Looks like no one added any tags here yet for you.
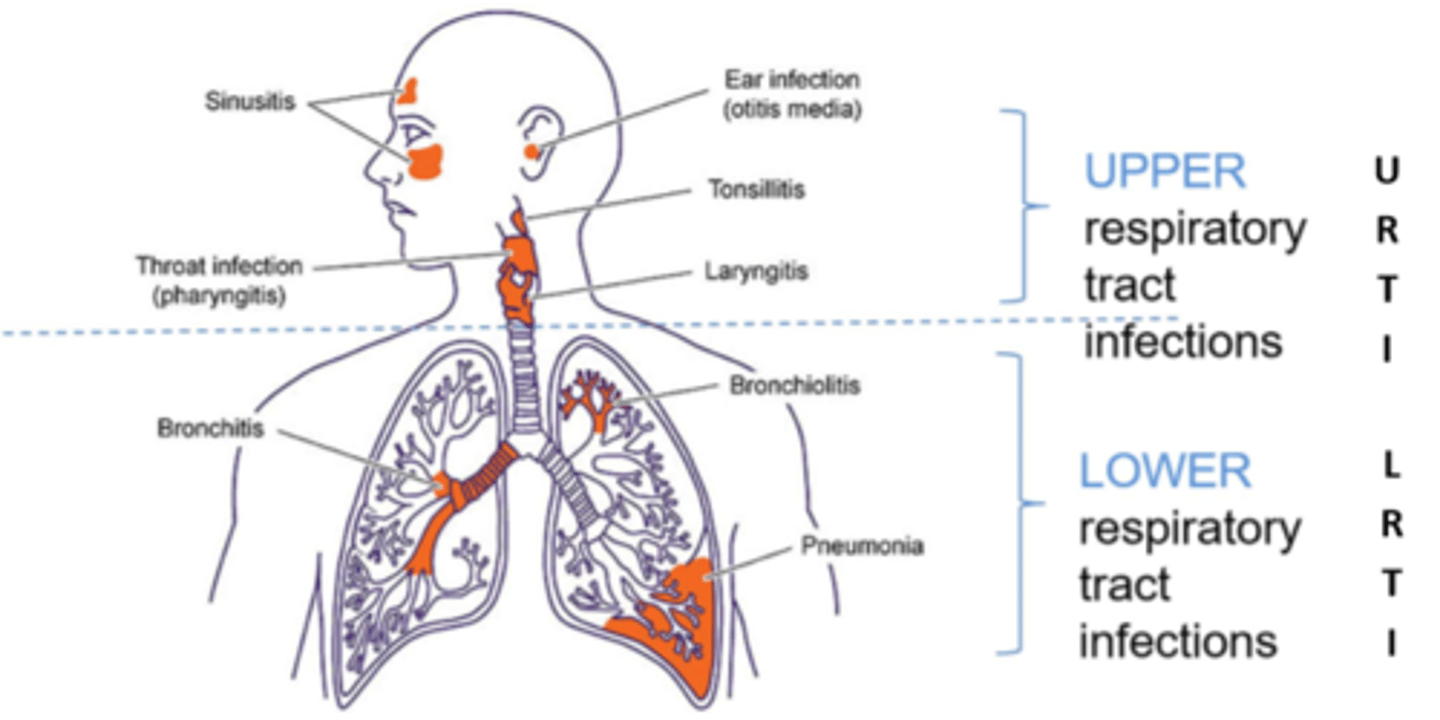
diagram of where is upper and where is lower
what are parts of the host defence?
mucus (trap microorganisms)
cilia (clear inhaled debris)
dendritic cells (antigen capture, T cell activation)
alveolar macrophages ( white blood cells, ingest and kill pathogens)
what are the parts of the upper respiratory tract?
nose, sinuses, pharynx, larynx and large airways.
what are the symptoms of upper respiratory issues?
cough, sore throat, nasal congestion, runny nose, headache.
what are the risk factors in upper respiratory tract diseases?
smoking, immune compromise, frequent exposure (e.g. childcare)
what the the viruses that causes the common cold?
rhinovirus
enterovirus
adenovirus
influenza
respiratory syncytial virus (RSV)
what is the cause of sinusitis/otitis media?
usually bacterial in nature
what can cause pharyngitis/tonsilitis?
bacteria - streptococcus pyogenes (GAS)
viruses - adenovirus, rhinovirus, influenza, herpes simplex, HIV, Epstein-Barr virus (EBV).
symptoms and sings of infectious mononucleosis?
lymphadenopathy
fever
pharyngitis
fatigue
myalgia
what is the most common cause of infectious mononucleosis?
Epstein Barr virus (EBV) - glandular fever.
where would inflammation be in the lower respiratory tract?
trachea, bronchi, bronchioles, alveoli.
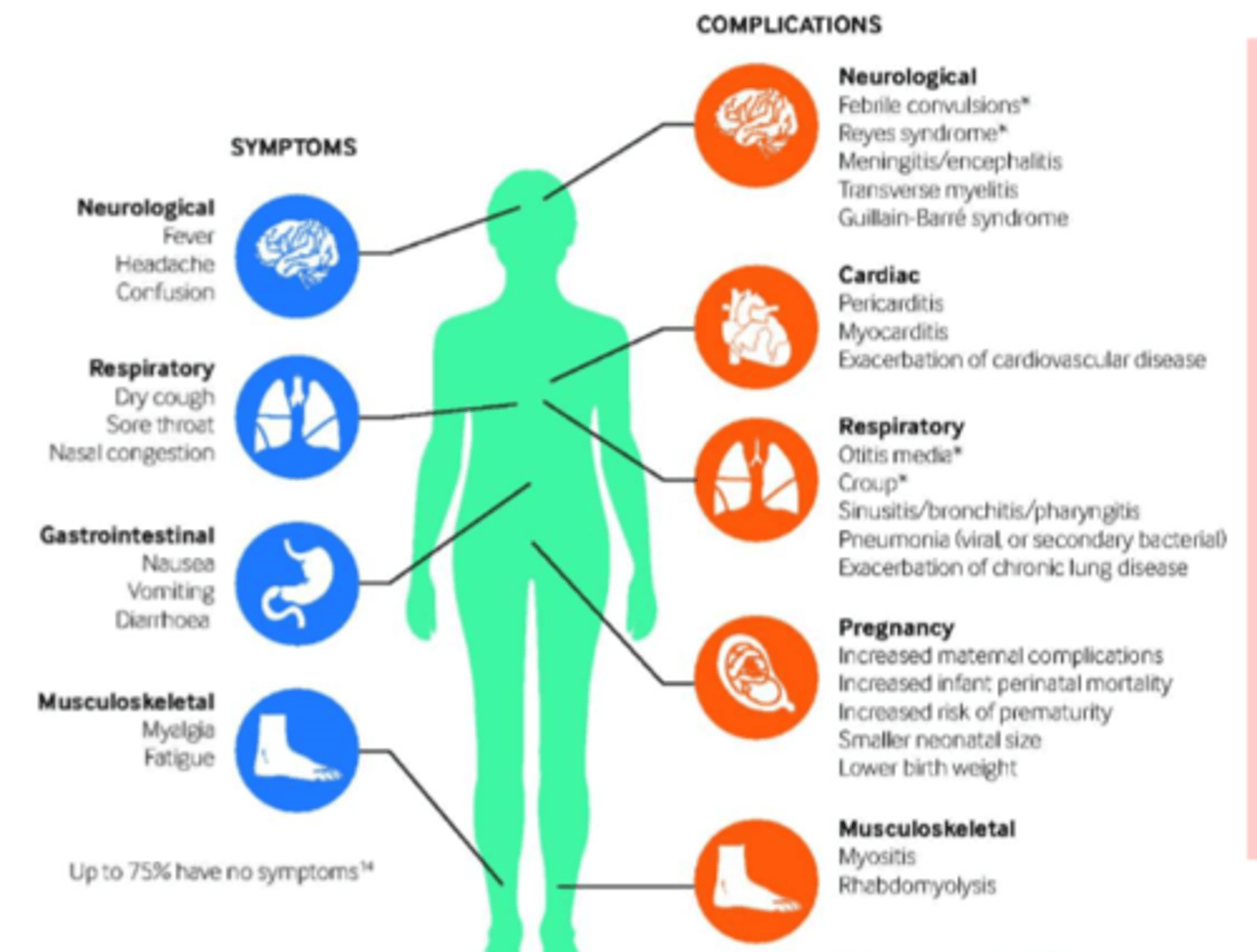
what symptoms of the lower respiratory tract infections are not respiratory related?
confusion, headache, myalgia, abdominal pain, vomiting and diarrhoea.
viral causes of lower respiratory tract infections?
influenza
respiratory syncytial virus (RSV)
SARS-CoV-2
Adenovirus
varicella zoster (VZV)
how to determine between upper and lower issues?
symptomology - non respiratory symptoms?
clinical examination - auscultation
radiological imaging - CXR, CT
what patient factors impact diagnosis?
age
immune status
vaccination history
infection control actions?
wash hands
cover mouth/nose = masks
cough cough/ sneeze
avoid close contact
clean/disinfect surfaces
what laboratory techniques are used for diagnosis?
nose/ throat swab
nasopharyngeal aspirate
bronchoalveolar lavage
endotracheal tube secretion/ aspirate
what are the 4 types of influenza virus?
influenzas A
influenzas B
Influenza C
influenza D
influenza A
Infect humans and many different animals. The emergence of a new and very different influenza A virus with the ability infect people and have sustained human to human transmission, can cause an influenza pandemic.
Influenza B
circulates among humans and cause seasonal epidemics. Recent data showed seals also can be infected.
Influenza C
can infect both humans and pigs but infections are generally mild and are rarely reported.
Influenza D
◦primarily affect cattle and are not known to infect or cause illness in people.
What type of virus is influenza?
enveloped, negative sense, segmented RNA virus
why can people be reinfected by some acute viral infections?
no or limited original immunity
loss of immunity
immune escape mechanisms (antigen drift/ antigen shift)
antigenic drift
via error prone replication (mutation)
more prominate in RNA.
mutation generally occurs at a similar rate across the genome but some residues tolerate nucleotides mutations better than others.
antigenic shift
via reassortment - segmented viruses.
influenza pathogenesis?
viral replication in epithelial cells.
multifocal destruction of epithelium of trachea and bronchi.
recruitment of pro inflammatory cells (neutrophils and macrophages).
airspaces fill with oedema, blood.
high risk groups for severe influenza?
children under 2.
adults of 65.
pregnant people.
immunosuppressed.
co-morbitities (asthma, heart disease, kidney disease ect)
BMI over 40.
influenza clinical presentation diagram
prevention of influenza?
live attenuated seasonal vaccine (children)
inactivated season vaccine (adults)
treatment of influenza?
neuraminidase inhibitors - oseltamivir, zanamivir.
cap-dependant endonuclear inhibitor - baloxavir.
how do neuraminidase inhibitors work?
inhibit the enzyme which enables the release of new viral particles from infected cells
how to cap dependant endonuclease inhibitors work?
inhibits viral replication.
oral single dose - not often used to to limited date and resistance development.
virology of RSV (respiratory syncytial virus)
enveloped, negative ssRNA.
10 genes encoding 11 polypeptides.
3 surface glycoproteins.
pathogenesis of RSV?
attachment to host cell via receptors.
fusion with cell membrane.
viral entry.
syncytia formation (cytopathic effect)
viral replication in cytoplasm.
spread to lower respiratory tract.
cell death - epithelial necrosis.
presentation of RSV in children under 2?
bronchiolitis.
short history cough, coryza, low grade fever.
symptoms peak after 3-5 days.
increased risk of asthma/wheeze later in life.
clinical presentation of RSV in adults
URTI.
viral induced wheeze.
acute exacerbation of asthma.
pneumonitis.
risk factors for RSV?
extremes of age.
congenital heart/lung disease.
infants born with low maternal antibody titre.
immunodefinaicancy.
smoke/ air pollution.
prevention techniques for RSV?
palivizumab (monoclonal antibody)
- directed against fusion protein
- only for kids
Nirsevimab (monoclonal antibody)
- directed against fusion protein
RSV vaccine (RSVpreF)
- mRNA and protein vaccines, all target fusion protein.
treatment for RSV?
Ribavirin - guanosine analogue that inhibits genome replication.
IVIG - mainly effective when given with ribavirin for immunosuppressed patients.
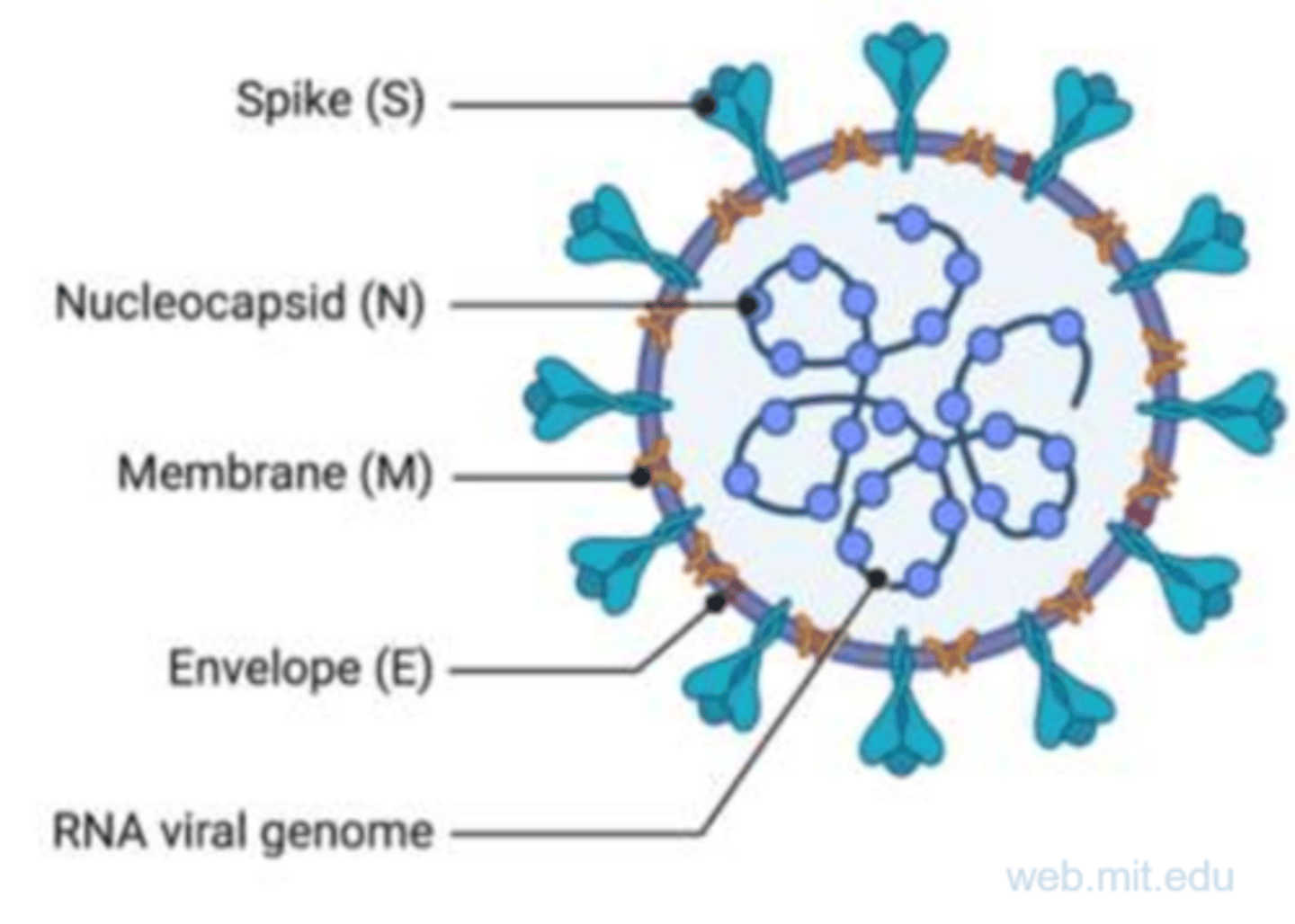
virology of SARS-CoV-2?
Spike - attachment protein
nucleocapsid - binds genome
membrane - coordinates assembly and morphology
envelope - small viroporin.
positive ssRNA genome.
How is SARS-CoV-2 transmitted?
respiratory droplets and aerosols.
what is the incubation period of COVID?
2-14 days (average 3-4), changes with each variant.
how does COVID invade cells?
receptors for SARS-CoV-2: angiotensin converting enzyme 2 (ACE2).
require co-expression of an enzyme (TMPRSS2) to enable function.
both upper and lower respiratory tract.
where does COVID replicate in host cells?
host cell cytoplasm.
what leads to cell death?
virion release.
damage to cells lining olfactory epithelium = loss of taste and smell.
asymptomatic presentation of SARS-CoV-2?
absence of symptoms and clinical signs of the disease, normal CXR, test positive for it though.
mild presentation of SARS-CoV-2?
URTI symptoms (cough sore throat), fever, malaise, headache, myalgia, nausea, vomiting, diarrhoea, anosmia.
No shortness of breath (dyspnea), or abnormal chest imaging.
moderate presentation of SARS-CoV-2?
Signs of lower respiratory disease during clinical assessment or on imaging, oxygen saturation measured by pulse oximetry (SpO2) ≥94% on room air at sea level.
severe presentation of SARS-CoV-2?
Individuals who have SpO2 <94% on room air at sea level, a ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO2/FiO2) <300 mm Hg, a respiratory rate >30 breaths/min, or lung infiltrates >50%.
critical presentation of SARS-CoV-2?
Individuals who have respiratory failure, coagulopathy, septic shock, and/or multiple organ dysfunction.
SARS-CoV-2 vaccine?
give to risk groups first (>65, pregnant, HCSW)
targeted against spike protein.
re-vaccination recommended due to antigenic drift/ mutation.
treatments for SARS-CoV-2?
antivirals - paxlovid/ remdesivir
anti-inflammatory - dexamethasone
supportive care - anticoagulation/ antibiotics.