Antimicrobial Therapy
1/96
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
97 Terms
What are the three types of antimicrobial therapy?
1. Prophylactic Therapy: given to prevent an infection
Consider in individuals at increased risk of developing infection
Infection that has not occurred
2. Empiric Therapy: treatment given when an infection is suspected, before the organism(s) is identified
Antimicrobial selection guided by patient’s presentation and history
3. Targeted Therapy: treatment selected to target a specific organism known to be causing an infection
Antimicrobial selection guided by organism culture results and sensitivities
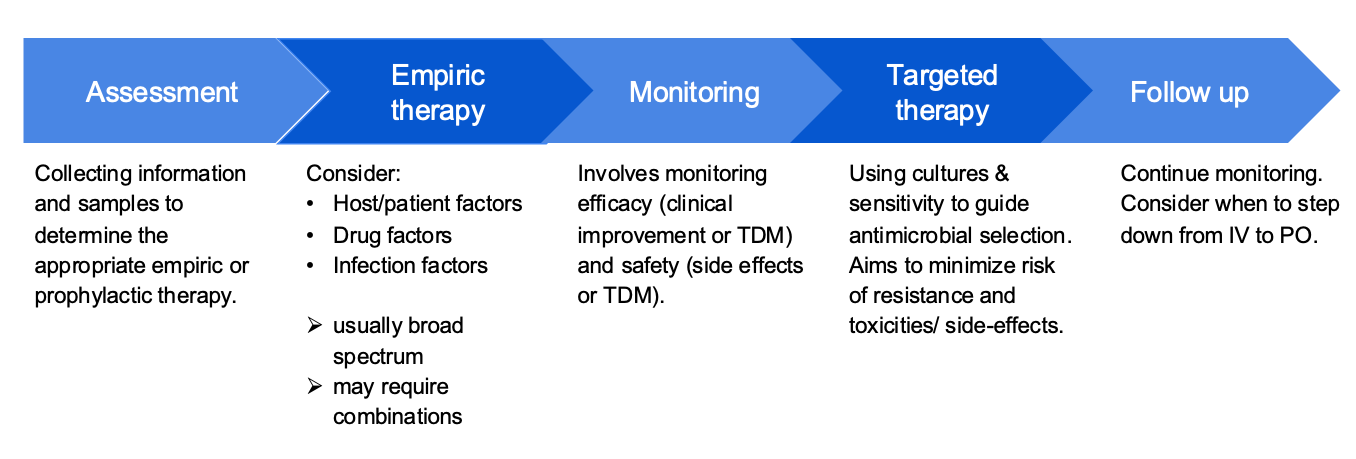
What are the 5 steps to antimicrobial therapy?
Assessment
Empiric therapy
Monitoring
Targeted therapy
Follow-up
Assessment step to microbial therapy
Information and Sample Collection
Information: Is there an infection? Any infectious history?
Sample: i.e. blood urine, sputum, for clinical or screening reasons.
Can conduct tests on them (gram staining, organism identification, and antibiotic susceptibility)
True or false: draw culture after administering antimicorbial agents.
False.
Especially for antibiotic susceptibility testing, collect sample first before antimicrobial therapy.
Drawing culture prior to administering any antimicrobial agents is important.
Collecting samples after a single dose of antimicrbials can refuce the likelihood of isolating an organism
What factors are involved with empiric therapy?
Host/Patient factors
Drug factors
Infection fators
What are some examples of host/patient factors?
Past medical history
Age
Allergies
Prior infections or hospitalization
Prior antimicrobial history
Prior drug colonization
History of resistance
What are the two main drug factors?
Pharmacokinetics (movement of drugs within the body)
Absorption: route of administration (IV vs PO)
Distribution: will the drug reach the site of infection?
Metabolism:
How is the drug broken down?
Drug-drug interactions
Excretion: how does the body get rid of the drug?
Pharmacodynamics (the action of the drug in the body)
Drug spectrum of activity
Mechanism of action
Combination therapy
Resistance
Drug Factors: What are the two antimicrobial spectrums?
Broad Spectrum: active against a large variety of organisms
Pro: Increased likelihood of activity against an unknown organism
Con: Promote the development of drug resistance
Should also consider the empiric therapy prior to organism identification
Narrow Spectrum: active against limited groups of organisms
Pro: Associated with reduced development of drug resistance
Con: Risk of poor activity / lack of effect against an unknown organism
Often used for targeted therapy after organism has been identified
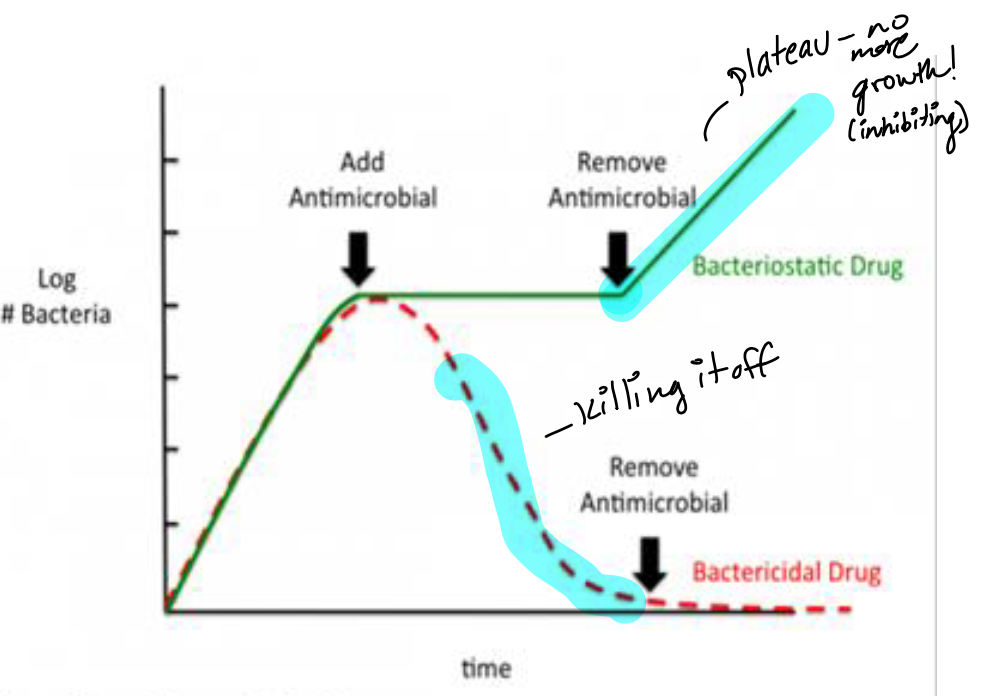
Bacteriostatic vs Bactericidal
Bacteriostatic:
Inhibits/slows bacterial growth
Requires a functioning immune system to clear infection
Used in less serious infections
Bactericidal:
Causes bacterial death
Preferred in serious infections or immunocompromised hosts
Drug factors: TIme vs Concentration dependent killing
TIme-dependent killing:
Drug concentration must remain above minimum inhibitory concentration for effect
The absolute amount of minimum inhibitory concentration does not impact activity
Concentration-dependent killing:
The peak drug concentration determines effect
Demonstrate a post-antibiotic effect where activity continues even when drug concentration is less than minimum inhibitory concentration
What are the types of combination therapy?
Synergism (combining different antimicrobials to produce an effect that exceeds the sum of their individual effects)
Broadens spectrum (combining antimicrobials with different spectrum to fill gaps in coverage)
Double coverage (combining 2 different antimicrobials with activity against the same organism of interest which increases likelihood of success and reduces development of antimicrobial resistance)
Antimicrobial Resistance
The ability of certain organisms to develop a tolerance to MDRO specific antimicrobials to which they were once susceptible
This process occurs naturally over time, but is accelerated by misuse and overuse of antimicrobials
Risk factors for developing drug resistant organisms
Prior antibiotic exposure
Underlying disease (hemodialysis)
Prior hospitalization
Invasive procedures in healthcare settings
What are the two main mechanisms of resistance for drugs?
Preventing the antimicrobial from reaching its target at sufficient concentrations
decreasing uptake into the organism
inactivating enzymes (i.e. beta-lactamases)
increased efflux
Modifying the target of the antimicrobial
altering the target
alternative enzymes
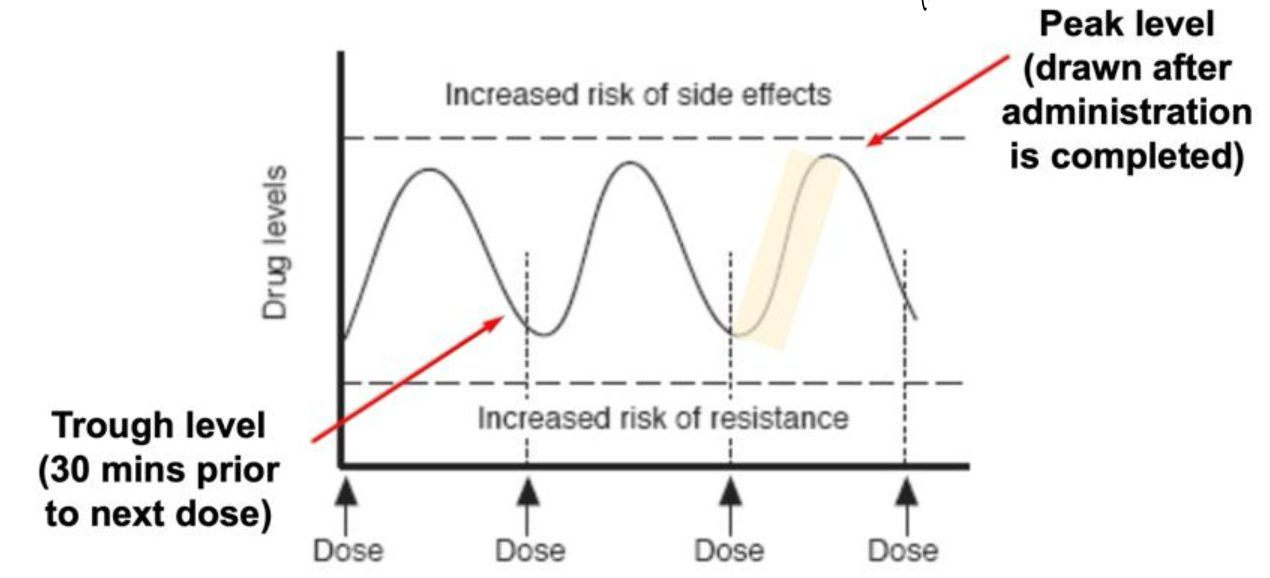
Different antimicrobials require levels to be drawn at various time points: Trough level
lowest serum concentration; draw blood 30 mins prior to next dose
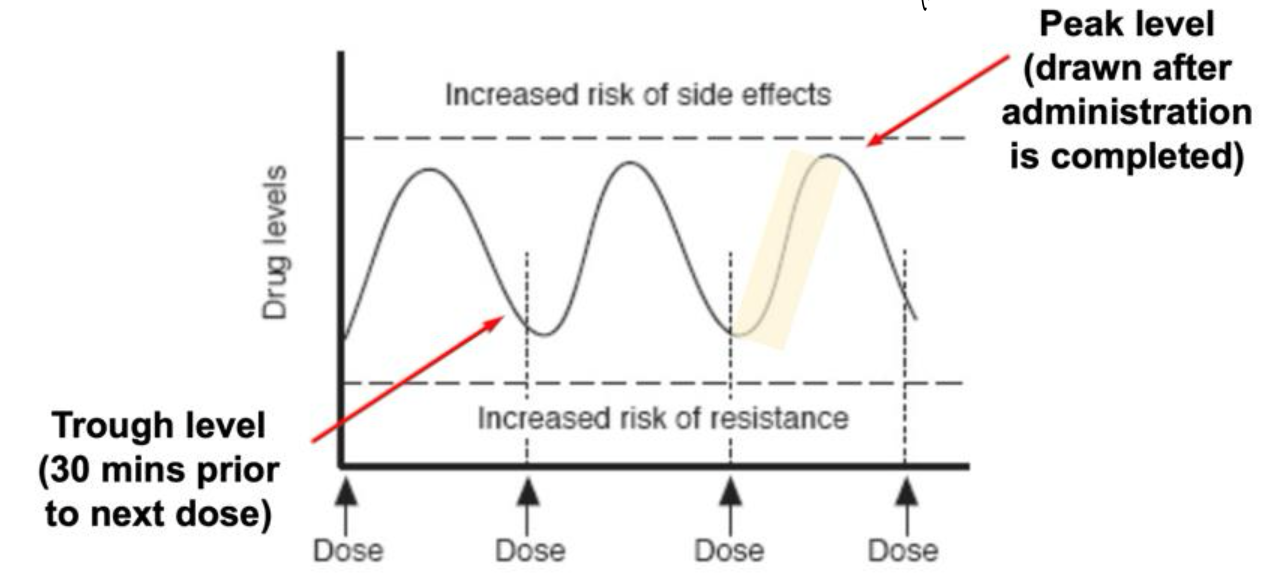
Different antimicrobials require levels to be drawn at various time points: Peak level
highest serum concentration: draw blood immediately after the dose has been administered
Are broad or narrow spectrum agents associated with a higher risk of resistance?
broad
Goal of targeted therapy
Choose an antimicrobial that has demonstrated activity against the organism but has the narrowest spectrum and the least toxicity
Antimicrobial Principles: Summary
What are some targets of antibiotics?
Cell wall
DNA / RNA synthesis
Plasma membrane
Ribosomes
Metabolic pathways
Create free radicals
What are bacterial cell walls made up of? What is transpeptidation?
Peptidoglycan: major component
Transpeptidation: the last step of cell wall synthesis
Penicillin binding proteins (PBPs) form cross links in the cell wall
What are the three main types of Beta-Lactams?
Penicillins, Cephalosporins, and Carbapenems
What is the mechanism of action for beta-lactams?
Beta-lactams interrupt cell wall synthesis by:
Binding to PBPs
Inhibits transpeptidation
Results in:
Improper cell wall formation → inability to withstand osmotic pressure → cell ruptures → cell death
Bactericidal, time-dependent killing
Beta-lactam penicillins: Spectra, Uses, Adverse effects
Spectra: Narrow, covers Gram-positives > Gram-negatives
Commonly used for: Otitis media, skin infections, strep throat
Adverse effects:
Common: GI upset, rash
Uncommon: Anaphylaxis, seizures, hemolytic anemia, neutropenia, thrombocytopenia
What are the mechanisms of resistance for beta-lactams?
1. Bacterial cell production of beta-lactamases
2. Modification PBP binding site (e.g., Methicillin-resistant Staphylococcus aureus [MRSA])
3. Changes to porin channels
4. Drug efflux pumps
What is Beta-lactamase?
an enzyme that cleaves the beta-lactam ring through hydrolysis
Inactivates beta-lactam antibiotics
breaks the bond between penicillin and the lactam ring
When are beta-lactams paired with beta-lactamase inhibitors? What may be some issues? What’s an example?
to overcome resistance
Inactive beta-lactamases to extend spectrum of activity → MSSA, gram negatives, anaerobes
Increase risk of nausea, vomiting and diarrhea (including C. difficile infections)
Examples: Amoxicillin-clavulanic acid (IV, PO), Piperacillin-tazobactam (IV)
Beta-lactam cephalosporins: Spectra, Uses, Adverse effects
Spectra: Mid-to-broad, covers Gram-positives and increasing Gram-negatives coverage with higher generations
Used for: Skin and soft tissue infections, pneumonia, intra-abdominal infections, pyelonephritis
Adverse effects: GI upset, rash, seizures. With higher generations there is an increased risk of C. difficile infection and resistance
What are the generations of cephalosporins?
First-fifth generations
Increasing generation → increasing gram negative coverage
Beta-lactam carbapenems: Spectra, Uses, Adverse effects
Spectra: Broad, covers Gram-positives, Gram-negatives, oral andgut anaerobes
Used for: Only for severe, infections caused by ESBL or Amp-C producing bacteria. Note: Infectious Disease team should be involved
Adverse effects: GI upset (nausea, diarrhea), eosinophilia, seizures, resistance, increased risk of C. difficile infections
Up to 10% of patients have a reported penicillin allergy, but < 1% are a true allergy. What is a true allergy?
Type I IgE-mediated: anaphylaxis, hypotension, angioedema
Avoid all penicillins and cephalosporins with similar side chain
Low cross-reactivity between beta-lactams, but stay away from all beta-lactams if you’ve ever had a reaction to one of them
What is an example of a severe non-IgE-mediated hypersensitivity reaction?
Type IV non-IgE-mediated: Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), drug rash with eosinophilia and systemic symptoms (DRESS)
Avoid all beta-lactams (penicillins, cephalosporins and carbapenems)
What antibiotics target the cell wall?
Beta lactams (penicillins, cephalosporins, monobactams, and carbapenems)
Glycopeptides (vancomycin)
Bacitracin
Fosfomycin
What is the mechanism of action for vancomycin?
Inhibits cell wall synthesis
Binds to the terminal end of peptidoglycan precursor → prevents polymerization → weakens the cell wall → cell death
Bactericidal, time- dependent killing
Vancomycin: Spectra, Uses, Adverse effects
Spectra: Gram-positives only, including MRSA
Uses: IV: MRSA infections, endocarditis, meningitis PO: C. difficile infections
Adverse effects: Ototoxicity, nephrotoxicity, infusion reactions, irritation and injection site reactions
Oral formulation used exclusively for C diff infections
Vancomycin can give an infusion reaction called Flushing Syndrome. What is it?
Characterized by pruritus, flushing, and erythema of the face and upper torso → NOT life-threatening
Due to rapid infusion of the drug leading to histamine release
Related to infusion rate
Managed by slowing the infusion rate
What makes a vancomycin allergy different than an infusion reaction?
Vancomycin allergy:
Anaphylaxis, hypersensitivity, hives, angioedema, bronchoconstriction → can be life-threatening
Managed by stopping infusion and administering epinephrine
What to monitor when on vancomycin?
Nephrotoxicity (increasing serum creatinine (SCr) and decreasing urine
output)
Serum trough levels once at steady state (pre-fourth dose)
Low trough (< 10 mg/L) → subtherapeutic, inadequate dose for treatment
High trough (> 20 mg/L) → supratherapeutic, increased risk of nephrotoxicity
If trough is out of range, let the pharmacist know for dose adjustment
What is the mechanism of action for fosfomycin?
Inactivates MurA enzyme involved in peptidoglycan synthesis → weakens cell wall → cell lysis
inhibits adherence of bacteria to epithelium
Bactericidal, concentration dependent killing
Fosfomycin: Spectra, Uses, Adverse effects
Spectra: broad, gram positives and gram negatives
Uses: Uncomplicated UTI (PO), meningitis, intra-abdominal infections, skin and soft tissue infections
Adverse effects: GI upset, electrolyte disturbances, C. difficile infection, hypersensitivity reactions
What antibiotics target the plasma membrane?
Polymyxins (polymyxin B and colistin)
Lipopeptides (daptomycin)
What is the mechanism of action of daptomycin?
Binds to the cell membrane leading to depolarization, efflux of potassium, and inhibition of DNA, RNA and protein synthesis
Bactericidal, concentration dependent killing
Daptomycin: Spectra, Uses, Adverse effects
Spectra: Gram-positives only, including MRSA
Uses: Complicated skin and soft tissue infections, S. aureus bacteremia, infective endocarditis
Adverse effects: Myopathy/rhabdomyolysis, eosinophilic pneumonia
Avoid with pneumonia
What to monitor for when patient is on daptomycin?
Rhabdomyolysis: rapid breakdown of skeletal muscle
Can be life-threatening
Monitor: patient reported muscle pain, creatine kinase (CK) and dark urine
Eosinophilic pneumonia
Monitor: eosinophils, new-onset fevers and dyspnea
What antibiotics target DNA synthesis?
Fluoroquinolones
Ciprofloxacin
Levofloxacin
Moxifloxacin
What antibiotics target RNA synthesis?
Rifamycins
Rifampin
What is the mechanism of action for Fluoroquinolones?
Inhibition of DNA synthesis by inhibiting bacterial DNA gyrase and topoisomerase IV → promotes the breakage of DNA
Bactericidal, concentration dependent killing
Fluroquinolones: Spectra, Uses, Adverse effects
Spectra: Broad, Gram-positives, Gram-negatives, and atypicals
Uses: Ciprofloxacin - UTIs, bacteremia, Levofloxacin, moxifloxacin - pneumonia
Adverse effects: GI symptoms, photosensitivity, C. difficile infections, QTc prolongation, tendonitis (most commonly Achilles tendon), seizures, CNS effects
Avoid if pregnant or breastfeeding
Fluoroquinolones and metal cations
Fluoroquinolones bind bivalent or trivalent metal cations → decrease absorption
Avoid administering oral fluoroquinolones with bivalent or trivalent metal cations by 2 hours
This includes supplements such as: zinc, magnesium, iron, calcium (e.g., TUMS and other antacids, multivitamins, iron supplements)
What antibiotics create free radicals?
Metronidazole
Nitrofurantoin
What is the mechanism of action for metronidazole?
Becomes reduced by anaerobic organisms → becomes cytotoxic free radical that breaks DNA, inhibits nucleic acid synthesis and results in loss of DNA integrity → cell death
Bactericidal, concentration dependent killing
Metronidazole: Spectra, Uses, and Adverse Effects
Spectra: Anaerobes
Uses: C. difficile infection, intra-abdominal infections
Adverse effects: Nausea/vomiting, metallic taste, peripheral neuropathy, disulfiram-like reaction with alcohol use
Avoid alcohol use.
What antibiotics affect metabolic pathways?
Folic acid synthesis
sulfonamides
sulfones
trimethoprim
mycolic acid synthesis
izoniazid
What is the mechanism of action for Sulfamethoxazole/Trimethoprim?
Sulfamethoxazole (SMX) and trimethoprim (TMP) work together synergistically
Inhibits folic acid synthesis which is necessary for DNA synthesis
Bactericidal; time dependent killing
Sulfamethoxazole/Trimethoprim: Spectra, Uses, and Adverse Effects
Spectra: Gram-positives (including MRSA) and Gram-negatives
Uses: UTI, Pneumocystis jiroveci prophylaxis
Adverse effects: Skin rash (SJS, TENS; uncommon), hyperkalemia, thrombocytopenia (rare), nephrotoxicity
Avoid for the following:
History of severe reaction to sulfonamides, pregnant (1st and 3rd trimester) and breastfeeding, neonates, glucose 6-phosphate dehydrogenase deficiency
What antibiotics affect the 30S subunit ribosome?
Aminoglycosides
Tetracyclines
What antibiotics affect the 50S subunit ribosome?
macrolides
lincosamides
chloramphenicol
oxazolidnones
What is the mechanism of action for Linezolids (oxazolidinones)?
Binds to the P-site of the 50S ribosomal unit → prevents formation of the 70S complex
Bactericidal against streptococci
bacteriostatic against staphylococci and enterococci
Time dependent killing
Linezolids: Spectra, Uses, and Adverse Effects
Spectra: Gram-positives (including MRSA)
Uses: Pneumonia, bloodstream infections, endocarditis, hospital-acquired meningitis
Adverse effects: Myelosuppression (> 2 weeks use), peripheral/optic neuropathy (> 4 weeks use), C. difficile infection, lactic acidosis, serotonin syndrome
Avoid if on MAOIs.
What is the mechanism of action for macrolides?
Reversibly binds to the 50S ribosomal subunit → prevents transpeptidation → protein synthesis inhibited
Bacteriostatic, time dependent killing
Ex. azithromycin, clarithromycin, erythromycin
Macrolides: Spectra, Uses, Adverse effects
Spectra: Gram positives, atypical bacteria and some Gram negatives
Uses: Community acquired pneumonia, sexually transmitted infections
Adverse effects: GI upset, QTc prolongation, hepatotoxicity, hypersensitivity reaction
What is the mechanism of action for clindamycin (lincosamide)?
Similar mechanism to macrolides: reversibly binds to 50S ribosomal subunit → inhibits transpeptidation → protein synthesis inhibited
Bacteriostatic, time dependent killing
Clindamycin: Spectra, Uses, Adverse effects
Spectra: Gram-positives, anaerobes
Uses: Skin and soft tissue infections, dental infections
Adverse effects: C. difficile infection, GI symptoms, rash
What is the mechanism of action for aminoglycosides?
Binds irreversibly to the 30S ribosomal subunit → prevents transpeptidation → protein synthesis inhibited
Bactericidal, concentration dependent killing
Aminoglycosides: Spectra, Uses, Adverse effects
Spectra: Gram negatives, synergy with beta-lactams for Gram positives
Uses: Sepsis caused by Gram-negatives, UTIs, intra-abdominal infections, endocarditis (with beta-lactams)
Adverse effects: Reversible nephrotoxicity (can monitor drug levels), irreversible oto- and vestibular toxicity
Aminoglycosides: Dosing types
Extended-interval dosing: single, large dose once daily
More rapid bactericidal activity and less toxic
Recommended for most infections in most patients
Traditional dosing: Smaller doses given multiple times a day
Used when can’t use extended-interval dosing and for synergy
What is the mechanism of action of tetracyclines?
Bind to the 30S ribosomal subunit → blocks the attachment of tRNA to mRNA-ribosome complex → protein synthesis inhibited
Bacteriostatic, time dependent killing
Examples: tetracycline, doxycycline, minocycline
Tetracyclines: Spectra, Uses, Adverse effects
Spectra: Broad, Gram-positives, Gram-negatives, certain anaerobes
Uses: Acne, skin and soft tissue infection, Lyme disease
Adverse effects: Damage growing bones and teeth, GI upset, dizziness/vertigo, photosensitivity
Avoid in pregnancy and children. Separate from metal cations.
What are the three types of fungi?
Yeast
Single celled, budding reproduction E.g., Candida species
Mold
Multi cellular, branching filaments E.g., Aspergillus species
Dimorphic fungi
Yeast at higher temps (37°C)
Mold at lower temps (25°C) E.g., Histoplasma
What is the cell membrane of fungi made up of?
Ergosterol → fungal version of cholesterol
Azoles and terbinafine target ergosterol synthesis
Chitin → like cellulose and beta-glucan → similar to fibre
two most important substances
Polyoxins inhibit chitin synthase
Echinocandins inhibit Beta-glucans synthesis
What is the mechanism of action for polyenes?
Binds to ergosterol in the fungal membrane → form a pore through the membrane → electrolyte leakage → cell death
Resistance: rare, due to decrease or change in structure of ergosterol
Fungicidal
Polyenes - Nystatin: Spectra, Uses, Adverse effects
Spectra: Candida
Uses: Superficial oral candidiasis (Thrush)
Adverse effects: Generally well-tolerated, gastrointestinal upset
Avoid with systemic infections (Poorly absorbed, cannot be used for systemic infections)
Polyenes - Amphotericin B: Spectra, Uses, Adverse Effects
Spectra: Most broad spectrum; most activity against infections
Uses: Systemic mycoses
Adverse effects: Nephrotoxicity, hepatotoxicity, infusion-related reactions (fever, chills, headache, arrhythmia, cramps, weakness), electrolyte abnormalities
Echinocandins - Mechanism of Action
Inhibits the synthesis of Beta (1,3)-D-glucan (component of the cell wall) by inhibiting Beta (1,3)-D-glucan synthase
Impaired cell wall synthesis→ cell rupture and death
Fungicidal (Candida) or Fungistatic (Aspergillus)
Echinocandins - Caspofungin, Anidulafungin, Micafungin: Spectra, Uses, Adverse Effects
Spectra: Most Candida Species, all Aspergillus species
Uses: Candidiasis, aspergillosis
Adverse effects: Typically well tolerated, infusion related reactions (rash, facial swelling, respiratory spasms, gastrointestinal distress), hepatotoxicity
Avoid with CNS, urinary or ocular infection
What to monitor for echinocandins?
Monitor for potential infusion reactions (e.g., facial swelling, flushing, rash)
Monitor liver function (caspofungin requires dose adjustment in hepatic impairment)
Echinocandins - What method of administration?
IV ONLY; if oral therapy is clinically warranted and the infection is susceptible, a switch to an alternate antifungal would be required
Poor penetration to CNS, vitreal fluid and urine
Very few drug interactions
Azoles - Mechanism of Action
Inhibits cytochrome P450 14-alpha lanosterol demethylase → inhibits conversion of lanosterol to ergosterol → increases permeability and accumulation of toxic sterols → cell death
Resistance: altered drug binding site
Fungicidal or fungistatic (depending on species)
Azoles: Spectra, Uses, and Adverse Effects
Spectra: Broad spectrum depending on agent
Uses: Topical Agents: Tinea infections, superficial candidiasis, Oral/IV agents: Systemic Mycoses (Candidiasis)
Adverse Effects: Headache, nausea and vomiting, diarrhea, rash, hepatotoxicity, QTc prolongation, hallucinations (voriconazole)
Clinical Pearls of Azoles
Intravenous to oral Step Down: bioavailability is typically high and oral may be used even for deep seated infections
Many drug interactions!
Renal and hepatic function must be monitored on oral/IV therapy; QTc prolongation can occur with any systemic azole
What azole has the best safety profile?
If susceptible, use fluconazole as it has the best safety profile + excellent oral bioavailability + excellent penetration into CNS/vitreal fluid
What is the mechanism of action for Terbinafine?
Interferes with squalene epoxidase → inhibit ergosterol biosynthesis → alter cell membrane permeability and accumulation of toxic sterols → cell death
Resistance: mutation in squalene epoxidase
Fungicidal
Terbinafine - Spectra, Uses, Adverse Effects
Spectra: Dermatophytes, Candida
Uses: Superficial Mycoses
Adverse Effects: Headache, nausea/vomiting, diarrhea, rash, skin reactions, hepatotoxicity
Avoid with breastfeeding
What are viruses?
Consist of DNA or RNA within a protein outer shell
Require the use of host cell machinery to replicate; cannot replicate on their own
Infect host cells and “re-program” to replicate and the virus
What are the two types of antivirals?
Neuraminidase Inhibitors and Polymerase Inhibitors
Neuraminidase Inhibitors – Mechanism of Action
Neuraminidase is an influenza viral enzyme that facilitates the release of new viruses
These drugs inhibit this process - preventing the virus’ ability to spread and replicate further
What allows for resistance to neuraminidase inhibitors?
Mutations in the neuraminidase enzyme prevent the antivirals from binding
Neuraminidase Inhibitors - Oseltamivir (PO), Zanamivir (inhaled) - Spectra, Uses, and Adverse Effects
Spectra: Activity against Influenza A & B
Uses: Prophylaxis or treatment of Influenza A or B
Adverse Effects: Oseltamivir: Nausea/vomiting, headache, confusion/delirium (rare), Zanamivir: bronchospasms (avoid in Asthma or COPD)
When should you take oseltamivir for maximum benefit?
Take oseltamivir with food (to improve tolerability), start treatment within 48 h for maximum benefit
Polymerase Inhibitors – Mechanism of Action
DNA polymerase is responsible for viral DNA synthesis
Polymerase inhibitors incorporate into viral DNA by competing for DNA polymerase → inhibits DNA synthesis
What causes resistance in Polymerase Inhibitors?
Mutations in viral DNA polymerase or thymidine kinase
Polymerase Inhibitors: Narrow Spectrum: Acyclovir (IV/PO), Valacyclovir (PO), Famciclovir (PO) - Spectra, Uses, Adverse Effects
Spectra: Narrow, activity against HSV, VZV
Uses: Treatment of oral herpes (HSV1), anogenital herpes
(HSV2) and shingles (VZV)
IV acyclovir often used HSV encephalitis
Adverse effects: Nephrotoxicity, headaches, anorexia, vomiting
IV acyclovir
infuse slowly and maintain hydration to reduce risks of nephrotoxicity
Polymerase Inhibitors: Broad Spectrum: Ganciclovir (IV/PO), Valganciclovir (PO) - Spectra, Uses, Adverse Effects
Spectra: Activity against HSV, VZV, CMV (only additional virus!)
Uses: Treatment or prophylaxis of CMV, VZV only
Adverse Effects: Neutropenia (20-40%), thrombocytopenia (10-20%), nephrotoxicity, diaphoresis, diarrhea, anorexia, vomiting
Oral ganciclovir
very poor bioavailability (5%) and rarely used, reduce risk of nephrotoxicity by slow infusion and maintaining hydration
The choice of empiric antibiotic therapy is influenced by what?
patient-specific factors, characteristics of the infection and pathogen, drug properties, and supporting clinical evidence
What is targeted antibiotic therapy?
tailored to a specific pathogen