EXAM 4: Lec 34. visual pathways
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
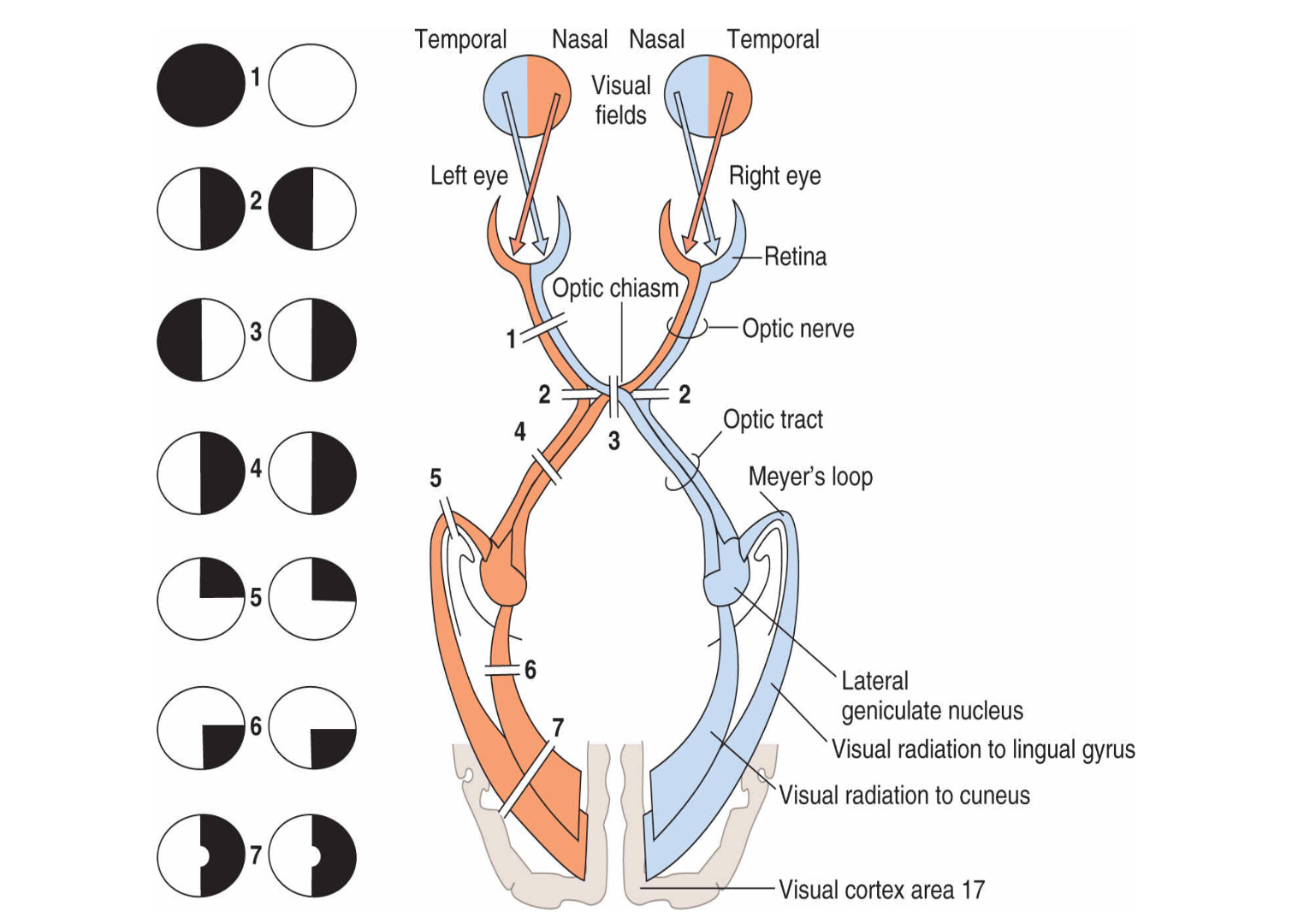
what is the primary visual pathways
*in order
1.Ganglion cell axons exit retina via optic disk
●
2.Axons bundle to form optic nerve
●
3.Optic nerve travels posterior to optic chiasm
●
4.Bilateral ganglion axons form optic tract
•Contains axons from both eyes
5.Travels to:
•Lateral geniculate nucleus (LGN) of the thalamus**
•Hypothalamus
•Superior colliculus
•Neurons in pretectum
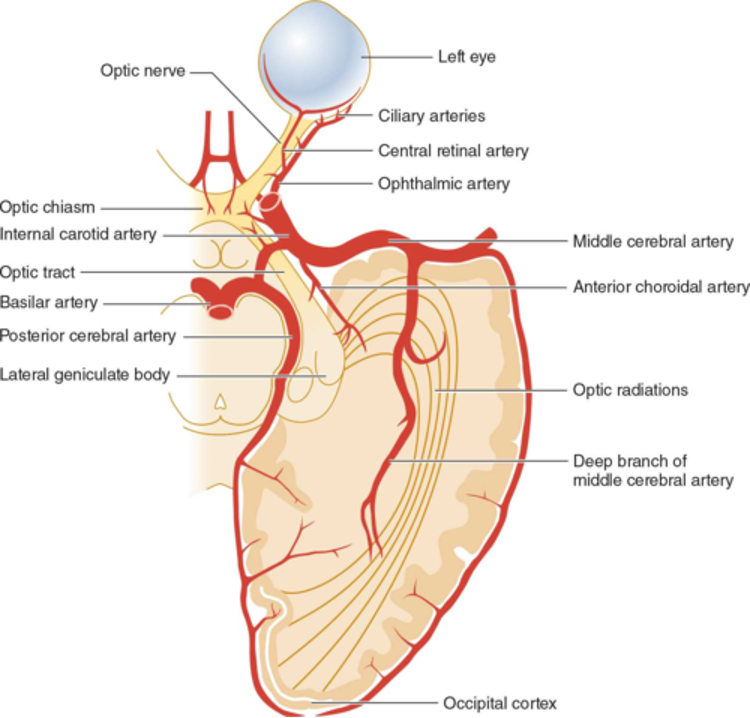
•Retinogeniculostriate pathway
•Retina —> LGN —> striate cortex
—
what pathway is this?
•Primary visual pathway
•Retino-hypothalamic
•Retina → hypothalamus
—
•does what function?
Coordinate structures controlled by ….
circadian rhythms
•Superior colliculus (Tectal system)
Retina —> superior colliculus
—
does what function?
•Coordinates head/eye movement towards visual targets
•Pre-Tectal system
•Retina → neurons in pretectum → Edinger Westphal nucleus
—
does what function?
•Coordinates pupillary light reflex, constricts pupil (para)
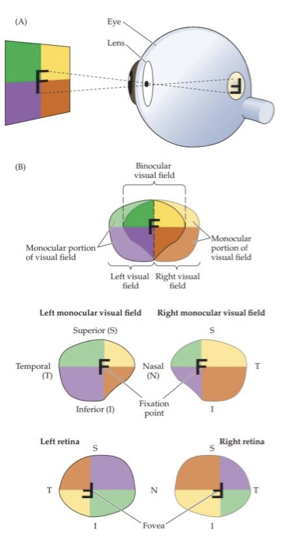
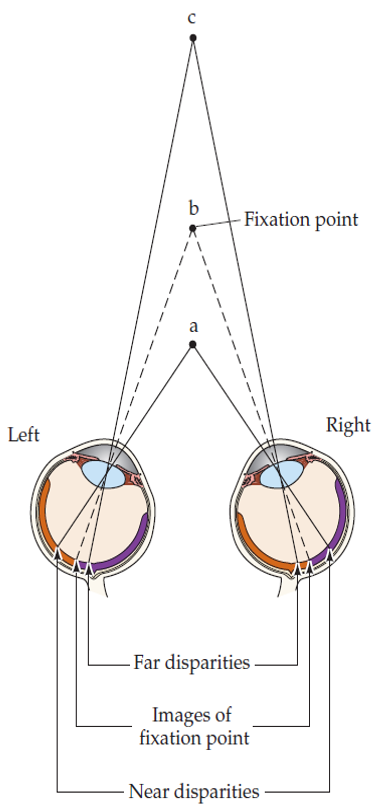
•Retinal surface subdivided into quadrants
intersect at point of fixation
Vertically –nasal vs temporal
Horizontal – superior vs inferior
•Diverging light rays from different points, cause images of objects to be inverted/reversed (top-down; left-right) onto the retinal surface
•Optic tract and beyond contains —
axons of ganglion cells originating in both eyes and represent the contralateral field of view
visual field
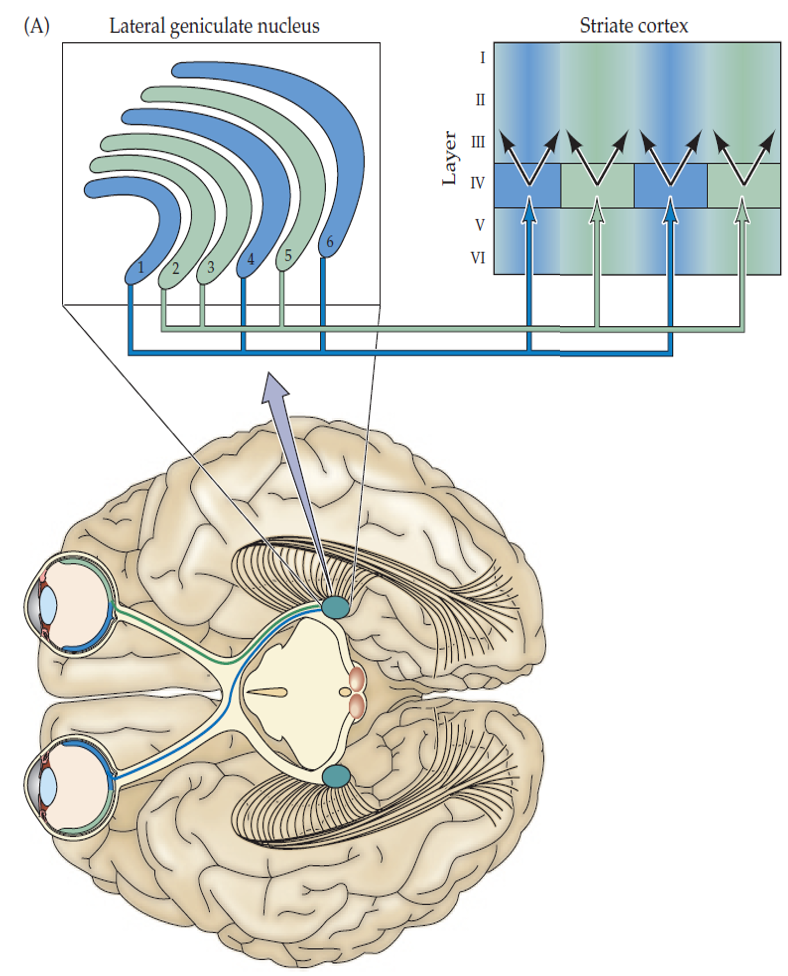
•Map is established in LGN and maintained in projections to striate cortex
“Retinotopic Organization”
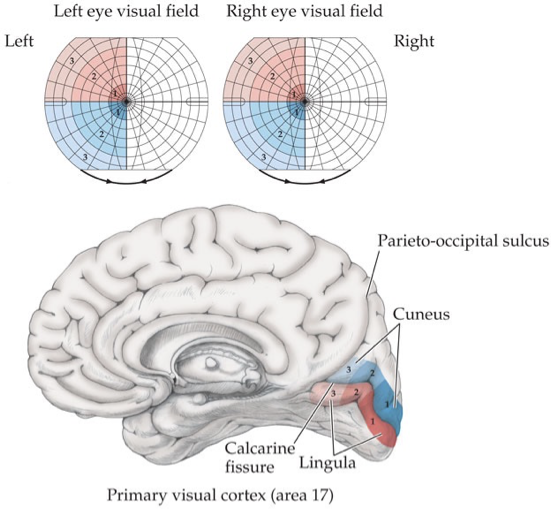
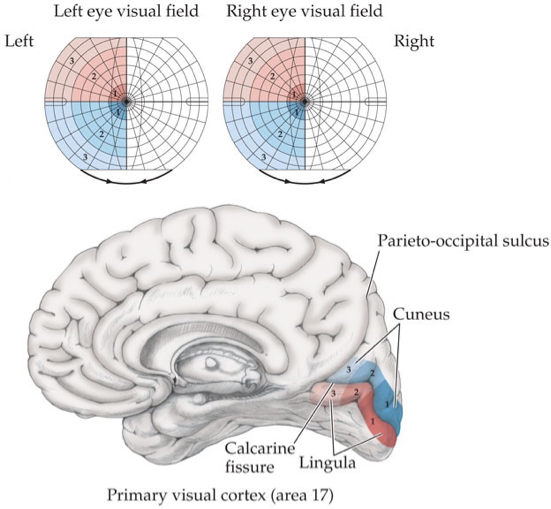
•Striate cortex organization of visual field
•Posterior – ________ regions
•Anterior – ______ regions
Posterior – foveal/macular regions
Anterior – peripheral regions
Optic radiations project to respective banks of calcarine fissure of occipital lobe (of the visual field):
-
•Upper visual field [above/below] fissure (?)
UPPER visual field is BELOW fissure
•Lower visual field above fissure
Neurons in visual processing:
•LGN are [monocular OR binocular] ??
•Striate cortex are [monocula OR binocular] ??
•LGN are monocular
•Striate cortex are binocular
In visual processing…
Ocular Dominance Columns
•Axons at LGN terminate in separate, alternating layers
-
Q. what cortical layer do we mostly get the mix of the striate cortex?
•Cortical layer 4 is primarily where we get the mix in the striate cortex
visual processing:
________ is the:
•Mixing of pathways at striate cortex
•Improves our ability to have depth perception
Stereopsis
Q. what pathway is this in visual processing?
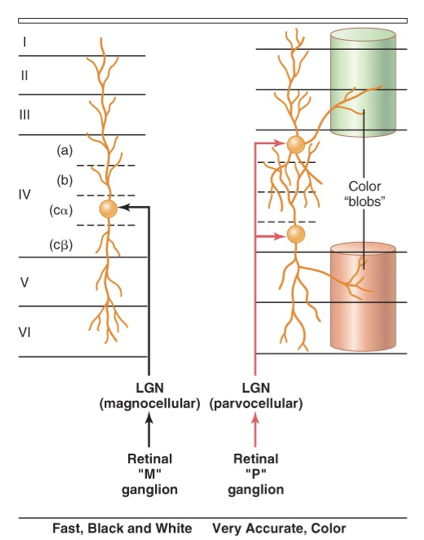
•Parallel pathways
•Convey distinct types of information to initial stages of cortical processing
Retinogeniculate pathway
what layers are being described below of the LGN?
•Large neurons
•Information from rods (i.e., peripheral retina)
•M-retinal ganglion cells terminate here
- part of visual processing
•Lesion: reduces ability to perceive rapidly changing stimuli
Ventral layers (2) = Magnocellular layer of LGN
— to remember:
(mega -maga) — big neurons, will be in the peripheral (where the rods are at)
what layers are being described below of the LGN?
•Small neurons
•Information from cones (i.e., fovea)
•P-retinal ganglion cells terminate here
- part of visual processing
•Lesion: Loss of visual acuity and color perception
Dorsal multi-layers (4) = Parvocellular layers of LGN
what affect would a lesion at the Ventral layers (2) = Magnocellular layer of LGN do?
Lesion: reduces ability to perceive rapidly changing stimuli
what affect would a lesion here - Dorsal multi-layers (4) = Parvocellular layers of LGN - do?
Lesion: Loss of visual acuity and color perception
corneal reflex
•Tactile stimulation of the cornea should result in bilateral (consensual) closing of the eyelids
•
•Reflex test typically done with cotton swab to cornea
•
•Afferent — what CN?
•Efferent — what CN?
•Afferent — Ophthalmic division of CN V to spinal trigeminal nucleus
•
•Efferent — CN VII via facial nucleus
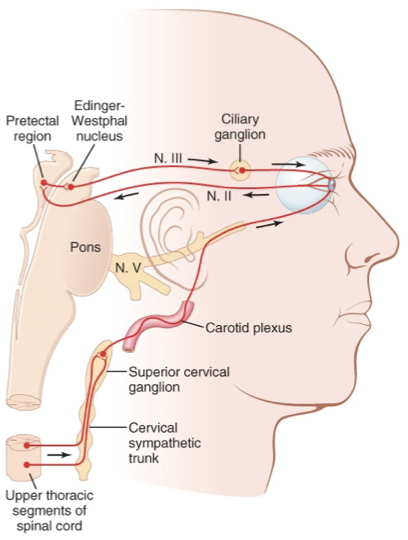
what reflex pathway is being described? & its func?
•Intermediolateral column of thoracic spinal cord (IML)
—> sympathetic trunk —> superior cervical ganglion
Fibers travel with internal carotid artery, then hop on CN V1 to enter orbit
Sympathetic Innervation
Function:
•Pupil dilation (iris radial m.)
•Eyelid elevation (superior tarsal m.)
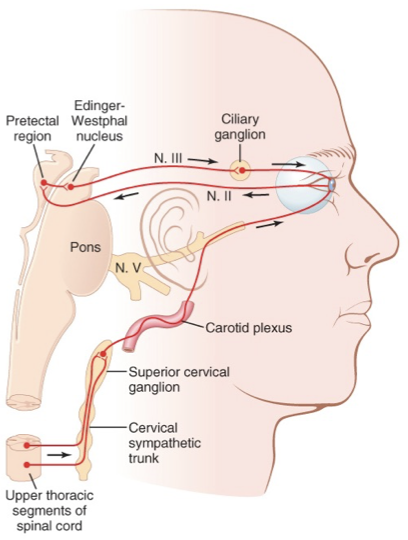
what reflex pathway is being described? & its func?
•Pretectal neurons —> Edinger-Westphal nucleus
Fibers travel to ciliary ganglion via CN III
Postganglionic fibers travel to eye via ciliary nerve
Parasympathetic innervation
Function:
•Pupil constriction
•Focus lens
what reflex?
Normal conditions:
•Stimulated eye = direct response
•Unstimulated eye = consensual response
—
•BOTH EYES RESPOND THE SAME, EVEN WITH ONLY ONE BEING STIMULATED.
Pupillary Light Reflex

how does the pupillary light reflex work in light?
& in the dark?
In Light
1.Light impinges on retina/ganglion cells
2.Impulses pass from CN 2 to pretectal nuclei
3.Secondary impulses pass to bilateral Edinger-Westphal nucleus
4.Signals pass back through CNIII parasympathetic nerves
5.Sphincter of both iris/pupil constricts
In Darkness
•Reflex becomes inhibited, permits pupil dilation
what clinical disorder is this?
Symptoms
•Pupil constriction (miosis)
•Drooping eyelid (ptosis)
•Lack of sweating (anhidrosis)
Potential lesions_________________________
•Central – between hypothalamus and sympathetic axons
•Peripheral – sympathetic trunk, superior cervical ganglion, or carotid artery
•Congenital – perinatal damage to sympathetic trunk
•Hereditary – autosomal dominant
Horner syndrome
•Small, irregular and asymmetrical pupils that fail to react to light but constrict on accommodation
•Accommodation (convergence, ciliary muscle contraction, pupil contraction) intact
•Potentially lesions to the pretectal nuclei in the midbrain
•Often seen in CNS syphilis or diabetes
Argyll-Robertson pupil
(Prostitute pupil; light-near dissociation)
•Degeneration of ciliary ganglia and postganglionic parasympathetic
•Sluggish, segmental pupillary responses to light but constrict on accommodation
•Typically, unilateral and common in females
•Accommodation (convergence, ciliary muscle contraction, pupil contraction) intact
Adie-Tonic Pupil
•Also called Holmes-Adie Syndrome