Cleft Types and Classifications
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
Unilateral Incomplete Cleft Lip
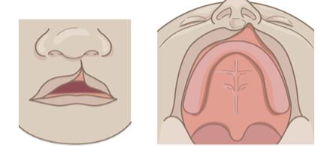
Unilateral Complete Cleft of the Primary Palate
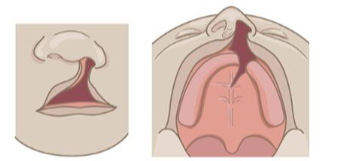
Bilateral Complete Cleft of the Primary Palate
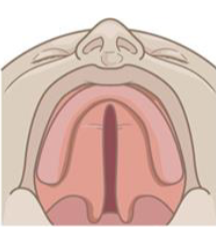
Incomplete Cleft Palate (secondary palate)
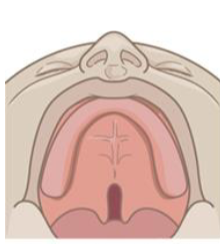
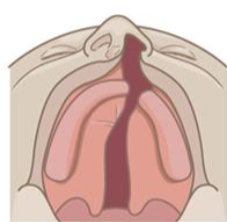
Complete Cleft Palate (secondary palate)
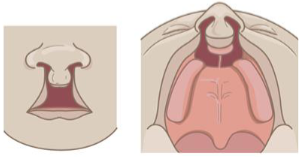
Unilateral Complete Cleft Lip and Palate (primary and secondary palate)
Bilateral Complete Cleft Lip and Palate (primary and secondary palate)
Wide bell-shaped cleft palate
A cleft palate where the opening is broad and flares outward, resembling a bell shape
common in Pierre Robin sequence
Caused by:
Micrognathia (small mandible)
Tongue falls backward (glossoptosis)
Tongue blocks palatal fusion during development → cleft palate forms
Microform Cleft Lip
mildest form of cleft lip
it occurs when the lip tissue fuses almost completely in the womb, leaving behind only a subtle notch, groove, or scar-like mark on the upper lip rather than an open gap

Prolabium
the central segment of the upper lip in a bilateral cleft lip.
occurs because philtrum columns did not fuse

Complete Cleft
extends to incisive foramen
primary palate: from the lip
secondary palate: from soft palate
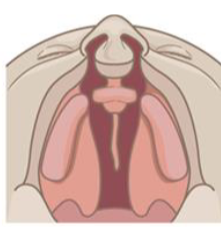
Submucous Cleft triad of characteristics
1. Bifid or hypoplastic (small or underdeveloped) uvula
2. Zona pellucida: Thin, bluish area in the middle of the velum
3. Notch in the hard palate where the posterior nasal spine should be, if the submucous cleft extends into the hard palate
Submucous Cleft: Embryology
• Fusion of the oral surface of the secondary palate occurs ahead of fusion of the nasal surface
• Oral surface of the secondary palate can be completely formed, while the nasal surface (or just the uvula) is incomplete
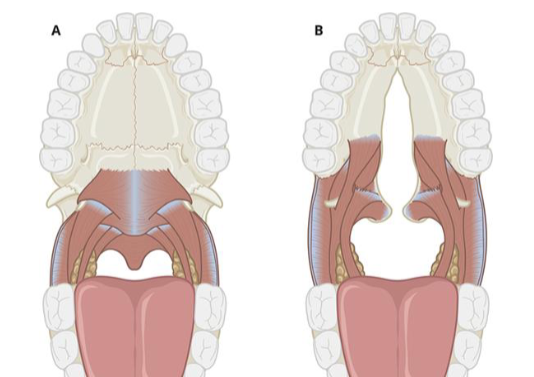
Submucous Cleft Anatomy
• Muscles of a submucous cleft are often affected in the same way as with a complete cleft palate
• Levator muscles insert on the posterior border of the hard palate rather than in the middle of the velum (called “muscles of Veau”)
Overt vs. Occult Cleft
• Overt (plainly or readily apparent): Visible from the oral surface
• Occult (hidden): Normal on the oral surface; abnormal within
Simonart’s Band
a thin, soft tissue bridge that connects the borders of a cleft lip, typically found at the base of the nostril or along the alveolar ridge.

Facial Clefts types
midline: through middle of face
oblique: diagonal across face
Amniotic Bands
one cause of facial clefts
• Inner membrane of the amniotic sac ruptures (for unknown reasons)
• Causes fibrous and sticky amnion tissue (bands) to float in the waters of the uterus
• Bands can entangle/attach to a body part, reducing blood supply
• Can cause “natural” amputation of digits or limbs before birth
• Can cause facial or oral deformations
Cleft of Primary Palate- Structure Impact
•Cleft lip and orbicularis oris
•Wide, flat nose with spreading nasal ala
•Short columella
•Abnormal dentition
Cleft of Primary Palate- Function Impact
•Specific articulation errors
•Resonance affected
Cleft of Secondary Palate- Structure Impact
Abnormal insertion of the levator velar muscles (called the “cleft muscles of Veau”)
Abnormalities in nasal septum
Cleft of Secondary Palate- Function Impact
Velopharyngeal insufficiency (affecting speech and/or resonance)
Feeding problems and nasal regurgitation
Eustachian tube malfunction
Submucous Cleft- Structure Impact
• Depends on the extent
• May include a minor abnormality of the uvula or a defect of the nasal surface of the velum and hard palate
• May include an altered insertion of the levator velar muscles (cleft muscles of Veau)
Submucous Cleft- Function Impact
• Velopharyngeal insufficiency (affecting speech and/or resonance)
• Feeding problems and nasal regurgitation
• Eustachian tube malfunction
Primary Palate Formation
7 weeks gestation
moves forward from incisive foramen
right side of lip closes first (left-sided cleft more common)
Secondary Palate Formation
forms at 9 weeks gestation
moves backward from incisive foramen