Renal physiology I - Glomerular filtration
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
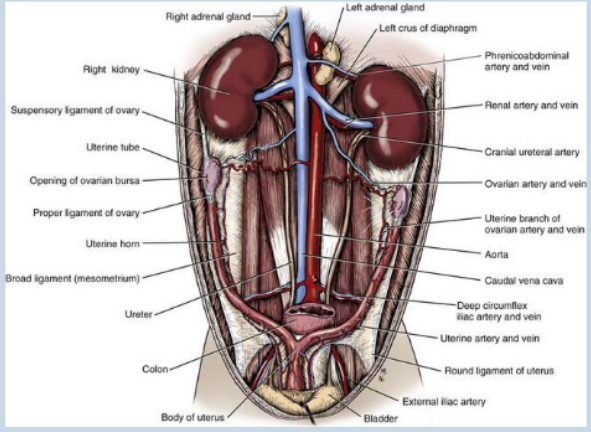
kidney
• Organs (x two) found in cranio-dorsal abdomen.
• Right typically more cranial than left, but left is more mobile.
• Retroperitoneal (meaning sitting behind the peritoneum – or dorsal in domestic animals).
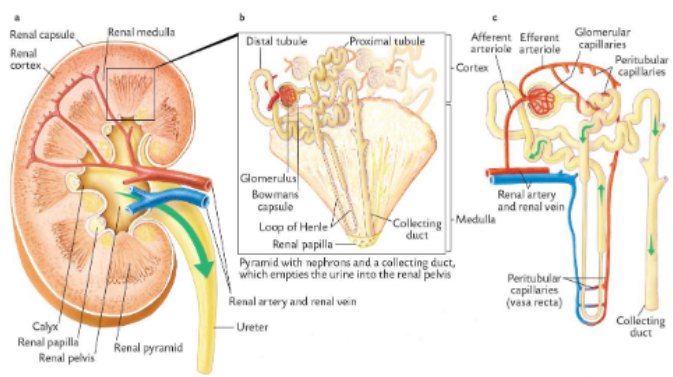
structure of the kidney
Composed of three areas:
• Cortex.
• Medulla.
• Pelvis.
Cortex contains:
• Glomerulus (glomeruli).
• Proximal Convoluted Tubule.
• Distal Convoluted Tubule.
Medulla contains:
• Loop of Henle.
• Collecting Duct.
Pelvis – feeds into ureter
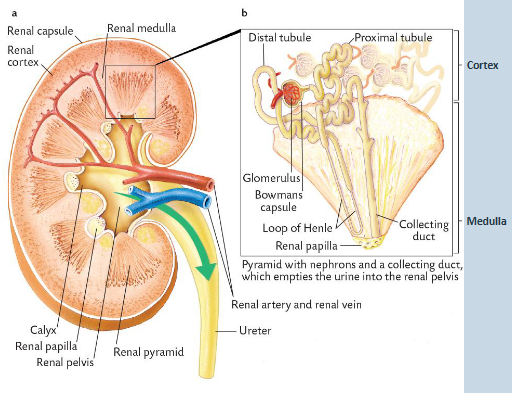
structure of the kidney cont
• Medulla formed of pyramid shaped areas
– called renal pyramids.
• Functional unit of a kidney is the nephron.
• Each pyramid contains approximately 100,000 nephrons.
A nephron can be divided into:
The renal corpuscle.
• Glomerulus and Bowman’s capsule.
The tubular system.
• Fluid-filled tubes made from a single epithelial layer and associated vascular supply
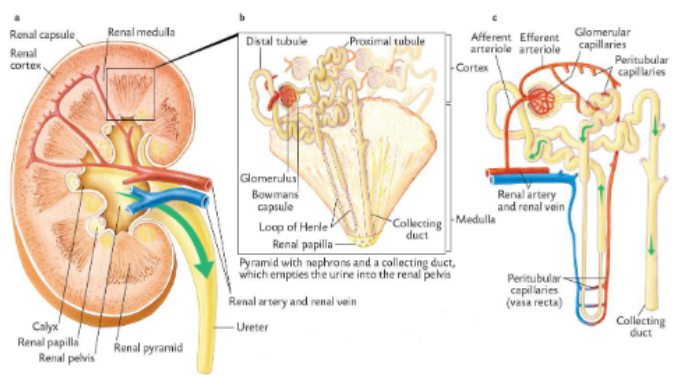
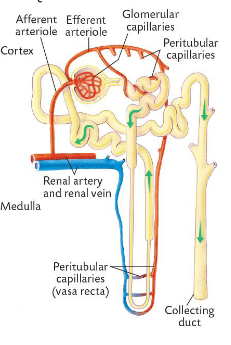
vascular and tubular component
Each nephron has a vascular component:
• (Renal artery).
• Afferent arteriole.
• Glomerular Capillaries.
• Efferent arteriole.
• Peritubular capillaries (Vasa Recta).
• (Renal vein).
Each nephron has a tubular component:
• Bowman’s Capsule.
• Proximal Convoluted Tubule.
• Distal Convoluted Tubule.
• Collecting Duct.
functions of the kidney
essentially a wet bed
• Acid-base balance.
• Water balance.
• Electrolyte balance.
• Toxin removal.
• Blood pressure control.
• Erythropoietin synthesis.
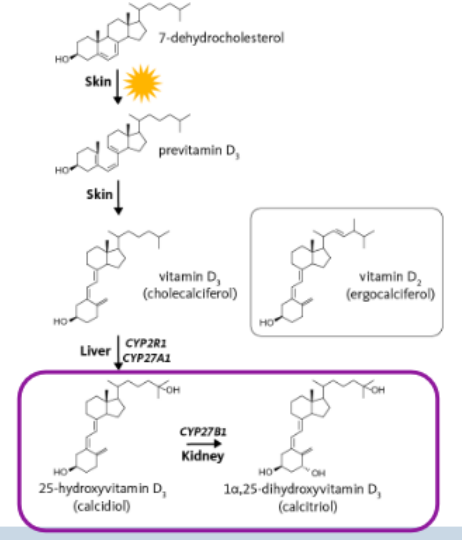
• D Vitamin D3 conversion from calcidiol to calcitriol
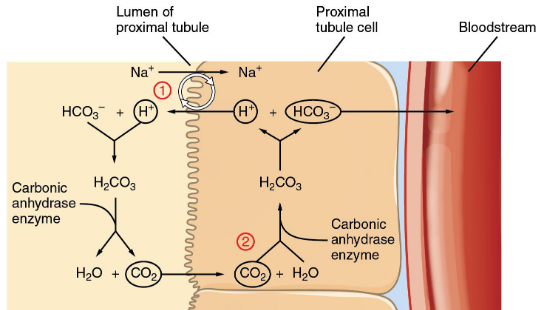
acid-base balance in the kidney
Contributing to the acid-base balance by varying urinary excretion of H+ and bicarbonates (HCO3-)
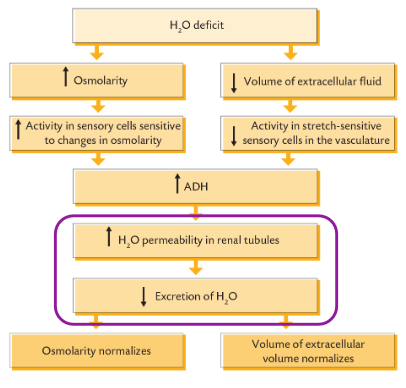
water balance in the kidney
Stabilising the volume of the extracellular fluid.
• Either through direct reabsorption in the permeable regions of the tubule or via the insertion of aquaporin channel.
• Counter-current mechanisms in nephron helps preservation of water and the formation of concentrated urine
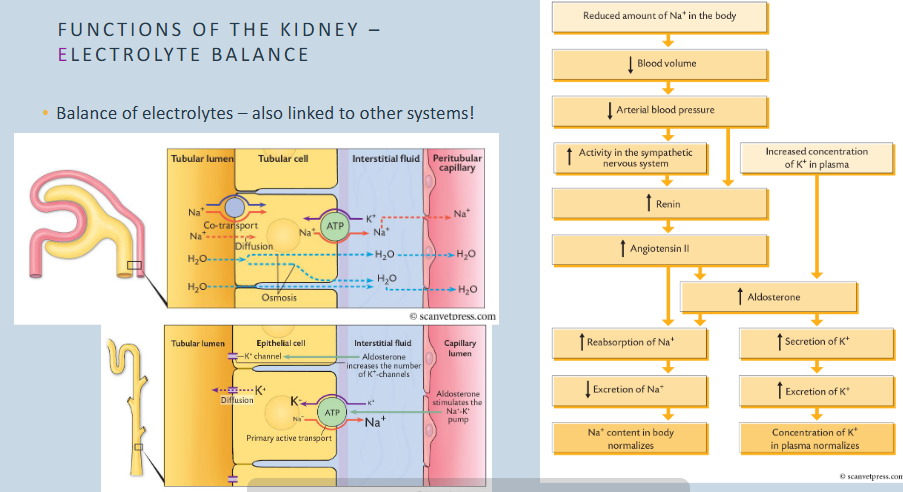
electrolyte balance in the kidney
toxin removal in kidney
Removing metabolic waste from the blood such as urea.
Removing foreign substances from the blood.
• Antibiotics.
• Beta blockers.
• Diuretics.
• Histamine (H2) blockers (e.g. ranitidine, cimetidine).
• Toxins.
• Food additives
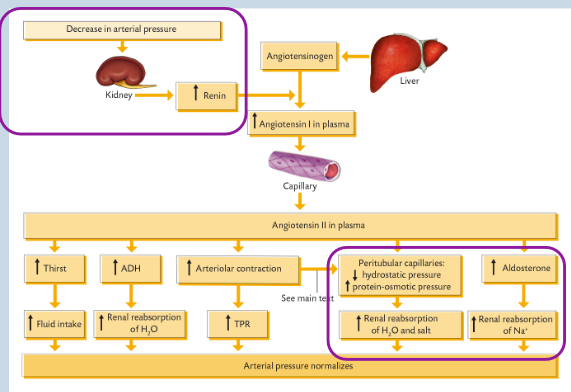
blood pressure control
• Production of Renin as part of renin-angiotensin-aldosterone- system (RAAS) to maintain blood pressure
renin is the enzyme, released by kidneys that converts angioteninsogen (cleavage) to angiotensin I in the liver.
ACE cleaves angiotensin I to angiotensin II in capillaries of lungs
angiotensin II is a vasoconstrictor that raises blood pressure
blood pressure control in kidney
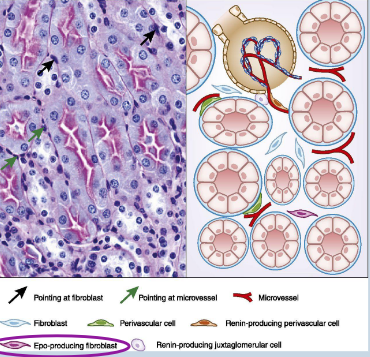
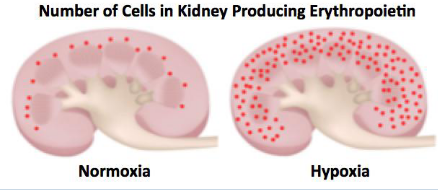
• Produce erythropoietin (hormone regulating RBC production in bone marrow esssential for O2 transport) in response to hypoxia (low oxygen)→ erythrocytes.
• Produced by cells within interstitium of cortex
vitamin D metabolism in kidney
• Produces calcitriol - active form of vitamin D.
• Performed by cells located in the proximal tubules of the nephron.
calcitriol regulates calcium and phosphorus levels in the body by promoting their absorption from instestines
also stimulates bone mineralization and inhibits secretion of PTH (cos parathyroid hormone increasing calcium levels by releasing them from bones)
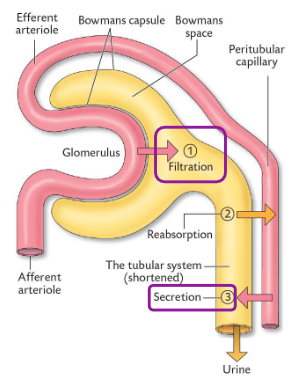
Most renal functions are achieved through three processes
1. Filtration of plasma – achieved by the renal corpuscle (composed of glomerulus and Bowman’s capsule).
2. Reabsorption of solutes and water – achieved by the proximal and distal tubules and the collecting duct.
3. Secretion of substances – achieved by tubular cells
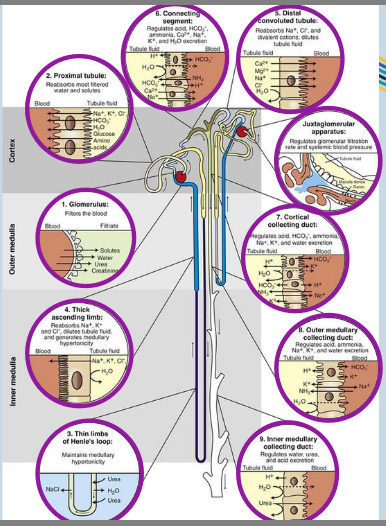
the nephron
1. Glomerulus – Filters the blood.
2. Proximal tubule – Reabsorbs most filtered water and solutes.
3. Thin limbs of Henle’s loop – Maintains medullary hypertonicity (high osmotic concentration mainly salt and urea for water reabsorption and urine conc).
4. Thick ascending limb – Reabsorbs Na+, K+ and Cl-, dilutes tubule fluid and generates medullary hypertonicity.
5. Distal convoluted tubule – Reabsorbs Na+, Cl- and divalent cations, dilutes tubule fluid.
6. Connecting segment – Regulates acid, HCO3-, ammonia, Ca2+, Na+, K+ and H2O excretion.
7. Cortical collecting duct – Regulates acid, HCO3-, ammonia, Ca2+, Na+, K+ and H2O excretion.
8. Outer medullary collecting duct – Regulates acid, ammonia, Na+, K+ and water excretion.
9. Inner medullary collecting duct – Regulates water, urea and acid excretion.
• Juxtaglomerular apparatus – regulates glomerular filtration rate and systemic blood pressure
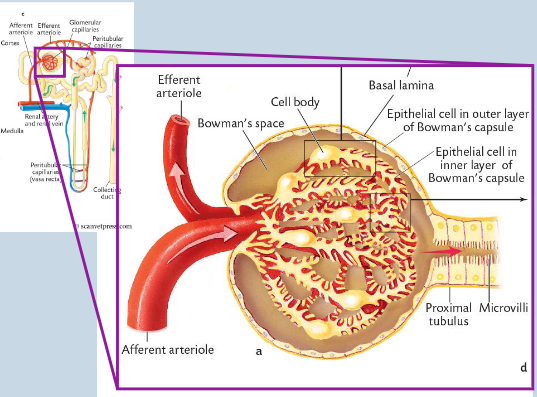
filtration - the glomerulus
is composed of three layers:
1. Endothelium of glomerular capillaries - Endothelium - Pores/fenestrae (70-100 nm) - Solutes, plasma proteins and fluid can pass through, but not blood cells.
2. Basement membrane/basal lamina - gelatinous matrix of glycoproteins and collagen that restrict plasma proteins from flowing out.
3. Epithelial cells of Bowman’s Capsule (podocytes).
Wrapped around capillaries.
Gaps between “feet” or slit pores serve as further barrier to proteins (40 nm).
Movement of protein also prevented by charge – plasma proteins are negative as is filter.
Therefore – protein in urine is always pathological
These three layers serve as a sieve/filtration barrier that has selective permeability
case 1
Betty, a 10 year-old FN Beagle presents with frothy urine and ascites
What is ascites - abnormal buildup of excess fluid in peritoneal cavity between lining of abdomen and organs
• Why is there ascites? Kidney disease damages the filtration barriers, causing severe protein loss that drops blood pressure and lets fluid leak into the abdomen.
• Where can protein be lost from?Protein is primarily lost from the glomeruli of the kidneys into the urine, though it can also be lost through the gastrointestinal tract.
• What is your plan?The plan is to run a urinalysis, UPC ratio, and blood profile, then start a low-protein diet, ACE inhibitors, and clot prevention.

glomerular filtration rate - GFR
Defined as:
Quantity of plasma (mL) filtered per min per kg of body weight through all glomeruli (mL/min/kg).
GFR normally constant throughout life but decreases in renal disease.
• Kidney will secrete renin to contribute to RAAS and keep systemic BP relatively constant.
GFR varies depending on mass (more in a smaller animals).
• Cat (example 3.64 ± 0.13 mL/min/kg).
• Dog (example 2.9 ± 0.3 mL/min/kg).
• Horse (example 1.55 ± 0.42 mL/min/kg)
H O W M U C H B L O O D I S T H AT ?
• Stan, a 20kg MN Border Collie.
• Cardiac output approx. 10% BW = 2 L/min.
• Kidneys receive 20% of the cardiac output (despite only being 0.5% of an animal’s BW!) = 400 mL/min.
• Taking haematocrit (cell volume in blood) to be approx. 45%.
400 mL blood = 220 mL plasma.
• Approx. 25% of that plasma is filtered = 55 mL/min.
Which would give a GFR of 2.75 mL/min/k

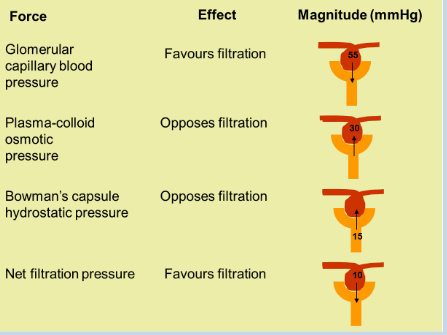
forces affecting GFR
• Balance of forces that favour or oppose filtration.
Difference in hydrostatic pressure on two sides of the filter.
• Blood pressure within glomerular capillaries.
• Fluid pressure within Bowman’s space.
Difference in protein-osmotic pressure on two sides of filter.
• Protein in blood within glomerular capillaries.
• Protein in fluid within Bowman’s space.
Is this an issue in a healthy animal? No-to maintain GFR without damaging the kidneys
Filtration Force: The hydrostatic blood pressure inside the glomerular capillaries pushes water and small wastes out into Bowman's space.
Opposing Forces: The fluid pressure in Bowman's space and the protein-osmotic pressure in the blood push back, preventing the kidneys from filtering too much fluid and causing rapid dehydration.
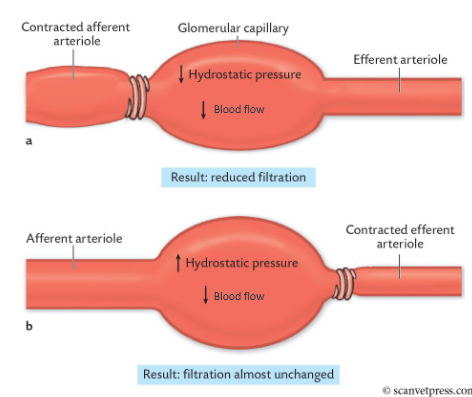
hydrostatic pressure
Constriction of the afferent arterioles decreases blood flow and decreases hydrostatic pressure. → Therefore, GFR is reduced
Constriction of the efferent arterioles also decreases blood flow but increases hydrostatic pressure.
• GFR remains almost unchanged as the decreased blood flow has an opposing effect to the increase in hydrostatic pressure
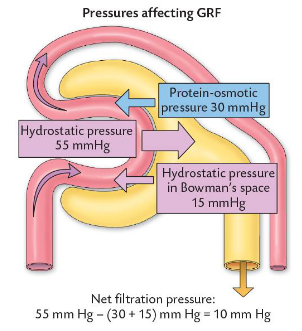
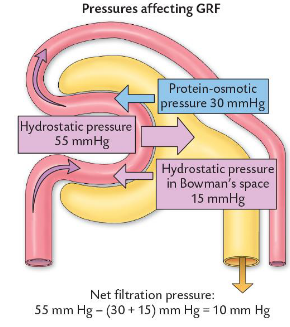
starlings formula
forces affecting GFR an be represented by formula (Starling’s formula):
GFR = Kf(ΔP) - Δπp
• (Kf = capillary filtration coefficient (barrier permeability x area)) – adjusted for in following values).
• GFR = (PGC - PBS) - (πGC - πBS)
• GFR = (55 - 15) - (30 - 0)
• GFR = 40 - 30
• GFR = 10 mmHg
The Three Pressures - blood vs tubule
Glomerular Capillary Blood Pressure (55 mmHg)
This is the main pushing force - we are pushing out everything in your blood except for blood cells and large proteins → filtrate (waste products and nutrients)
It pushes fluid out of the blood vessel.
It favors filtration
What gets pushed out:
Water: The main fluid carrying everything.
Wastes: Urea, uric acid, and creatinine.
Nutrients: Glucose (sugar) and amino acids.
Salts/Electrolytes: Sodium, potassium, and chloride.
What stays behind in the blood (because too big pass through):
-red and white blood cells, large proteins like albumin creating that pulling force
Plasma-Colloid Osmotic Pressure (30 mmHg)
This is a pulling force caused by proteins (cos blood contains large proteins like albumins, they are too big to pass through filter, so they stay trapped inside the blood vessel, and by physical law (osmosis) water is naturally pulled back in because the blood is now concentrated.
It pulls fluid back into the blood vessel.
It opposes filtration.
Bowman's Capsule Hydrostatic Pressure (15 mmHg)
This is a back-pressure from fluid already filtered - it’s like a funnel-think of coffee, fluid can only drain down the tube so fast, because the funnel stays full, fluid backs up - creating this backup of fluid
It pushes fluid back into the blood vessel.
It opposes filtration.
Essentially, this renal corpuscle just sorts things out by size and not usefulness, because your kidney accidentally pushings things your body needs like sugar and water, so later down the tube the kidney needs to actively grab the good stuff back in and put it in your blood.
In terms of squeezing blood out of the blood vessel and into the capsule, the fluid passes through a three-layer sieve:
capillary pores (fenestrations) - to stop blood cells from escaping
basement membrane - gelatin mesh barrier - uses negative charge to repel large proteins
podocyte filtration slits - foot processes of podocytes interlocking and creating narrow gaps called filtration slits - finest gateway letting fluid escape into rest of kidney
pathological factors affecting GFR
remember, GFR is the speed of fluid moving through the kidney tubules
(55 – 15) – 30) = 10
• Unregulated influences on GFR.
Decrease in plasma protein reduces pulling force opposing filtration so this increases GFR (burn patients/ liver disease).
cos basically less plasma protein in the blood because of this burn patient/liver disease case, less pulling force from water exiting the kidney tubule (osmosis) and entering the blood the vessel, so the blood vessel pressure stays low, and the tubule stays high, so the GFR stays high because the GFR measures the speed of fluid moving through the kidney tubules
• E.g. (55 – 15) – 20 = 20
Plasma-colloid pressure increases in dehydrating diarrhoea, so GFR is decreased.
• E.g. (55 – 15) - 35 = 5
In dehydrating diarrhoea, your body loses massive amounts of pure water. You’re losing water, not large plasma proteins, so those proteins become heavily crowded and concentrated inside your blood vessels. This creates huge osmotic pulling force from the proximal convoluted tubule, which drecreases the GFR
Urinary tract blockage – increases pressure in Bowman’s capsule – decreases GFR.
• E.g. (55 – 20) – 15 =
Urinary tract is blocked, so the fluid doesn't escape into the bladder, it backs up to the ureter tubes, up the kidney tubules, and back to the bowman's capsule. This creates massive hydrostatic pressure (back-pressure), this pushes firmly against the blood capillaries, and this opposing capsule pressure acts like a physical wall that blocks blood fluid from crossing the filter membrane to the point filtration stalls, causing GFR to decrease dramatically.
physiological factors affecting GFR
Factors adjust the renal blood flow and/or hydrostatic pressure.
Three main ways:
• Autoregulation (Intrinsic-internal/local control).
• Angiotensin II (Extrinsic-external/body-wide control).
• Sympathetic nervous system (Extrinsic)
Just a quick reminder:
Renin is made, stored and released by juxtaglomerular cells in the kidneys
Liver creates angiotensinogen. Renin converts angiotensinogen to angiotensin I in the capillares/blood stream.
ACE enzyme in the lungs converts angiotensin I to angiotensin II
This is triggered by low blood pressure, low salt/sodium, sympathetic energy
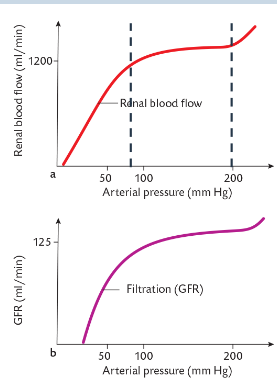
renal autoregulation
• The ability of the kidney to regulate its own blood flow
Functions to:
• Prevent large changes in GFR and urine output.
• Protect fragile glomerular capillaries.
• Variations in arterial blood pressure between 80-200 mmHg have little effect on perfusion of the kidneys and GFR.
• Blood flow (Q) = Change in arterial pressure (ΔP) / Afferent arteriole resistance (R)
• Q = ΔP / R
• Autoregulation is the kidney’s ability to change R so that Q is maintained despite changes in P
how is renal autoregulation achieved
• Involves only the afferent arteriole.
• The efferent arteriole is NOT involved.
Two mechanisms:
• Myogenic Response.
• Tubulo-glomerular Feedback
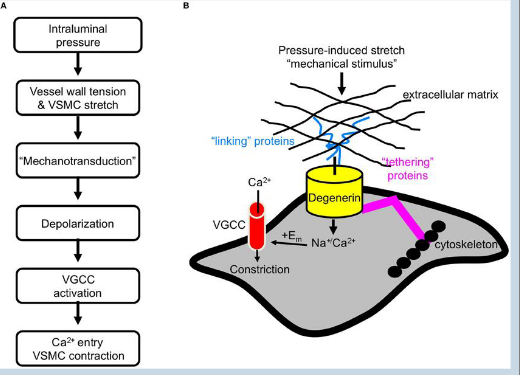
myogenic response - autoregulation 1
1. Arterial pressure increases (e.g. stress or exercise).
2. Afferent arteriole wall stretches under increased pressure.
3. Vascular smooth muscle cells (VSMC) detect stretch.
4. “Mechanotransduction” leads to depolarisation of the VSMC membrane.
5. Activates voltage-gated Ca2+ channels.- remember Ca2+ for actin-myosin movement
6. Influx of Ca2+ leads to the contraction of the VSMC.
7. Afferent arteriole constricts reducing the renal blood flow to the glomerulus
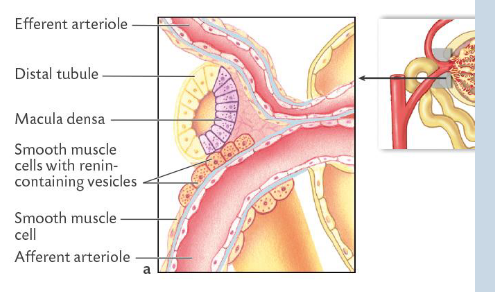
tubulo glomerular feedback - autoregulation 2
Distal convoluted tubule located in close proximity to afferent arteriole.
• Juxtaglomerular complex.
• Formed of junction between DCT/ascending loop of Henle and the afferent and efferent arterioles.
• Tubular wall has specialised epithelial cells that form the macula densa.
• Afferent arteriole wall has specialised smooth muscle cells in the wall called granular (juxtaglomerular) cells with renin- containing vesicles
Macula Densa Cells (The Sensor)
Where they are: They live inside the wall of the distal convoluted tubule
Their job: They act as chemical sensors. They constantly taste the fluid passing by to measure the amount of salt (sodium and chloride).
How they communicate: If salt levels drop, they send a chemical signal across the gap to their neighbors (the juxtaglomerular cells).
Juxtaglomerular Cells / JG Cells (The Worker)
Where they are: They live inside the wall of the afferent arteriole (the blood vessel bringing blood into the filter).
Their job: They act as physical pressure sensors and factories. They physically make, store, and release renin into the blood. - remember they indirectly cause vasoconstriction so renin has to trigger the RAAS pathway to eventually cause angiotensin II to vasoconstrict
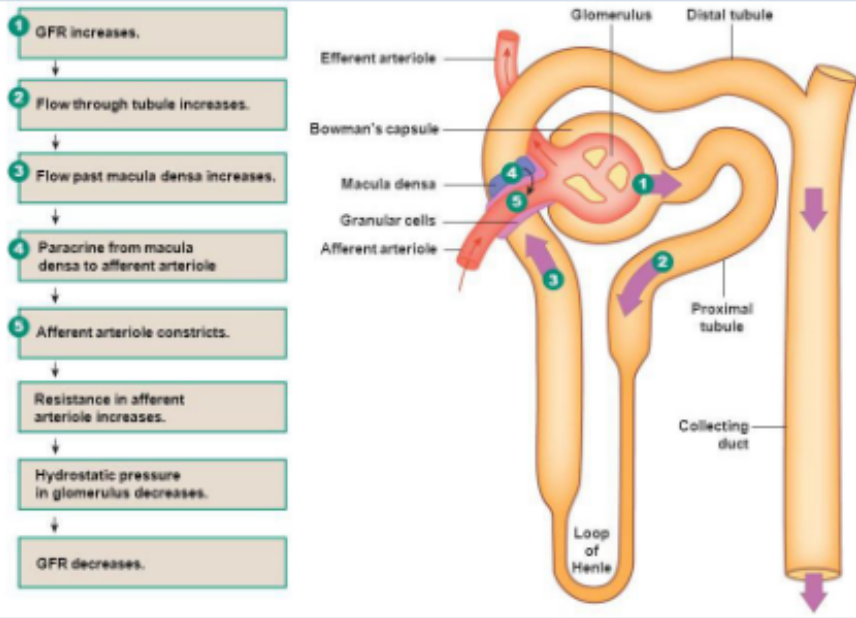
tubulo glomerular feedback - macula densa -local kidney protection-protect kidney from getting overwhelmed
• When pressure increases in the afferent arteriole, GFR increases.
• Increased GFR will lead to increased tubular flow rate.
• Increased tubular flow rate means increased NaCl flowing in the tubules as well.
• Macula densa cells sense this increase in NaCl flow leading to increased reabsorption of NaCl by the macula densa cells.
• NaCl uptake activates a non-selective cation channel which gates calcium entry that causes the macula densa cells to release paracrine agents such as adenosine or ATP.
• Juxtaglomerular cells respond to the paracrine agents and act to constrict the afferent arteriole.
renin- angiotensin - aldosterone system
Renin – produced and released by the granular juxtaglomerular cells in
response to a sustained low pressure.
• Enzyme that converts the precursor angiotensinogen to angiotensin I.
• Angiotensin converting enzyme (ACE) in pulmonary capillaries
converts angiotensin I to angiotensin II.
• Angiotensin II has numerous effects on the body to maintain arterial pressure.
• Constricts both afferent and efferent arterioles.
• Reduces blood flow but maintains GFR.
• A response to sustained or prolonged BP drop
additional mechanisms
Neural control.
• Renal arterioles and juxtaglomerular cells innervated by sympathetic nervous system.
• Can stimulate arteriole constriction.
• Can stimulate renin production.
• Similar effects to angiotensin II.
Hormonal control- extrinsic mechanism - body-wide volume relief-emergency system launched by the heart-protect heart from stretching and failing due to too much blood volume. Baiscally if you have too much water and salt in your body, your blood volume explodes, this stretches the chambers in the heart, heart gets stressed and dumps ANP into the blood. It does opposite to macula densa pathway, dilates the afferent arteriole to block salt rebsorption from GFR, so it forces kidneys to excrete the excess water and solt to low blood volume
• Atrial natriuretic peptide is a hormone that inhibits Na+ reabsorption thereby increasing Na+ loss in urine.
• Produced in the heart and secreted when plasma volume increases, which increases urine production.
Intrinsic and extrinsic mechanisms act to maintain GFR as best as possible – however GFR can be altered by physiological mechanisms