Respiratory System
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
100 Terms
what does the upper respiratory tract include?
The nasal cavity and paranasal sinuses
The pharynx
The larynx, above the level of the vocal folds
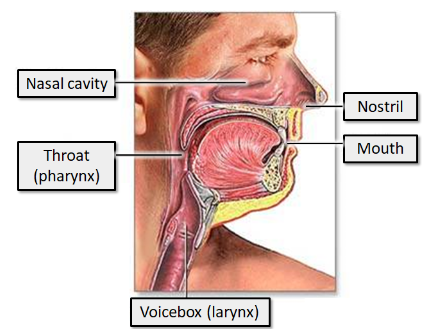
what 3 things does the upper respiratory system ensure about the inspired air?
Before reaching the lungs, air is:
Warmed to body temperature
Humidified
Filtered for particulates (>10μm)
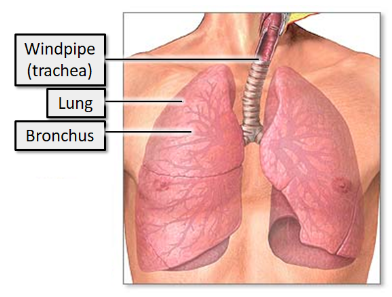
what does the lower respiratory tract include?
The larynx below the level of the vocal folds
The trachea
The bronchi
The bronchioles
The lungs
what is the purpose of the lower respiratory tract?
is concerned with gas exchange, by conducting inspired air to the tissues involved in gas exchange, and further trapping and removal of particulates.
what controls the rhythm of breathing?
brainstem
lower part of the brainstem, in an area called the medulla oblongata
what neurones automatically maintain a rhythmic cycling pattern of inspiration and expiration?
“inspiratory neurones” which are active during inspiration and inactive during expiration
active during expiration but not inspiration: the “expiratory neurones”
is the right or the left lung bigger and why?
The right lung is normally a little larger than the left lung because the middle mediastinum, containing the heart, bulges more to the left than to the right.
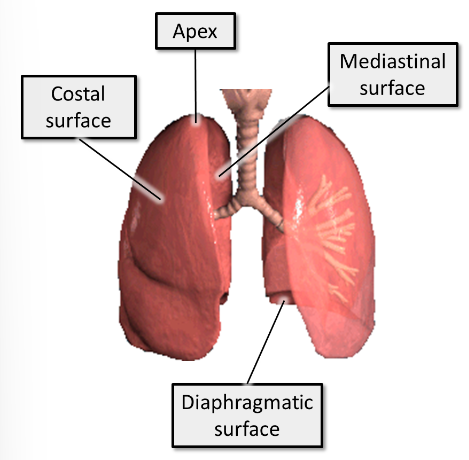
where is the apex located in relation to the neck and ribs?
An apex - this extends superiorly into the root of the neck, above the first rib
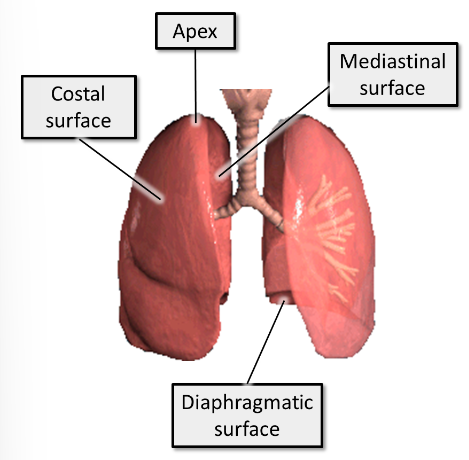
what 3 surfaces do the lungs have?
1. Costal - close to ribs/costal cartilages and intercostal spaces
2. Mediastinal - close to the mediastinum anteriorly and vertebral column posteriorly. This surface contains the hilum of the lung
3. Diaphragmatic (base of lung) - sits on the diaphragm
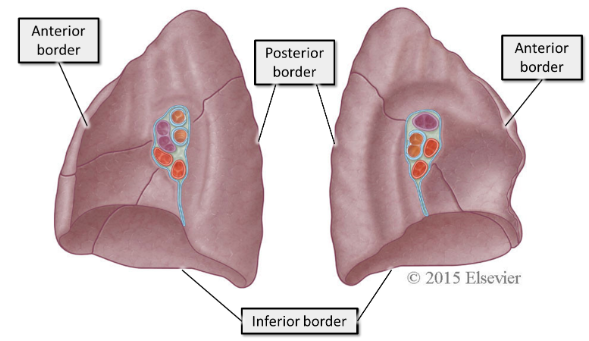
what borders do the lungs have?
1. Inferior - separates the base from the costal surface
2. Anterior - separates costal surface from mediastinal surface. The anterior border of the right lung is relatively straight, whereas the anterior border of the left lung has a deep cardiac notch.
3. Posterior - separates costal surface from mediastinal surface. The other two borders are sharp, but the posterior border is smooth and rounded
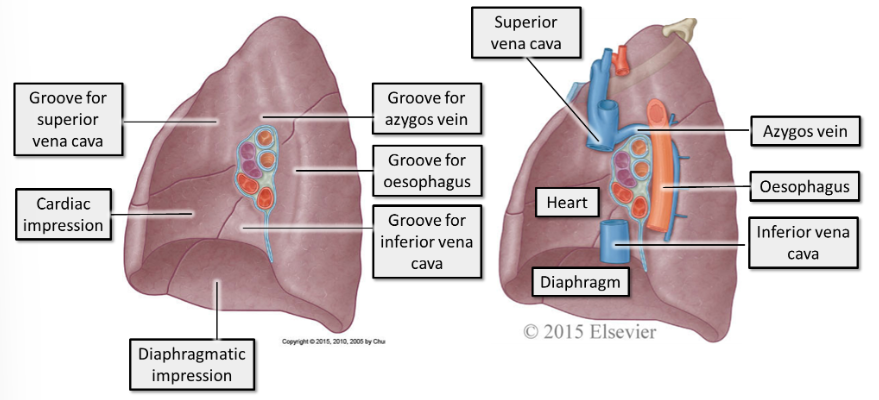
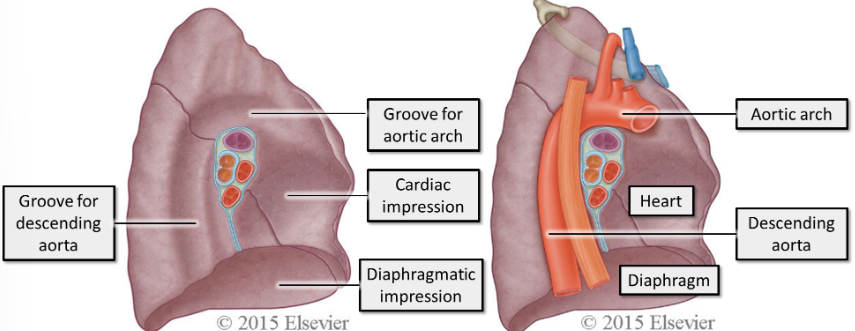
what are the mediastinal surfaces?
The mediastinal surfaces of the lungs are closely related to several structures. These structures leave impressions in the spongy surface of the lung.
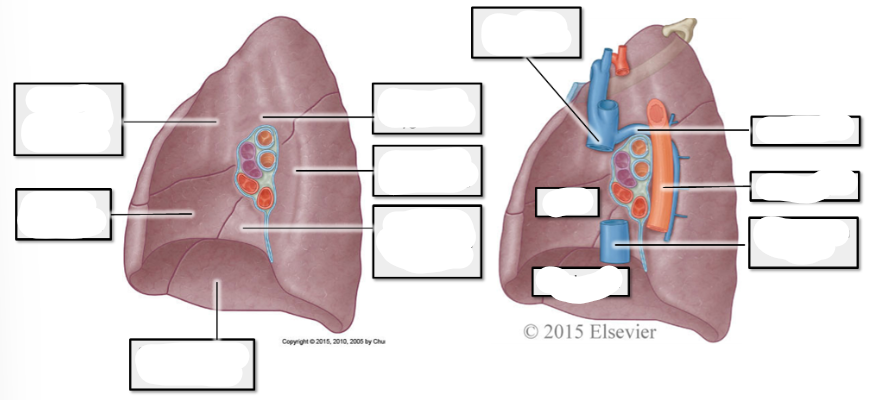
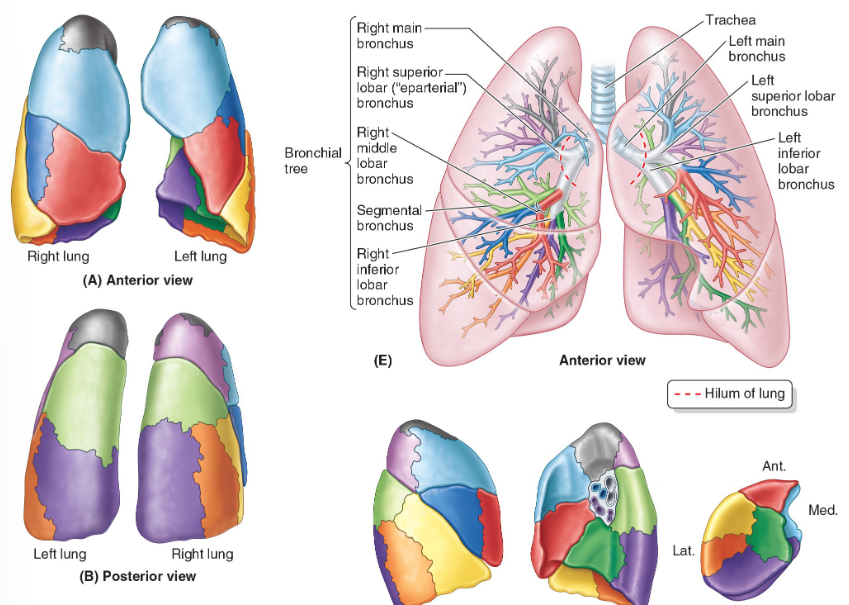
label right lung
label left lung
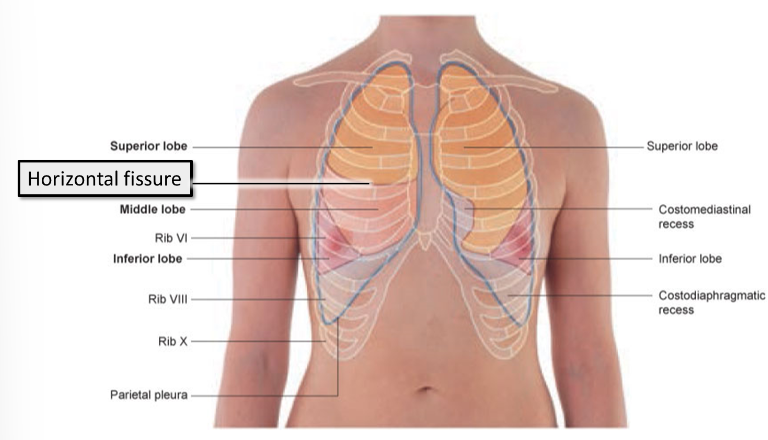
how many lobes does each lung have?
The right lung - has 3 lobes separated by 2 fissures
The left lung - has 2 lobes separated by 1 fissure
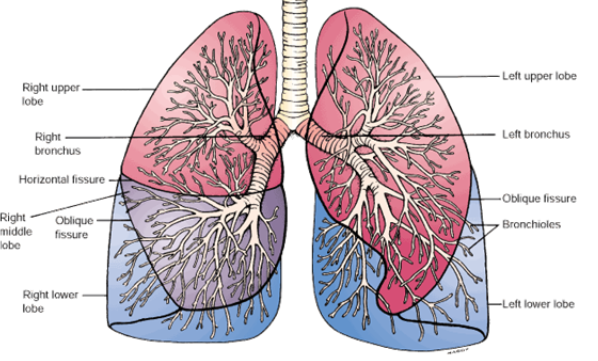
what fissures divide the lungs into lobes?
horizontal and oblique fissures
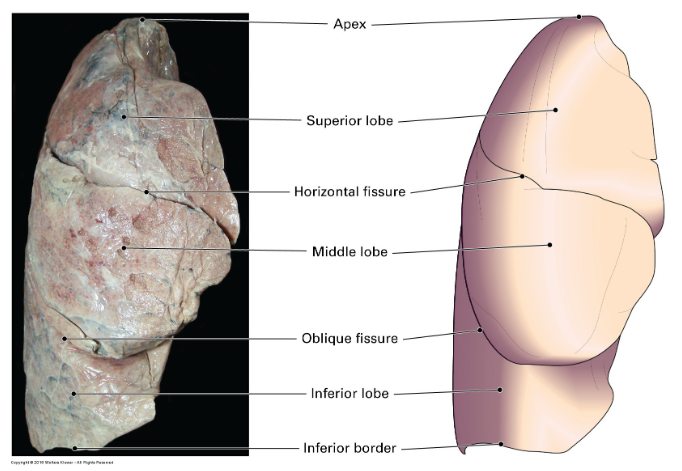
what are the names of the right lungs lobes?
The superior lobe is mainly in contact with the anterior thoracic wall and projects into the root of the neck
The middle lobe is mainly in contact with the anterior and lateral thoracic wall
The inferior lobe is mainly in contact with the posterior and inferior thoracic wall
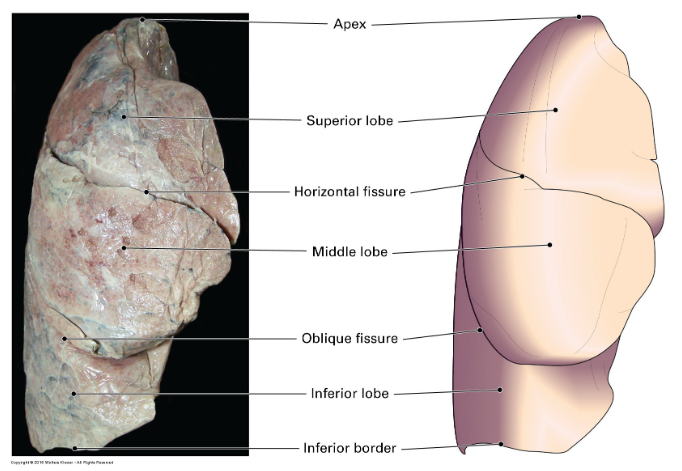
which fissures separate which lobes on the right lung?
The oblique fissure separates the inferior lobe from the superior lobe and the middle lobe.
The horizontal fissure separates the superior lobe from the middle lobe.
what are the names of the left lungs lobes?
The superior lobe is mainly in contact with the upper part of the anterior and lateral thoracic wall and projects into the root of the neck
The inferior lobe is mainly in contact with the posterior and inferior part of the thoracic wall
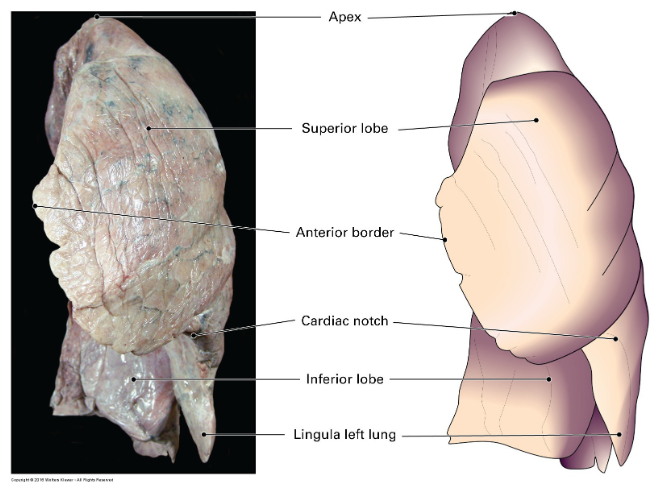
which fissures separate which lobes on the left lung?
The oblique fissure separates the inferior lobe from the superior lobe.
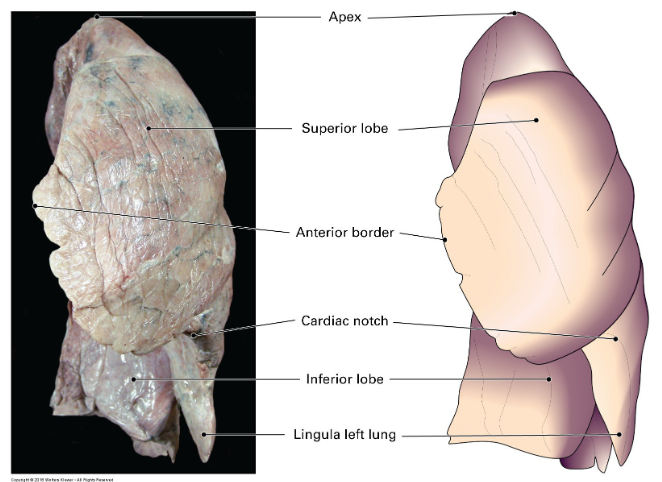
what additional structure does the left lung contain to covers the heart?
The left lung also has a lingula, a tongue-like projection that extends over the anterior surface of the heart.
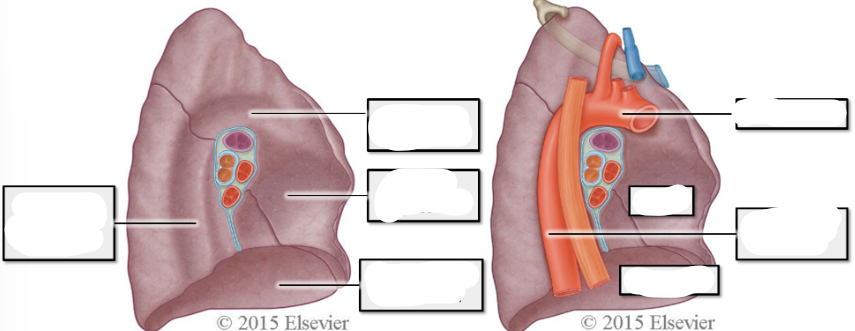
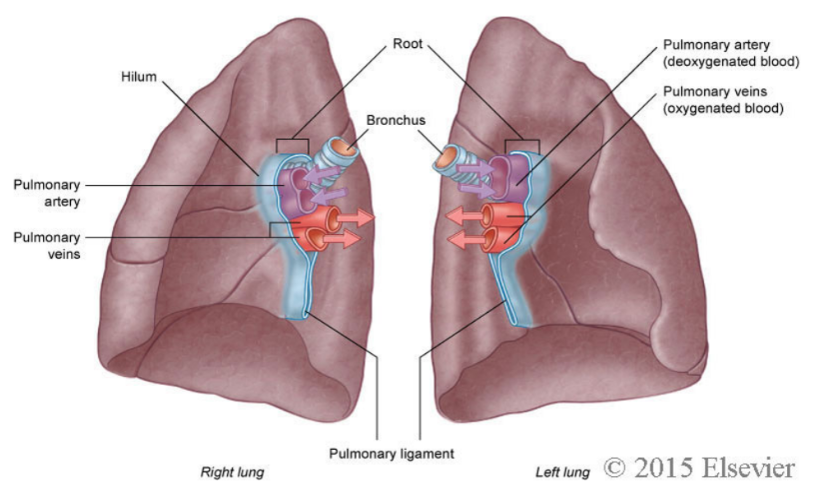
what is the hilum of the lung?
The lungs attach to the heart and trachea by several structures that are collectively referred to as the roots of the lungs.
The area at which these structures enter and leave the lung is known as the hilum of the lung.
what structures make up the root of the lung and enter/leave at the hilum?
A pulmonary artery
Two pulmonary veins
A main bronchus
Bronchial vessels
Nerves
Lymphatics
differentiate between the wall thickness of bronchi, pulmonary arteries and pulmonary veins
Bronchi have the thickest, strongest walls. They are strong, cartilaginous and do not compress or collapse easily.
The pulmonary arteries have thinner walls than bronchi, however they are thicker than pulmonary veins. Arterial walls are elastic, and if compressed, will spring back into shape on being released.
Pulmonary veins have the thinnest walls. They are easily collapsible and are not elastic, so do not retain their tubular shape as easily as bronchi or arteries.
what is the position of the bronchi, pulmonary arteries, pulmonary veins in relation to each other
The exact position of these structures at the hilum can vary, but the pulmonary artery is usually more superior, the pulmonary veins are inferior, and the bronchi are more posterior in position.
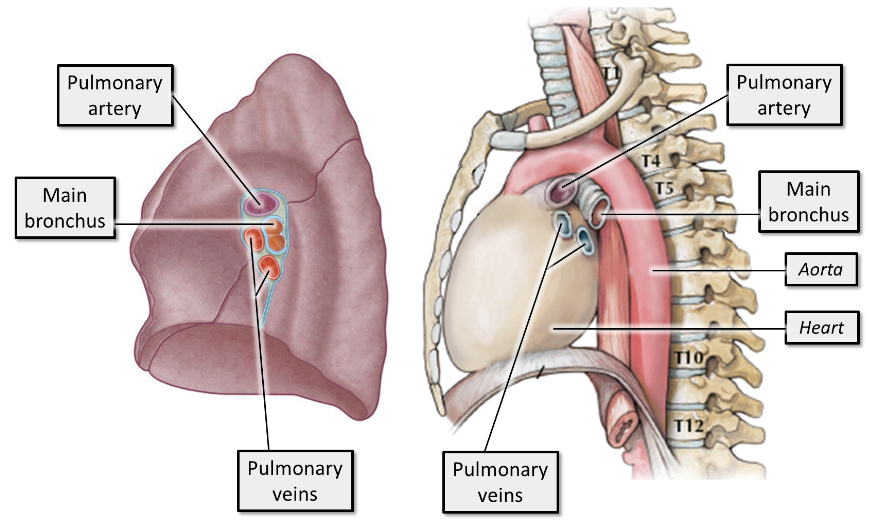
what structures of the lung are level with T1, T10, and T12
The most superior aspect of the lungs is their apex. The apex of the lungs lies just above the first rib superiorly, level with T1.
The most inferior aspect of the lungs is level with T12 at their most inferior point in the posterior thorax on inspiration. The inferior aspect of the lungs is in contact with the diaphragm.
In quiet respiration, the inferior margin of the lungs travels around the thoracic wall, following rib 6 down to rib 8, from vertebral level T10 posteriorly.
where is the oblique fissure?
Posteriorly - in the midline, near the spine of vertebra T4
Laterally - descends diagonally, crossing the 4th and 5th intercostal spaces to reach rib 6
Anteriorly - follows rib 6 and its costal cartilage
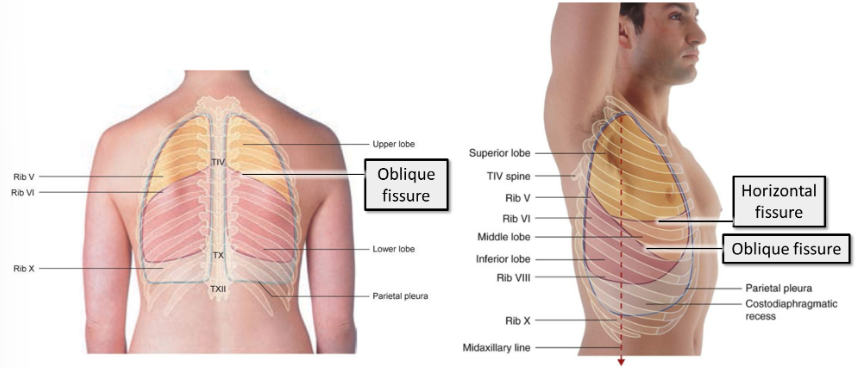
where does the horizontal fissure lie?
Lies anteriorly, following the contour of rib 4.
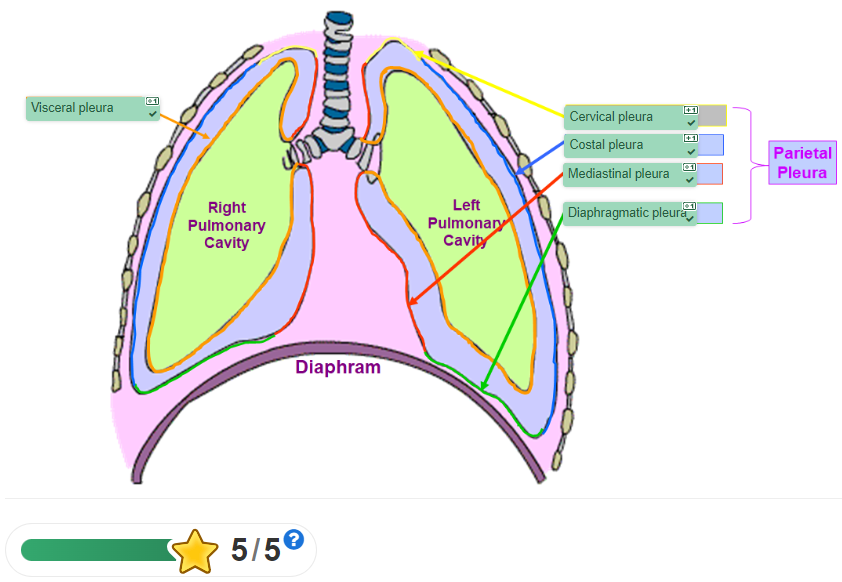
what is the pleura?
The lungs are enclosed by a thin membrane known as the pleura. The pleura also lines the walls of the thoracic cavity.
what is the parietal and visceral pleura?
The pleura that is associated with the walls of the cavity is known as parietal pleura. The parietal pleura lines the pulmonary cavities, and is adherent to the thoracic wall, the mediastinum and the diaphragm.
The pleura that is associated with the lungs is known as visceral pleura. The visceral pleura covers the lungs and is adherent to all its surfaces, including the horizontal and oblique fissures; it cannot be separated from the lungs.
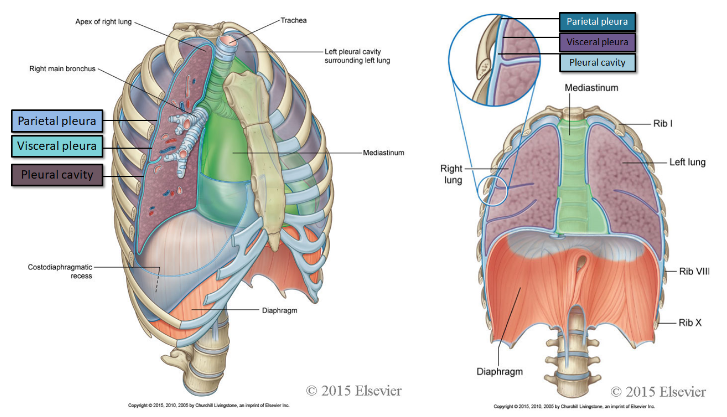
what is the pleural cavity?
The space between the two layers of pleura is a potential space known as the pleural cavity.
what does it mean that the pleura is a serous membrane?
This means it produces serous fluid, a lubricating fluid that is present in the potential space between the visceral and parietal layers of pleura.
what is the function of the pleura and serous fluid?
The function of the pleura and serous fluid is to allow smooth movement of the lungs as they expand and collapse throughout respiration. The fluid also provides the surface tension that keeps the surface of the lung in contact with the thoracic wall; consequently the lung expands and fills with air when the chest expands and the diaphragm flattens.
what four parts can the parietal pleura be divided into?
Costal pleura covers the internal surfaces of the thoracic wall.
Mediastinal pleura covers the lateral aspects of the mediastinum.
Diaphragmatic pleura covers the superior aspect of the diaphragm on each side of the mediastinum.
Cervical pleura extends through the superior thoracic aperture forming domed pleura over the apex of the lung (also known as dome of pleura or pleural cupola)
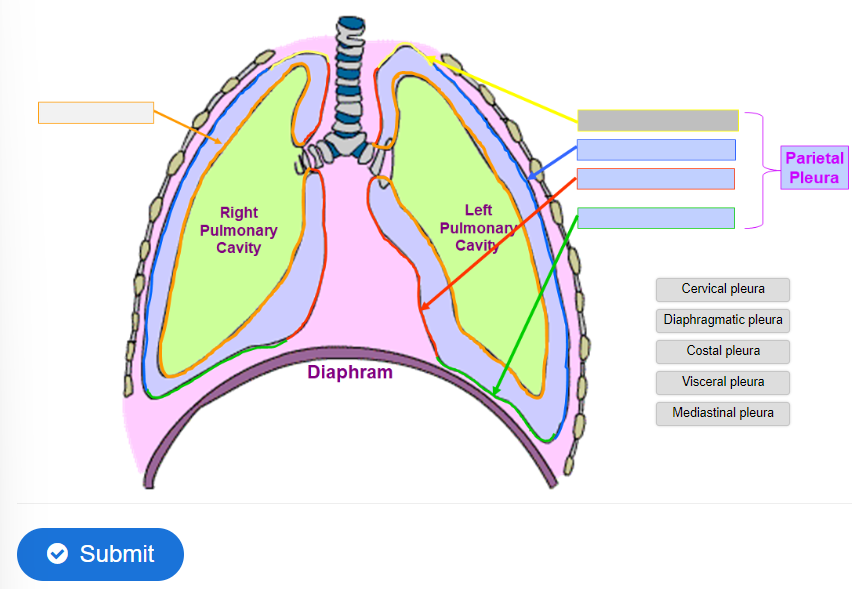
label the diagram
pleural cavity extends further than the lungs
Superiorly - pleural cavity projects as much as 3–4 cm above the first costal cartilage
Anteriorly - left and right pleural cavities approach each other posterior to the sternum. However, more inferiorly, the parietal pleura does not come as close to the midline on the left side as it does on the right because the middle mediastinum, containing the pericardium and heart, bulges to the left.
Inferiorly - the costal pleura extends to rib 8 in the midclavicular line and to rib 10 in the midaxillary line. More posteriorly, the inferior margin courses horizontally, crossing ribs 11 and 12 to reach vertebra T12. From the midclavicular line to the vertebral column, the inferior boundary of the pleura can be approximated by a line that runs between rib 8, rib 10, and vertebra T12.
what causes a collapsed lung?
If a significant amount of air or fluid enters the pleural cavity, the surface tension adhering the visceral and parietal pleura is broken and pleural cavity becomes a real space (no longer a potential space).
what is a pneumothorax?
A common cause of this is a puncture wound to the thorax (e.g. a gunshot wound, stabbing injury). As a result air rushes into the pleural cavity.
what is called hydrothorax?
Accumulation of fluid in the pleural cavity may result from pleural effusion (escape of fluid into the pleural cavity).
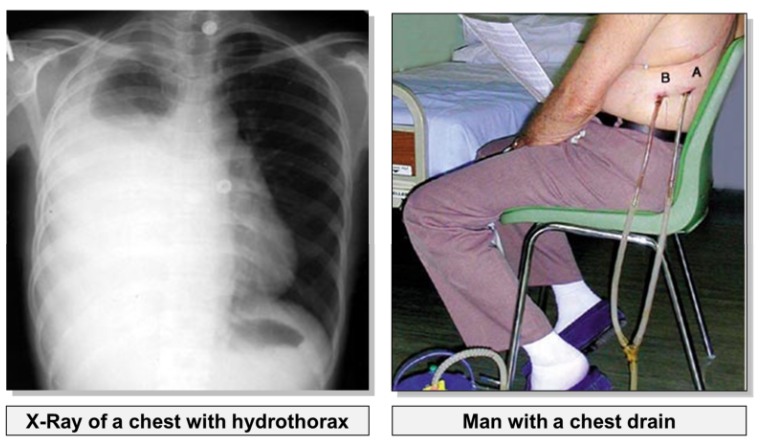
what is haemothorax?
In a chest injury, blood may also enter the pleural cavity. Haemothorax is usually a result of injury to a major intercostal vessel (usually by a fractured rib), rather than laceration to the lung.
In order to re-inflate the lung, fluid must be drained from the pleural cavity using a chest drain.
what is the function of the following bones:
sternum, 12 pairs of ribs and their costal cartilages, and the 12 thoracic vertebra (T1 - T12).
Provide attachment points for the muscles of respiration
Move to facilitate breathing
Provide protection for the vulnerable organs within the thorax
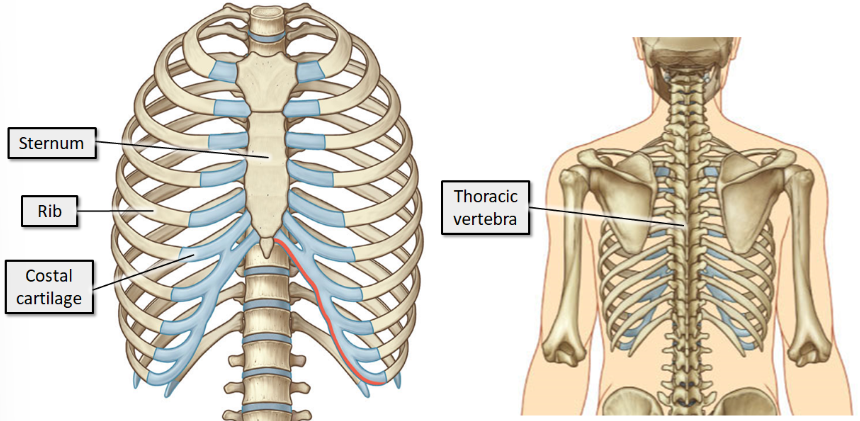
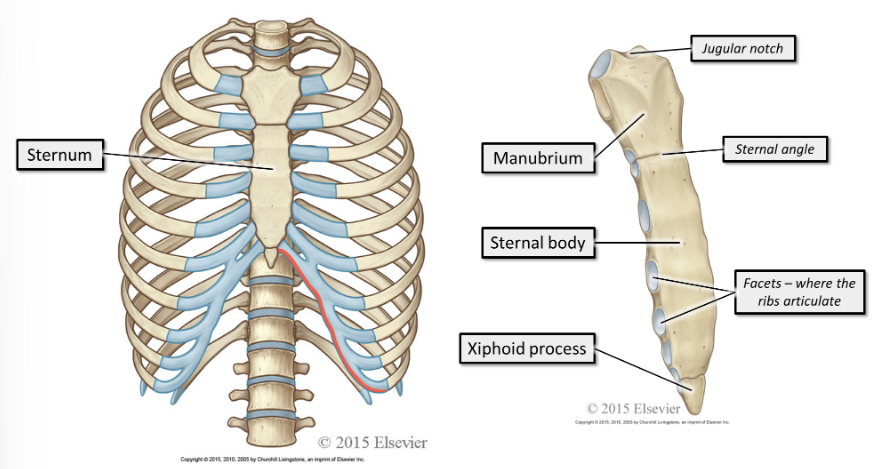
where does the sternum sit and what is it made up of?
The sternum sits anteriorly. It consists of the manubrium, sternal body and xiphoid process.
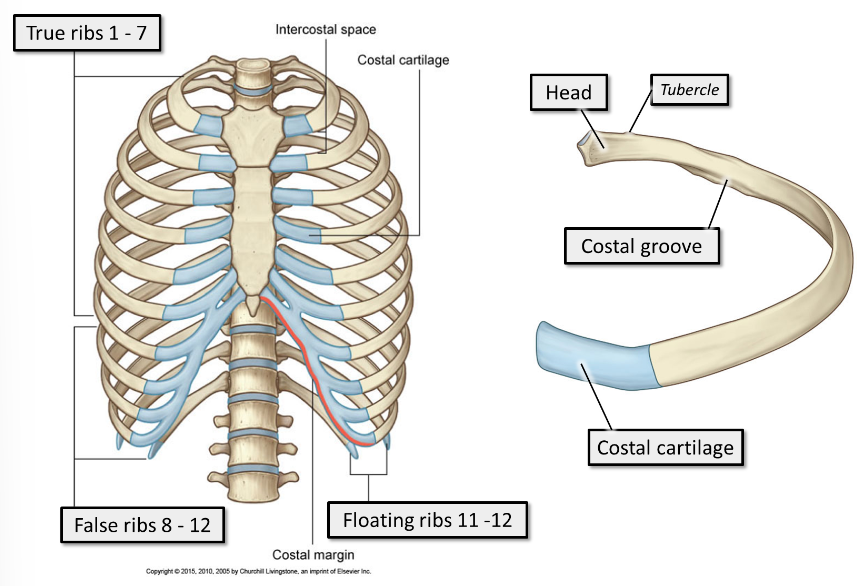
where do the ribs sit?
All the ribs articulate posteriorly with the thoracic vertebra. The end of the rib that articulates with the vertebra is the head of the rib.
Anteriorly, the ribs end in costal cartilage
what are the different types of ribs?
Ribs 1 - 7 are true ribs. True ribs articulate directly with the sternum anteriorly, via short costal cartilages. Every true rib has its own costal cartilage
Ribs 8 - 12 are false ribs. False ribs articulate indirectly with the sternum anteriorly, via long, shared costal cartilages, or do not articulate with the sternum at all.
Ribs 11 - 12 are floating ribs. They do not articulate with the sternum anteriorly, and are shorter and pointier than the other ribs.
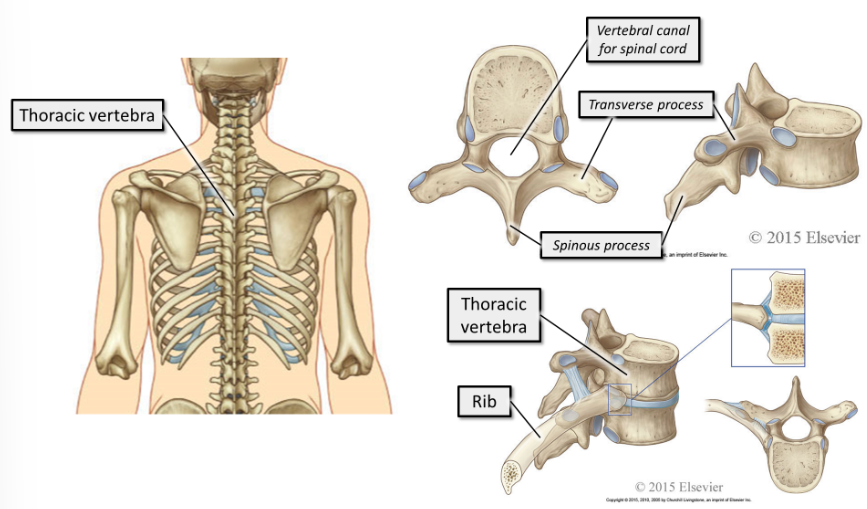
what is the thoracic vertebra?
The 12 thoracic vertebra make up the posterior element of the thoracic cage. They articulate with the ribs and with each other.
what are characteristics of the diaphragm?
The diaphragm is a thin, musculotendinous, dome-shaped sheet of muscle that separates the thorax from the abdomen.
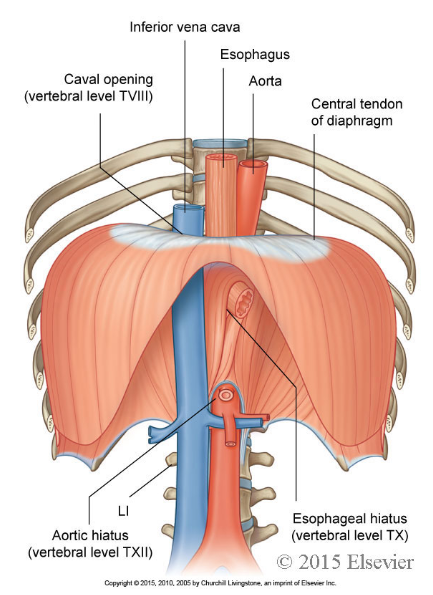
what is the tendon that the diaphragm has called?
It has a large, flat central tendon.
what is the diaphragm attached to?
The diaphragm is attached to the lower ribs and vertebral column.
what nerves control the diaphragm?
It is innervated by the right and left phrenic nerves, which have their origins at the third to fifth cervical spinal nerves (C3-C5).
"C3, C4, C5 keeps the diaphragm alive"!
where does the diaphragm sit in relation to T9 and T12?
While at rest, its highest point it is level with T9, inferiorly it is attached to the body wall level with T12.
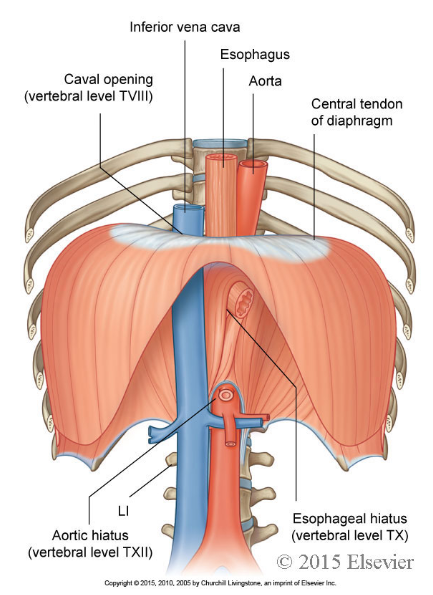
what are the 3 major structures of the diaphragm?
The aorta
The inferior vena cava
The oesophagus
where does blood enter and leave the diaphragm?
Blood supply of the diaphragm originates from the intercostal arteries
Venous drainage is to the inferior vena cava.
how much does the diaphragm move during deep and quiet breathing
During quiet breathing, the diaphragm contracts and flattens, the apex moves inferiorly by 1-2cm.
During deep breathing the diaphragm can move inferiorly up to 10 cm.
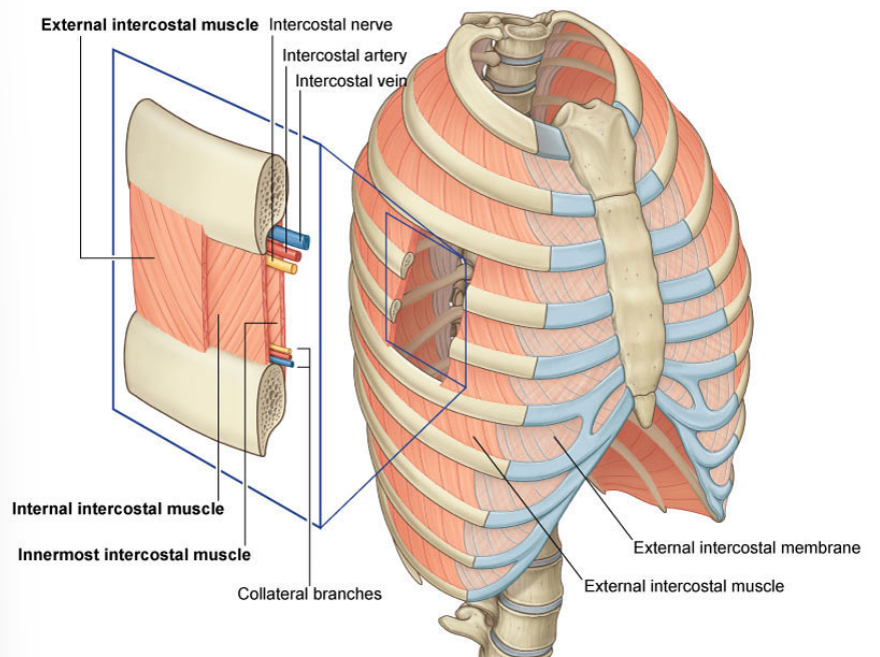
where are the external intercostal muscles in relation to the internal intercostals?
The external intercostals are superficial to the internal intercostals. The innermost intercostals are the deepest of the three.
how many sets of each type of intercostal muscles are there?
There are 11 sets of each.
where does the blood supply to the intercostal muscles come from?
Their blood supply comes from the intercostal arteries
Venous drainage is via the intercostal veins. They are innervated by the intercostal nerves.
what is the intercostal neurovascular bundle?
The intercostal artery, vein and nerve travel together in the intercostal space. They lie at the lower border of each rib.
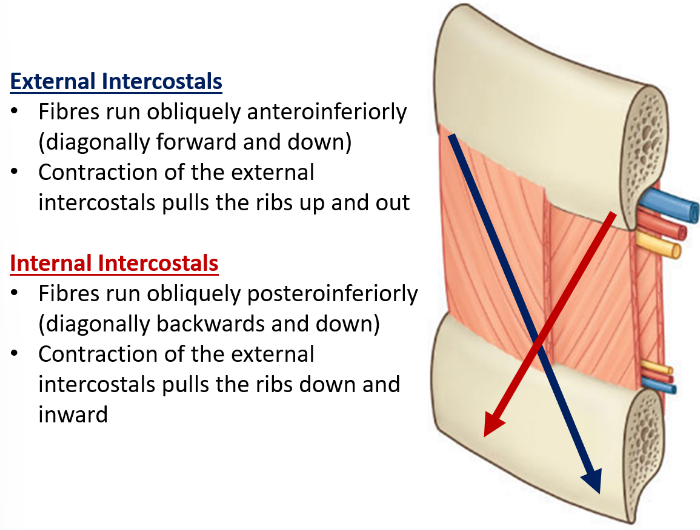
in which direction do external and internal intercostals sit?
what does their contraction cause?
where do the external intercostal muscles extend from and to?
they extend from the lower border of the rib above, to the upper border of the rib below. They run around the wall of the thorax, from the tubercles each rib posteriorly, to the cartilages of the ribs anteriorly. They end anteriorly in thin membranes, the anterior (external) intercostal membranes, which continue forward to the sternum.
where do the internal intercostal muscles extend from and to?
The internal intercostal muscles run between the most inferior lateral edge of the costal grooves of the ribs above, to the superior margins of the ribs below. They begin anteriorly, at the sternum in the spaces between the cartilages of the true ribs (ribs 1-7) and at the most anterior edge of the cartilages of the false ribs (8-12). They extend downward as far as the angles of the ribs, where they continue to the vertebral column as thin membranes called the posterior (internal) intercostal membranes.
where do the innermost intercostal muscles extend from and to?
The innermost intercostal muscles are incomplete and variable. They pass from rib to rib deep to the internal intercostals. Their fibres run in the same direction as the internal intercostals. The innermost intercostal muscles are separated from the internal intercostal muscles by the bundle of intercostal blood vessel and nerves.
what muscles can assist due to their attachment to the ribs?
sternocleidomastoid, pectoralis minor and the scalene muscles
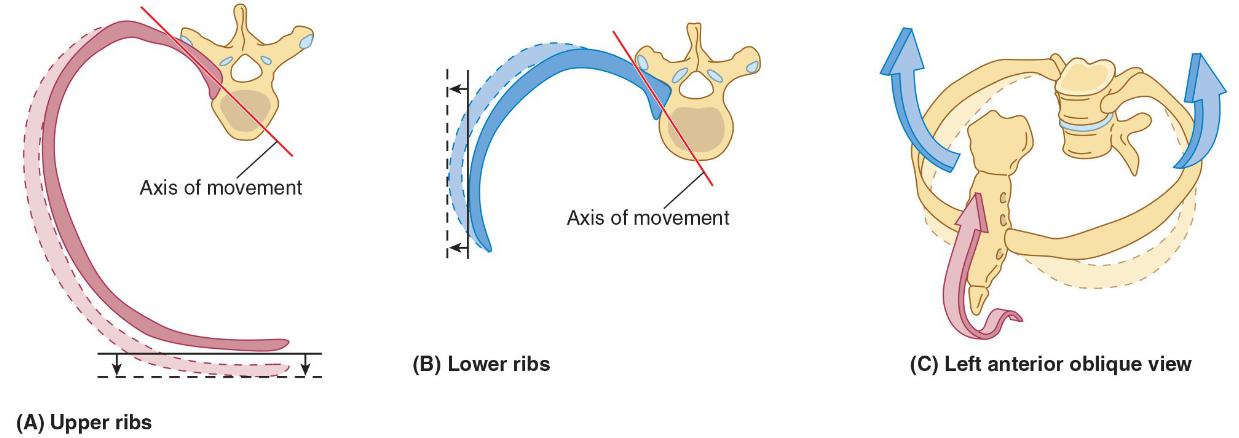
during breathing, in what two planes do the ribs move in?
forwards and backwards (anteroposterior) and laterally
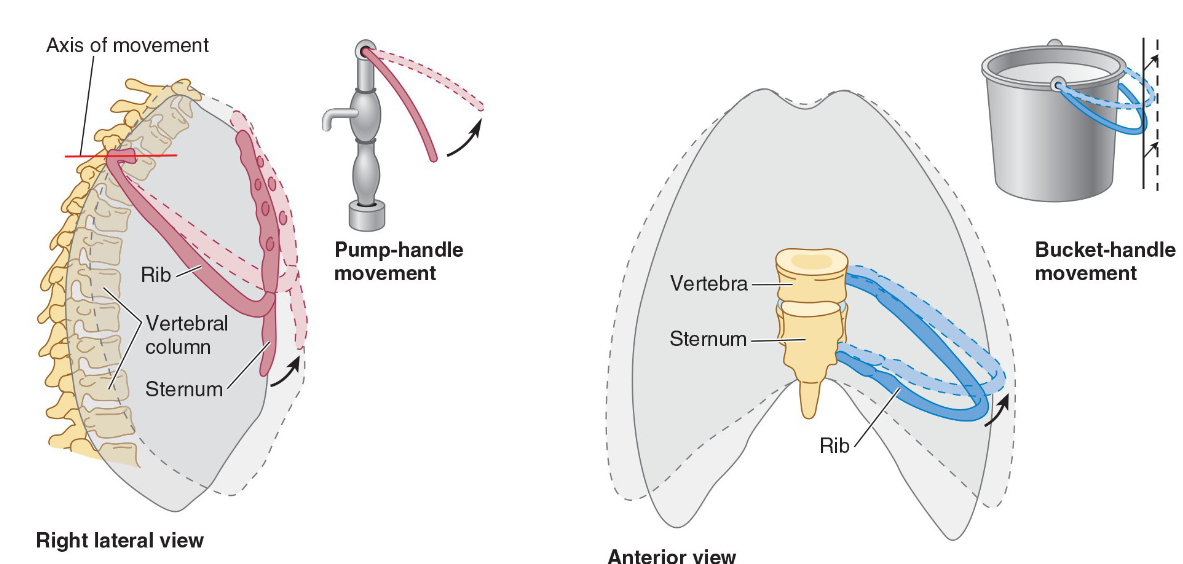
what is the anteroposterior motion and lateral movement?
The anteroposterior motion is often compared to a pump handle action where the ribs are the handle of the pump.
The lateral movement is often compared to a bucket handle where the ribs are a handle pivoting at the spine and sternum.
what two tree-like structures is each lung composed of?
vascular tree and the airway tree,
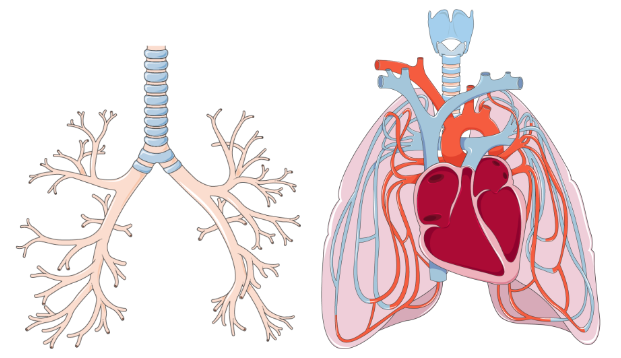
what are the two tree-like structures is each lung?
The vascular tree is composed of the arteries, veins and capillaries which conduct poorly oxygenated blood to the lungs and returns highly oxygenated blood to the heart.
The airway tree consists of air-filled branching tubes, originating from the trachea, which conduct ‘new’ atmospheric air to the gas exchange surfaces and return ‘used’ air to the environment.
what is a pulmonary oedema?
Pulmonary oedema is a build-up of fluid in the interstitial space in the lungs. This increases the diffusion distance of gases between blood and the alveoli
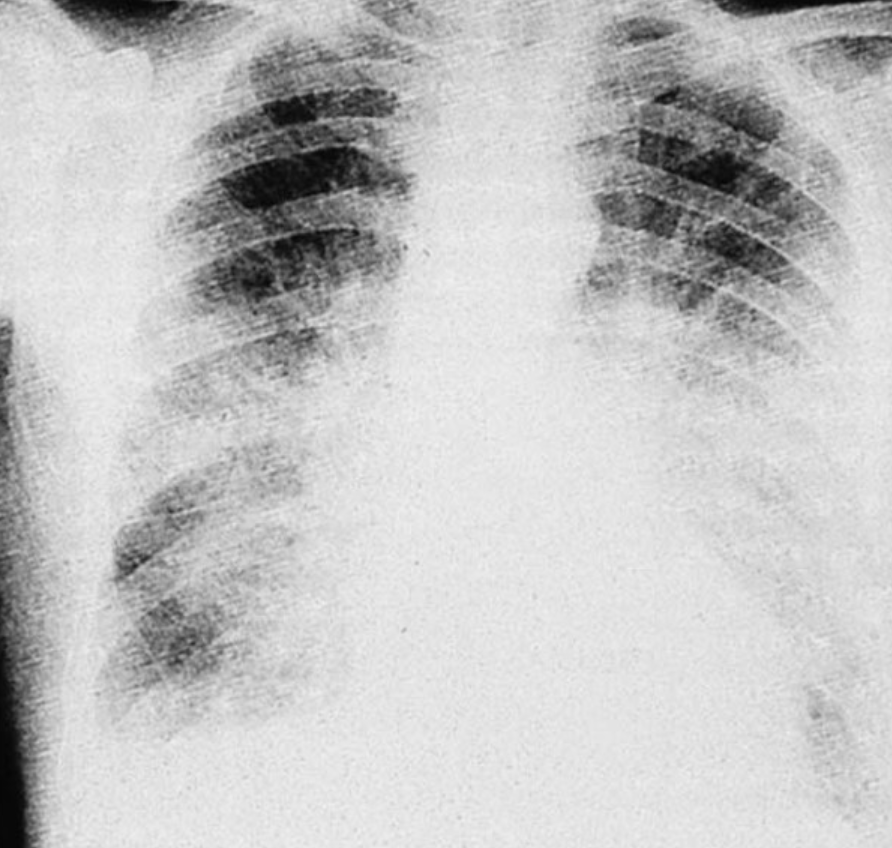
is a pulmonary oedema a primary or secondary condition?
Pulmonary oedema is often secondary to another condition such as left heart failure, renal failure, pneumonia or cirrhosis of the liver.
what will pulmonary oedema eventually lead to?
The increase diffusion distance leads to hypoxia as the blood loads with less oxygen. Carbon dioxide levels in the blood, however, may be normal as carbon dioxide is more soluble than oxygen.
what are early and late symptoms of a pulmonary oedema?
Early symptoms include shortness of breath, cough and various disruptions to the rate and rhythm of breathing. Later symptoms go on to include cyanosis and a cough with a foaming red sputum.
what treatments are available to a pulmonary oedema?
Initial treatment aims to treat the hypoxia using 100% oxygen while later treatment goes on to address the underlying cause.
what is the trachea?
The trachea is the single widest of the conducting airways, however it has the smallest total cross-sectional area and therefore is responsible for most of the airway resistance.
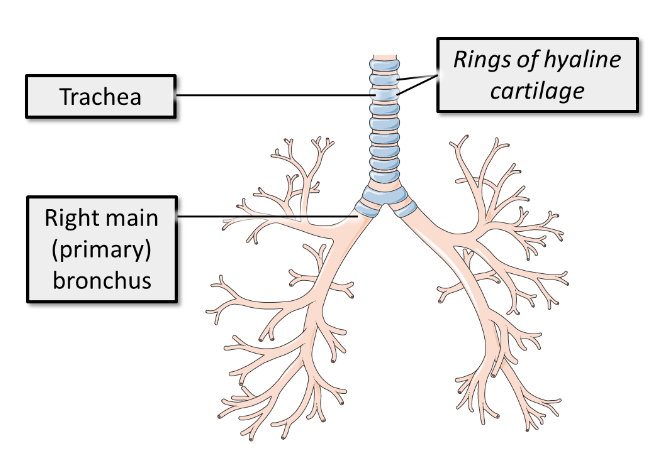
what does the trachea contain to prevent it from collapsing?
To prevent collapse on inspiration, it is surrounded and supported by rings of hyaline cartilage which can be easily felt at the base of the neck.
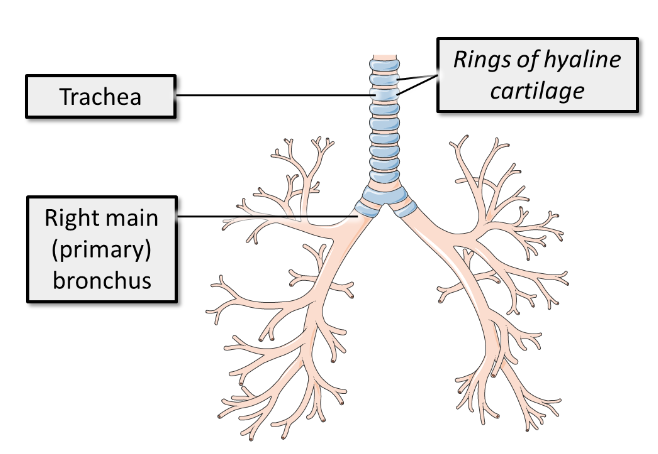
what does the trachea split into and what what location is this split?
The trachea bifurcates into two primary or main bronchi which enter the lung. The bifurcation of the trachea occurs at vertebral level T4.
what are important landmarks of the vertebral level T4?
It is the level of the sternal angle (angle between the manubrium and body of the sternum)
It is the level where the trachea bifurcate into the two main bronchi
It is the level of the arch of the aorta
It is where the second rib articulates with the sternum
what are the differences between the right and left main bronchus?
The right main bronchus is wider and shorter and runs more vertically than the left main bronchus to enter the hilum of the lung
The left main bronchus is oriented more horizontally, and runs inferior to the arch of the aorta and anterior to the esophagus and thoracic aorta, to reach the hilum of the lung.
what does the main bronchi divide into and what do they contain to support against collapsing?
The main bronchi first divide into secondary/lobar bronchi, one per lobe of each lung, and then these divide into tertiary/segmental bronchi. Each tertiary bronchus supplies a different segment of the lung.
These conducting tubes are also supported by rings of cartilage.
what makes up the conducting zone of the lower respiratory system?
The first 17 generations of airway (i.e. the trachea and 16 successive airway branches) form the conducting zone of the lower respiratory system.
at what number division do the bronchi change to bronchioles?
At about the 12th division of the bronchi, bronchioles can be found.
describe the walls of the bronchioles
These are small, collapsible passageways with smooth muscle walls.
how many more times do the bronchioles divide until the respiratory bronchioles appear?
The bronchioles then continue to further branch (up to 11 times) until the respiratory bronchioles begin to appear.
what are respiratory bronchioles?
Respiratory bronchioles are the transition between the conducting airways and the gas exchanging tissues of the lung. These terminate at the alveolar ducts which lead to the alveoli.
what is the respiratory zone of the lower respiratory system?
The structures from the respiratory bronchioles to the alveoli form the respiratory zone of the lower respiratory system.
what does each tertiary bronchus supply?
Each tertiary bronchus supplies a different bronchopulmonary segment of the lung.
what are lung lobes?
Alveoli are arranged in lung lobules which are a cluster of alveoli surrounded by elastic fibres and a network of capillaries.
A lung lobule is a cluster of alveoli supplied by a single respiratory bronchiole, surrounded by the connective tissue of the lung:
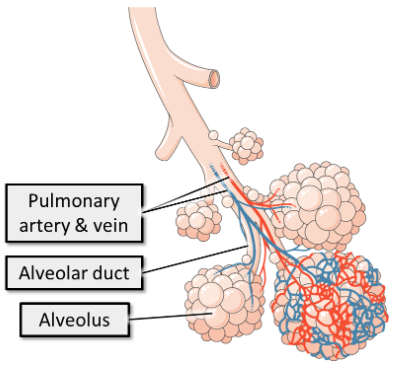
what is the apical surface of the alveoli covered in?
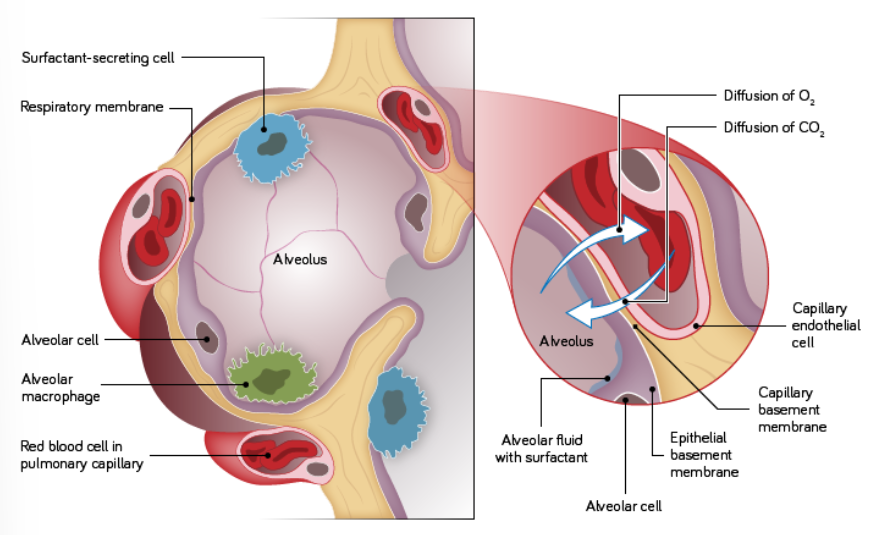
The apical surface is covered in a surfactant into which gases dissolve to aid their diffusion.
what is emphysema?
Emphysema is a condition largely associated with smoking. It is caused by gradual damage to the alveoli, usually by irritants or infection, which makes them loose their natural elasticity.
This means that the lungs are unable to expel all the air on expiration and leaves them feeling continually over inflated and the patient struggles to force air in and out of their lungs.
what does reduced ventilation in emphysema eventually cause?
The reduced ventilation, in turn, leads to a state of chronic hypoxia causing fatigue and weight loss. It may only start off as breathlessness however it may lead to the patient being housebound and reliant on oxygen supplies.
what is chronic obstructive pulmonary disease (COPD)?
This disease is sometimes complicated by combination with chronic bronchitis, where the lungs are unable to clear mucus (due to damage to the respiratory epithelium, often by smoking) which becomes infected.
This combination is called Chronic Obstructive Pulmonary Disease (COPD).
what are the treatment options and consequences of emphysema?
There is no cure for emphysema, however early symptoms can be controlled with bronchodilators. If COPD advances too far, patients may end up needing mechanical help to breath.
what is the current theory about the cause of asthma?
The theory states that there are both inducers and triggers. The inducer is the original antigen that elicited an immune response and act as an allergen. On exposure to this antigen the immune system gives an inappropriate response which results in an over-reaction to an otherwise harmless antigen causing swelling of the airways and recruitment of eosinophils. As a result of the increased number of eosinophils, the patient is ‘sensitised’.
what is status asthmaticus?
Status asthmaticus (an acute asthma attack) is then later triggered by an irritant. In a non-asthmatic, the irritant would not cause the same degree of reaction, however in an asthmatic the airways are ‘hypersensitive’. The reaction causes varying degrees of bronchoconstriction.
what are treatment options for acute asthma attacks?
During treatment of the acute asthma attack bronchodilators such as salbutamol (ventolin) are used. Prophylactic inhaled steroids such as beclomethasone dipropionate (BDP) helps reduce long-term airway damage and is currently the first line and preferred treatment in conjunction with an inhaled bronchodilator for acute attacks.
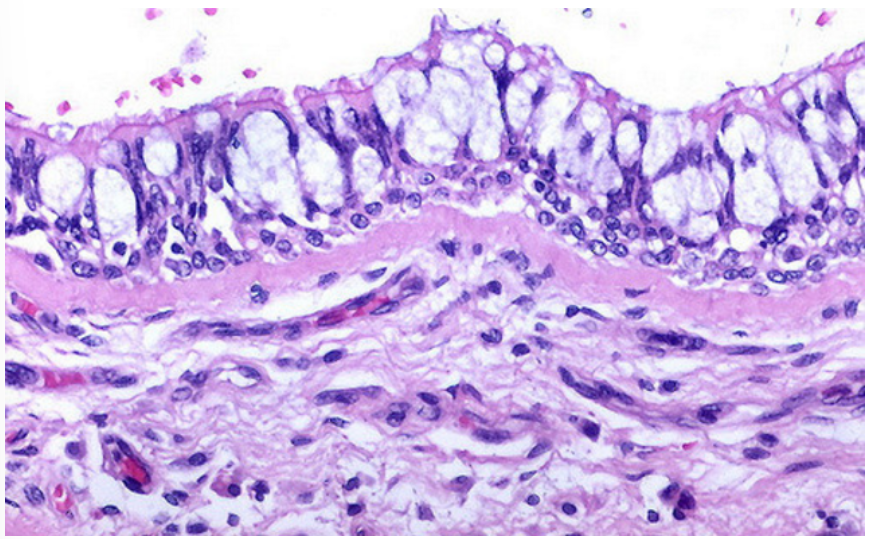
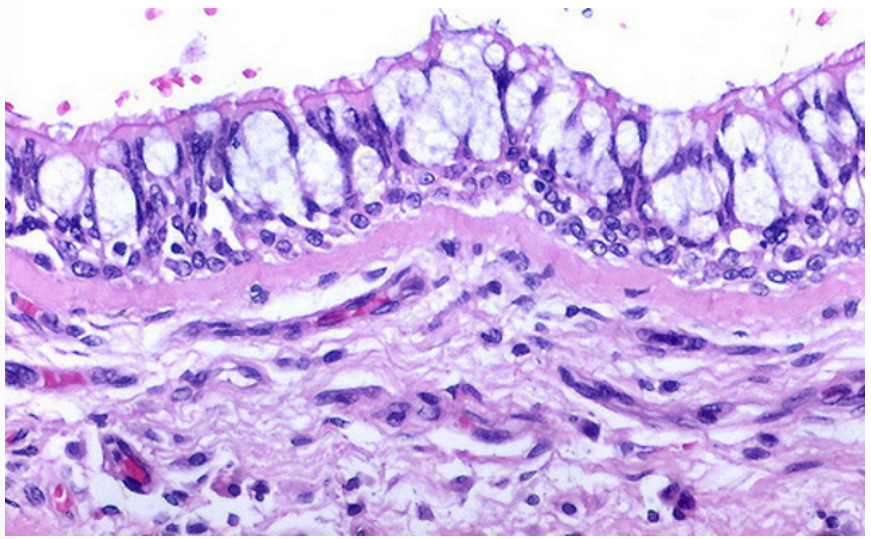
what are some characteristics of the upper respiratory tract?
The architecture of the nasal cavity and sinuses is designed with a large surface area to warm and moisten inhaled air.
The cavities are lined with pseudostratified columnar epithelium.
The columnar cells have numerous cilia on their surface.
The epithelium also contains mucous secreting goblet cells.
This type of epithelium (pseudostratified columnar, with cilia and goblet cells) is present throughout the upper respiratory system and is known as respiratory type epithelium.
The walls of the trachea and large bronchi are supported by rings of hyaline cartilage and have incomplete smooth muscle support.
As the airways become smaller, cartilage rings are replaced with cartilage plates (in the intrapulmonary bronchi) and eventually smooth muscle becomes the major component of support.
what are some characteristics of the lower respiratory tract?
The bronchial tree is lined with respiratory type epithelium in the larger bronchi.
In the more peripheral branches the epithelium becomes thinner though cells are still ciliated columnar with goblet cells.
The bronchioles are lined by simple (not pseudostratified) ciliated columnar epithelium and goblet cells are sparse.
Bronchioles are distal airways located between the cartilage-walled bronchi and the point where ciliated epithelium ceases.
The distal respiratory tract is the site of gaseous exchange.
The most proximal components are the respiratory bronchioles which are lined with cuboidal ciliated epithelium.
The alveolar ducts (passageways formed mostly from the openings to alveoli) are lined with flattened epithelium.
what types of alveoli are there?
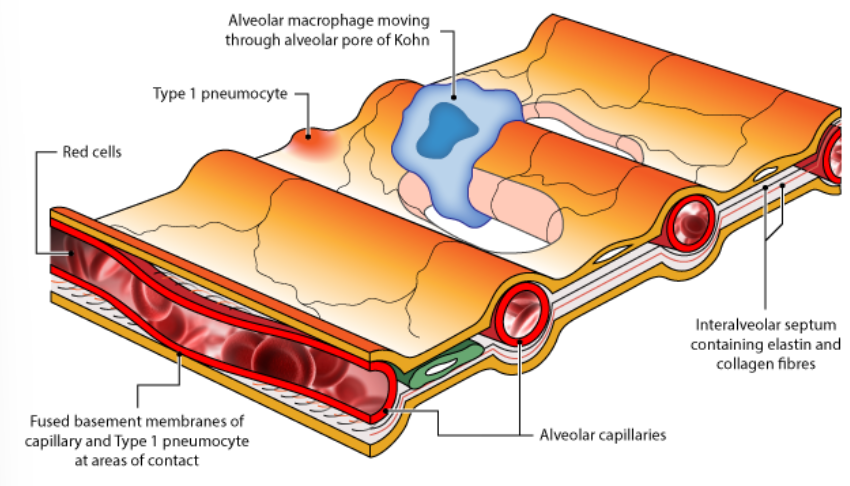
The alveoli consist of Type I and II pneumocytes that lie on the basement membrane and also of alveolar macrophages.
what does the alveolar wall contain? what does this do?
elastin
Elastin allows the lungs to stretch to accommodate inspired air, it recoils to its original shape, allowing air to be expelled and it acts as a support, attaching airways with no cartilage firmly to the connective tissue of the lung.
what are Type I Pneumocytes?
Type I pneumocytes are very thin cells which allow gaseous diffusion. They represent about 40% of the number of alveolar cells but 90% of the surface area lining the alveoli.
They are flattened cells with flattened nuclei and are joined together by tight junctions.
They have few organelles and provide a very thin covering over the basement membrane; the thinness of which contributes to the efficiency of gaseous exchange.
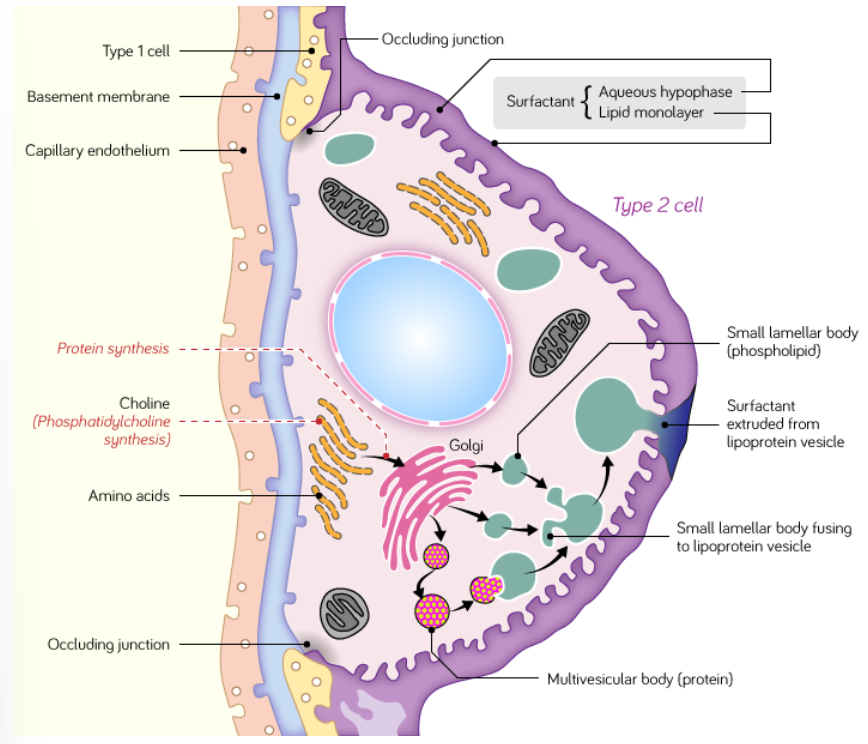
what are Type II Pneumocytes?
Type II pneumocytes secrete surfactant. They represent 60% of the number of alveolar cells but only 5-10% of the surface area lining the alveoli.
These cells are rounded in shape and contain numerous mitochondria.
Surfactant acts as a detergent, reducing alveolar surface tension, preventing collapse of the alveoli during expiration and facilitating inspirational expansion.
Some type II pneumocytes act as precursor stem cells for type I pneumocytes.
what are alveolar macrophages?
Alveolar macrophages ‘patrol’ the alveolar air spaces and the interalveolar septa (the walls of the alveoli) and can pass freely between the two.
They phagocytose inhaled debris and pathogens.
Following phagocytosis they may pass into the lymphatic system or adhere to mucous-coated ciliated epithelium and continue up the mucociliary escalator to the trachea where they are cleared by coughing.