Case 8: Thomas Gagnon - Asthma
1/37
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
38 Terms
Respiratory Epithelium
Ciliated pseudostratified columnar epithelium
Cells:
Ciliated Columnar: Apical cilia
Goblet
Brush: Apical microvilli, basal nerve endings (chemosensory)
Small Granule
Basal: Stem cells
Basement membrane
Lamina propria
Nasal Cavity Epithelium
Respiratory + olfactory epithelia
Pseudostratified columnar epithelium
Olfactory neurons
Supporting cells
Basal cells
Paranasal Sinuses: Thin respiratory epithelium
Less goblet cells
Pharynx Epithelium
Naso: Resp epithelium
Oro: Stratified squamous
Laryngo: Loose connective tissue + elastic fibres in lamina propria
Larynx Epithelium
Epiglottis: Stratified squamous epithelium → Resp epithelium
Vestibular Folds: Resp epithelium + seromucous glands + lymphoid nodules
Vocal Folds: Stratified squamous epithelium
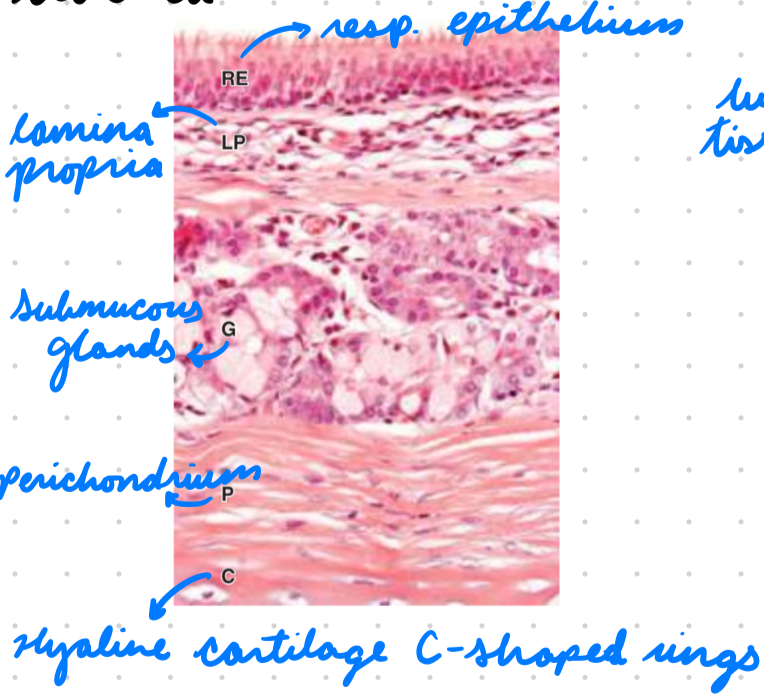
Trachea Epithelium
Resp epithelium
Seromucous glands produce mucus
Anterior: C shaped hyaline cartilages
Posterior: Trachealis smooth muscle (for esophagus expansion)
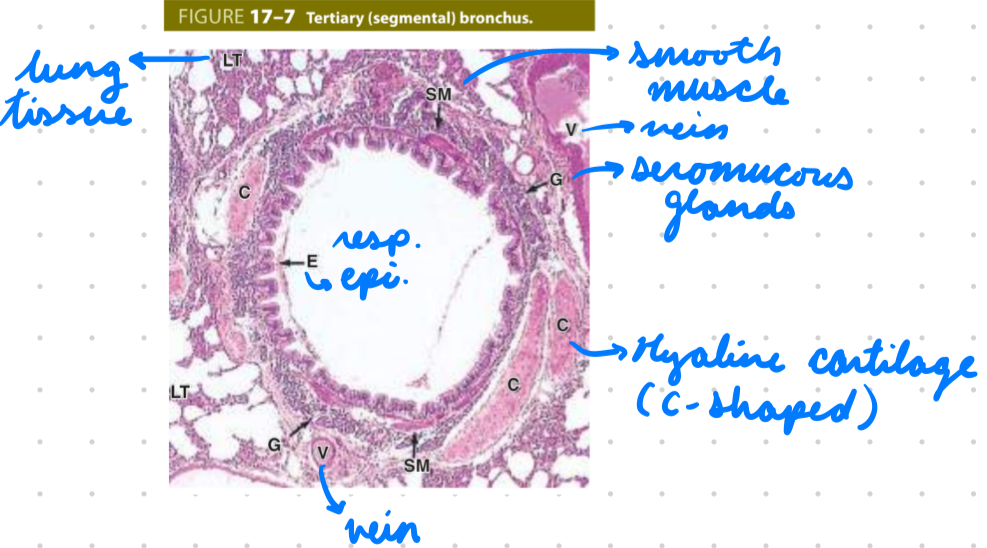
Bronchial Tree Epithelium
Primary Bronchi: Resp epithelium + cartilage rings
Mucous and serous glands
Smooth muscles
Elastic fibres
Other Bronchi: Resp epithelium + hyaline cartilage
Increase smooth muscles and elastic fibres
Bronchiole Epithelium
Resp epithelium
Connective tissue + smooth muscle
Terminal Bronchiole Epithelium
Ciliated simple columnar or simple cuboidal
Club Cells: Non-ciliated, contain secretory granules
Immune protection
Brush cells
Small granule cells
Alveoli Epithelium
Simple squamous epithelium
Smooth muscles, elastic, collagen
Type 1 and 2 pneumocytes
Resp membrane
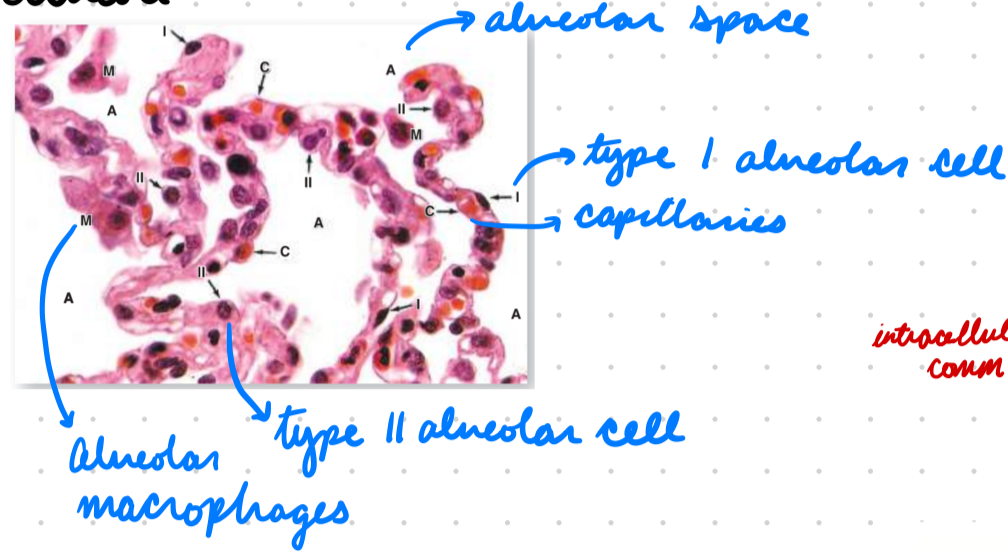
Alveoli: Alveolar Sacs
Thin elastic and reticular fibres
Alveoli: Interalveolar Septa
Between alveoli
Fibroblasts
ECM: Connective tissues (elastic and reticular fibres)
Alveoli: Resp Membrane
Blood-air barrier
Fused basal lamina (alveolar cell lining) and endothelial cells (capillaries)
Airway Epithelium Physiology
Clean and protect airway
Secrete mucus
Mucociliary clearance
Airway Goblet Cells Physiology
Secrete mucins (mucus)
Trap foreign particles
Mucociliary clearance
Airway Inflammatory Cell Physiology
Innate host defense
Release chemokines and cytokines
Phagocytosis
Airway Smooth Muscle Cell Physiology
Control airflow
Regulate contraction and relaxation
Secrete ECM proteins
Contribute to airway remodelling during disease
Factors Influencing Airway Diameter
ANS causing bronchoconstriction and bronchodilation
Smooth muscle hypertrophy
Airway wall thickness (inflammation, edema, mucus)
Lung volume (hyperextension = pull open airways)
Asthma: Description
Resp disease with chronic airway inflammation (hyperactivity)
Restrict expiration
Allergic and non-allergic
Asthma: Epidemiology
Risk Factors:
Perinatal/childhood exposures (resp infections, maternal smoking)
Environmental exposures (smoking, mold, farming)
NSAIDs
Genetics
Obesity
Asthma: Etiology
Bronchial hyper-responsiveness causing chronic inflammation
Asthma: Pathogenesis
Immune dysregulation = Persistent inflammatory and structural airway changes
Immune cells respond to antigen-induced alarmin molecules to recruit inflammatory cells and cytokines
Mast cells (histamine), eosinophils
Bronchoconstriction + airway obstruction = Low V = Low V/Q
Hypoxia
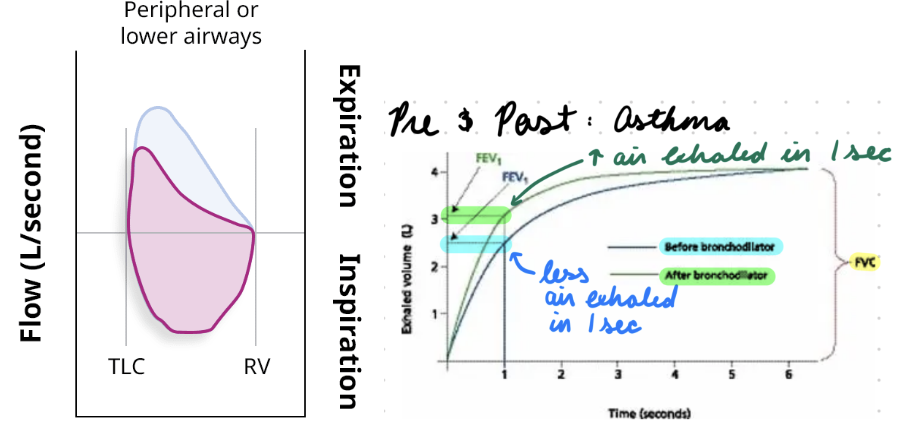
Asthma: Investigation
Spirometry:
Airflow obstruction (flow-volume loop scooping)
Pre- and post- bronchodilator administration
Peak Expiratory Flow (PEF):
Max speed when forcibly exhaling air
Supportive
NO IMAGING
Asthma: Clinical Presentation
Coughing and wheezing
Dyspnea
Chest tightness
Recurring symptoms
Worse at night
During exercise
With allergen exposure
→ GINA severity
Asthma: Treatment/Management
Step-wise approach
Increase management with severity + previous treatment response
Avoid allergens
Pharmacological
Exacerbations:
O2 administration
SABA + IV systemic CS
Asthma Treatment: Pharmacological
Inhaled Corticosteroids (ICS): Inhibit pro-inflammatory gene transcription
Short-Acting Beta-2 Agonist (SABA) and LABA: Bind beta-2 adrenergic receptors = Bronchodilation
Tachyphylaxis: Rapid tolerance from internalized receptors
Short-Acting Muscarinic Antagonist (SAMA) and LAMA: Prevent acetylcholine binding = Block PNS = Bronchodilation
Ab Therapy: Anti IgE and IL-5
Atopic Triad
3 conditions caused by allergen-triggered IgE mast cell activation
Commonly manifested together
Genetic predisposition
Asthma, atopic dermatitis, allergic rhinitis
Atopic Triad: Asthma
Type 1 hypersensitivity
Chronic airway inflammation
Initial Sensitization
Reexposure
Chronic
Asthma: Initial Sensitization
APC (dendritic cells) identify and load allergen on MHC II
APC present MHC-allergen to helper T-cells for activation
Th2 cells release chemical mediators = B-cells produce antigen-specific IgE
IgE bind receptors on mast cell and basophils
Asthma: Reexposure
Inhaled allergen bind IgE antibody on mast cells in bronchial lumen
Activate mast cell to release mediators (histamine, leukotrienes)
Induce bronchoconstriction and mucus production
Antigen binds IgE on mast cells in epithelium = Release more mediators
Induce bronchoconstriction and inflammation
Asthma: Chronic
Airway remodelling (decreased lumen) from:
Smooth muscle hypertrophy
Increased mucus glands
Epithelial detachment from basement membrane
Fibrosis
Atopic Triad: Atopic Dermatitis
Eczema: Chronic inflammatory skin disease
Atopic Dermatitis: Etiology
Epidermal barrier dysfunction (tight junctions)
Poor defense against pathogens and water loss
Atopic Dermatitis: Pathogenesis
Type 2 hypersensitivity
Filaggrin gene mutation = Increase water loss and pathogen penetration
Increase Th2 + cytokines = Increase IgE from B-cells
IgE bind receptors (mast cells) = Inflammatory skin response
Atopic Triad: Allergic Rhinitis
Hay Fever: Inflammation of nasal mucosa
Allergic Rhinitis: Etiology
Allergen exposure
Allergic Rhinitis: Pathogenesis
Type 1 hypersensitivity
Allergen exposure = Increase APC/dendritic cell presentation to T-cells
Increase Th2 cell activation = Increase IgE production from B-cells
IgE bind receptors (mast cells, eosinophils, basophils) = Release histamine (inflammation)
Allergies: Description
Abnormal immune response to harmless environmental stimulus
Allergies: Management
Avoid allergens
Anti-inflammatory therapy
Corticosteroids
Anti-histamines
Biologic therapy
Inhibit type 2 cytokine signalling