Patient centered care
Distribution of Fluid in body
females 55%, males 60% of body weight
2/3 intracellular fluid
1/3 extracellular fluid
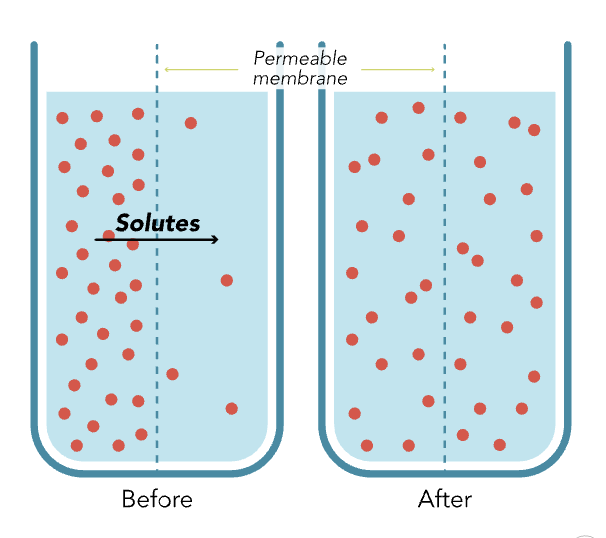
Diffusion
Movement of solutes from an area of greater concentration to an area of lesser concentration.
Osmosis
Movement of water from a dilute solution (low concentration of solute) to a more concentrated solution (high concentration of solute)
Water moves
Hydrostatic Pressure (Filtration)
The pressure that a liquid puts on something when the liquid is at rest.
Osmotic Pressure
The pressure needed to stop a liquid from moving through a semi-permeable membrane from one side to the other.
Fluid Volume Deficit
Negative fluid balance, dehydration, volume depletion.
Risk Factors:
Vomiting, bleeding, diarrhea
Diabetes insipidus
Burns
Excessive sweating
Third-spacing
Diabetic ketoacidosis
Diuretics
Altered intake
Older age
Signs of Fluid Volume Deficit
Hypotension, tachycardia
Confusion
Increased respiratory rate
Oliguria (dark urine)
Dry mucous membranes, poor skin turgor
Increase BUN, serum osmolality, urine osmolality
Hgb & Hct elevated if due to water loss
Hgb & Hct low if due to blood loss
Impact on Health: Fluid Volume Deficit
organ and tissue damage
cerebral hypoperfusion
safety
morbidity (very young or >65)
Fluid Volume Excess
Heart failure, liver cirrhosis, kidney disease/injury, IV therapy.
Risk Factors:
Cardiac, liver, renal, and endocrine disorders
Pregnancy
Excessive IV fluid Admin
Older than 65 with cardiac or renal disorders
Signs of Fluid Volume Excess
Hypertension, bounding pulses, jugular vein distention
Sodium dilution, decreased LOC, convulsion
Lung crackles, pulmonary congestion, dyspnea, hypoxia
Polyuria
Pitting edema, ascites
Decreased urine specific gravity, BUN, and Hgb & Hct
Nursing care for Fluid Imbalance
Employ fall preventions
Client education
Daily weights
Increase fluid and sodium intake (DEFICIT)
Place in trendelenburg postion (DEFICIT)
Restrict fluid and sodium (EXCESS)
Place in semi or high-fowler’s positions (EXCESS)
Fluid Imbalance: Evaluate Outcomes
Deficit:
urine output
labs
hypovolemic shock
Excess:
respiratory status
edema
cardiac status
BNP
pulmonary edema
Hyponatremia
Sodium less than 130 mEq/L.
Labs:
blood sodium and osmolarity decreased
urine sodium and urine specific gravity decreased
Risks factors:
excessive sweating
diuretics
wound drainage
NG tube suction
decreased secretion of aldosterone
hyperlipidemia
kidney disease
low-sodium diet
cerebral salt wasting syndrome
hypotonic fluid excess
fresh water submersion accident
kidney or heart failure
SIADH
anticonvulsant meds, SSRIs, and desmopressin
older adults
Hyponatremia Expected Findings
Low sodium.
hypervolemic with low sodium = bounding pulse, higher BP
hypovolemia: hypothermia, tachycardia, rapid thready pulse, hypotension, orthostatic hypotension, diminished peripheral pulses
headache, confusion, lethargy, muscle weakness, fatigue, decreased DTRs, seizures, lightheadedness, dizziness
increased GI motility, hyperactive bowels, abdominal cramping, nausea
Hyponatremia Nursing Care
If CKD, no salt substitutes
encourage sodium containing foods and hypertonic fluids
administer IV fluids
Restrict water intake if fluid overload
monitor I&Os and weight
monitor VS and LOC
Implement seizures precautions
Maintain an open airway
What is sodium’s main function?
Help maintain electrical membrane excitability.
Hypernatremia
Sodium excess.
Risk Factors:
Kidney failure
Cushing’s syndrome
Aldosteronism
Medications
Excessive intake of oral sodium
Water deprivation (NPO)
Hypertonic enteral feedings without adequate water supplement
Diabetes insipidus
Heatstroke
Hyperventilation
Watery stools
Burns
Excessive sweating
Hypernatremia Expected Findings
Thirst
Hyperthermia, tachycardia, orthostatic hypotension
Restlessness, irritability, muscle twitching, respiratory compromise, decreased/absent DRTs, seizures, coma
Dry mucous membranes, nausea, vomiting, anorexia, occasional diarrhea
Hypernatremia Nursing Care
Monitor LOC and safety
Vital signs and heart rhythm
Auscultate lung sounds
oral hygiene and other comfort measures to decrease thirst
monitor I&Os, alert physician if inadequate urinary output
monitor potassium level if diuretics are administers
encourage water intake
discourage sodium intake
Administer loop diuretics for patients with poor kidney excretion
Hypokalemia
Low potassium.
Risk Factors:
overuse of diuretics, digitalis, corticosteroids
Increased secretion of aldosterone
Cushing’s syndrome
Loss via GI tract
NPO status
Kidney disease, impairs reabsorption of potassium
Alkalosis
Hyperinsulinism
Total parental nutrition
Water intoxication
older adults
Hypokalemia Expected Findings
Decreased BP, thready weak pulse, orthostatic hypotension
Altered mental status, anxiety, lethargy, acute confusion, coma
ECG: flattened T wave, prominent U waves, ST depression, prolonged PR interval
Hypoactive bowel sounds, nausea, vomiting, constipation, abdominal distention, paralytic ileus can develop
muscular weakness, DRTs reduced
shallow breathing
Hypokalemia Nursing Care
Administer potassium replacement
Observe for shallow ineffective respirations and diminished breath sounds
Monitor cardiac rhythm
Monitor clients receiving digoxin
Monitor LOC
Monitor bowel sounds and abdominal distention
Oxygen sat level
assess DRTs
Implement fall precautions for muscle weakness
Encourage foods high in potassium
IV potassium supplementation (slow drip)
NEVER IV PUSH POTASSIUM (cardiac arrest)
Hyperkalemia
High level of Potassium
Risk factors:
Overconsumption of high potassium foods or salt substitutes
excessive or rapid potassium replacement
RBC transfusion
Adrenal insufficiency
ACE inhibitors or potassium sparing diueretics
Kidney failure
Extracellular shift from decreased insulin production
Acidosis (DKA)
tissue damage
Hyperuricemia
Hyperkalemia Expected Findings
Slow irregular pulse, hypotension
Restlessness, irritability, weakness, paresthesia
ECG: premature ventricular contractions, ventricular fibrillation, peaked T waves, widened QRS
Increased GI motility, diarrhea, hyperactive bowel sounds
Oliguria
Hyperkalemia Nursing Care
Monitor EKGs
Assess for muscle weakness
Avoid salt substitutes
Treatments to decrease potassium
Administer IV fluids with dextrose and regular insulin
Sodium polystyrene sulfonate (Kayexalate) to excrete K+ through feces
Loop diuretics to deplete K+ through renal system
Albuterol to shift K+ into intracellular space
Hypocalcemia
Low Calcium
Risk Factors:
renal failure
decreased parathyroid hormone
Inadequate intake of calcium or vitamin D
Sepsis
diarrhea, steatorhea
end-stage kidney failure
wound drainage
Hypocalcemia Expected Findings
Tetany
Paresthesia of the fingers and lips
Muscle twitches
Seizure due to irritability of CNS
Charley horses
Hyperactive DTRs
Positive chvostek’s sign
Positive trousseau’s sign
Prolonged QT interval
Hyperactive bowel sounds, diarrhea, abdominal cramps
Hypocalcemia Nursing Care
Administer oral or IV calcium supplements. Vitamin D supplements enhance absorption of calcium
Implement seizure and fall precautions
Avoid overstimulation
Have emergency equipment on standby
Encourage foods high in calcium
Treatment with calcium gluconate or calcium chloride if life-threatening.