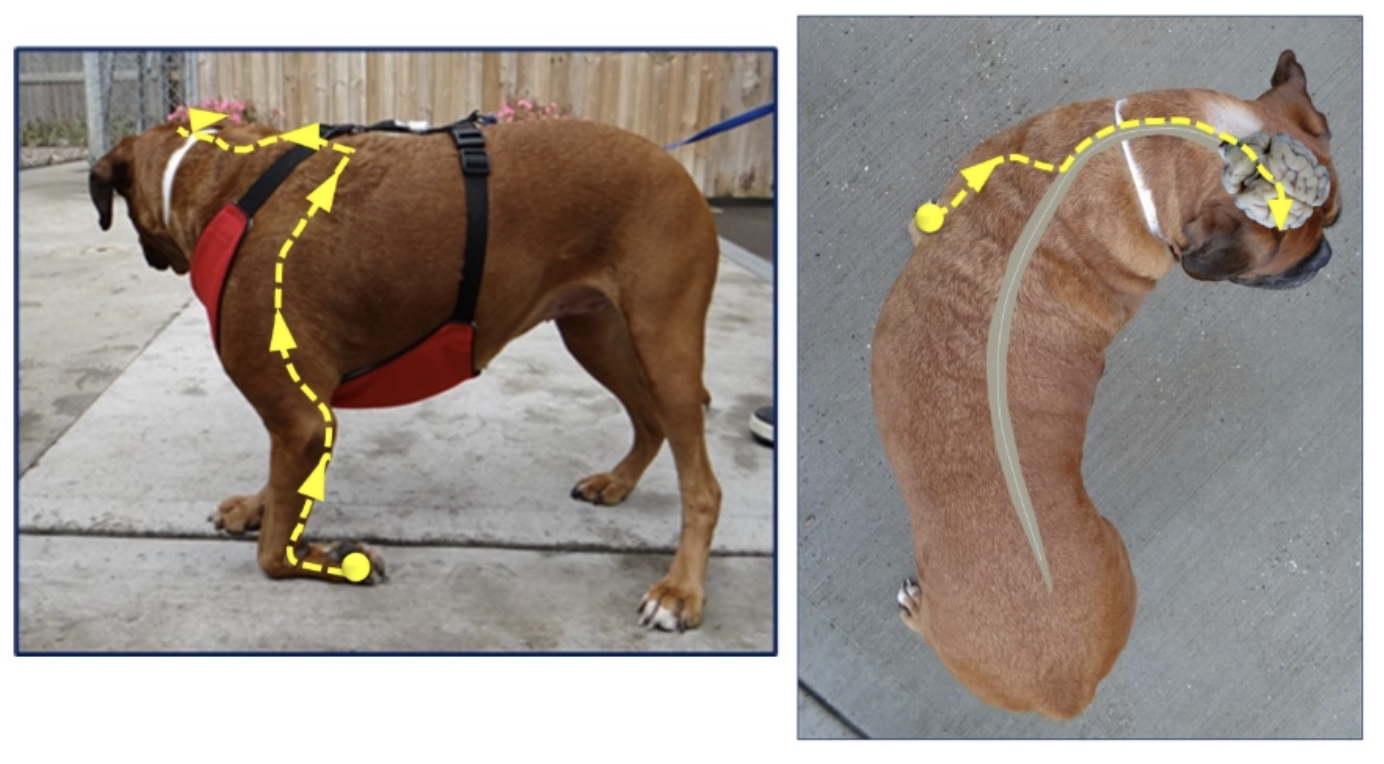
Neurolocalisation: Where is the lesion?
Mild proprioceptive ataxia
Reluctance to turn left
Head turn to right when standing still
Absent paw positing responses in left limbs (does not correct knuckling)
Absent vision/menace response on left
No response when touched on left side of face BUT good palpebral reflex on left
Only ate from right side of bowl
Abnormal processing of information that requires a CONSCIOUS response → Suggests problem with RIGHT forebrain
NOT brainstem because:
Left eye can blink (facial nerve/nucleus normal)
Good palpebral reflex on left (trigeminal nerve → brainstem → facial nerve normal)
Does not track cotton ball on left side which only evaluates visual pathway with several forebrain structures
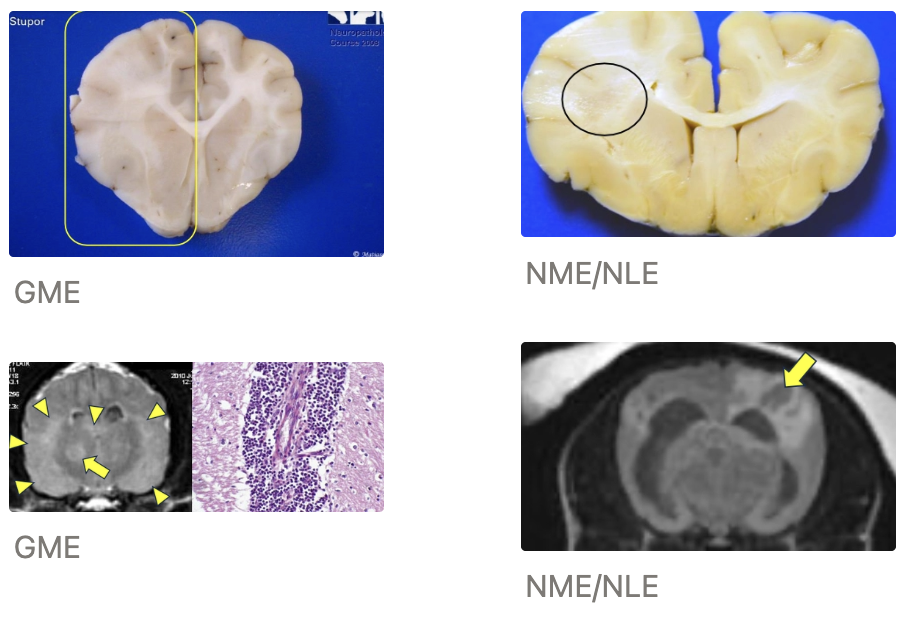
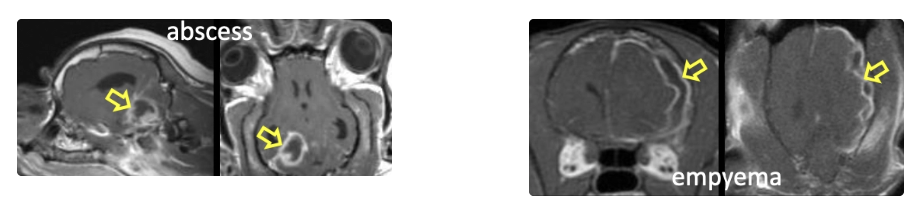
Meningoencephalomyelitis of Unknown Origin (MUO)
2 Types (+ severity)
4 Diagnostic tools
Clinical signs
Signalment (species, age and breed)
Treatment
Prognosis
Types:
Granulomatous meningoencephalitis (GME) = Swelling of brain on MRI → Less severe
Necrotising meningoencephalitis (NME) = Soft tissue loss → More severe
Diagnosis: Presumptive diagnosis based on signalment, history and neurolocalisation →
CSF result (± mononuclear pleocytosis and high protein)
MRI appearance
Response to treatment
Definitive diagnosis requires histopathology to differentiate GME from NME/NLE
Clinical Signs: Multifocal CNS signs with predominant forebrain involvement
± Cranial nerve dysfunction (i.e. brainstem involvement)
Ocular GME form → Involves optic nerve
Idiopathic hypertrophic pachymeningitis (form) → Cranial nerve compression
Signalment: Young to middle-aged dogs (4 - 8yr)
GME: Small breeds (eg. terriers and poodles)
NME: Pugs, Chihuahuas, Maltese, Pekingese, Shih Tze, West Highland White Terriers, Papillons, Coton du Tulear, Griffon Bruxellois
NLE: Yorkshire Terriers, French Bulldogs
Eosinophilic ME: Medium to large breeds
Idiopathic hypertrophic pachymeningitis: Greyhounds/lurchers, labradors
Treatment: Multimodal immunosuppression
eg. Prednisone ± cytarabine, cyclosporine, azathioprine, mycophenolate mofetil
Duration: MONTHS to YEARS with very slow tapering (potentially lifelong)
Cessation of treatment is fatal
Prognosis: Up to 30% mortality BEFORE treatment (survival of 1 - 2 months from diagnosis → May survive years)
Survival depends on MUO severity (worse outcome for NME/NLE)
Better outcomes for treatments than what is published (can only publish with definitive diagnoses of disease which requires PM biopsy and histology)
Potential for permanent deficits
Infectious Disorders of the Forebrain
2 Bacterial infections
3 Viral infections
2 Fungal infections
2 Parasitic infections
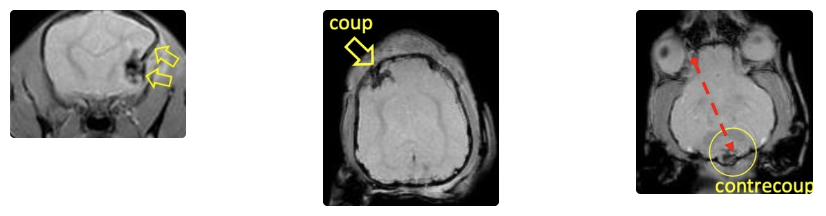
Bacteria:
Abscess = Inflammatory pus walled off (superior drainage)
Empyema = Pus everywhere within cavity with no walling off
Virus:
Canine distemper virus (vaccine-induced in NZ)
Rabies*
Feline coronavirus (FIP)
Fungus: Local extension from nose OR haematogenous spread
Aspergillosis
Cryptococcosis

Parasite:
Protozoal (neosporosis OR toxoplasmosis)
Migrating parasites (eg. Cuterebra*)
Traumatic Disorders of the Forebrain
2 Types of traumatic brain injury
2 Reasons why clinical signs may be multifocal
Types:
Penetrating injury (eg. cat bite)
Blunt trauma (eg. HBC)
Multifocal: Various clinical signs
Haemorrhage
Coup and contrecoup injury
Coup = Brain trauma immediately below site of impact
Contrecoup = brain trauma directly opposite side of impact as brain collides into the back of the skull
6 Example toxins causing forebrain dysfunction
Plant and algal toxins
Anticoagulant rodenticides
Anti-parasitics (eg. flea and worm products)
Care with avermectins in collies (mdr1 mutation)
Recreational drugs (eg. CBD oil and THC)
Human medications (ask owner about human medications eg. anti-depressants)
Iatrogenic/overdose
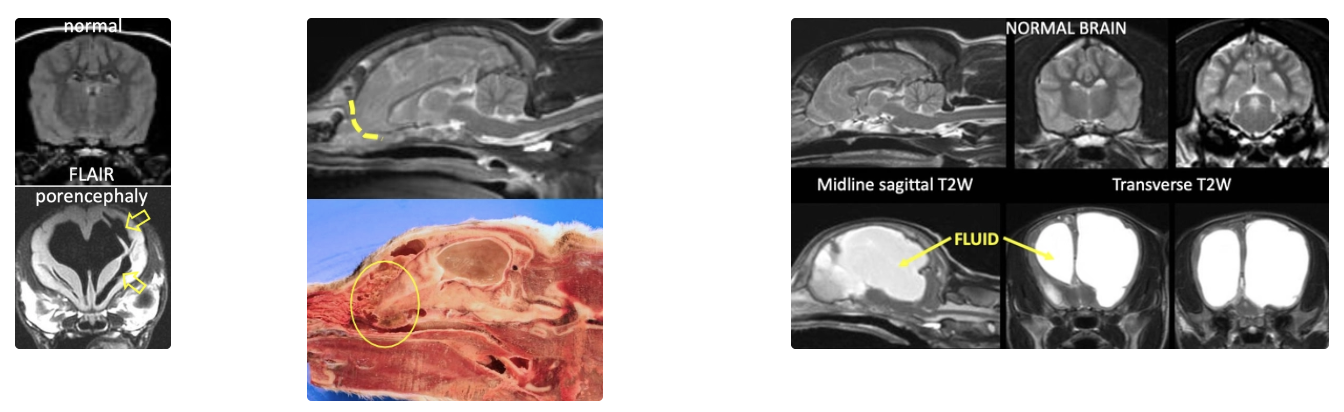
List and define 5 examples of anomalies affecting forebrain function
Porencephaly (small chunks of brain replaced with CSF) or anencephaly (large chunk of brain missing)
Porencephaly more common and often clinically insignificant (vs. anencephaly → Clinical signs)
Meningocele and meningoencephalocele (CSF-filled meninges ± brain protrude through defect in skull)
Post-op OR anomalous
Do NOT poke lump on the head of a young animal (may be meningocele)
Skull malformation
eg. absent cribriform plate → Brain herniates through nasal cavity → Predisposes to dural tearing → Air enters ventricular system
Congenital hydrocephalus and cyst development (eg. quadrigeminal cyst)
Abnormal neuronal migration/neural tract pathways (eg. neurons in abnormal locations or absent neural tract pathways)
List 3 causes of acquired hydrocephalus
Obstruction/slowing of CSF flow (eg. tumours of arachnoid cell infection)
Increased CSF production
Impaired CSF absorption
Congenital Hydrocephalus
Pathogenesis
Clinical signs
Diagnosis
Signalment (species, breed and age)
3 Treatment options
Pathogenesis: Due to mesencephalic aqueduct stenosis (between 3rd and 4th ventricle → Lateral ventricles become enlarged with CSF) #1
3rd ventricle = CSF space encircling the interthalamic adhesion
OR due to impaired reabsorption
Clinical Signs:
Domed head (skull bones not yet fused)
Difficulty training
Abnormal behaviour
Diagnosis: Signalment, history and clinical signs → U/S through fontanelle to visualise excessive CSF (compare with other litter mates)
Do NOT need advanced imaging for definitive diagnosis
Signalment: Small dog breeds (eg. chihuahua, maltese, English bulldog, pug) with clinical signs observed in the first months of life
Uncommon in cats
Treatments:
Medical = Decrease CSF production with prednisolone
Surgical = Shunt CSF into abdomen with drain placed in the ventricle → burrow under skin to exit in the abdomen
-ve:
Infection, blockage, migration, inflammation → Replace regularly
Overdraining CSF → Brain collapse
Similar outcome to medical management
Treat seizures
Electrolyte Imbalances causing Forebrain Dysfunction
Effects of calcium imbalance
Effects of sodium imbalance (+ treatment when chronic)
Calcium:
Hypercalcaemia = Intracellular toxicity → Cell death
Hypocalcaemia = Increased cell membrane excitation → Seizures (eg. lactation)
Sodium:
Hypernatraemia = Cell dehydration → Shrinkage → Shrunken RBCs tear blood vessels → Haemorrhage
Hyponatraemia = Cells swell → Oedema
Chronic sodium imbalance:
Na+ extremes persist for > 2 - 3 days
Brain cells actively produce osmolar substances (osmoles) to compensate for sodium imbalance
RAPID correction of chronic sodium imbalance → Switch to other end of the spectrum
→ Severe oedema OR cell shrinkage + haemorrhage and demyelination
List 4 endocrine diseases causing forebrain dysfunction
Hyperthyroidism (→ flighty cat)
Hypothyroidism (→ slow/sluggish cat)
Diabetes mellitus (→ hypoglycaemic encephalopathy)
Hyperadrenocorticism
Paroxysmal Gluten-Sensitive Dyskinesia
Signalment (breed)
2 Clinical signs
Diagnosis
Treatment
Signalment: Border terrier
Clinical Signs:
Paroxysmal cramping (responsive) lasting 2 - 30 minutes ± abnormal behaviour before/after
± GI signs
Diagnosis: History of GI signs → Serology = Measure anti-gliadin and anti-transglutaminase-2 Ab (NOT in NZ)
Treatment: STRICT gluten-free diet (treatment trial for diagnosis)
List 2 vitamin deficiencies causing forebrain dysfunction
Cobalamin (vitB12)
Thiamine (vitB1) → Vestibular signs with cervical ventroflexion
List 5 primary and 3 secondary nervous system tumours
Primary:
Meningioma
Glioma (eg. oligodendroglioma and astrocytoma)
Oligodendrocyte = CNS myelination
Astrocyte = Structure, homeostasis and BBB
Microglia = CNS macrophages
Ependymoma
Choroid plexus tumour (papilloma and carcinoma)
Schwannoma/nerve sheath tumours
Secondary:
Sarcoma (dog = HSA #1)
Lymphoma (cat #1)
Carcinoma
Meningioma vs. glioma
Meningioma
Extra-axial (OUTSIDE brain)
Slow-growing
Compression > invasion
“Benign”
Glioma
Intra-axial (INSIDE brain)
Relatively fast-growing
Invasion > compression
Canine vs. feline intracranial neoplasia
Prevalence of 1˚ vs. 2˚
Signalment (breed and age) OR common types
Canine
Prevalence: EQUAL 1˚ and 2˚
Signalment: Boxer, Boston terrier, golden retriever, French bulldog
Meningioma → Dolicocephalics and breeds >15kg
Glioma → Brachycephalics
8yr 10m
Meningiomas present when significantly older than other 1˚ tumour types
Feline
Prevalence: 71% of intracranial tumours are 1˚
Most common:
Meningioma
Lymphoma
Pituitary
Neoplastic Disorders of the Forebrain
Clinical sign
4 Treatment options
Prognosis
Clinical Sign: Seizure activity = #1 abnormality noted (generalised seizure with cluster > single > SE)
Treatments:
Surgical resection ± radiotherapy
Radiotherapy
Palliative (corticosteroids, AEDs and analgesia)
Chemotherapy if 2˚ (NOT successful when 1˚)
Prognosis: Depends on tumour type, location, treatment and species
Cats = Tumours shell out → Easy to resect → Long MST before meningioma grows back
Dogs = Tumour removed in pieces → Radiotherapy preferred due to recurrence
Lafora Disease
Pathogenesis
Signalment (breed and age)
5 Clinical signs
Treatment
Pathogenesis: Genetic mutation → Intracellular accumulation of polyglucosan (neurotoxin)
Signalment: Miniature wire-haired dachshund, beagle, basset hound
Middle-aged and progressive
Clinical Signs:
Myoclonic seizure = Single contraction of muscle triggered by visual/audio cues →
Visual impairment
Dementia
Deafness
Aggression
Treatment: Levetiracetam → Myoclonus becomes refractory → Euthanasia
Describe the location and structure of the cerebellum
Location: Within the caudal fossa of the skull, dorsal to the medulla oblongata
Structure:
Vermis = Midline region (vermis = worm)
2 bilateral hemispheres
Paired Peduncles: Stalks made of white matter tracts connecting the cerebellum to the brainstem
Rostral cerebellar peduncle = Connects cerebellum and midbrain (primarily efferent)
Afferent: Spinal cord and midbrain tracts
Efferent: Midbrain (esp. red nucleus), pallidum, thalamus
Middle cerebellar peduncle = Connects forebrain to cerebellum (completely afferent)
Caudal cerebellar peduncle = Connects spinal cord and medulla oblongata to cerebellum (primarily afferent)
Afferent: Spinal cord and vestibular system
Efferent: Vestibular nuclei and reticular formation (inhibition of vestibular nuclei)
Regions:
Cerebrocerebellum (pantocerebellum/nocerebellum) = Regulates skilled movement, planned movements and motor learning
Spinocerebellum (paleocerebellum) = Regulates truncal and limb movements through feedback loops
Vestibulocerebellum (archicerebellum) = Regulates balance, posture and coordination of eye movements
Clinical signs associated with ONE region more likely (vs. vestibular system AND cerebellum)
Receives proprioceptive information but does NOT determine if the animal will correct an abnormal posture
Animal with cerebellar disease SHOULD correct knuckled paw, but exaggerated way
3 Functions of the cerebellum
Coordination (controls rate, range and force of movement)
Equilibrium (regulate muscle tone at rest or during motion through close association with vestibular system)
Inhibit urination
Does NOT initiate movement: Cerebellum involved in multiple feedback loops to regulate movements
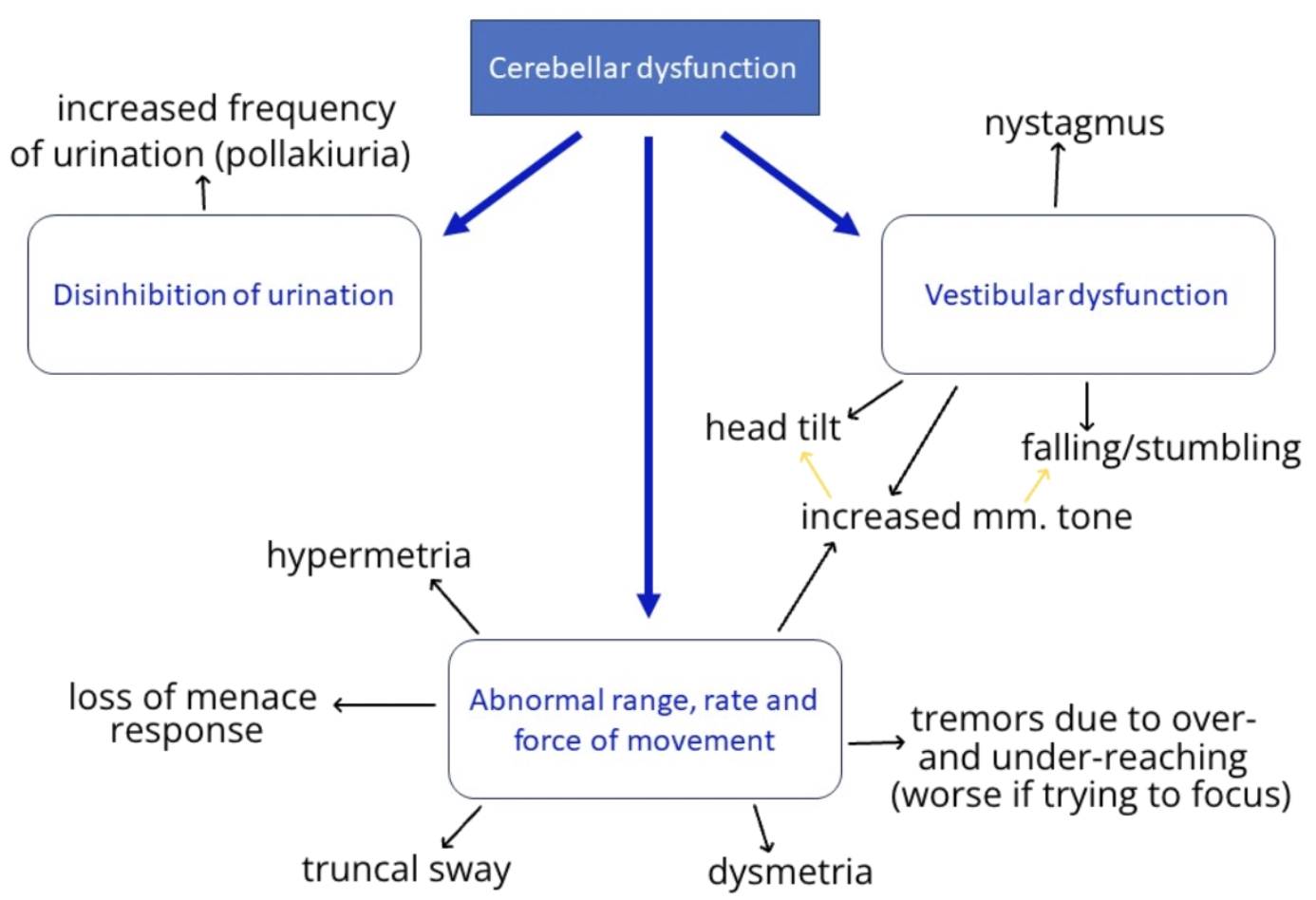
Describe 5 clinical manifestations of cerebellar dysfunction (+ normal)
3 Regions + Absent menace and pollakiuria
Cerebrocerebellum dysfunction = Movements not synchronised → Overshooting intended movements
Dysmetria = Loss of control of range, rate and force of movement → Cerebellar ataxia
Intention Tremours = Manifestation of loss of control over range and force of planned movements which worsen with concentration
Alternating over-reaching and under-reaching movements → Oscillation
Cerebellum required for planned movements, therefore, more planning → More difficulty accomplishing task
Refractory to diazepam
Spinocerebellum dysfunction = Exaggerated truncal and limb movements
Hypermetria = Excessive lifting of lower limbs when ambulating (“marching” or “prancing” gait)
Increased limb tone = Spasticity → Stumbling/falling
Vestibulocerebellum dysfunction = Loss of equilibrium/balance
Truncal sway, wide-based stance, falling to one side, head tilt ± strabismus and nystagmus
No menace response
Pollakiuria
Normal:
Mentation (no forebrain involvement)
Paw positioning (exaggerated)
Transient Ischaemic Attack on the Rostral Cerebellar Artery
Clinical signs and duration
Diagnosis
3 Causes
Clinical Signs: Vestibulocerebellar OR purely cerebellar signs which typically self-resolve after <24hr
Small clots → Short signs (minutes to hours)
Large clots → Lasting signs (days to weeks)
Diagnosis: Markedly elevated D-dimers → Presumptive diagnosis (must be run on 1st sample)
Causes:
Infarction
Brain tissue compression
Cardiac arrest/vessel compression
List 6 causes of haemorrhage into the nervous system
Coagulation disorder
Trauma
Haemangiosarcoma metastasis
Parasitic (migration tract of Angiostrongylus vasorum*)
Cerebral microbleeds
2˚ to another lesion (eg. tumour or inflammation)
Corticosteroid-Responsive Generalised Tremour Syndrome (aka. Idiopathic Tremour Syndrome)
Aetiology
Signalment (species, breed, age)
3 Diagnostic tools
2 Treatments
Aetiology: Immune-mediated inflammation of the cerebellum
Signalment: Small/medium dogs (<15kg) @ 1 - 5yr (often <2yr)
Diagnosis: Signalment, history and neurolocalisation →
Normal brain on imaging
Response to treatment
± Mild to moderate lymphocytic pleocytosis on CSF analysis
Treatments:
Immunosuppressive doses of corticosteroids and diazepam → Improvement within 3d
Max 5 days diazepam
Taper prednisolone over 6 months → Discontinuation
Spontaneous remission possible after several months
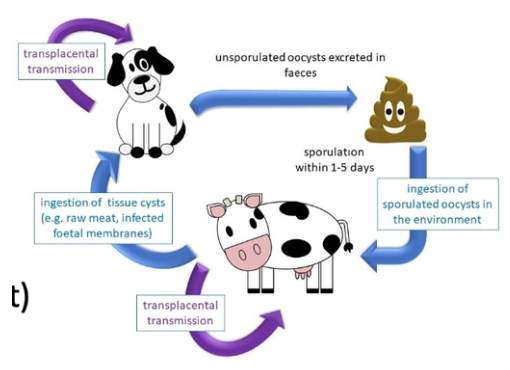
Neosporosis
Prevalence
2 Modes of transmission
Pathogenesis in puppies vs. adults (+ clinical signs)
2 Treatment options (+ duration)
Prevalence: 76% seroprevalence in urban dogs (22 - 100% in farm dogs)
VERY common in NZ
Transmission:
Vertical (transplacental)
Horizontal (ingestion of infected tissues eg. raw meat)
Pathogenesis:
Puppies = Protozoal myositis-polyradiculoneuritis → Ascending HL paresis and rigid hyperextension
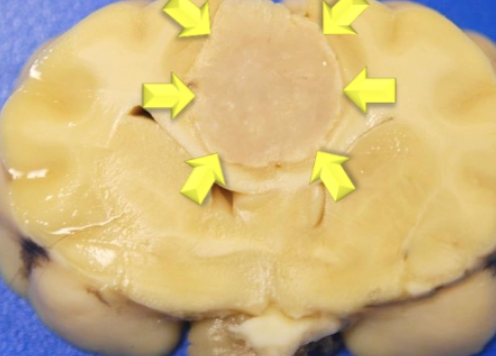
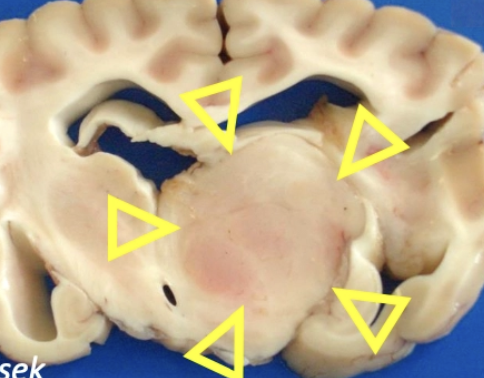
Adults = Protozoal encephalomyelitis → Necrotising cerebellitis
Treatments: FOUR weeks of
Clindamycin and/or
TMS
List 2 degenerative diseases targeting the cerebellum
Spinocerebellar ataxia (JRTs, Parson Russel Terriers)
Cerebellar cortical degeneration (abiotrophy)
Many other degenerative neurological diseases have a cerebellar component
Genetic tests may be available
Non-Cerebellar Head Tremours (aka. Idiopathic Head Tremours)
Signalment (breed, age)
Clinical signs
Prognosis
Signalment: Bulldog, boxer and dobermans <4yr
Clinical Signs: <5 minute episodes (may be up to several hours) which typically occur at REST and improve with distraction, supporting head or turning head in opposite direction
Prognosis: Episode resolves over time in most dogs
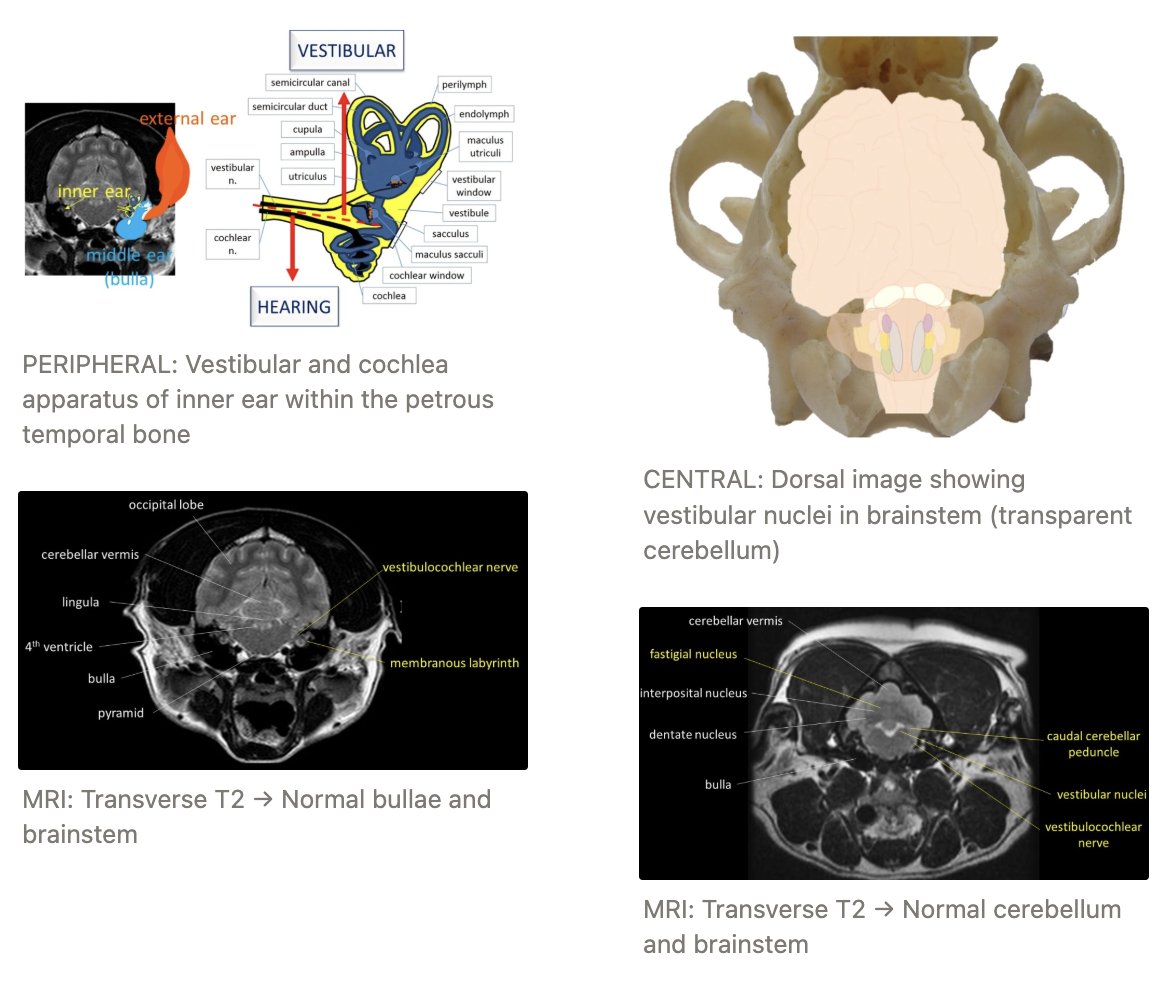
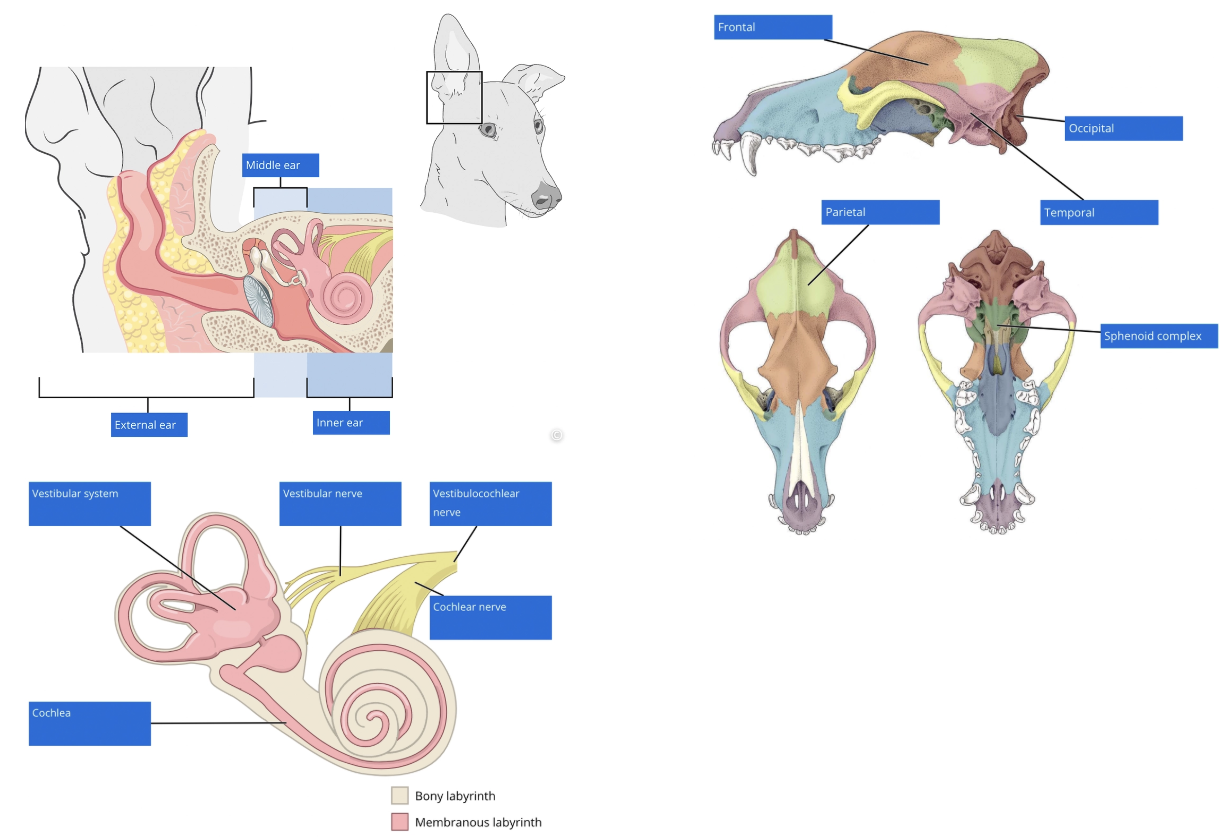
Describe the structure and location of the vestibular system
Structure:
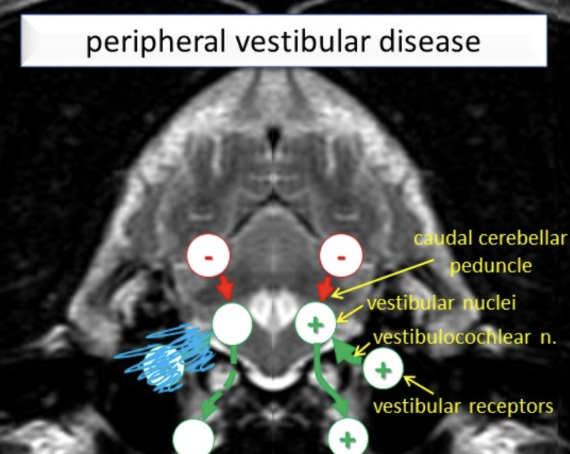
Peripheral vestibular system = Vestibular receptors within the inner ear + vestibular component of the vestibulocochlear nerve (CN VIII)
Central vestibular system = Vestibular nuclei within the brain stem + vestibulocerebellum
Some axons leave CN VIII → Caudal cerebellar peduncle → Fastigial nucleus in cerebellum
Function of vestibulocerebellum: Feedback loop for regulation of balance and posture
Some cerebellar neurons travelling through the caudal cerebellar peduncle INHIBIT vestibular nuclei (interruption of this inhibitory pathway → PARADOXICAL vestibular syndrome)
Location: Inner ear located in the petrous temporal bone
Cochlear nerve + vestibular nerve → Vestibulocochlear nerve (CN VIII)
2 axons of the vestibulocochlear nerve separate at the brainstem to travel to their respective nuclei
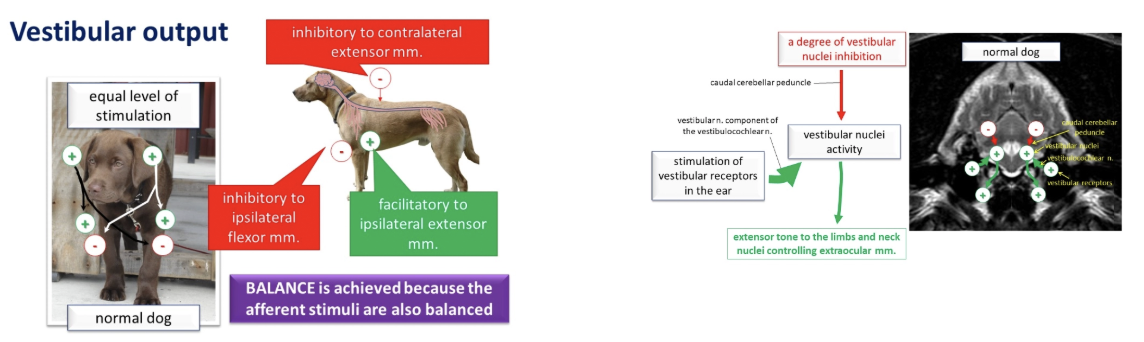
5 Outputs of the vestibular system
Upper motor neuron spinal cord tracts to correct changes in body position
Turning heads to the RIGHT:
Increased vestibular activity on the right side → Increased stimulation of RIGHT vestibular receptor
→ Vestibular system causes the following to prevent falling over: Extension of ipsilateral limb and flexion of contralateral limb
Stimulation of ipsilateral (RIGHT) extensor muscles
Inhibition of ipsilateral (RIGHT) flexor muscles
Inhibition of contralateral (LEFT) extensor muscles
Nuclei of CN III (oculomotor), IV (trochlear) and VI (abducens) to control eye movements
Cerebellum to coordinate movement of eyes, neck, trunk and limbs with respect to movement of the head
Cerebrum (via the thalamus) for conscious perception of balance
Occasional vestibular dysfunction due to thalamic pathology (forebrain dysfunction)
Vomiting centre of the brainstem
What is nystagmus? What is its purpose?
Nystagmus = Normal physiological reflex whereby eyes tend to flick towards the direct the head is turning and then move slowly in the opposite direction (left/right/dorsal)
ONLY when head is changing position (no nystagmus when still → Pathological nystagmus)
aka. vestibulo-ocular reflex
Purpose of physiological nystagmus: Allows line of sight to remain still as the head turns for as long as possible → Time for retinas to capture clear image before eyes flick again → Prevents vision blurring while moving head
Describe 3 clinical manifestations of vestibular system dysfunction (+ pathogenesis)
PEN
Postural and Gait Abnormalities = Head tilt, rolling/falling/tight circling, vestibular ataxia, wide-based stance with lowered centre of gravity
Abnormal Eye Movements
Spontaneous/resting nystagmus = Brain triggers nystagmus as it thinks the head is turning (pathological)
Horizontal OR vertical with fast phase in one direction and slow phase in the opposite
Pendular nystagmus = Spontaneous nystagmus in normal, blue-eyed cats due to abnormal proportion of optic nerve axons crossing the optic chiasm (no lateralisation)
Positional nystagmus = Head position must be changed to trigger pathological nystagmus
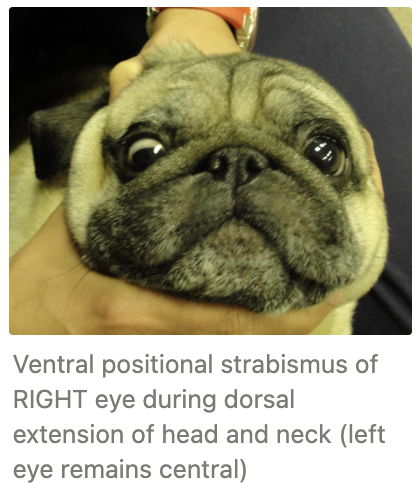
Positional strabismus = Abnormal position of eye within orbit due to change in head position
NORMAL: Gaze remains central when head and neck extend dorsally (vs. horses)
Loss of vestibular function: Extraocular muscles on affected side fail to maintain central gaze → Ventral positional strabismus of affected side
Static strabismus = Abnormal eye position at ALL times (due to orbit conformation or mechanical dysfunction of the extraocular muscles)
Nausea
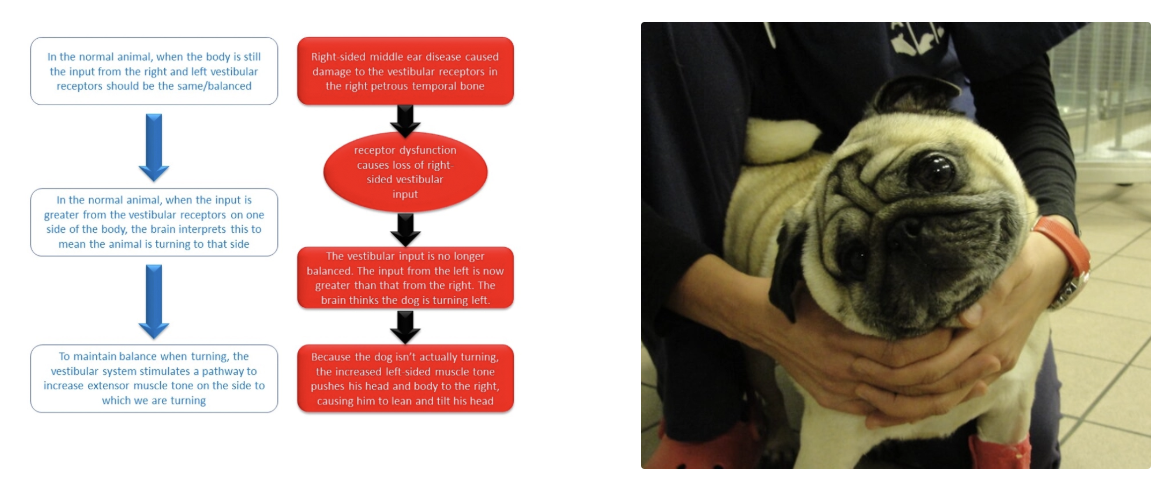
Pathogenesis:
Pathological lesion → Loss of input from vestibular receptors/loss of vestibular nuclei function on ONE side
→ Less vestibular activity on that side
→ Comparatively more vestibular activity on the CONTRALATERAL side
Brain cannot differentiate between an imbalanced vestibular system due to turning OR pathology → Normal vestibular stimulation results in ABNORMAL posture and movements
→ Increased extensor muscle tone on side of greater activity
BUT because the animal is NOT turning, it causes them to lean/fall/circle/roll towards side of lesser vestibular activity
Tight circling to due stumbling and falling off balance
Increased extensor tone of neck on side of greater activity pushes the head to the other side causing head tilt TOWARDS the side of less vestibular activity
List and describe 3 types of ataxia
Vestibular ataxia = Usually unilateral
Bilateral = Crouching, reluctance to move, side-to-side head movements, wide-based stance, alterating rotation of head
Cerebellar ataxia = Dysmetria and hypermetria (over-reaching/high-stepping)
Proprioceptive ataxia = Scuffing paws, swaying gait, wide-based stance, long-limbed strides
Describe how you could neurolocalise for a dog with no menace response
Menace Response Pathway:
Afferent = Retina, optic nerve, cerebellum, brainstem
Site of processing = Forebrain
Efferent = Facial nerve and muscles of the eyelids
Other Tests that Overlap with the Pathway:
Retina/Optic Nerve = PLR (bypasses forebrain) and electroretinography (ERG)
Visual Pathway = Maze testing or visual tracking
Forebrain = Nasal sensation, proprioception test
Cerebellum = Hypermetria/tremours?
Facial nerve and Eyelid Muscles = Palpebral reflex
Where do ascending nerves decussate?
AFTER the thalamus: In the forebrain, information is processed on the CONTRALATERAL side to the stimulus (brainstem, cerebellum and spinal cord → IPSILATERAL deficits)
Provide definitions for the following terms
Term | Definition |
|---|---|
Ataxia | |
Paresis | |
Paralysis | |
-plegia | |
-paretic | |
Tetra- | |
Para- | |
Hemi- | |
Mono- |
Term | Definition |
|---|---|
Ataxia | Incoordinated movement, wobbliness and poor control of ambulation due to sensory dysfunction |
Paresis | Motor weakness of limbs → Partial loss of motor function |
Paralysis | Complete loss of voluntary motor function → Inability to move (BUT reflexes may be present) |
-plegia | Paralysis |
-paretic | Paresis (muscle weakness) |
Tetra- | Affecting all FOUR limbs |
Para- | Affecting hindlimbs |
Hemi- | Affecting limbs on ONE side |
Mono- | Affecting only ONE limb |
5 Grades of spinal injury
Grade:
0 = Normal animal
1 = Pain from lesion ONLY (no neurological signs)
2 = Ataxia OR ambulatory paresis → Muscle weakness
3 = Non-ambulatory paresis → Partial loss of motor function (residual movement eg. wants to walk if supported off ground)
4 (IVa) = Plegia and motor paralysis → Complete loss of motor function
5 = Loss of pain sensation
Cutaneous (IVb) = Superficial pain (eg. pinching skin or webbing)
Periosteal (IVc) = Deep pain (eg. pinch P3 within base of claw OR long bone with crushing clamp over tibia)
Deep pain fibres are last to be damaged → Loss of deep pain sensation = Most severe spinal injury
Superficial pain fibres slightly easier to be damaged as larger and myelinated
Motor nerves very easy to be damaged → Conscious movement (eg. walking) requires function of the UMN and LMN → 2nd thing to disappear (after ataxia and conscious perception)
List 5 types of spinal cord injuries requiring surgery (+ 3 example DDx)
Intervertebral disc disease (IVDD Type I/II)
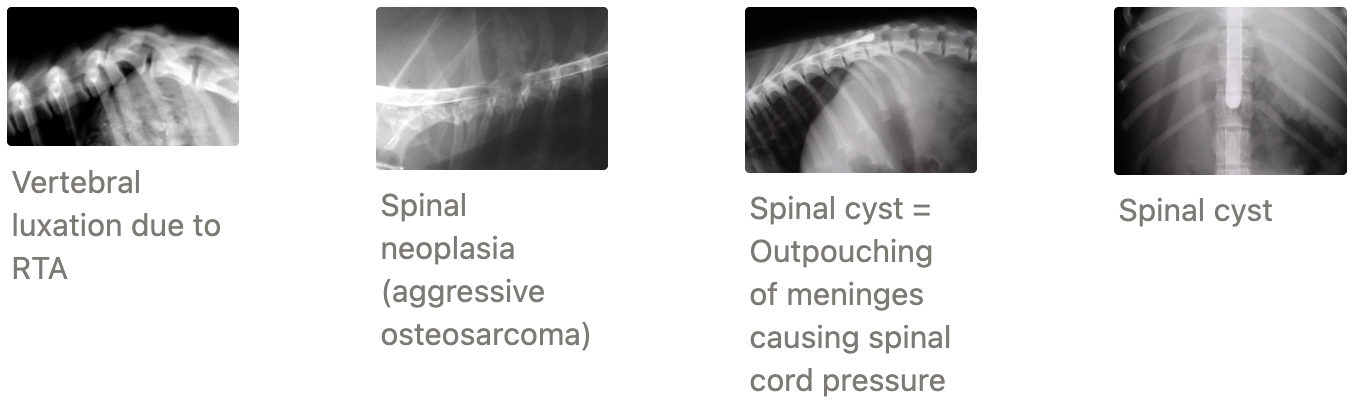
Spinal fracture/luxation (eg. HBC)
Spinal tumour
Spinal abscess
Spinal cyst
Examples:
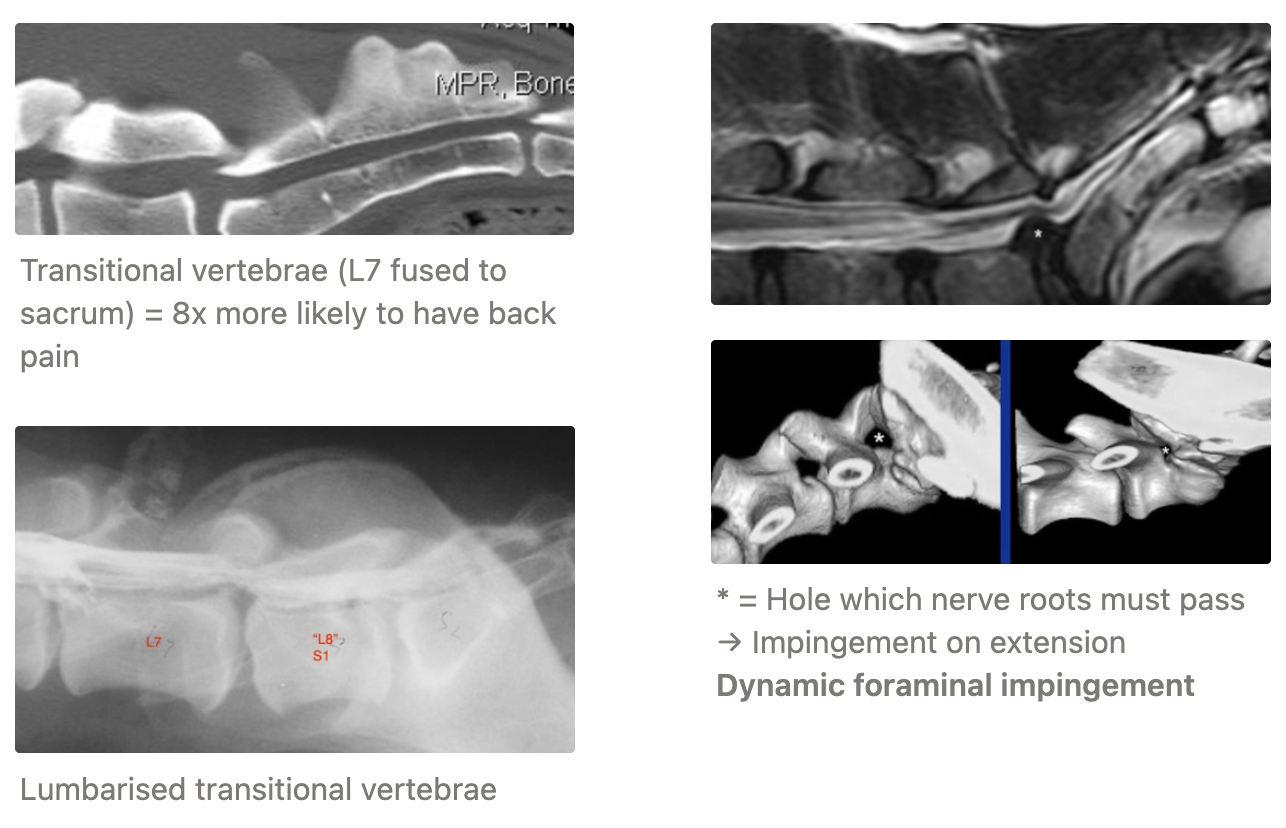
Lumbosacral disease (aka. Cauda Equina Syndrome)
Caudal Cervical Spondylomyelopathy (aka. Wobbler’s Syndrome)
Atlantoaxial instability
Describe the anatomy of a vertebra and intervertebral disc
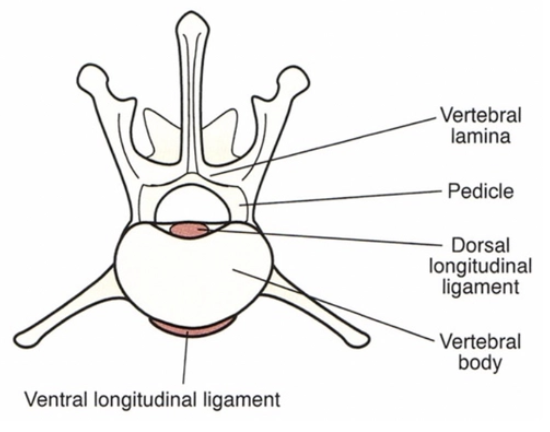
Vertebra:
Vertebral lamina = Roof of the vertebral canal
Intervertebral foramen = Hole between two adjacent vertebrae to allow nerves to pass from the spinal cord
Pedicles = Help encase the spinal cord and acts as a bridge between the vertebral body and the rest of the vertebra
Intervertebral Disc: Fibrocartilaginous disc between bodies of each pair of vertebrae to act as shock absorber and prevent damage to the spinal cord during movement
Annulus fibrosus = Outer area of tough fibrous connective tissue (concentric rings of collagen)
Nucleus pulposus = Inner core of gelatinous material
List 5 surgeries to treat neurological disease
Decompression = Remove pressure on spinal cord via removal of disc, clots, bone, cyst fluid or tumour mass
Stabilisation of spine = Required due to movement from disc degeneration or luxation from trauma
Stabilisation and decompression of fractures
Drainage and curettage of discospondylitis
Biopsy or removal of spinal cord/brain tumours
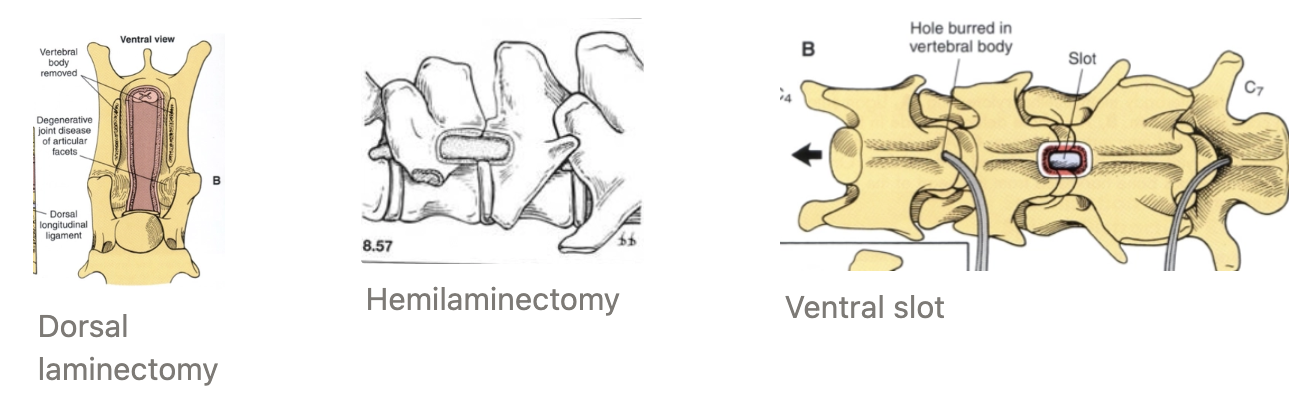
3 Surgical approaches to the spinal cord
Definition
Indication
Dorsal laminectomy = Removal of vertebral lamina (vertebral bone dorsal to spinal cord)
Indication: Dorsal lesions → NOT discs as too ventral
Hemilaminectomy = Removal of vertebral lamina on ONE side and lateral to the spinal cord
Indication: Disc disease
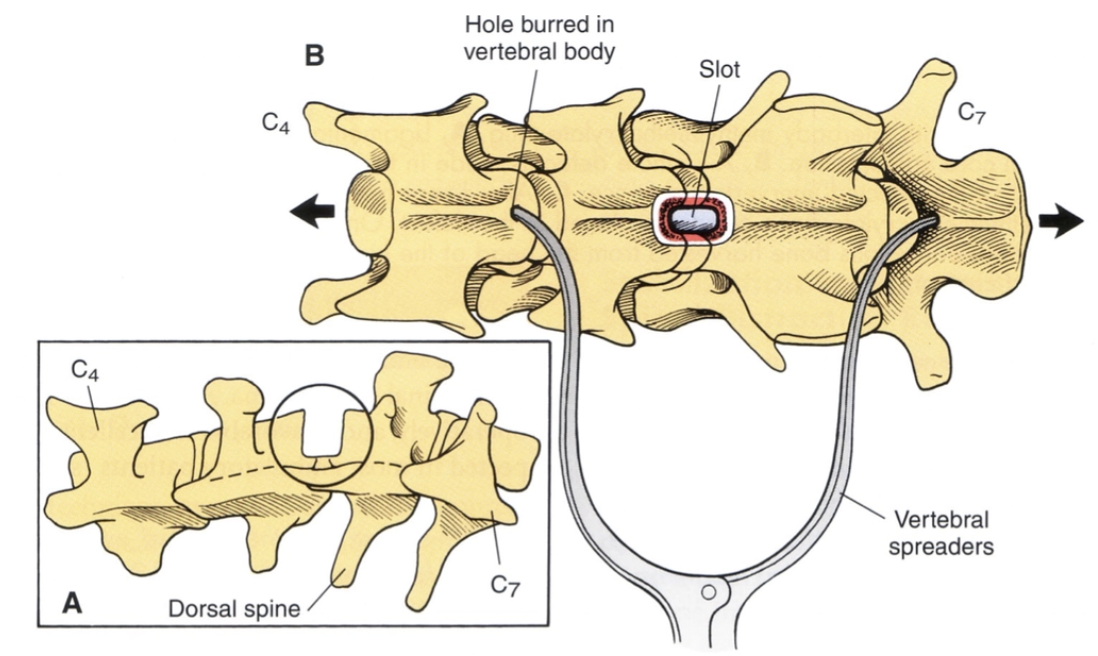
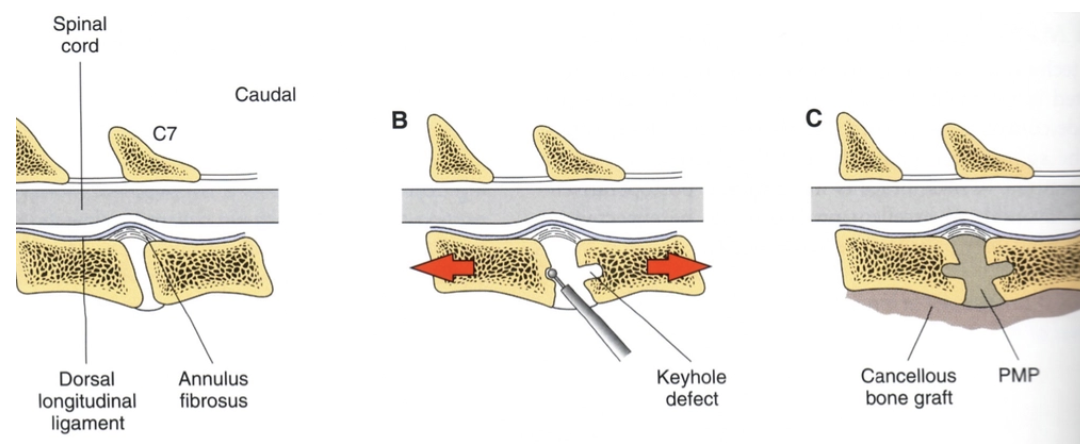
Ventral slot = Removal of rectangular portion of bone and intervertebral disc ventral to spinal cord → Push everything out of the way first
Indication: Access cervical vertebrae
List and describe 4 diagnostic methods for spinal cord injury
Plain radiographs: Assess for
Narrow intervertebral disc space → IVDD
Calcified disc → IVDD (usually cannot see disc if not calcified)
Fractures and luxations
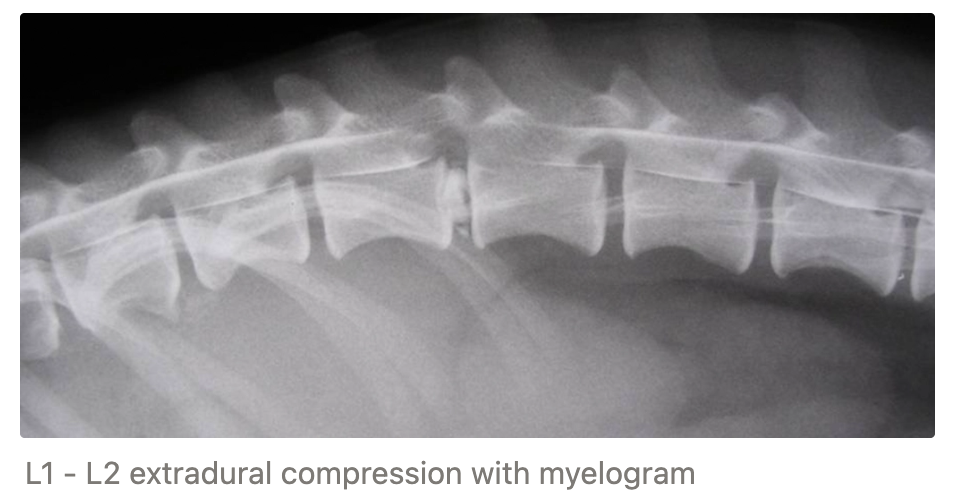
Myelography = Injection of water-soluble iodine contrast into the subarachnoid space
-ve: NOT common now due to high risk of seizures and spinal cord injury → Superseded by advanced imaging modalities
Sites:
Lumbar puncture
Cisterna magna
CT → Fracture diagnosis
MRI → Tumour diagnosis
Spinal Patient Care
5 Steps of pre-operative TRANSPORT care of spinal patients
2 Features of pre-operative IN-HOSPITAL care of spinal patients
7 Features of conservative management and post-op care
3 Features to monitor for (+ treatments)
Transport:
Handle with EXTREME care (poor handling → increases injury severity AND causes struggling if hurt)
Advise owner to gently slide onto sheet/coat/towel
On arrival, if dog is non-ambulatory, strap down with tape onto board to carry
Small dogs and cats can be carried by supporting backs in neutral position
Keep animal taped down to board until radiographs have been taken to rule out spinal injury
Pre-Op Care:
Total cage rest for 2 - 4w (analgesia and no cage rest → further herniation)
Analgesia (opioids OR NSAIDs)
Post-Op Care:
Intensive nursing care to avoid bed sores, decubital ulcers and muscle atrophy
Padded bedding (eg. water bed or air mattress)
Regular turning and periods in sternal recumbency if plegic
Passive flexion and extension physiotherapy
Active supported standing physiotherapy
Hydrotherapy (combine with bathing)
Access to feed and water → Monitor intake and assess weight changes + hydration status
Monitor:
Urination → Expression needed if UMN bladder
Repeated catheterisation (males)
Indwelling closed system (females)
Diazepam → Decreased external skeletal muscle sphincter tone
Phenoxybenzamine → Decreased internal smooth muscle sphincter tone
UTI → Common with spinal patients due to catheterisation and/or retained urination
Longer hospitalisation → Higher risk of UTI
Therapeutic antibiotics (empirical → culture and sensitivity of catheter)
Defaecation → Usually voluntary (otherwise microenemas)

Which drug should NEVER be given to spinal patients? Why?
NEVER give dexadreson = Most dangerous corticosteroid
-ve: Fatal colonic perforation in dogs with thoracolumbar disease → Septic shock
Can give low dose prednisolone for inflammatory aetiologies
Intervertebral Disc Disease (IVDD)
Definition
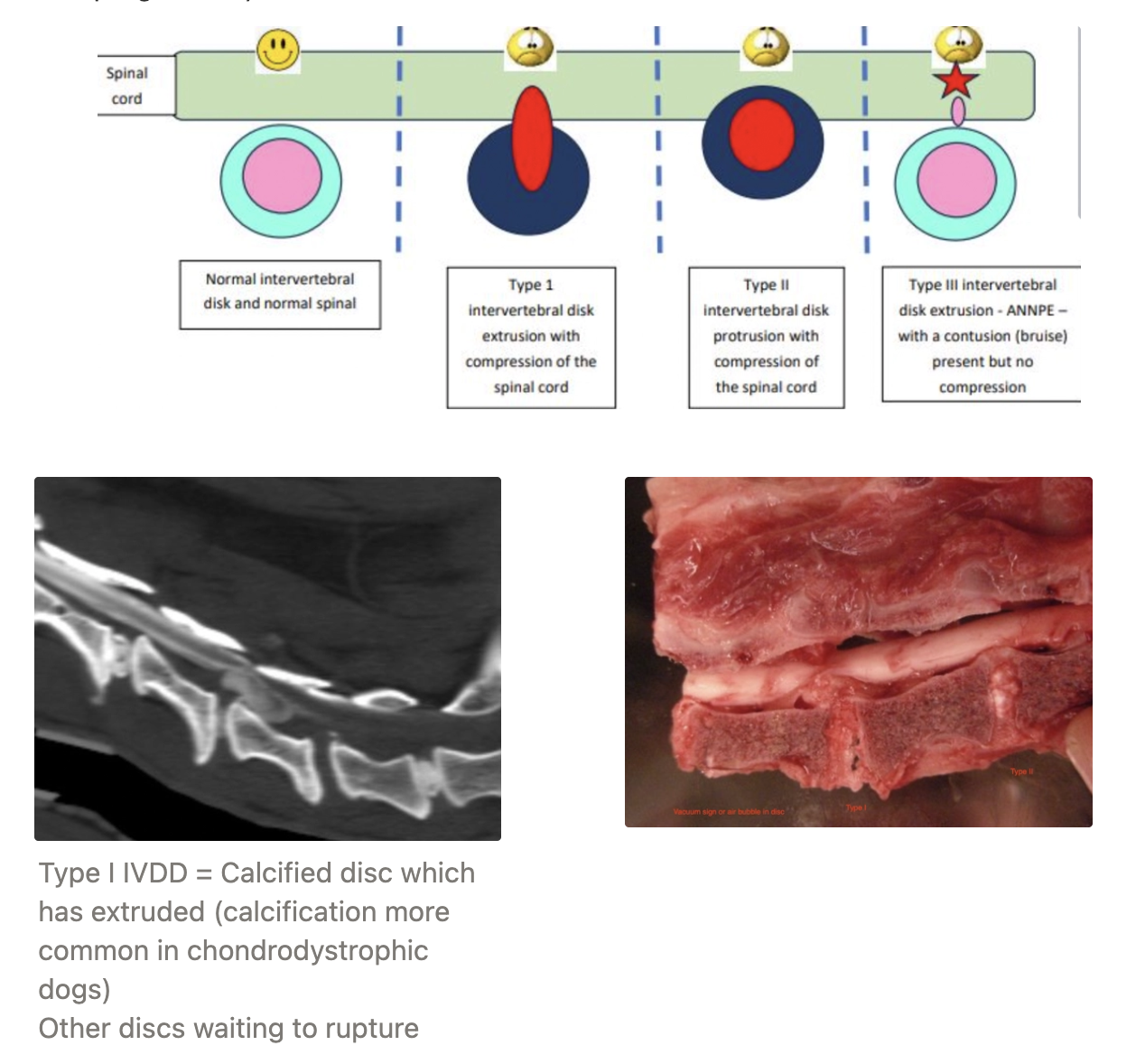
3 Types
Definition
Clinical features
Signalment
Definition: ANY type of cord compression due to intervertebral disc herniation (dorsal annulus fibrosus thinnest)
Types:
Hansen’s Type I IVDD (extrusion) = NP pushes through AF into vertebral canal
→ Compression AND contusion
Acute ± progressive (grade 1 - 5 presentation)
Signalment: Chondrodystrophic breeds which deteriorate discs earlier in life (eg. Beagle, spaniel, dachshund) @ ~3 - 6yr
Acute Non-Compressive Nucleus Pulposus Extrusion (ANNPE) aka. Type III = Low volume, high velocity (bullet-like) NP shoots through the AF and hits the spinal cord → Disperses around spinal cord (no space occupying lesion and nothing to remove)
→ Contusion
Peracute and non-/mild progressive
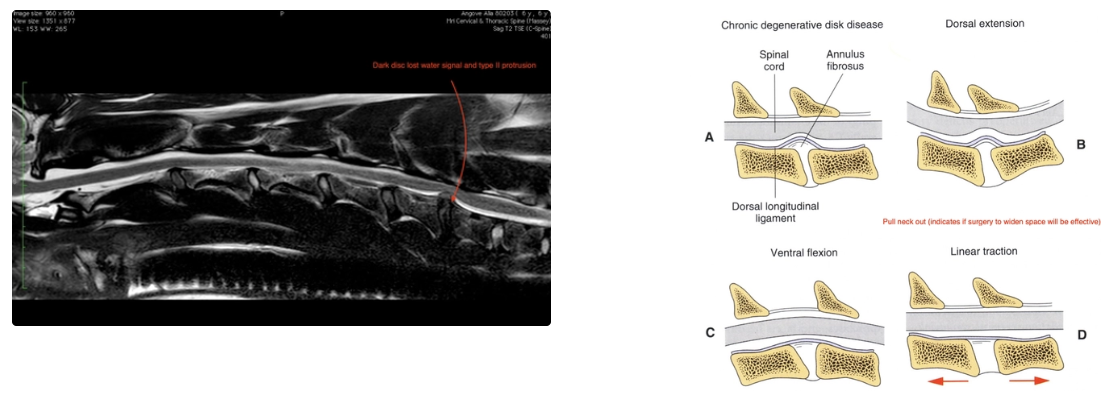
Hansen’s Type II IVDD (protrusion) = Hypertrophic AF bulges into the vertebral canal
→ Compression
Insidious, static OR progressive (earlier grade presentation due to slow progression)
Signalment: Non-chondrodystrophic breeds (ANY old dog due to normal disc degeneration throughout life = Water loss of NP → Bulging of AF
5 GP vet roles in IVDD
Rapid recognition of clinical signs
Localise lesion site
Assess severity and relate to prognosis for owner
ID cases requiring surgery vs. those that can be managed conservatively
Rapid referral to neurosurgeon
Taking radiographs is NOT necessary
Cervical IVDD
Typical grade of severity
2 Indications of surgical treatment
2 Disadvantages of conservative management of cervical IVDD
2 Methods of surgical treatment
Advantage
Disadvantage
Grade: Lower neurological grade as those more severe cannot move respiratory muscles → Euthanasia due to respiratory arrest
Indications for Surgery:
Lack of response to conservative treatment (still painful) after 1 - 2w
ALL dogs with neurological deficits (grade 2 - 5)
-ve of Conservative Management:
Significant pain due to mobile neck (faster recovery from pain post-op)
30% recurrence with conservative treatment
Surgical Methods:
Ventral Fenestration = Remove window of annulus to free nucleus
+ve: Easy to perform
-ve: NOT recommended in all cases with neurological disease
Ventral Slot Decompression = Remove disc material from spinal canal via removal of central 1/3rd of body via ventral approach
+ve: Faster recover
-ve: Stabilisation NOT performed in most cases
Thoracolumbar IVDD
Most common segments affected
Diagnosis
Indication for conservative management
3 Advantages of surgical treatment of thoracolumbar IVDD
3 Surgical methods
Segment: >50% at T12 - T13 OR T13 - L1
85% between T11 - T112 and L2 - L3
→ Lever arm at junction of thoracic and lumbar vertebrae
Diagnosis: Localisation of lesion from neurological exam → Radiographic and myelogram to determine site (lack of horse head intervertebral foramen shape)
Conservative Management: Indicated for lower grades of spinal injury and financial/equipment constraints
+ve of Surgical Treatment:
Faster recovery and better outcome for grade II - IV
Grade V must be operated ASAP (7% success with conservative management)
Less risk of residual neurological deficits
Surgical Methods:
Dorsal or dorsolateral approach for:
Hemi-laminectomy #1
Mini-hemilaminectomy (minimal approach)
Pediculectomy minimal approach
→ Retrieval of disc material and blood clots which is decompressive AND reduces inflammation
Remove overlying lamina to allow cord to bulge with no compression
Prognosis for Type I IVDD (grade I - V)
Conservative % recovery (wks)
Decompression % recovery (wks)
Grade | Conservative | Surgical |
I | 100% (3w) | 97% (<2w) |
II | 84% (6w) | 95% (<2w) |
III | 93% (6w) | 95% (<2w) |
IV | 81% (9 - 12w) | 95% (1 - 4w) |
V | 7% | 64% (5 - 10w) |
Grade I = Good response to conservative management BUT common relapse (investigate recurrent pain)
Grade I - II is good with conservative management
Good recovery for dogs with grade I to III
Recurrent after conservative therapy → More severe deficits later
Higher grade = Better surgical prognosis and worse conservative prognosis
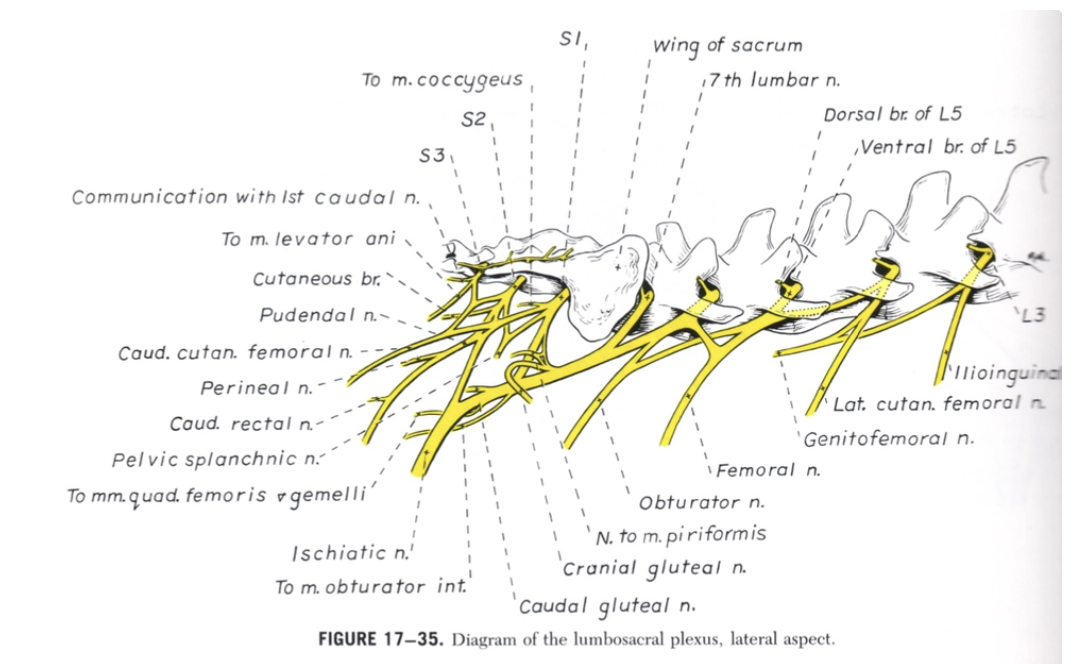
Describe the anatomy of the cauda equina
Bundle of spinal nerve roots at the end of the spinal cord derived from L5 - S2
Dog spinal cord proper ends BEFORE vertebral column → Continues as the cauda equina to supply the caudal segments of the body
20% of dogs have the conus medullaris ending BEFORE the lumbosacral space
Overview of Cauda Equine Syndrome
Definition
5 Clinical signs
5 Imaging modalities
Most common DDx
Definition: Presentation of lumbosacral disease with MULTIPLE different causes → Compression of spinal nerve roots (NOT spinal cord) of the cauda equina
eg. empyema due to grass seed
Clinical Signs:
Lumbosacral pain
Tail Jack (-ve: Many normal dogs do not tolerate → False positives)
Pelvic Tilt = Cradle pelvis with one hand and place other hand over back to act as fulcrum → Extension of back and NOT back legs (+ve: Best test with highest DSp)
Lordosis Test = Concurrent hip AND back extension (-ve: Must test hip pain first to rule out possible cause of possible lordosis test)
Nervous Dog = Place in lateral recumbency with knee in back while attempting to bring dog’s knees caudally to extend back
Difficulty jumping or climbing stairs (may walk normally, but hold hindlimb up after jumping into car/upstairs = Dynamic impingement of nerve)
Rare incontinence (severe signs)
Hindlimb ataxia but NOT paralysis
Femoral nerve (L4 - L6) has already passed out intervertebral foramen innervate hindlimb motor function before cauda equina is compressed
Sciatic nerve (L7 - S1) has yet to pass out of the intervertebral foramen → Dragging hindlimbs but not paralysis
LMN hindlimb signs and normal forelimbs = Decreased reflexes, poor muscle tone and neurogenic muscle atrophy in hindlimbs
Imaging: Dynamic views with flexion AND extension of back (differentiate between static vs. dynamic)
Plain radiographs
Myelogram (conus medullaris ends before lumbosacral space in 20% of dogs)
Epidurogram (difficult to interpret)
Discogram (inability to inject is diagnostic)
MRI #1 for lateralised disc material
BUT 20% normal dogs have false positive → Interpret with clinical signs
Most Common DDx: Degenerative Lumbosacral Stenosis (DLSS)

Degenerative Lumbosacral Stenosis (DLSS)
Signalment
Pathogenesis (4 causes of pain)
3 DDx
2 Treatment options
Signalment: Large working dogs (eg. GSD) required to jump into cars often
Pathogenesis: Extension/overuse of back → Pain due to
Nerve impingement
Type II IVDD → Compression of cauda equina
All dogs have a lumbosacral disc bulge, but not all cause pain → Over diagnosis of DLSS with radiography
Articular facet DJD
Instability/subluxation of lumbosacral joint
DDx:
Sore muscles (eg. torn semitendinosus or iliopsoas muscle)
Strains
Hip displasia
→ Get dog to jump into car or walk upstairs to place stress on lumbosacral region
Treatment:
Conservative Management (as for DJD + lifestyle modification eg. purchase ramp for car and stop running up stairs)
NOT for working dogs
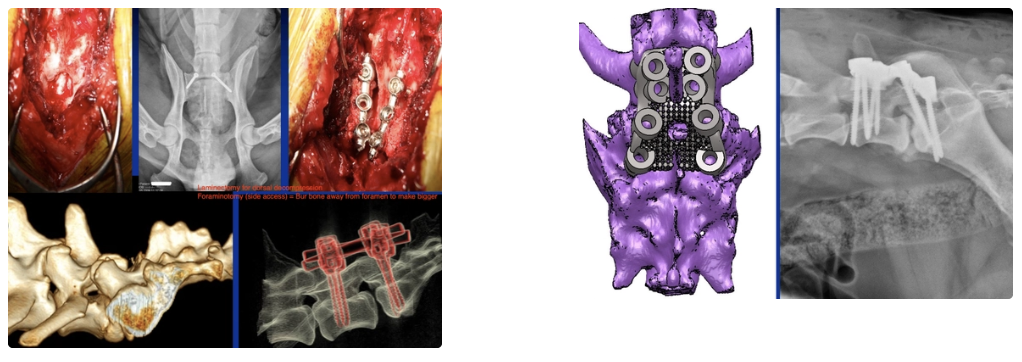
Surgical = Decompression ± stabilisation
Decompression and removal of impinging soft tissue ± stabilisation by facet screws
Laminectomy or foraminotomy
± 3D printed jack for screw placement of internal fixation between L6 and S1
Caudal Cervical Spondylomyelopathy (Wobbler’s Syndrome)
2 Signalments (+ type of disease)
3 Clinical signs
2 Imaging modalities (+ features)
3 Treatment options
Indication
Prognosis with surgical treatment
2 Post-op risks
Signalment:
Middle-aged (~5yr) Doberman = Disc-associated wobblers (type II IVDD)
Young Great Danes = Osseous-associated wobblers (cervical vertebral malformation → improvement OR waxing/waning)
Clinical Signs: Progressive but waxing/waning
Ataxia of HL → FL (chronic)
Despite cervical lesion, absent forelimb ataxia is common in early disease
Neck pain
Rare tetraplegia
Imaging:
Plain radiographs
Narrowed IVD space between C4 - T1 (usually C6/7 or C5/6)
Plowshare-shaped vertebrae → Abnormal force of disc
Spondylosis
Stenosis of canal at disc space
Cervical myelography with CT → Referral but required due to high risk of seizures
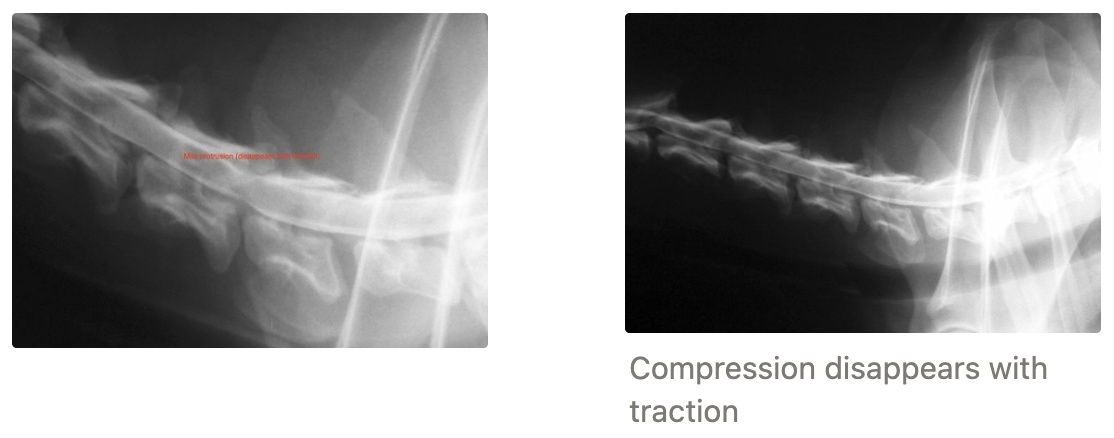
Shows ventral and/or dorsal extra-dural sign which can be dynamic
Take multiple images in dorsal extension, ventral flexion and linear traction on neck to assess for dynamic change
Treatment:
Conservative Management = Harness (no neck collars), do not exercise where they will trip easily, dietary management with OA Wobbler’s in great dane
Indication: Minor signs, stable disease without severe neck pain
Ventral Slot Decompression = Remove annulus
Indication: Severe signs, deteriorating disease or severe neck pain and STATIC lesions
Distraction Fusion ± Ventral Slot = Make disc space wider with traction on neck then fuse this position to prevent disc bulging
Indication: Severe signs, deteriorating disease or severe neck pain and DYNAMIC lesions
Prognosis: 7/10 dogs (surgery often not recommended before conservative management attempted due to high risk of no response OR making pain worse)
Post-Op Risks:
Risk of dominos = Fusion of C5/6 with surgery → Transfer load to C6/7 and Wobblers in next cervical vertebra
Risk of haemorrhage
Atlantoaxial Instability
Aetiology
Signalment
Pathology
Clinical signs
Diagnosis
2 Treatment options
Indication
Disadvantage
Methods
Prognosis with surgical treatment (+ risk)
Aetiology: Congenital or developmental → Dens of axis too small + ligaments bad + stretching with trauma (eg. hitting head against wall)
Signalment: Toy dog breeds (esp. Yorkies and Chihuahuas) → Pathology of the atlantoaxial junction
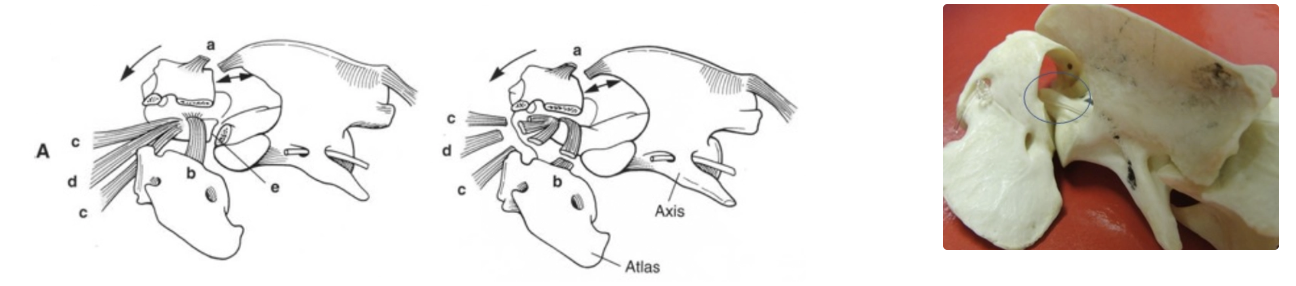
Pathogenesis:
Skull → C1 (atlas) and C1 → C2 (axis) are proper synovial joints (diarthrodial) with no discs
Hence, ligaments between C1 and C2 + dens of axis are very important and AA instability results from failure of these supporting structures → Dens compresses spinal cord esp. in ventroflexion of neck
Causes of Atlantoaxial Instability:
Fracture/absence/malformation or hypoplasia of dens → Non-functional attachment of alar, apical and transverse ligaments
Improper formation, laxity or rupture of alar, apical, transverse or dorsal atlantoaxial ligaments (required to hold dens against the floor of the spinal canal)
→ Instability, ventral subluxation and compression of cervical spinal cord (C1 - C5) by dens
Clinical Signs: Neck pain and tetraplegia with UMN forelimbs and hindlimbs
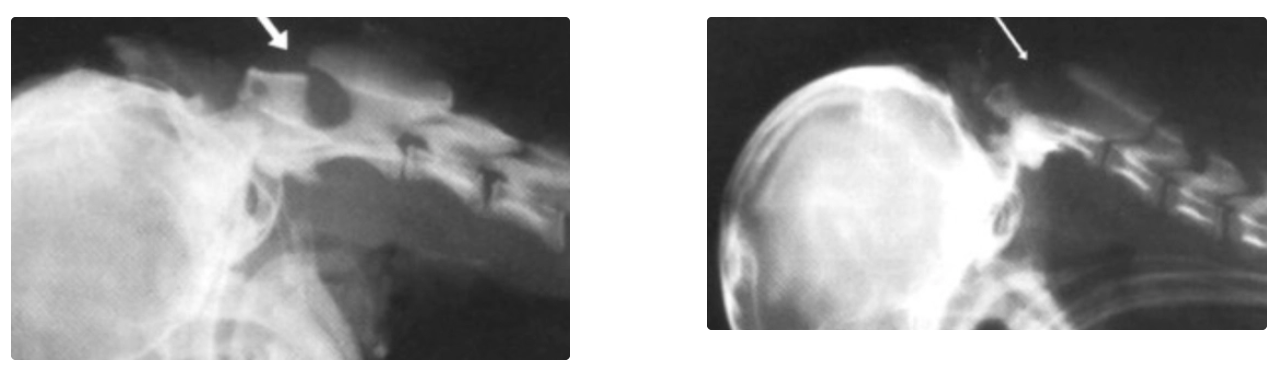
Diagnosis:
Radiographs in lateral and VD to assess for neck fractures and luxations
Normal → Progressively more flexed lateral views taken a step at a time to avoid pithing patient by dens hitting cord
As soon as you see distance between C2 and C1 changing → STOP flexing (will cause death in patient due to compression of spinal cord by dens)
Compare distance between dorsal process of C2 and lamina of C1
Arrows in image should NOT change
Treatments:
Conservative Management = Healing of minor ligamentous lesions with neck brace for few weeks to prevent neck movement
Indications:
May help some dogs improve after traumatic exacerbation of signs
Useful for stabilisation during transport
-ve: Poor tolerance and sedation in crate often required
Surgery
Indication: Unstable cases with bony abnormalities and those that recur with conservative management
Methods:
Dorsal wiring (higher risk of cord injury or vertebral artery rupture)
→ 3D print patient-specific jack for wire placement
Ventral stabilisation with cross pins or screws
Prognosis: More successful in dogs <2yr and those with clinical signs <10 months
Risk = Implant failure
Excellent results assuming no implant failure (no recurrence vs. conservative management → Common relapse)