ES380-Chapter 9: Cardiorespiratory responses to acute exercise
1/61
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
62 Terms
what is the main goal of the CV with exercise?
increase bloodflow to working muscle to meet O2 demand
Heart rate increase will affect what 5 other functions?
Stroke volume
cardiac output=Q
blood pressure
blood flow
blood
what is the equation for the fick principle that quantifies VO2 uptake?
VO2=Q x (a-v)O2difference
O2 use depends on what 2 factors?
Tissue bloodflow
O2 extraction
what is the mean BPM
75
what 3 things affects the BPM
Vagal tone(PNS)
Temperature
Altitude
Big point: what is the anticipatory response?
Increase HR above RHR just before exercise
Big point: what are the 2 steps that affect the anticipatory response?
1. withdrawal of vagal tone(PNS)
2. increased SNS causing increased NE and Epi
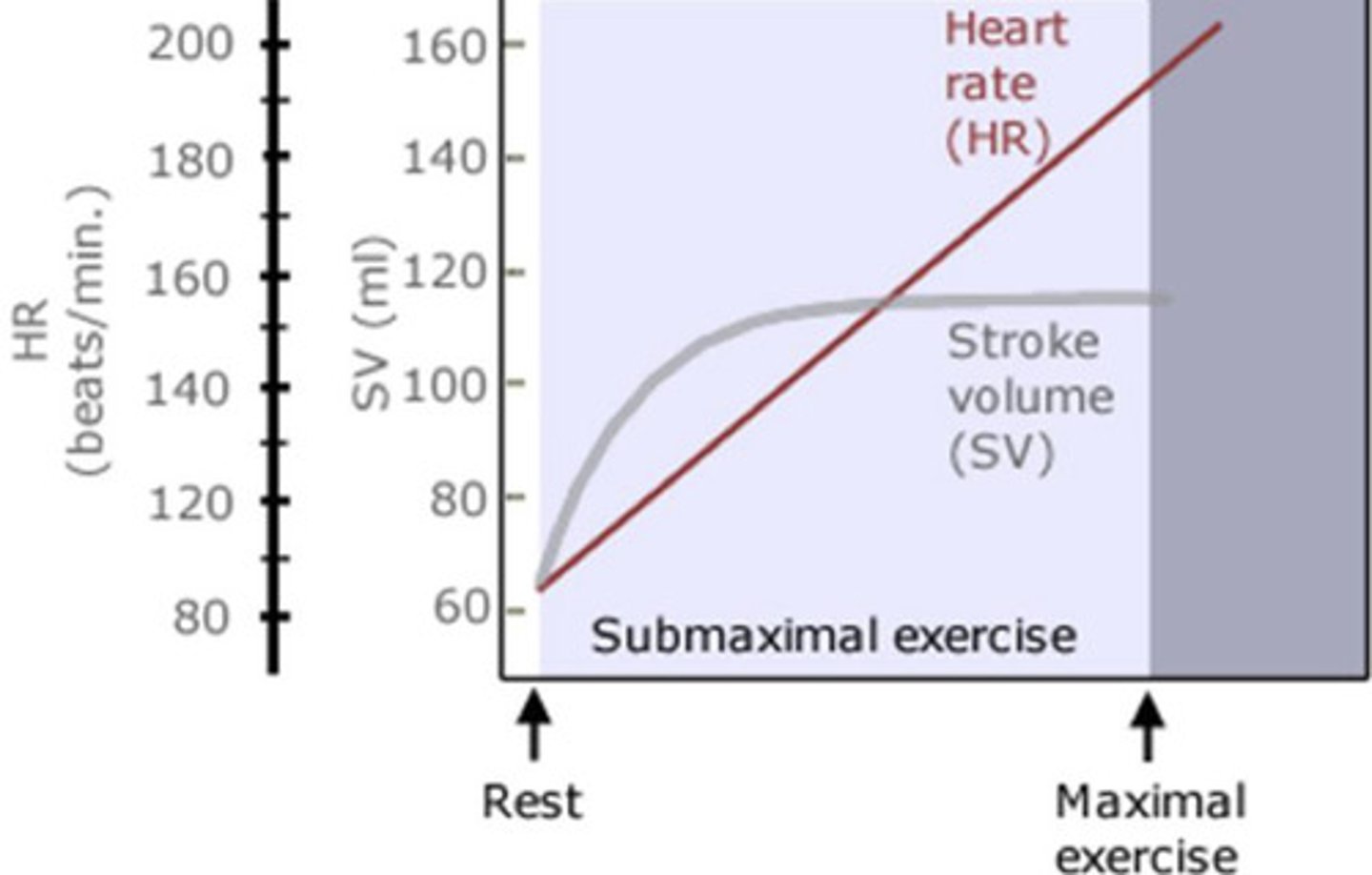
how does HR increase with exercise intensity?
linearly
what are the 4 steps of increasing HR in response to exercise intensity?
1. decreased PNS(until HR of 100)
2. increased SNS(over HR of 100)
3. group III/IV muscle afferents
4. SNS stimuli Epi/NE secretion
True/false: maximum HR is not reproducible and not good for exercise prescription
FALSE
HRmax is highly reproducible and thus very good for exercise prescription
what is the timeframe for the physiologic adjustment period?
2-3 mins
what is the main activity that maintains HR after the adjustment period and what functions control that?
Sympathetic activity
-command center + muscle metaboreceptors
how much does HR have to increase above VO2max to increase CO(in a percent)?
above 50% of the VO2 max
why does SV increase during low to moderate intensity?
what 3 mechanisms cause this?
compensation of mobilization of venous blood
-oneway valves, muscle pump, respiratory pump
training status and exercise mode dependent
what are the 5 mechanisms that increase SV during exercise?
-Frank-starling mechanism
-Increased SNS/ circulating NE or Epi
-Anrep and bowditch effects
-decreased afterload
-torsional contraction of the ventricles
4 effects of frank-starling mechanism during exercise?
increased EDV causes Increased ventricular stretch causes increased Ca2+ which causes increased contractility
effects of SNS activity on SV?
increased SNS-> increased NE/Epi-> increased Ca2+-> contractility
BIG POINT: what is the biggest cause for increased SV during low to intermediate work and what mechanisms cause that(think about cause and effect and work backwards)?
VO2 max increased SV b/c EDV increases caused by increased preload from frank starling mechanism
BIG POINT: what is the biggest cause for increased SV during intermediate to peak work and what mechanisms cause that(think about cause and effect and work backwards)?
VO2 max, increased SV b/c decreased ESV from SNS/NE, ANREP and bowditch effects, as well as torsional contraction
BIG POINT: what is the biggest determining effect of VO2 max?(think about what could we increase to have the most prevalent effect)
increases in SVmax
what are 7 other factors that can affect VO2 max?
blood volume, cardiac size/mass/compliance, muscle BF, capillary density, mitochondrial content
why does cardiac output have the greatest rate of change(rise the fastest) during the beginning of exercise?(think about Q=HR x SV)
fast increase in SV to accommodate
memorize: what is the resting Q(CO)?
5 L/Min
memorize: what is the untrained Qmax?
20-25 L/min
list the 5 steps of how Plasma volume(PV) increases VO2max?
Increased PV->Increased VR-> Increased EDV->Increased Qmax-> Increased VO2max
if larger individuals have more blood volume, how does this affect their plasma volume and left ventricles?
Increased PV
Increased Left Ventricles
if the MAP is increasing, what must happen to TPR during exercise to achieve steady state? [MAP = (HRxSV)xTPR, be careful and consider the variables]
decrease until steady state
does an decreased TPR aid in increasing muscle blood flow?
YES
allows the heart to beat faster and push more volume out since there is decreased pressure against it
what factor of MAP has the biggest effect on BP during resistance training?(MAP=1/3 SBP x 2/3 DBP)
2/3 DBP
massive driving force for increased bP
how does the valsalva maneuver increase BP?
prolonged use causes decreased preload, decreased CO and decreased MAP which can lead to syncope
what are the 3 biggest differences between CV adjustments to exercise for lower body exercise(LE) vs upper body exercise(UE)
1. VO2max is 20-30% lower during UE
2. HRmax and Vemax are lower during UE
3. during submax, UE elicits higher relativbe BP, HR, RPE, Ve, and VO2
what are the 5 mechanisms for differences between CV adjustments to exercise for lower body exercise(LE) vs upper body exercise(UE)
1. smaller muscle mass=less VR and SV
2. increased feedforward stimulation to CCC(cardiac command center
3. increased feedback to medulla from peripheral receptors in active tissue(groups 3/4 stimulation)
4. narrowed blood vessels and shorter vessel length in UE= increased BF resistance leading to increased BPs
5. energy demands of trunk stabilization impairing mechanical efficiency
what will eating a large meal do to blood going to metabolically active tissue?
decrease blood flow since it has to route blood to the GI
what two factors will worsen the competition for blood?
dehydration and heat
what is the Po2 during exercise, specifcally at metabolically active tissue?
0
due to the tissue taking all available O2
what is the Po2 during max exercise in general, more importantly, why?
16- 17 mmHg
mixing with venous blood from none metabolically active tissues
what 3 pressures affect capillary fluid into and out of a tissue(think about what is blood made of and the pressure associate with those)?
Hydrostatic (SBP and DBP)
Oncotic pressure (Proteins)
Osmotic Pressure (Electrolytes)
what occurs to plasma volume during upright exercise and what causes this via what 3 functions?
Decreased PV: due to intensity
1. increased MAP -> Increased capillary hydrostatic pressure
2. Metabolite buildup in muscle-> increases tissue osmotic pressure
3. sweating further will decrease plasma volume
what are 4 net effects of decreasing PV(think about thick blood)?
RBC concentration increases
Hb concentration increases
O2-carrying capacity increases
Increased blood viscosity->increased HR
big point: what is the central command theory, and where are effects seen?
Higher brain centers co-activate motor and CV centers( neuronal spillage) in a feedforward fashion
-1 AP could signal 2 tissues
effects can be seen in skeletal m., heart, lungs, and group 3/4
does the CCC(cardiac command center) use negative or positive feedback, what 2 receptors provide this information and what does it do with these responses?
1. negative.
-why the hell would it use positive, its not giving birth.
2. Central and peripheral receptors
3. used to fine tune CV responses for MAP regulation
Big Point: T/F humans will NOT prioritize MAP above other physiologic needs.
the biggest FALSE ever
-it will always come before every need because without it we cant do those other needs.
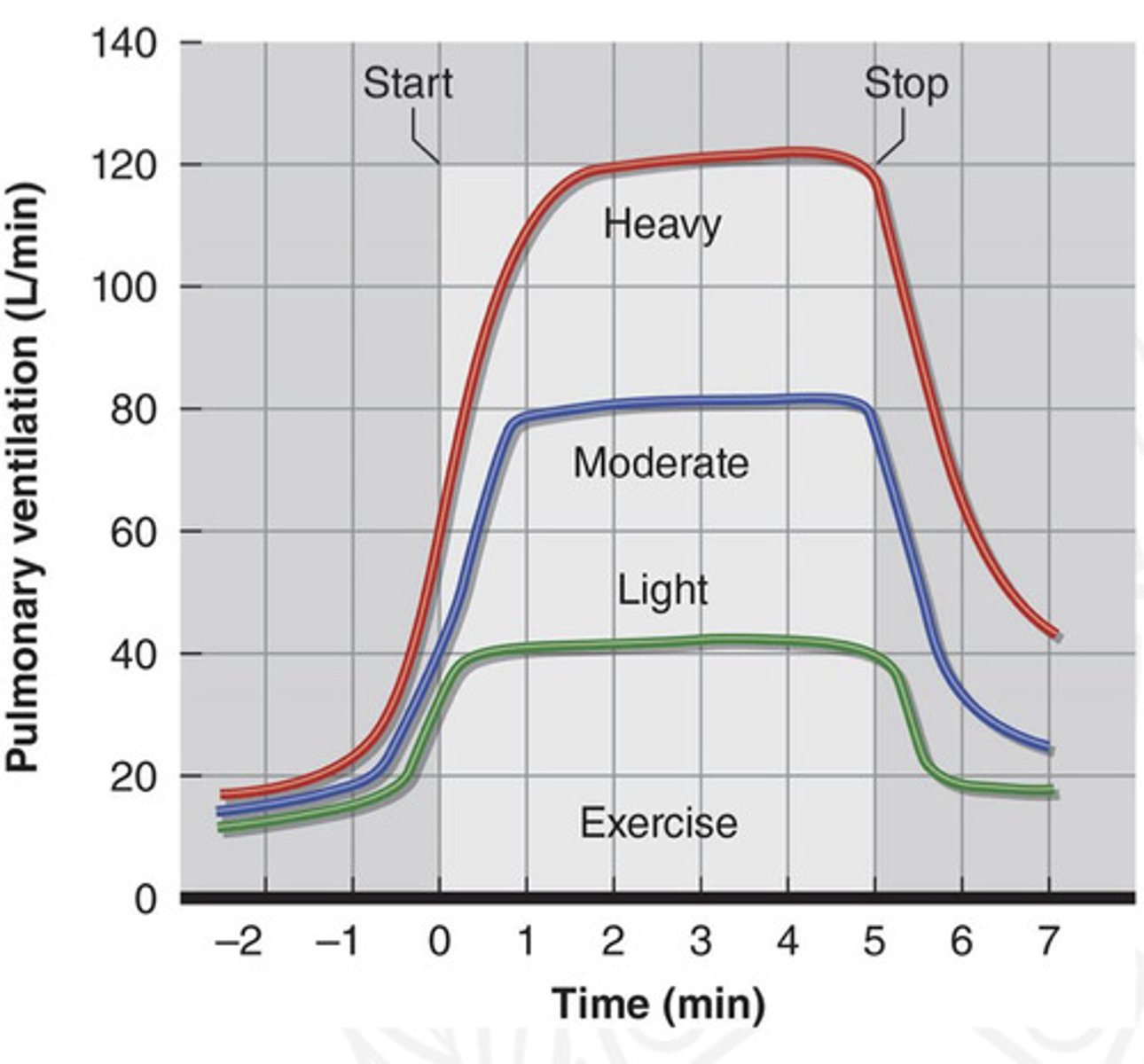
describe the 3 phases of minute ventilation(VE) during exercise
Phase 1: immediate increase in VE
-can occur before or at onset of exercise from the neural system
-anticipatory response from central command group 3/4 muscle afferents
Phase 2: gradual increase in VE
-driven by hormonal and chemical changes(increase CO2, K+ and H+) in arterial blood sensed by peripheral chemoreceptors
Phase 3: VE achieves steady state
-via peripheral and central feedback
what feedback comes from right atrial stretch receptors?
An increase in VE is proportional to increase in Cardiac Output
Ventilation will increase proportionally to metabolic demand. At low exercises, what respiratory volume will be the main cause of an increase in VE?
Tidal Volume
what occurs to Tidal Volume and respiratory rate during >60% VO2 max, and how does this affect VE?
Tidal volume: will slowly plateau but never entirely, VE will be sustained from this
Respiratory Rate: increase accordingly, driving VE up
Big Point: tidal volume is similar to SV(he said to write this down so)
Synthesis point: why does VE remain high during post exercise?
it will help in oxidizing lactate, removal of metabolites, cori cycle, lactate shuttle
what are the 3 regulatory process of post-exercise breathing?
1. Acid-base balance (blood pH)
2. restoration of Pco2
3. return of blood temperature
Dyspnea is classified as ?
a shortness of breath
-caused by an inability to adjust high blood Pco2 and H+
hyperventilation is classified as ?
what occurs to the PaCO2 and PAO2 (partial pressure of CO2 and O2 in arteries and alveoli)?
excessive ventilation:breathing in a bag does have a physiological explanation
-respiratory alkalosis, often created by anxiety or anticipation about exercise
-decreasing PaCO2 will increase PAO2 (alveolar
-decreasing PaCO2 -> increased blood pH-> decrease drive to breath
(often syncope(fainting) occurs)
Big point: what is Ventilatory Equivalent and what does it represent?
-Ventilatory Equivalent= Ve/VO2 (L air breathed / L O2 consumed /(per) min)
-represents and index of how well the control of breathing is matched to the bodys demand for oxygen
BIG POINT: what is Ventilatory Threshold (Vt) and what does it represent?
-it is a point where Ve increases disproportionately to L O2 consumed
-indicates a shift towards increasing anaerobic metabolism, increasing VCO2 stimulates respiration
when will Vt (as a percent of VO2 max) in untrained and trained individuals?
55-70% from untrained to trained
Big point: T/F Lactic Acid and CO2 WILL accumulate simultaneously.
TRUE
-RER will increase while this happens to above 1 due to alot of factors but the buffers become overwhelmed and cannot remove H+ so they move away from Oxidative metabolism.
what are 3 ways you can increase your bicarbonate reserve?
training
supplements
nutrition
BIG POINT: what is the ventilatory equivalents method, when does it occur and what are the steps to determine Vt?
1. Ventilatory threshold reflects the disproportionate increase in VE (to remove CO2) relative to VO2
2. theres in increase in Ve/VO2(ventilatory equivalent of Oxygen) WITHOUT an increase in Ve/VCO2(ventilatory equivalent of Carbon Dioxide)
3.
step one: find the lowest point of Ve/VO2 curve just before an increase(should happen first)
step two: find the plateau of Ve/VCO2 curve
(possible)Exam Question: identify the workload that the VT occurs at from the graph
occurs around 175 watts
use the steps listed: of course he wont give us the Vt
step one: find the lowest point of Ve/VO2 curve just before an increase(should happen first)
step two: find the plateau of Ve/VCO2 curve
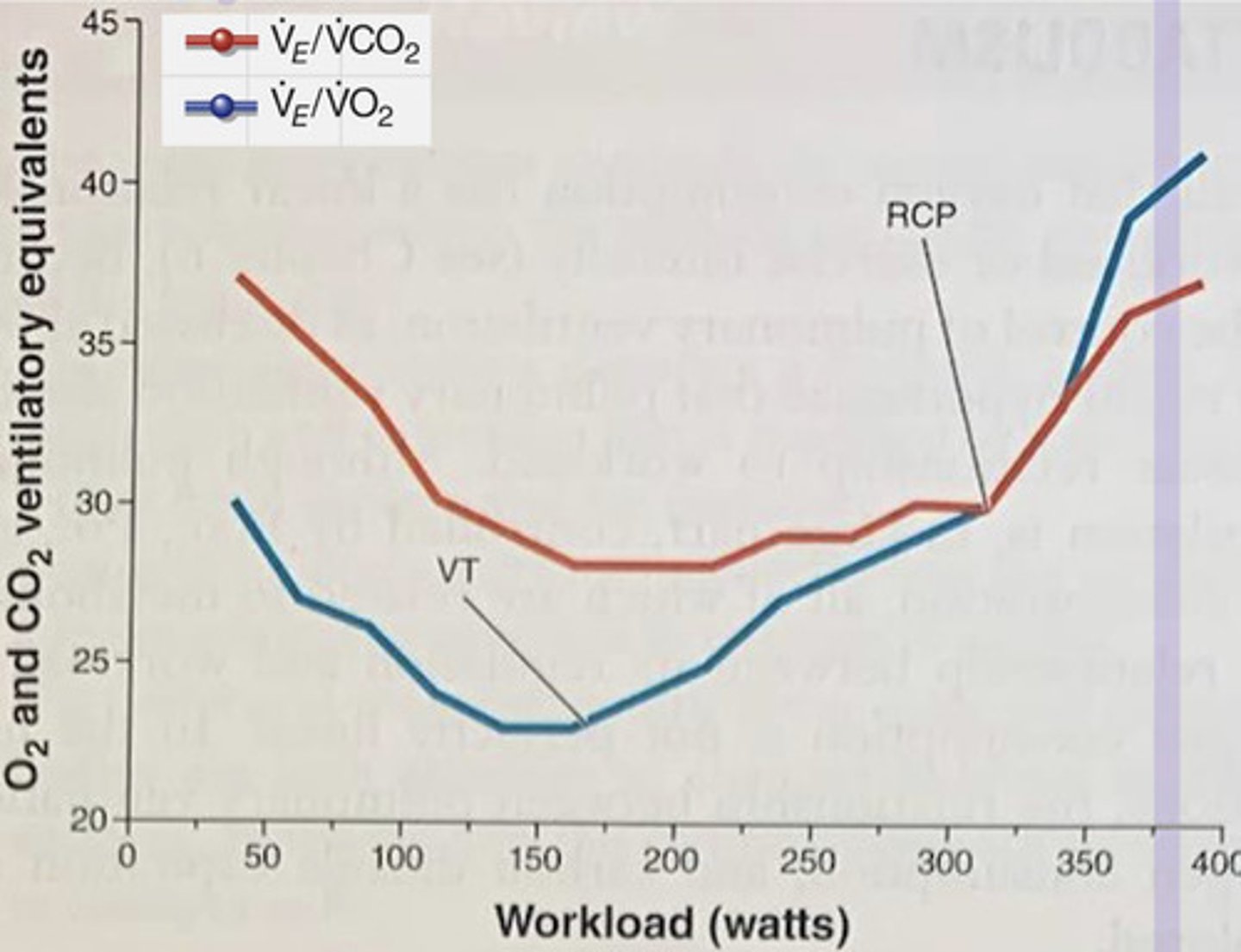
what is the RCP and what does this represent?
-the point on the ventilatory equivalents graph where Ve/VO2 and Ve/VCO2 both increase
-uncoupling of PCO2 control of VE, indicates the Bicarb Buffering system has been surpassed.
what is V-slope method used for?
determining anaerobic threshold
BIG POINT: What is Exercise-induced arterial hypoxemia and who is mainly affected?
1. it is a pulmonary diffusion limitation, essentially the ventilation and cardiac output is way too fast for the blood to become saturated with Hb
2. only affects super elite athletes, not regular people
Big point: what is the best way for quicker reduction in blood lactate levels during active recovery and what 2 mechanisms support this?
1. keeping the blood circulating, just keep moving and dont sit down or stop moving
2.
-respiratory/renal removal of excess CO2 via bicarbonate buffering system
-lactate removal by muscles, liver and heart(cori cycle, lactate shuttle)