midterm patho unit 5-7
1/132
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
133 Terms
Signs and symptoms of pulmonary disease Dyspnea
discomfort in breathing shortness of breath signs include flaring of the nostrils, use of accessory muscles of respiration
Signs and symptoms of pulmonary disease Orthopnea
dyspnea upon lying down (abdominal contents put pressure on diaphragm)
Signs and symptoms of pulmonary disease Paroxysmal nocturnal dyspnea PND
waking up at night with dyspnea
Signs and symptoms of pulmonary disease Cough
initiated by irritant receptors in the airway. Few of these receptors in the distal portions of the respiratory tree, so significant secretion build up before the cough reflex occurs
Signs and symptoms of pulmonary disease Abnormal sputum
changes in the amount color and consistency microscopic observation can reveal cellular debris and microorganism
Signs and symptoms of pulmonary disease Hemoptysis
expectoration of blood (bright red, alkaline pH, frothy sputum
Signs and symptoms of pulmonary disease
Abnormal breathing pattern
hypo- or hyperventilation
Hypoventilation is a breathing condition where your airflow is too slow or too shallow to meet your body's needs
Signs and symptoms of pulmonary disease Cyanosis
bluish discoloration of skin and mucous
membranes, due to increased amounts of deoxygenated
hemoglobin in the blood
Signs and symptoms of pulmonary disease Clubbing
selective bulbous enlargement at end of a digit

Signs and symptoms of pulmonary disease Pain
originates in pleurae,
airways or chest wall. Caused by
infection, inflammation, stiff muscles
from coughing, etc.
Conditions caused by pulmonary disease or injury Hypercapnia (hypercarbia)
increased carbon dioxide in the arterial blood
Caused by hypoventilation of the alveoli only
CO2 passes very readily from the blood to the alveolar space 20x more readily that O2 so is affected only by exchange in alveolar gases that occurs within ventilation not diffusion
Can be a result of anything decreasing drive/ability to breath including
Drugs
Damage to medulla
Physiologic dead space e.g caused by emphysema
Conditions caused by pulmonary disease or injury Hypoxemia
reduced oxygenation of arterial blood
Different from hypoxia: reduced oxygenation of tissue cells
It Is much harder for 02 to diffuse across the alveolocapillary membrane than CO2, so several factors affect oxygenation of the blood
Hypoxemia results from defects in one or more of the three mechanisms of oxygenation
Oxygen delivery to the alveoli
Diffusion of oxygen from the alveoli to the blood
V/Q mismatch
Decreased diffusion across alveolocapillary membrane
Anatomical right to left shunt
Alveolocapillary
(or alveolar-capillary) refers to the functional unit in the lungs where the exchange of oxygen and carbon dioxide takes place
Oxygen delivery to the alveoli
Decreased oxygen in the air or decreased ventilation
Individuals who are unconscious, have disease that restricts chest expansion
Diffusion of oxygen from the alveoli to the blood
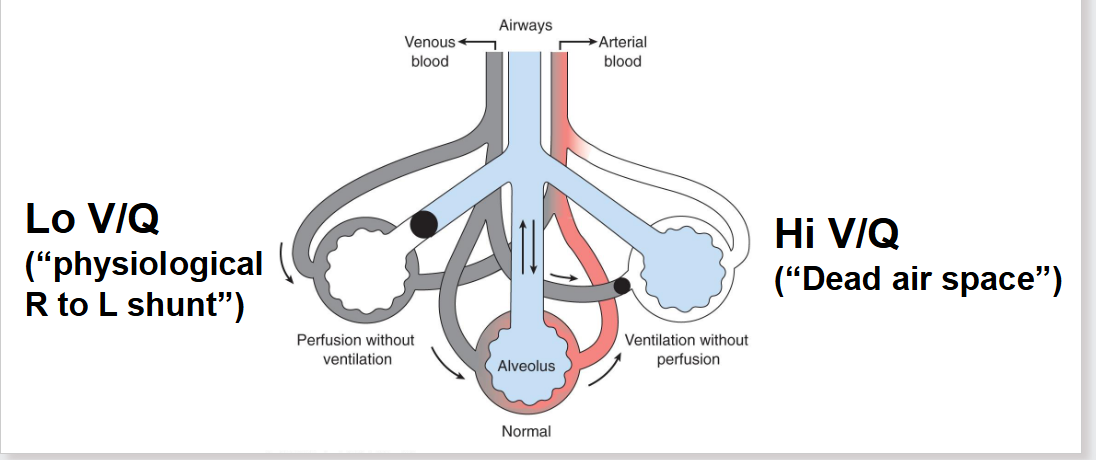
V/Q mismatch: imbalance between alveolar ventilation V and perfusion Q
Most common cause of hypoxemia!
High V/Q or low V/Q
Decreased diffusion across alveolocapillary membrane
Due to thickened membrane because of edema or fibrosis
pulmonary embolism
A pulmonary embolism (PE) is a sudden blockage in one of the pulmonary arteries in your lungs.
V/Q Mismatch explained Ventilation perfusion ratio
High V/Q: inadequate perfusion of well-ventilated area producing alveolar dead space (wasted ventilation). Occurs mainly due to pulmonary embolism
Low V/Q inadequate ventilation of well perfused area of lung
Occurs with atelectasis, asthma, pulmonary edema
Referred to as physiological right to left shunt = blood moving through unventilated part of lung vs anatomic right to left shunt next slide
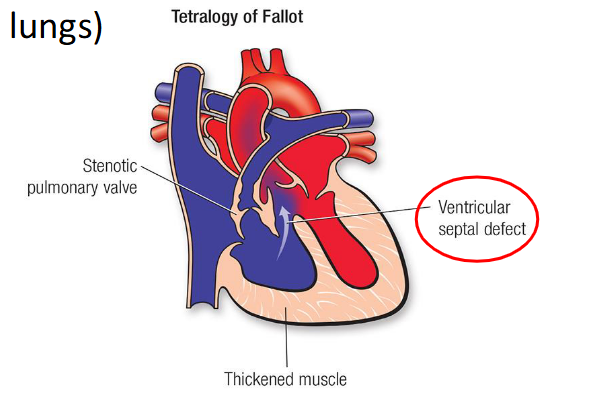
Anatomical right to left shunting
Where blood doesn’t physically go through the lungs, due to structural defect in the heart (abnormal blood flow from heart to lungs
The pulmonary circulation is partially bypassed due to a physical short circuit of blood flow through the heart. Blood flow to the alveoli is therefore reduced
Disorders of chest wall and pleura
Chest wall restriction
Results in decrease in tidal volume
Occurs when the chest wall is deformed, traumatized immobilized
Examples
neuromuscular diseases -poliomyelitis, muscular dystrophy
trauma to chest wall
flail chest from fracture of several
consecutive ribsparadoxical movement, looks like ur rib change is caving in
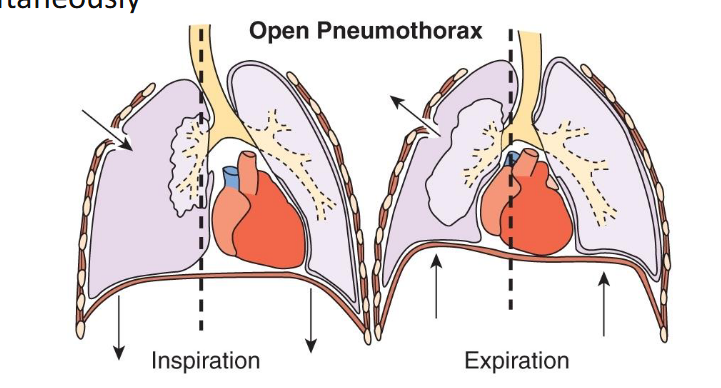
Disorders of lung inflation Pneumothorax
Presence of air in the pleural space caused by a rupture in the visceral or partial pleura. Air pushes on the outside of the lung and makes it collapse
Treatment involves inserting a needle or chest tube between the ribs to remove the excess air; a small pneumothorax may heal spontaneously
Disorders of lung inflation Pleural effusion
Presence of excess fluid in the pleural space
Usually through migration of fluid through walls of capillaries bordering the pleura
Disorders of lung inflation Empyema
Infected pleural effusion a collection of pus in the pleural space
Complication of pneumonia, surgery etc
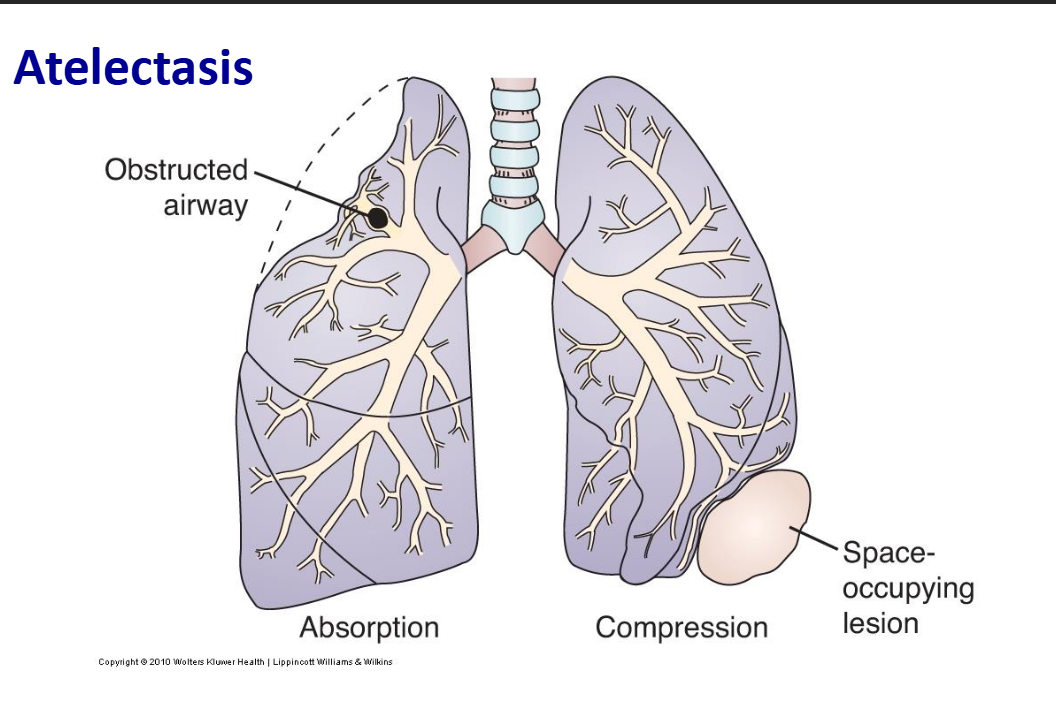
Disorders of lung inflation Atelectasis
Collapse of lung tissue deflated alveoli by
External compression e.g fluid in pleural space, tumor, abdominal distension
Obstructed airways: air is absorbed from obstructed alveoli and they collapse
Decreased production of surfactant e.g anesthesia
Clinical manifestations: dyspnea, cough, fever, leukocytosis
Commonly develops after surgery patients in pain breathe shallowly, produce viscous bronchial secretions- narcotics/ anesthesia dry up surfactant
Post surgery patients advised to breathe deeply, become ambulatory asap (start walking), and change positions frequently when laying down
Disorders of lung inflation Bronchiectasis
Permanent dilation of the bronchi, secondary to other diseases that cause chronic inflammation of bronchial wall
e.g TB tuberculosis, cystic fibrosis
Chronic inflammation leads to destruction of elastic and muscular components of bronchi walls and permanent dilation
Clinical manifestations include chronic cough, recurring lower respiratory tract infection, production of purulent sputum cupfuls (yellow mucus), hemoptysis9cough blood) and clubbing of the fingers
Disorders of lung inflation Cystic Fibrosis (CF)
Autosomal recessive disorder
• Mutation in chloride channel causes
thick mucus in airways
– Cl- ion is NOT transported out of cells into airway
– increased absorbance of sodium and water from
respiratory (and pancreatic) secretions →
– very thick mucous→
– mucous accumulates (cilia cannot move)→
– increasing the risk of infections (especially with
Pseudomonas aeruginosa)
Porth p742-3
• Recurring infections produce bronchitis, eventually bronchiectasis
• Treatment: includes antibiotics to control infection, managing
pancreatic enzymatic insufficiency, supporting lung function
Pulmonary vascular disease Pulmonary embolism
Occlusion of a portion of the pulmonary vascular bed by an embolus
Most common embolus is a clot from deep venous thrombosis in lower leg
Obstruction of blood flow causes pulmonary vessels to constrict, resulting in impaired gas exchange V/Q mismatch Occlusion of a portion of the pulmonary vascular bed by an embolus
If clot is not dissolved fast the resulting hypertension could lead to heart failure
Clinical manifestations Pulmonary embolism
• Depends upon size and location
of obstruction
• Small emboli may go unnoticed
unless patient’s health is
otherwise compromised
• Moderate emboli: sudden
onset chest pain, dyspnea,
tachypnea, tachycardia
• Massive emboli: sudden
collapse, crushing chest pain,
shock – often fatal
Pulmonary vascular disease Pulmonary hypertension
Elevated mean pulmonary artery pressure
Most cases develop as a serious complication of many acute and
chronic pulmonary disorders (e.g., COPD)
• A common cause is continued exposure of pulmonary vessels to
hypoxemia, which causes these vessels to constrict (unlike systemic
vessels, which dilate)
• Can also be caused by mitral valve disorders or left ventricular diastolic
dysfunction, which raise left atrial pressure (ie caused by LHF)
Pulmonary vascular disease Cor pulmonale
Right ventricular enlargement (hypertrophy, dilation, or both) caused
by chronic pulmonary hypertension
• Results in increased systemic venous circulation = peripheral edema
Pulmonary vascular disease Pulmonary edema
Excess “water” in the lungs
– Most common cause is left-sided heart failure
• Failure of left ventricle→ increased filling pressure, → causes back-up of
blood in lungs→ increasing pressure in lung capillaries. When this exceeds
osmotic pressure of lung capillaries→ fluid and RBCs leave capillaries and
collect in the interstitial space
– When there is too much interstitial fluid for lymph system to collect,
edema occurs. Fluid eventually leaks into the alveoli:
– fewer alveoli available to expand with air
– means a reduction in surface area of respiratory membrane
– fluid “thickens” respiratory membrane (increased distance for gas diffusion)
– Results in reduced oxygen diffusion rate → hypoxemia
– Clinical manifestations: dyspnea, cyanosis, increased physical effort
in breathing, blood-tinged frothy sputum
Obstructive lung diseases
due to airway obstruction that is worse with expiration - emptying of the lungs is slowed
caused by conditions such as asthma, chronic bronchitis and emphysema
because the latter two often occur together they are called chronic obstructive pulmonary disease COPD
unifying symptom in dyspnea
unifying symptom is wheezing
Emphysema
is a chronic lung disease where the tiny air sacs (alveoli) in your lungs are permanently damaged and destroyed
Bronchial Asthma basic definition
a chronic inflammatory disorder to the bronchial mucosa that causes hypersensitivity and constriction of airways
interplay of genetic and environmental factors
exposure to an allergen results in a cascade of inflammatory events leading to acute and chronic airway dysfunction
Bronchial asthma Acute phase response
Acute
Usual type I hypersensitivity response: allergen
exposure to the bronchial mucosa activates B
cells (plasma cells) to produce IgE which
complexes with mast cells
– Further exposure cross-links the IgE, causing the
mast cells to release a host of chemicals→
causing vasodilation, increased capillary
permeability, mucosal edema, bronchial smooth
muscle contraction and mucous secretion. (See
diagram; also Module 2 )
– Clinical manifestations at the beginning of an
attack:
• chest constriction, expiratory wheezing,
dyspnea, tachycardia, coughing
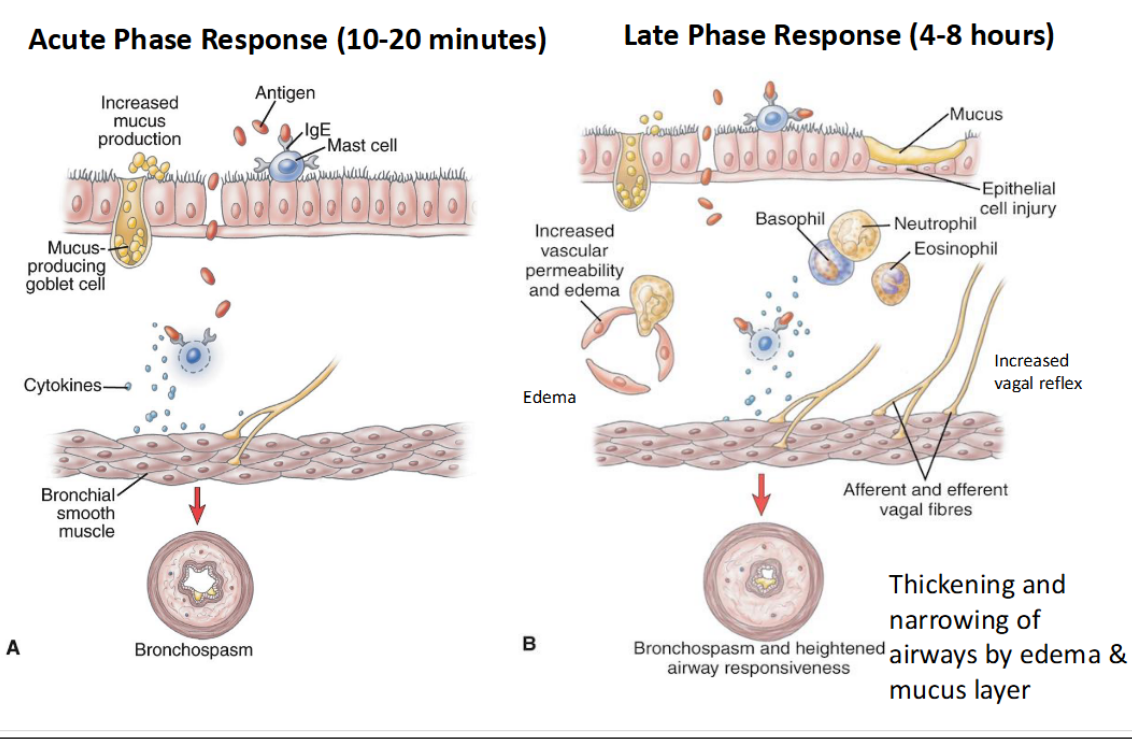
Bronchial asthma late phase response
– Begins 4-8 hours after the early response; can be
more severe than initial attack
1. Release of inflammatory chemicals
– Chemokines released by cells in early response call
other inflammatory cells: neutrophils, eosinophils
and lymphocytes, to the area
– Inflammatory chemicals released by these cells
cause further bronchospasm, edema and mucous
secretion
2. Cell damage and mucous accumulation
– Damage from these chemicals occurs to ciliated
epithelial cells. Mucous accumulates and cellular
debris forms plugs in the airways impeding alveolar
ventilation. (See diagram)
– Untreated inflammation can lead to long-term
airway damage that is irreversible
3. Air trapping → hypoxemia → respiratory
alkalosis
– The obstructed airway makes it more difficult
to expire, causing air to be trapped in alveoli,
increasing alveolar gas pressures. This causes
decreased perfusion of blood over the alveoli
(capillaries collapse), leading to hypoxemia
– The hypoxemia stimulates the respiratory
centre → hyperventilation
– CO2 diffuses out of blood causing hypocapnia
and respiratory alkalosis
. Impairment of respiratory muscles → respiratory
acidosis
• The continued obstruction of airways increases
air trapping (incomplete expirations), which
hyperexpands the lungs and thorax, decreasing
the tidal volume and increasing hypoxemia
• At this point, CO2 levels will rise, leading to
hypercapnia and respiratory acidosis; the
situation is life-threatening if treatment does not
reverse the process quickly (mechanical
ventilation may be required)
• Mainstays of treatment are:
• avoidance of allergens
• inhalation of anti-inflammatories,
bronchodilators and adrenaline in acute
attack
Chronic obstructive pulmonary disease COPD
characterized by airway obstruction that causes
difficult exhalation
= both emphysema and chronic bronchitis
Chronic bronchitis
Very commonly caused by smoking
Porth p738
Definition:
– Hypersecretion of mucous and chronic productive
cough for at least 3 months of the year, for at least
2 consecutive years
Development:
1. The airway becomes inflamed with inspiration of
irritants. Edema occurs, along with the production
of thick, tenacious mucous
2. Continual inflammation leads to increases in size
and number of mucous glands and goblet cells in
the airway epithelium
Continual inflammation brings in macrophages and
neutrophils that release proteases, which harm ciliated
epithelial cellsDue to impairment of the ciliary function, the mucous
cannot be clearedAirways are constricted by thickened bronchial wall
(increased gland size) and mucous. Expiration becomes
more difficult as airways are narrowed during this part of
respiratory cycle (they’re still pulled open for inspiration)Obstruction eventually leads to hypoxemia
Eventually the airways collapse early in expiration, causing
air trapping. This expands the thorax, making expiration
even more difficult = decreased tidal volume,
hypoventilation and hypercapnia
Once pathologic changes occur, they are not reversible
• “blue bloaters”: hypoxemia and edema, caused by
eventual right heart failure
Treatment of chronic bronchitis :
• Bronchodilators and expectorants as needed to control
cough and reduce dyspnea
• Stop smoking
• Chest physical therapy
• Eventually antibiotics (infection), steroids (last resort),
home oxygen therapy
Emphysema
Characterized by a loss of lung elasticity and abnormal
enlargement of the airspaces distal to the terminal bronchioles,
with destruction of the alveolar walls and capillaries
• “Obstruction” results from changes in the lung tissue, primarily
loss of elastic recoil (rather than from mucous production and
inflammation as for chronic bronchitis)
• Causes:
• most commonly inhalation of irritants – e.g., cigarette smoke,
air pollution - that increases number of inflammatory cells
• an inherited condition - insufficiency of alpha1-antitrypsin
that normally combats naturally-occurring proteases from
inflammatory cells
Development of emphysema
1. Inflammation occurs, and inflammatory cells (neutrophils,
macrophages) release proteases that cause destruction of
alveolar walls. This eliminates part of capillary bed and increases
volume of alveoli.
2. This produces large air spaces within the lungs (bullae), and on the
surface of the lungs, next to the pleura (blebs). These air spaces
can not function in gas exchange, which increases hypoxemia.
3. Damage from inflammation includes a loss in the elastic lung
tissue, which normally helps to keep air passages open.
Expiration becomes more difficult, thus trapping air in the lungs.
4. This hyperexpands the thorax (barrel chest), making it difficult to
breathe, causing hypoventilation and hypercapnia.
Treatment of emphysema
• Must include cessation of smoking (if the patient
smokes)
• Inhalation of corticosteroids and bronchodilating drugs
• Oxygen therapy, if required
• Possible lung reduction surgery or transplant
Pink puffers
• initially hypoxemia is not
serious -because increased
breathing can keep up with
oxygen demand until late
stages of the disease
• classic tripod breathing
position, with lips pursed
increases lung pressure
during exhalation, in an
attempt to keep breathing
passages open
Acute lung injury (ALI) /
acute respiratory distress syndrome (ARDS)
ARDS is a more severe version of ALI
• Both involve acute lung inflammation and injury to the
alveolocapillary membrane, leading to severe pulmonary
edema and hypoxemia
• Causes include:
• sepsis, trauma, pneumonia, drug overdose, smoke inhalation,
aspiration of gastric contents (acid)
• Injury and edema is due to inflammatory response to
initial injury or to direct cause (smoke inhalation)
Development of ALI/ARDS
• As a response to injury, neutrophils and platelets release
inflammatory chemicals that damage the alveolocapillary membrane
and greatly increase capillary membrane permeability, allowing blood
to leak into the interstitial spaces and alveoli = edema
• There is surfactant inactivation, causing collapse of alveoli, which
adds to decrease in gas exchange
• A hyaline membrane forms, impairing gas exchange
• If injury is extensive, repair of tissues may produce fibrosis
Clinical manifestations of ALI/ARDS include
Rapid onset of respiratory distress (marked dyspnea, rapid, shallow
breathing, inspiratory crackles), usually within 12-18h of injury
– Severe hypoxemia occurs that cannot be successfully treated with
supplemental oxygen therapy
– There may be a systemic response as the inflammatory compounds
spread through the body
• Treatment includes supplying oxygen (assisted ventilation with high
concentrations of oxygen) until lungs heal
• ARDS is difficult to diagnose and can prove fatal if not properly
treated within 48 hours
– Mortality associated with ARDS remains at 50-70%.
Acute respiratory failure (ARF)
Inadequate gas exchange, leading to lower PaO2,
higher PaCO2 and pH <7.30
– Can be divided into two types:
• Hypercapnic/hypoxemic - due to failure of ventilation
• Hypoxemic - due to failure of gas exchange within the lungs
– These two types can overlap
– Important potential complication of surgery
• atelectasis, pneumonia, pulmonary edema and pulmonary
embolism
Hypercapnic/hypoxemic
respiratory failure
• Due to failure in ventilation causing the increase in
arterial CO2 and hypoxemia
• Causes of interrupted/abnormal ventilation:
– E.g. diseases of the nervous system, disorders of the respiratory
muscles
• Can be treated with mechanical ventilation
Hypoxemic respiratory failure
Brought about through either:
• Ventilation/perfusion mismatch – often seen in people with
COPD, where a lung region may either not be perfused or
not ventilated
• Impaired diffusion – often seen in interstitial lung disease,
ARDS, pulmonary edema and pneumonia (why?)
• Treatment: administration of high concentrations of oxygen
(increases the diffusion gradient)
Age-Related Issues
Vital capacity and respiratory muscle peaks at 20-25
yr and then decreases
• After 40 years - alveolar surface area decreases
• After 50 years - alveoli start to lose elasticity and
decrease in chest wall motility
Alterations of pulmonary function in children:
Croup
Porth p714-5
• Characterized by inspiratory stridor (wheezing tone
during inspiration due to URT
obstruction/inflammation), hoarseness and a barking
cough
• Can be caused by virus, allergy or bacteria
– most commonly laryngotracheobronchitis (LTB)
caused by viruses, mainly in children 6 mo – 5 yrs
• Severe croup results in retractions (indentations of
skin around ribs and sternum) showing use of
accessory muscles of respiration
• Usually self-limiting
Bronchiolitis
Inflammation of small airways (bronchioles), caused by
virus
• Common in children 2-12 mo
• Wheezing, dyspnea, cough
Epiglottitis
Caused by bacterial infection
• Swelling of larynx, epiglottis
• Fever, sore throat, inspiratory stridor
Respiratory distress syndrome in infants (IRDS
Premature infants, due to surfactant deficiency
Gastroesophageal reflux disease (GERD)
Development: Return of stomach
contents into the esophagus because
of relaxation of the lower
esophageal sphincter or
gastroparesis (slowing of movement
of food from the stomach), by
increasing gastric volume and
pressure
Porth p941
• Clinical manifestations: heartburn (burning sensation under the
sternum) and dyspepsia (indigestion)
• If reflux is frequent, esophagitis can occur
• Long-term inflammation can lead to fibrosis and precancerous
lesions
can occur spontaneously, even in normal individuals; gastric contents are usually
neutralized and cleared within minutes
Factors increasing the likelihood of
Gastroesophageal Reflux
Infancy – positional and reduced sphincter tone
• Increased intra-abdominal pressure
– obesity
– pregnancy
• Smoking
• Certain foods relax the LES
– fats
– coffee
– alcohol
• Individuals with lupus have more problems with
GERD due to connective tissue problems
Peptic Ulcer Disease
Break down in the protective mucosal lining of the lower
esophagus, stomach or duodenum
• Ulcers can be single or multiple, acute or chronic, and
superficial (more properly called “erosions”) or deep
• Most common complications:
1. hemorrhage - causes hematemesis (vomiting of blood, bright red
or “coffee ground”) or melena (black foul-smelling stools)
2. perforation - ulcer erodes through wall and contents enter
peritoneum
3. penetration - ulcer erodes into another organ, e.g., liver
4. gastric/duodenal outlet obstruction (from edema or scarring)
Helicobacter pylori passes through the
protective mucous layer of the stomach
Stomach acid keeps the mucin
lining the epithelial cell layer in a
spongy gel-like state, which is
impermeable to H. pylori
• However, the bacterium releases
urease which neutralizes the
stomach acid and liquefies the
mucin
• The bacterium can now penetrate
it and reach epithelial cells
inducing inflammation
→ Stomach acid and pepsin can now penetrate the
mucosal barrier, leading to ulceration
NSAIDS interfere with prostaglandin synthesis
Prostaglandins inhibit acid secretion and stimulate mucous and
bicarbonate secretion
• NSAIDS inhibit prostaglandin production thus blocking production of
mucous and bicarbonate and increasing acid production --> making the
stomach vulnerable to injury from acid and enzymes
1. Gastric Ulcers
Tend to develop in older people (55- 65 yr)
• About ¼ as common as duodenal ulcers
• Major causes:
– infection with H. pylori
– chronic use of NSAIDs
• Clinical manifestations:
– intermittent pain in epigastric region (upper abdomen)
– pain frequently occurs immediately after eating
– gastric ulcers tend to be more chronic than duodenal ulcers
and the duration of treatment is longer
2. Duodenal Ulcers
Occur with greater frequency than other types of peptic
ulcers
– tend to develop in younger people, and more commonly in
males
• Also mainly caused by H. pylori infection and chronic use
of NSAIDs
• Clinical manifestations:
– Chronic intermittent pain in the epigastric area
– Pain begins 2-3 hr after eating (empty stomach) and is
relieved rapidly by ingestion of food or antacids
Peptic Ulcer Treatment
Eradicate H. pylori with antibiotics
• Reduce acidity
– antacids e.g. calcium carbonate
– proton pump inhibitors (interferes with the
secretion of hydrogen ion from parietal cells)
– H2 receptor antagonists (blocks the action of
histamine which causes HCl secretion)
• Minimally invasive surgical resection if ulcers are
bleeding or have perforated the GI wall
Ulcerative colitis
Chronic inflammatory disease of colon
• Ulceration of the colonic mucosa; most commonly in the
rectum and sigmoid colon.
– Usually beginning in the rectum, the ulceration spreads in a
continuous manner. Condition can be sporadic
• Cause as yet unknown
– current thinking: normal state of bacterial tolerance has been
disrupted, producing an unregulated immunological response
• Risk factors include age (20-40 yrs of age) and family
history
Development of ulcerative colitis
1. Inflammation of the mucosa results in edema and thickening of the
wall of the tract
2. Destruction of the mucosa causes bleeding, pain, and an urge to
defecate, even if colon is empty (= tenesmus).
• Frequent bloody diarrhea is the common symptom (1-10+ BM per day)
3. Fluid loss, bleeding and inflammation produce dehydration, weight
loss, anemia and fever
4. High risk for development of cancer of the colon
• Extreme cases can develop toxic megacolon, an abrupt increase in
diameter of colon (within one to a few days) that could rupture
• Treatment may involve
– Anti-inflammatory drugs
– IV administration of fluid for dehydration and malnutrition
– Surgical resection - removal of the colon/anus results in need of a colostomy bag
Crohn’s disease
Also an inflammatory disease of the intestine, thought also to be
unregulated response against bacteria
• Inflammation begins in submucosa – activated neutrophils and
macrophages cause tissue injury, resulting in granulomas developing
in the intestinal wall. Lesions have a “cobblestone” appearance
• Affects both large and small intestine (rectum is seldom involved)
• Inflammation of the entire width of the intestinal wall (from serosa
to mucosa) occurs, sometimes in patches (skip lesions)
• Over time, the bowel becomes thickened and inflexible
• Risk factors include family history
• Age range is 20-30; slightly more common in women
Crohn’s disease cont’d
Often asymptomatic for years, syndrome can also be sporadic
• Problems with absorption can cause electrolyte imbalances, anemia
(if the ileum is involved - cannot absorb vitamin B12)
• Most common symptom is diarrhea (not as commonly bloody as with
UC) with tenesmus, accompanied by weight loss and abdominal pain
(usually in lower right quadrant).
• Toxic megacolon may also occur (less than with UC)
• Complications can include fistulas, abscesses, obstruction
• Treatment is similar to ulcerative colitis
Celiac Disease
Malabsorptive disease where the mucosa fails to absorb
digested nutrients
• Also called sprue or gluten-sensitive enteropathy
• Development:
– T-cell mediated immune disorder
– an intense immune reaction to gluten (gliadin - the protein
component of cereal grains)
– inflammation damages small intestinal villous epithelium,
interfering with absorption of macro and micronutrients
• Usually appears in infants when gluten containing
substances are added to diet but occurs at older ages too
• Primary treatment is removal of gluten from diet
Clinical Manifestations of Celiac Disease
• In childhood: failure to thrive
• Abdominal pain and bloating
• Diarrhea with fatty stools
• Malabsorption of nutrients leading to:
– Osteoporosis, seizures/tetany from lack of calcium
– Anemia from lack of iron
– Short stature (developmental form) from general
malnutrition
– In pregnancy: miscarriage, neural tube defects due to
lack of folic acid, and other nutrients
Liver Disorders
Disorders of the liver are extremely serious, due to the
liver’s function in many metabolic processes
• Common complications of liver disorders:
1. Portal hypertension - abnormally high blood pressure in
the portal venous system
– caused by disorders that obstruct blood flow through the
portal venous system or vena cava
• including thrombosis of hepatic veins, severe right-sided heart failure,
alcoholic cirrhosis
–Long term portal hypertension can result in further
complications
• including ascites, splenomegaly and portosystemic shunts with
accompanying esophageal varices
2. Ascites:
accumulation of fluid in the peritoneal cavity
• Caused by:
― portal hypertension or
― decrease in serum protein production by liver
― lower osmotic pressure of capillaries-> retention of fluid in the tissues,
which then seeps into peritoneal cavity
• Fluid (up to 15L) in abdominal cavity pushes on diaphragm,
causing breathing difficulties
• Treatment: paracentesis - drainage of fluid from
abdominal cavity using a needle; with caution (to avoid
shock)
• ascites will re-occur if liver problem is not fixed
3. Portosystemic Shunts –
Diversion of blood to inferior vena cava via other veins to
bypass the liver
e.g to esophageal veins causing esophageal varices
Development:
a) There are veins that drain from the esophagus -> hepatic portal vein,
and also veins that drain from the esophagus -> inferior vena cava
b) If blood flow is impaired through the hepatic portal vein, the pressure in
the “portal” system becomes greater than normal. There will be an
increased resistance impeding blood to flow from the esophagus->portal
system
c) Collateral veins develop between veins of esophagus and vena cava->
blood will back up from the portal system through the esophageal veins
and into the inferior vena cava
d) Blood will therefore bypass the liver…
e) The collateral veins that develop
cannot withstand the pressure of
the blood coming from the portal
system→ they swell and distend
(varicose veins = “varices”)
• Esophageal varices within the
esophageal wall easily rupture
• Manifestations:
• hematemesis and melena
– hemorrhage can be life-
threatening
Porto-systemic shunts also cause varices
in other veins
• Caput medusae
- collateral veins form
varices on the abdominal wall
• Hemorrhoids
- collateral veins form varices
in the rectum
4. Hepatic encephalopathy
in liver dysfunction, toxins (e.g., ammonia) remain
in bloodstream and reach brain
• Because collateral vessels are shunting blood past the
liver where ammonia should be converted to urea
• Neurotransmission is affected
• Manifestations: personality changes, memory loss,
confusion, flapping of hands (asterixis), possibly
worsening to coma
5. Jaundice (icterus)
• RBC are broken down in the spleen and the liver -> releasing
bilirubin, which the liver processes and excretes in bile
• Jaundice is the green/yellow tinge to skin caused by
hyperbilirubinemia
• High concentrations of bilirubin in the blood can have 3 causes:
– too many RBC being broken down
– interference within the liver that alters the processing of bilirubin
– obstructions of the common bile duct, with the result that the liver cannot
excrete processed bilirubin into the bile
• Bilirubin normally excreted into feces (via bile) can be passed into
urine
• Icterus: yellow discolouration occurs first in sclera of the eye,
and then the skin
6. Splenomegaly
Spleen enlarges due to portal hypertension
• hypertension in portal vein causes shunting of blood into
the splenic vein
• Formed elements take longer to filter through the
enlarged spleen, leading to increased rate of
removal
• Result = anemia, thrombocytopenia, leukopenia
Disorders of the Liver
1. Viral hepatitis
– Five usual strains of virus: A, B, C, D and E
• All can cause acute hepatitis
• HBV and HCV can also cause chronic liver disease and liver cancer
– Acute hepatitis
• causes destruction of hepatocytes, scarring and hyperplasia of hepatic
macrophages
• if intrahepatic ducts are damaged, obstruction and jaundice can occur.
Damage is more extensive with HBV and HCV
– Co-infection with HBV, HCV, HDV and HIV can occur because
the route of transmission is the same (body fluids) = more rapid
progression of liver disease
– Diagnosis - test for specific type of hepatitis is based on
antibody assay
– Vaccine available for HAV and HBV
Acute Viral Hepatitis – clinical manifestations
Abnormal liver function test results (assay of compounds
released/affected by the liver)
• Disease typically progresses through 3 stages:
1. Prodromal phase = viral inflammatory effects: begins 2 weeks
after exposure and ends with jaundice. Marked by fatigue,
vomiting, headache, cough, low-grade fever. Very infectious during
this stage
2. Icteric phase = effects of liver damage: lasts 2-6 weeks. Jaundice,
dark urine, clay-colored stools, liver is enlarged and tender –
palpation causes pain
3. Convalescent phase = healing and repair: begins with resolution of
jaundice and most symptoms (about 6-8 weeks after exposure), but
liver remains large and tender. Liver returns to normal function 4-
14 weeks after onset
Chronic Viral Hepatitis
Persistence of clinical manifestations and liver
inflammation after acute stages of HBV and HCV
infection
– Virus persists in hepatocytes producing a prolonged
immune response, extending liver damage
– Liver function tests remain abnormal for >6 months and
HBV / HCV surface antigen persists
• Risk factor for cirrhosis and liver cancer
2. Cirrhosis
Irreversible fibrotic liver disease,
caused by direct damage and
inflammation
Many causes: HBV/HCV infection, excessive alcohol consumption,
prolonged exposure to drugs or toxins (hepatotoxin)
• A multiple system disease causing hepatomegaly, splenomegaly,
ascites, portal hypertension, hepatic encephalopathy and
esophageal varices
• Liver metabolism and liver structure are altered by blockage of
channels necessary for liver function
• No specific treatment: rest, vitamin supplements, good nutrition,
management of complications, (cessation of drinking, if applicable),
possible liver transplant (depends upon cause
3. Liver failure
• Most severe clinical consequence of liver disease – can
result from acute or chronic diseases
• The inability of the liver to perform its normal synthetic
and metabolic function as part of normal physiology
– 80-90% reduced liver function
Disorders of the Gallbladder
Cholelithiasis: formation of gallstones
• Cholecystitis: inflammation of the gallbladder- if
gallstones obstruct the outlet to the gallbladder
(cystic duct)
• Most gallstones are formed from cholesterol;
fewer are from bilirubin and calcium
• Gallstone formation is favoured by:
o abnormalities in the composition of bile (e.g., more
cholesterol excreted into bile)
o stasis of bile (gallbladder obstruction)
o inflammation of the gall bladder (causes excessive
absorption of water and bile salts)
Cholelithiasis: clinical manifestations
Often asymptomatic
• Abdominal pain and jaundice
• Pain occurs 30 min to several hours after eating a fatty
meal
– caused by the lodging of one or more gallstones in the cystic
or common duct
• Risk factors include:
• obesity, being female, bearing several children, contraceptive
pills (estrogen increases the excretion of cholesterol)
• Treatment may include endoscopic removal of
gallstones and/or gall bladder
Jaundice indicates that the stone is lodged in the
common bile duct since bile backs up into the liver
• Lodging of a stone in the cystic duct will cause
cholecystitis
Disorders of the Exocrine Pancreas
Acute Pancreatitis
Reversible inflammatory process caused by
premature activation of pancreatic enzymes
– Common manifestation: ongoing abdominal pain
– Outflow of pancreatic digestive enzymes is obstructed, causing:
1) accumulation of pancreatic secretions
2) pathologic activation of enzymes within the pancreas
3) results in autodigestion, leading to vascular damage, necrosis, edema,
inflammation
– Can develop into “severe-acute” form
• release of inflammatory cytokines into the bloodstream-> causes systemic
effects -> may lead to renal failure, respiratory distress syndrome
– Causes: gall stones or alcohol abuse
Disorders of the Pancreas Chronic Pancreatitis
Prolonged, progressive and irreversible destruction of the
exocrine and then endocrine pancreas
• Manifestations relate to loss of pancreatic function, and
the outcomes of chronic inflammatory processes
– Malabsorption, weight loss, diabetes mellitus
– Release of inflammatory cytokines into the bloodstream
→ systemic effects: nausea & vomiting, anorexia
• Risk factor for pancreatic cancer
• Most common cause is chronic alcohol abuse
Atherosclerosis
principally a disease the intima of arteries
• Fibrous fatty lesions form in large / medium sized e.g.
– aorta, femoral, carotid and
coronary
• Results in:
– increased wall thickness,
decreased elasticity
– reduced vessel radius → reduced
flow rate
– ischemia to supplied organ /
tissue
Etiology Atherosclerosis
• Rated to endothelial cell damage from, e.g.,:
– hyperlipidemia, cigarette smoke, immune mechanisms,
turbulent blood flow – which results in:
1. Increased endothelial permeability to plasma protein and lipids
that move into vessel walls
2. Migration monocytes and other leukocytes into sub-
endothelial layers
3. Monocytes differentiate to macrophages, which oxidize lipids
in LDL and ingest them transforming into lipid filled foam cells.
4. Macrophages release growth factors that proliferate smooth
muscle, ROS and other toxic substances damaging endothelial
cells
5. Progressive tissue damage and growth of plaque lesion.
Plaques harden.
Low density lipoproteins
A transport form of lipid in
blood
• LDLs are oxidized by ROS in
plaques and then
phagocytized by
macrophages
• The is a strong association
between high levels of
plasma LDLs and coronary
artery disease – as a result
of atherosclerosis
Predisposing risk factors for atherosclerosis
Elevated cholesterol (may be genetic)
• High blood pressure > endothelial cell damage
• Obesity
• Diabetes
• Smoking
• Sedentary lifestyle
Coronary artery disease (CAD)
Cause of ischemic heart disease
• Third of all deaths in
industrialized West
• Nearly all elderly have some
coronary impairment
• For health care professionals –
essential to understand
pathophysiology
Ischemic heart disease: IHD
a disease characterized by ischemia
(reduced blood supply) of the heart muscle,
usually due to coronary artery disease
(atherosclerosis of the coronary arteries)
Since coronary artery disease is the major
cause of ischemic heart disease, the two terms
are often used interchangeably
Coronary arteries
Left (main) and Right
• Both originate from aorta
• Main arteries on surface, deeper
branches penetrate muscle
Myocardial blood flow
Myocardial blood flow
• In strenuous exercise coronary blood flow 3-4X
• Nervous control of myocardial blood flow operates by two
mechanisms, producing vasodilation or constriction of
coronary blood vessels:
1. Autonomic control:
– Parasympathetic via vagus nerve
– Sympathetic: α receptors constrict
β receptors dilate
2. Local autoregulatory control
Myocardial blood flow: autoregulation
Local metabolism is a major control of myocardial blood flow:
vasoactive mediators of (such as adenosine and nitric oxide)
produce vasodilation or constriction of coronary blood vessels to
match metabolic / oxygen demands of cardiac muscle
Myocardial blood flow
Myocardial blood flow
In CAD Subendocardial regions of muscle are usually damaged
first as they have most difficulty obtaining adequate blood flow
When the ventricles contract
(systole) the muscle compresses
muscle capillaries, reducing blood
flow
Reduced flow is greatest in
Subendocardial regions (below the
endocardium): muscle here is
usually damaged first if the blood
supply is reduced
Lifesaving value of
collateral circulation
– many connections called
anastomoses exist between
smaller coronary arteries
– during acute ischemia the
anastomoses dilate within
seconds, providing an
alternative path for blood
flow
Atherosclerosis as a cause of ischemic heart disease
Pathogenesis
1. Cholesterol deposited beneath endothelium
of arteries
2. deposits invaded by fibrous tissue
3. deposits often become calcified =
atherosclerotic plaques
4. plaques protrude into vessel lumens
5. block or partially block blood flow
6. a common site for atherosclerotic
plaques is the first few cms of
coronary arteries
7. A gradual hardening and narrowing of the
coronary arteries can lead to angina pectoris
and eventually complete occlusion
(myocardial infarction
Angina pectoris
Stable angina
• Chest pain caused by transient myocardial ischemia
not severe enough to cause necrosis
• brought on through physical exertion/emotional stress
• Myocardial blood flow cannot respond to increased
demand for blood due to narrowing of one or more
coronary arteries by atherosclerotic plaque
In angina pectoris (and myocardial
infarction) pain radiates from the
sub-sternal region of the chest to
the jaw and down the arms.
Angina pectoris
Unstable angina
• The surface of a plaque experiences small disruptions,
leading to the development of small thromboses, which
cause periods of occlusion
• Very important to recognize unstable angina, as it may
predict eventual myocardial infarction
• requires immediate hospitalization for rest, observation
and treatment: oxygen, aspirin (reduce clotting), nitrates
(vasodilator), morphine
Differentiating between stable and unstable angina
Stable
plaque intact partially obstructing coronary artery
pain predictably brought on by physical exertion / emotional stress
symptoms last less than 15 mins
symptoms relieved by GTN (Glycerol trinitrate) vasodilator
effect of ischemia on myocardium are temporary no necrosis
Differentiating between unstable angina
Unstable angina
chest pain is sudden and unpredictable
chest pain is not in response to exertion or stress, but spontaneous
pain generally more severe and lasting longer than 20 mins
plaque movement or small thrombi formation » temporary ischemia
may lead to life threatening myocardial infarction MI
Acute Coronary Syndrome (ACS)
ACS represents a spectrum of ischemic heart
diseases: ranging from unstable angina to
myocardial infarction
Pain persists longer than 20 minutes
• Pain may increase in severity
• May have previous history of unstable angina as
risk factor
• Symptoms not relieved short acting vasodilators –
e.g. glycerol trinitrate (GTN)
• In most cases of unstable angina there is recovery
and the effects are temporary
Myocardial infarction
Immediate result of complete coronary occlusion
• Blood flow ceases in vessels beyond occlusion except for
small amount of collateral flow
• Produces acute ischemia in the myocardium supplied
and varying degrees of ischemic injury and necrosis
• The area of affected myocardium is said to be infarcted
• The overall process is called a
myocardial infarction or MI
Two important classifications of myocardial infarction
Prognosis depends on the degree of muscle damage:
• STEMI MI
– the clot lodges permanently in the vessel and the entire
thickness of the myocardium becomes ischemic
– this type of MI is associated with ST segment Elevation on
ECG “STEMI”
– Serious : requires immediate emergency intervention
• Non-STEMI MI
– sometimes thrombus disintegrates before complete tissue
necrosis: only sub endocardium affected
– sometimes transient ST elevation, then T wave inversion
General Manifestations of
Acute Coronary Syndrome
Abrupt onset
• Severe and crushing pain, usually substernal,
radiating to the left arm, neck, or jaw
• Gastrointestinal complaints (nausea and vomiting)
• Complaints of fatigue and weakness
• Tachycardia, anxiety, restlessness, feelings of doom
• Pale, cool, and moist skin
• A “silent MI” occurs when a person does experience
any symptoms or has atypical symptoms
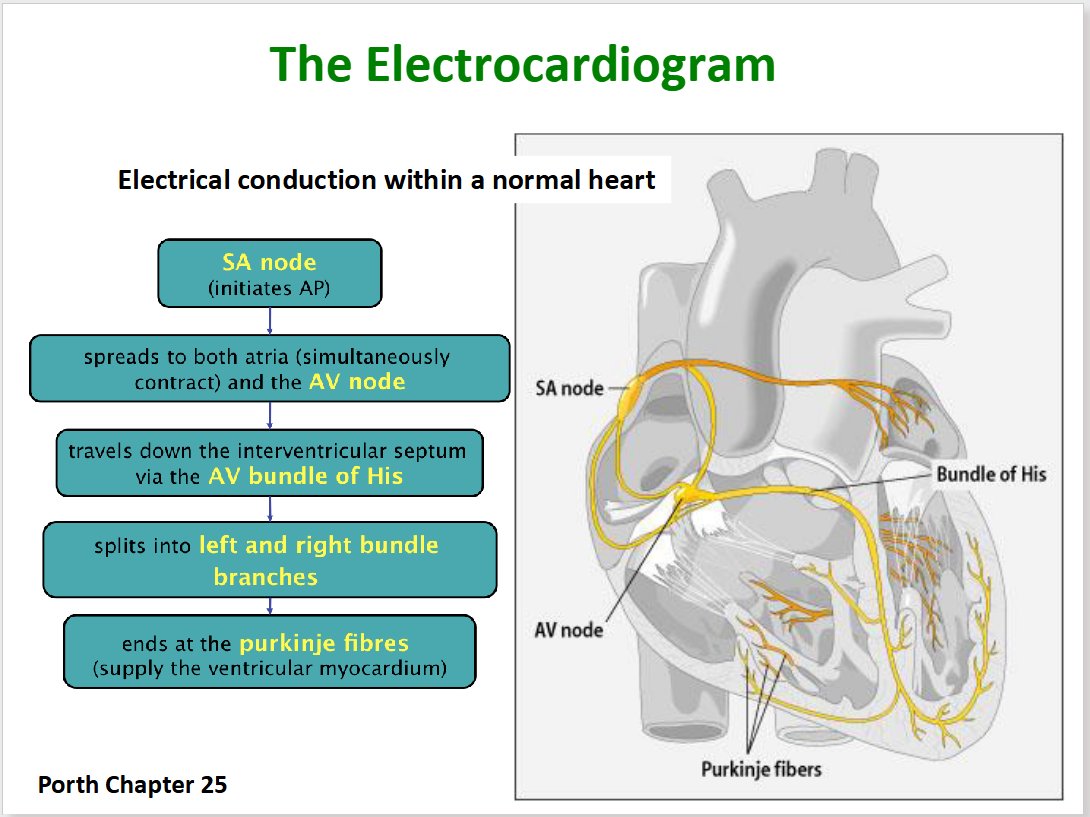
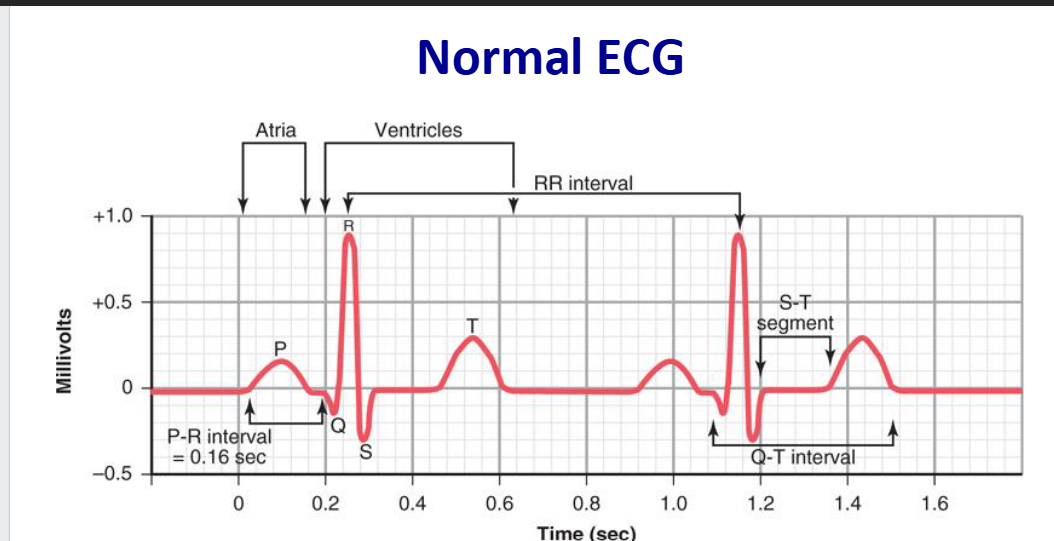
P wave: Atria depolarize
QRS complex: Ventricles depolarize
T wave: Ventricles recover from depolarization (repolarize
Types of normal ECG
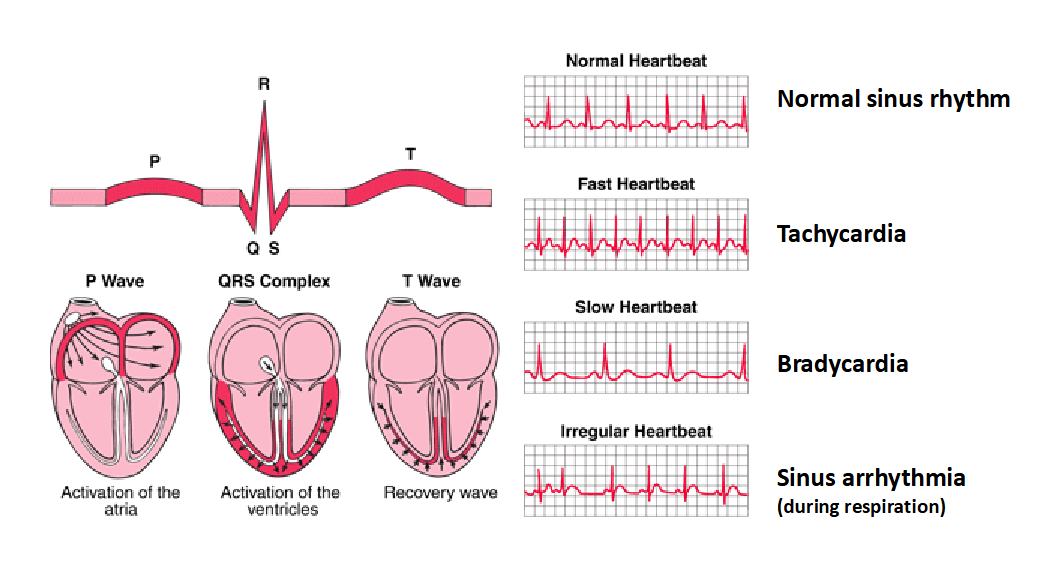
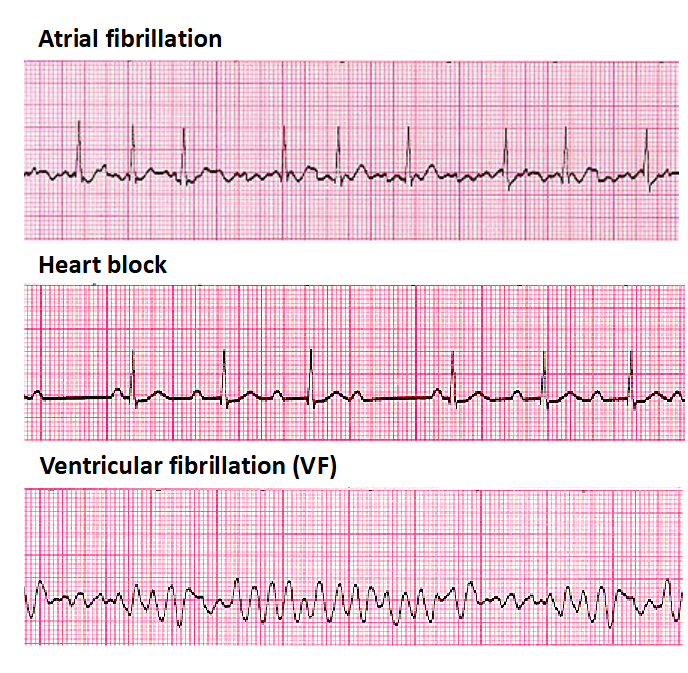
Some cardiac arrhythmias (abnormal ECG)
Many sites within the atria
are generating their own
electrical impulses, leading
to irregular conduction of
impulses to the ventricles
that generate the heartbeat
Not all atrial beats getting
through to the ventricles
Disorganized electrical
signals: ventricles quiver
instead of contract. Patient
unconscious as blood is not
pumped to the brain.
Immediate defibrillation is
indicated. May occur in MI.