IBD Pharmacotherapy
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
What are some common signs/symptoms of IBD?
- Fever
- Abdominal pain/tenderness
- GI bleeding
- Unexplained weight loss
- Join pain
What lab tests can be used for IBD?
- CBC
- Chemistries
- C-reactive protein
- Erythrocyte sedimentation rate
- Fecal calproectin
What imaging can be used to diagnose IBD?
- Computed tomography, magnetic resonance imaging
- Endoscopy (including capsule endoscopy)
What kinds of things are assessed to determine disease activity?
- Number of luqid/soft stools
- Abdominal pain
- General well being
- Presence of complications
- Abdominal mass presence
- Hematocrit
- Weight
What are the 5 categories of the CDAI and their interpretation?
1. Remission = <150
2. Response = >70-100
3. Mild disease = 150-220
4. Moderate disease = 220-450
5. Severe disease = >450
What 5 things does the Mayo composite index assess for UC activity?
1. Stool frequency
2. Rectal bleeding
3. Findings on flexible proctosigmoidoscopy
4. Physician's global assessment
What is calprotectin?
A neutrophil-derived protein with bacteriostatic and fungistatic properties. Easily detectable in stool.
What are the roles of fecal calprotectin in IBD?
- Distinguishing IBD from other bowel disorders
- Assessing efficacy of IBD treatments
- Predicting relapses or flares of IBD
What are the ranges of fecal calprotectin? No inflammation, mild, and active
None: <50 µg/g
Mild: 50-250 µg/g
Severe: >250 µg/g
What are the goals of therapy for IBD?
- Induce and maintain response/remission (mucosal healing, limit surgery)
- Prevent complications from disease and drugs
- Improve quality of life
Rank the IBD drug classes from most to least safe
1. Vedo, IL-23/12, IL-23, S1P
2. TNFi
3. JAKi
4. Thiopurine
5. Thiopurine/TNFi combo
6. Corticosteroids
What is a key corticosteroid used for IBD?
Budesonide - given PO in a controlled-release formulation designed to release in the terminal ileum or colon depending on product, or as a rectal foam. Undergoes extensive first-pass metabolism so systemic exposure is minimized
What is the preferred dose for prednisone/prednisolone in IBD?
20-60 mg
Does budesonide or prednisone have more side effects?
Prednisone, fewer with budesonide
Why is their a risk switching from budesonide to prednisone?
Risk of impaired adrenal function when transferring from glucocorticoid treatment with high systemic effects, taper slowly with some overlap of therapy
When are steroids used in therapy?
- For induction of remission ONLY
- NO role for maintenance therapy, "steroid-dependent" patients need other immunosuppressive therapies
Aminosalicylates are only effective in...
UC, NOT effective in CD
Describe aminosalicylates place of therapy for UC
- 1st line option
- can use topical alone (distal disease) or in combo
What are some common side effects of aminosalicylates?
- HA
- N/V
- abd. pain/cramping
- anorexia
- rash
- fever
Sulfasalazine has what unique side effects?
- decreased sperm production/function
- pancreatitis
- Sulfa allergy
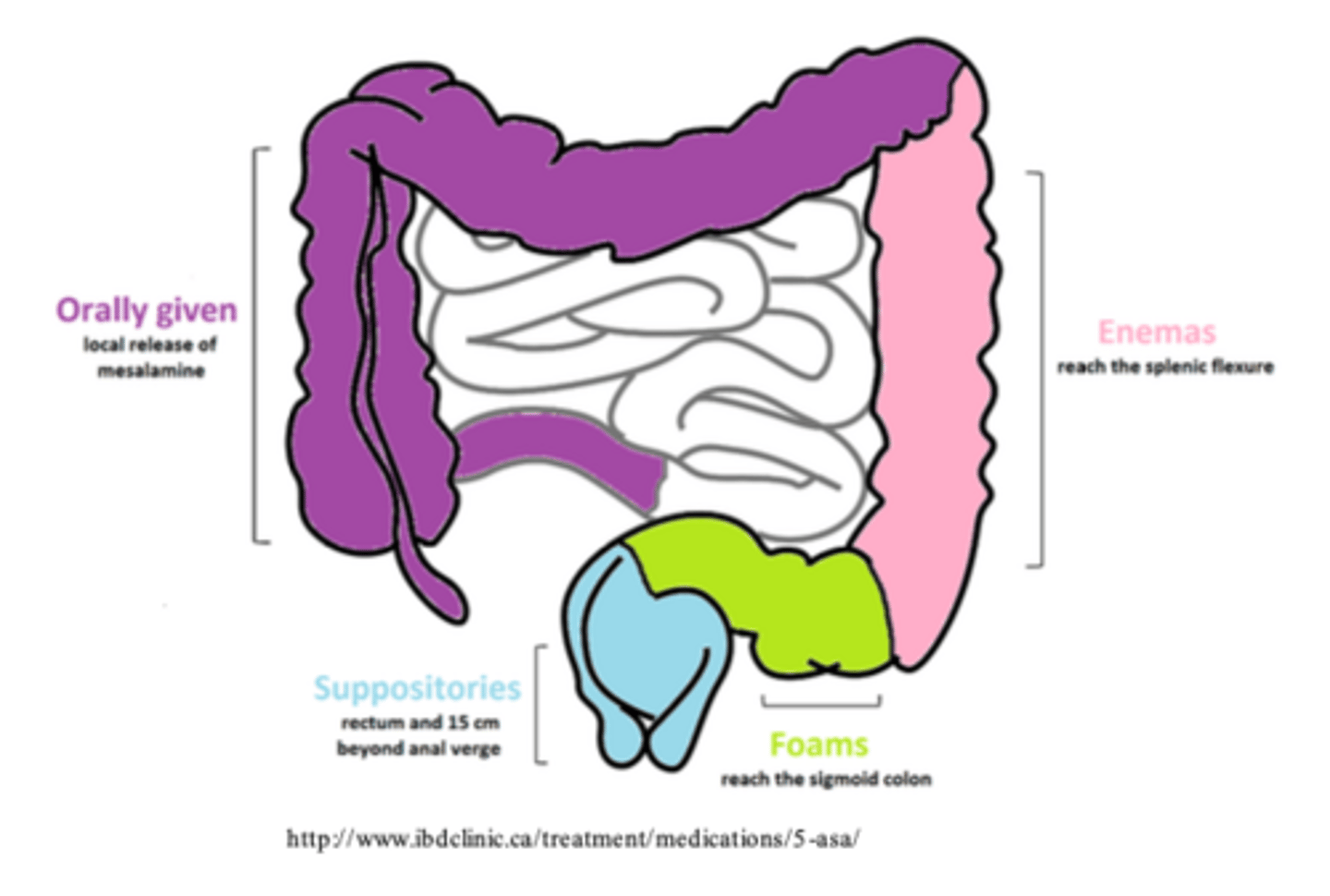
Where can different drug dosage forms reach in the GI tract?
Immunosuppressants are useful for...
steroid-sparing effects
The full therapeutic effects of Immunosuppressants are...
delayed
What are some adverse drug reactions of azathioprine/6-mercaptopurine?
- Pancreatitis
- BM suppression
- Infection
Azathioprine/6-mercaptopurine has a ____% RR of remission vs placebo
20-50%
What should be assessed before azathioprine/6-mercaptopurine initiation?
TPMT activity at baseline
When is methotrexate used?
Induction/maintenance therapy in CD
What are some ADEs for methotrexate?
- BM suppression
- pulm/hepatic fibrosis
What type of supplementation is needed for methotrexate?
folinic acid
Azathioprine dosing
1-2.5 mg/kg/d
Mercaptopurine dosing
1-1.5 mg/kg/d
Methotrexate dosing
15-25 mg IM/week
Cyclosporine dosing
2-4 mg/kg/d IV
Mycophenolate dosing
1-2 g/d PO
Tacrolimus dosing
0.1-0.2 mg/kg/d PO
What is foundational for moderate-severe disease?
"Advanced therapy"
Which biosimilars are considered to be equivalent to the originator biologic?
- infliximab
- adalimumab
- ustekinumab
How do the SC options of infliximab and vedolizumab compare to IV?
They are comparable
What does regiment is useful in severe disease?
Extended induction or dose-escalation
For moderate-severe disease, ____________ beats ____________
Top-down or early escalation beats slow step-up. Starting more aggressively up front has better chance of having future improvements
What is the favored treatment for mod/severe CD?
Early initial advanced therapy favored over step-therapy with steroids/immunomodulators
What is the favored treatment for mod/severe UC?
Early advanced therapy +/- immunomodulator rather than step-up after 5-ASA failure
What does the profile study show for patients with crohn's disease?
There were much better outcomes (steroid/surgery free remission and endoscopic remission) when "top down" therapy was used compared to step-up therapy
A combo of ________ + __________ supported in CD and UC
Anti-TNF + immunomodulator
What specific Anti-TNF + immunomodulator combo is best for CD?
infliximab + thiopurine PO works better than infliximab or thiopurine monotherapy
What specific Anti-TNF + immunomodulator combo is best for UC?
infliximab/adalimumab/golimumab with immunomodulators (thiopurine PO or methotrexate SC/IM)
What are the benefits of Anti-TNF + immunomodulator combo therapy?
- Improved efficacy outcomes (steroid free clinical remission)
- Reduced risk of immunogenicity to biologic
What are the risks of Anti-TNF + immunomodulator combo therapy?
- infections
- hepatosplenic T-cell lymphoma (rare, life-threatening event primarily in young males, associated with past/current thiopurine exposure in patients receiving anti-TNF therapy)
Order infliximab, azathioprine, or a combo in terms of steroid-free remission rates and mucosal healing from best to worse
1. Combo
2. Infliximab
3. Azathioprine
Why is a combo infliximab therapy better than monotherapy?
Over time, more patients will develop antibodies to infliximab if used as a monotherapy (loses its efficacy over time)
How do we de-escalate or come off combination therapy?
- Don't stop the anti-TNF (biologic) first
- For UC and CD, suggests against TNF antagonist withdrawal
- Withdraw the immunomodulator
What is the goal of therapeutic drug monitoring (TDM) in IBD?
Optimize biologic therapy in treat-to-target model
When is reactive TDM used?
When objective inflammation persists or loss of response on anti-TNF regimen
When is proactive TDM used?
Check levels at a set time. Insufficient/conflicting evidence to recommend over reactive TDM
Reactive TDM results are as follows: low drug and no/low antibody presence. How would you interpret this and what action should be taken?
PK underdosing, increase dose or shorten interval
Reactive TDM results are as follows: low drug and high antibody presence. How would you interpret this and what action should be taken?
Immune-mediated clearance, switch therapy +/- immunomodulator
Reactive TDM results are as follows: therapeutic/high drug and no/low antibody presence. How would you interpret this and what action should be taken?
Mechanistic failure, switch out of class
What 2 drugs are only used in CD?
1. Certolizumab
2. Methotrexate
How should 5-ASAs be managed following treatment escalation?
Stop the 5-ASA
What are preferred treatments in pregnancy?
Any biologic (anti-TNF)