Derm Exam 2: Yamaki RA
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
36 Terms
Epidemiology of RA
Onset is 3rd to 4th decades of life, and prevalence increases with advancing age (Usually manifests ~______).
50 years
Etiology of RA
Immune cells, pro-inflammatory cytokines, and signaling pathway:
______ (______ mediated)
______ (______ mediated)
______, ______, and ______
______
T cells, cell, B cells, humoral, TNF, IL-1, IL-6, JAK
Rheumatoid Arthritis (RA)
Inflammatory polyarthritis, especially the ______ of the hands and feet.
Untreated chronic inflammation → joint erosions and joint destruction.
Need to treat to ______
RA is characterized by:
autoantibody production [______, ______]; highly specific for RA
synovial ______ and hyperplasia (pannus);
cartilage and ______ (deformity); and
extra-articular involvement: CV, pulmonary, skeletal, ocular, and skin involvement
Inflamed and pain in joint, bone deformity, etc.
smaller joints, prevent progression of destruction, RF, ACPA, inflammation, bone destruction
Clinical S/Sxs
Slow but progressive
Stiffness is ______
Can decrease stiffness in the AM ______
worst in the morning, with activity
Common Joints of Involvement
Most common joint involvement: ______ joints affected, no ______
______ (90%)
______ joint (PIP)
______ joint (MCP)
______ (90%)
metatarsophalengeal joint (MTP)
1st or 2nd, distal, hands, proximal interphalangeal, metacarpophalangeal, toes and feet
Signs and Symptoms
Untreated RA can go beyond joints and ultimately ______
affect organs
Diagnosis of RA
Score of ______ indicates RA
High Specificity for RA diagnosis
______
______ (highly specific for RA)
6 or higher, RF, ACPA
General Principles in the Treatment of RA
______ treatment for ______ diagnosed with RA. (More aggressive than previous approaches decades ago)
Baseline testing before starting DMARDs:
______ with differentials (cell counts)
______
______ (renal function)
Selection of ______ based on:
severity of RA & stage of RA (DMARDs naïve or experienced)
patient’s preference
insurance coverage
presence of adverse prognostic findings (______, other factors)
DMARD, all pts, CBC, LFTs, BUN/SCr, DMARDs, comorbid conditions
General Principles in the Treatment of RA
Anti-inflammatory (______) or ______ therapy for ______ therapy ONLY
______: Achieve and maintain tight control of disease activity, defined as ______ or a state of ______
Treatment failure defined as ______ / ______, following ______ of DMARDs at optimal dosing
NSAIDs, glucocorticoid, bridging, treat to target, remission, low disease activity, lack of remission, low disease activity, 3-6 months
Functional Status Instrument Tools
______ is worse
higher number
Non-Pharm Therapy
Relate to Help Inflammation
______
______
______ (______ = pro-inflammatory)
______ reduction
______
Counseling
Physical Therapy
Surgery (last resort) - aims to relieve pain, correct deformities, improve joint function → enhancing the quality of life
Exercise, massage, smoking cessation, smoking, stress, diet
DMARD naïve - Low vs High RA Activity
Level of RA activity will guide how to start treatment for patients ______ to patient specific factors
In addition
DMARDs
Non-Biologics
______ (______)
HCQ (Plaquienil)
Sulfasalazine (Azufidine)
Leflunomide (Arava)
______ combine with each other, ______ (non-b + non-b and non-b + biologic)
Biologics
-mab and -cept
Tofacitinib & Baricitinib (JAK/STAT kinase inhibitors) → technically not a biologic
______ combine biologic DMARDS with each other
Methotrexate, Trexal, okay to, up to triple therapy, Do not
Methotrexate (MTX)
Anti-inflammatory and immunosuppressive action (1st line DOC for moderate/high)
Given ______ PO or SQ, start with PO
Titrate to >15mg per week within 4-6 weeks (2.5 mg per week), 30mg weekly upper max limit
SEs
______ (monitor for liver dysfunction)
______ (monitor CBC)
______ (take supplemental folic acid 1mg PO daily)
Leucovorin (folinic acid) can be used if folic acid does not help
Potential to ______ with ______ (avoid ______ administration ______)
weekly, LFTs increase, Suppression of blood counts, decreases folic acid, decrease MTX efficacy, Leucovorin, same day, PO/IV
Methotrexate (MTX)
Contraindicated
Liver disease (severe)
______
Precautions
______ (AKI or CKD)
______
Pregnancy (X), renal elimination, liver dysfunction
Hydroxychloroquine (HCQ)
Moderately effective ______
______
SEs (well tolerated in general)
Rare (but serious): ______ (______) with long-term use with doses greater than 5 mg/kg
Patients should have a complete ______ done at ______ and every 5 years thereafter
alone for mild RA, Safe in pregnancy, retinal toxicity, retinopathy, eye exam, baseline
Sulfasalazine (SSZ)
Onset (______)
______
SEs
GI upset (nausea and vomiting) may limit use, rash development
Serious:
Hepatitis- monitor ______
Leukopenia- monitor ______
______
Takes a long time, safe in pregnancy, LFTs, CBC, Agranulocytosis
Leflunomide (LEF)
SEs
Diarrhea is most commonly the limiting effect in treatment
______
______
Rash
Reversible alopecia
Rare but serious - interstitial ______ disease and ______
C/I
______ and carcinogenic in animal studies (______)
Liver toxicity, myelosuppression, lung, peripheral neuropathy, Teratogenic, do not use in pregnancy
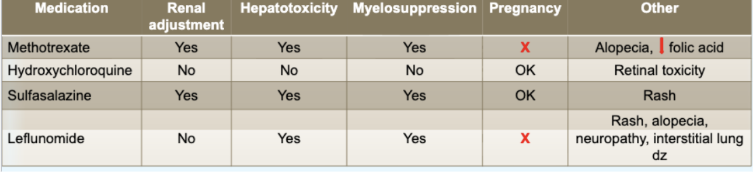
KNOW IMAGE
Biologic DMARDs
______
Adalimumab
Etanercept
Infliximab
Certolizumab
Golimumab
______
______ (IL-1 inhibitor)
______ (IL-6 inhibitor)
______ (B cell inhibitor)
______ (co-stimultation inhibitor)
______ & ______ (JAK/STAT kinase inhibitors) (technically not a biologic)
______ combine biologic DMARDS with each other
Anti-TNF Biologics, Non-TNF Targeting Biologics, Anakinra, Tocilizumab, Rituximab, Abatacept, Tofactinib, Baricitinib, do not
TNF Inhibitors → Anti-TNF Biologics
TNF inhibitors: ______, ______, ______, ______, ______
Common SEs (boxed warning):
______: URTI, pneumonia, UTI, skin and soft tissue infection
______: ______ (reactivation of latent disease), invasive fungal infections, reactivation of hepatitis B. ______
______: lymphoma, nonmelanoma skin cancer
Warnings, precautions:
Not recommended in patients with ______, ______, and ______ dyscrasias
Adalimumab, Certolizumab, Etanercept, Golimumab, Infliximab, Infection, Opportunistic Infection, TB, must treat TB completely before starting, Cancer, CHF, transient neutropenia, blood
T-Cell Co-Stimulatory Blockade
Abatacept Adverse Effects
______ (mild to severe)
Pneumonia (esp. in patients with ______), opportunistic infections (less risk than TNFi’s)
TB cases have been ______, but screening is still recommended. (Can start if being treated currently for ______, preferred over ______)
Increased risk of infections, COPD, few, TB, TNFi
______
Tocilizumab (Actemra®) SEs
Increase risk of infection and serious infection. (Can start if being treated currently for TB)
Increased risk of GI perforation
IL-6 Inhibitor
Interleukin-6 Inhibition
______ (______®) SEs
Increase risk of ______ and serious ______. (Can start if being treated currently for ______)
Increased risk of ______
Tocilizumab, Actemra, infection, infection, TB, GI perforation
______
Rituximab Adverse Effects
Infections: reactivation of viral infections (hepatitis B)
B-Cell Depletion
B-Cell Depletion
______ Adverse Effects
Infections: ______ (______)
Rituximab, reactivation of viral infections, HepB
______
Modest increase in risk of infection
IL-1 Antagonists
______
Precautions: Infections
Warnings
Thrombosis, serious infections (TB, bacteria, invasive fungal, viral and opportunistic infections), lymphoma, malignancies, viral reactivation EBV & HSV.
No in pregnancy
JAK Inhibitors
JAK Inhibitors
Precautions: ______
Warnings
______, serious infections (______, bacteria, invasive fungal, viral and opportunistic infections), lymphoma, ______, viral reactivation EBV & HSV.
______
Infections, thrombosis, TB, malignancies, do not use in pregnancy
Comparison of Biologics (and JAK/STATi) + ADRs
Infliximab, adalimumab, etanercept, etc. (TNF Inhibitors) → ______, ______
Tocilizumab (IL-6 inhibitor) → ______
Tofacitinib / Baricitinib (JAK inhibitors) → ______
cancer, HF exacerbation, GI perforation, Boxed Warning for VTE/PE
Treatment Goals
Treat to ______
Evaluate ______ for treatment success
target approach, every 3 months
Treatment Approach
Combo Traditional DMARDs → DMARD non-biologic
______
TNF Inhibitors (Anti-TNF) +/- MTX
Non-TNF Biologic +/- MTX
At this point >6 months
Preferred now over combo traditional DMARDs
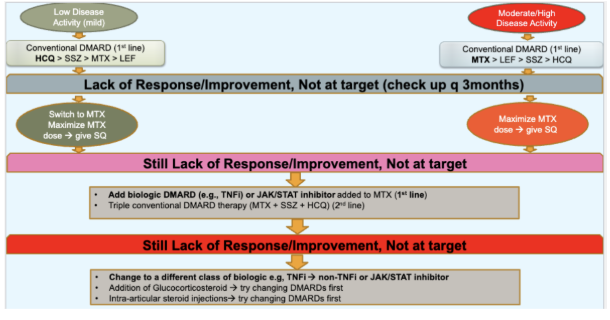
KNOW IMAGE
Treatment Approach IMAGE (ENTER AFTER EACH FILLED BULLET POINT)
Low → ______ > SSZ > MTX > LEF
Lack of Response/Improvement, Not at target (check up q3months) → Switch to ______ + ______ → give ______
Moderate/High → ______ > LEF > SSZ > HCQ
Lack of Response/Improvement, Not at target (check up ______) → ______ → give ______
Still Lack of Response/Improvement, Not at Target
______ (e.g., ______) or ______ added to ______ (1st line)
Still Lack of Response/Improvement, Not at target
Change to a different ______ e.g, ______ → ______ or ______
HCQ, MTX, maximize MTX dose, SQ
MTX, every 3 months, maximize MTX dose, SQ
add biologic DMARD, TNFi, JAK/STAT inhibitor, MTX
class of biologic, TNFi, non-TNFi, JAK/STAT inhibitor
Bridge Therapy
Wait for DMARD to start → ______
3 months
RA Remission/Low Activity
Approach if only on MTX → ______, ______
If on MTX + biologic or JAKi, can start to ______ (not the ______)
decrease dose (taper), do not just stop, gradually discontinue MTX, biologic or JAKi