Chapter 22: 2nd and 3rd Trimester Obstetrics (13-42 weeks)
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
Pregnancy
By week 12, majority of organs are formed during 1 trimester and are located in final anatomic position; first trimester is termed trimester of differentiation and development and 2nd/3rd are referred to as trimesters of growth and maturation
Placenta
Sonographically visible at 10 weeks functions; functions as organ or respiration for fetus- exchange of gases
carbon dioxide is higher in fetal blood and moves into maternal blood
oxygen higher in maternal blood and moves into fetal blood
Circulatory surface allows nutrients/metabolic waste products to be exchanged in placenta
Placenta Volume
Can be used as accurate predictor for abnormal fetal outcome; in most normal cases, placenta should be approx. equal in thickness (in mm) to gestational age in weeks + 10mm; measuring placenta is not standard practice but most experts agree that it should not exceed 4cm
Grade 0 Placenta
Represents normal placenta; smooth chorionic plate; basal layer that is free of bright reflective densities; homogeneous; medium/low level echoes; may be interrupted by anechoic lacunae (small anechoic pools of maternal blood)

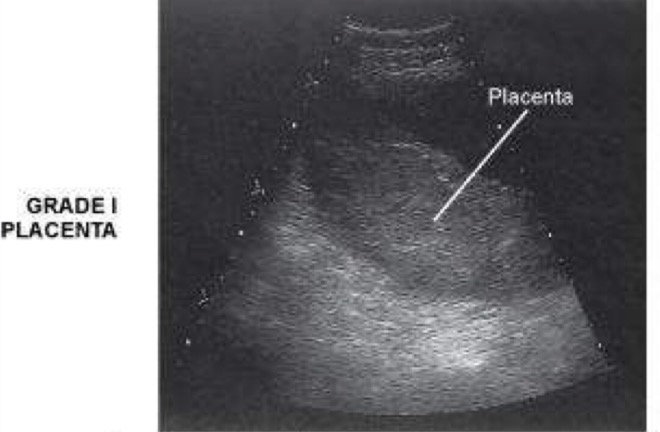
Grade 1 Placenta
Chorionic plate shows some subtle indentation; basal layer appears hypoechoic compared with placental substance; placenta exhibits a few scattered hyperechoic “calcifications”; normal changes at any time after 34 weeks of development
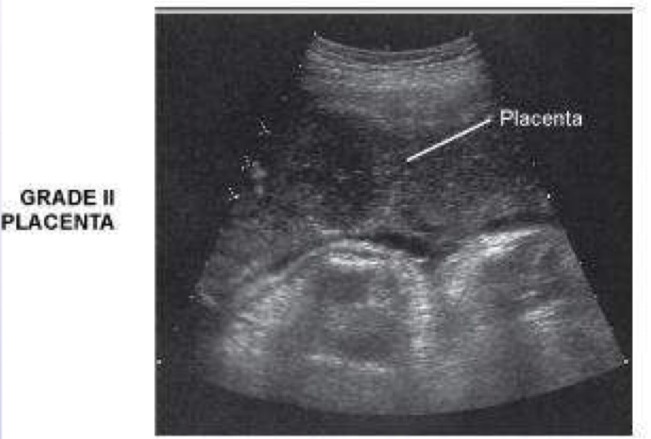
Grade 2 Placenta
Chorionic plate exhibits mild/medium sized indentations; basal plate contains few small bright linear densities; contains scattered “comma-like” densities (calcifications); normal at any time after 36 weeks of development
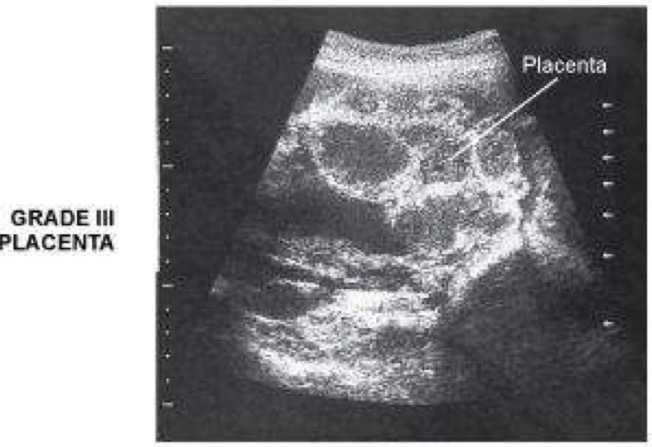
Grade 3 Placenta
Obvious indentations in chorionic plate that extend as far as basal layer- divides placenta into segments; basal layer of placenta has very long, linear, highly echogenic echoes; may contains both bright highly echogenic areas and anechoic areas; considered normal at any time after 38 weeks of development
Placenta Placement
Evaluate position of placenta within uterus relative to internal os of cervix to rule out placenta previa
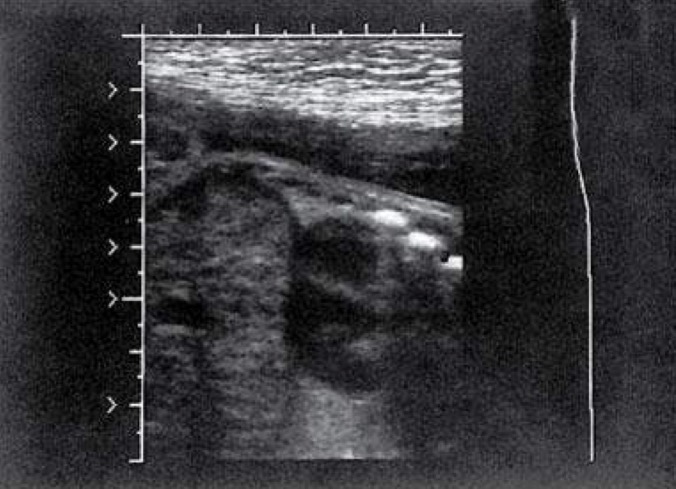
Placenta Previa
Any portion of cervical internal os is obstructed by placenta. risk factors are Hx of previa, prior c-section, ama, increased parity, smoking and enlarged placenta; 4 types of previa:
total or complete: occurs when entire cervical os is obstructed by an overlying placenta; associated with vaginal bleeding and necessitate cesarean delivery (in image)
partial or incomplete: occurs when portion of cervical os is obstructed by overlying placenta; associated with vaginal bleeding and necessitates cesarean delivery
marginal: placenta extends up to but not above the internal cervical os; follow-up exams during final weeks of pregnancy to see whether position of placenta has changed
low lying: occurs when placentas lower edge lies within 0.5-5cm from internal cervical os; in follow-up ultrasound exams, placenta frequently appears to move farther from internal cervical os

Amniotic Fluid Volume (AFV)
Amount of amniotic fluid in amniotic cavity is determined by:
maximum vertical pocket
use 2cm as minimum normal amount
Amniotic fluid index (AFI)
sum of 8 to 25 cm is considered normal
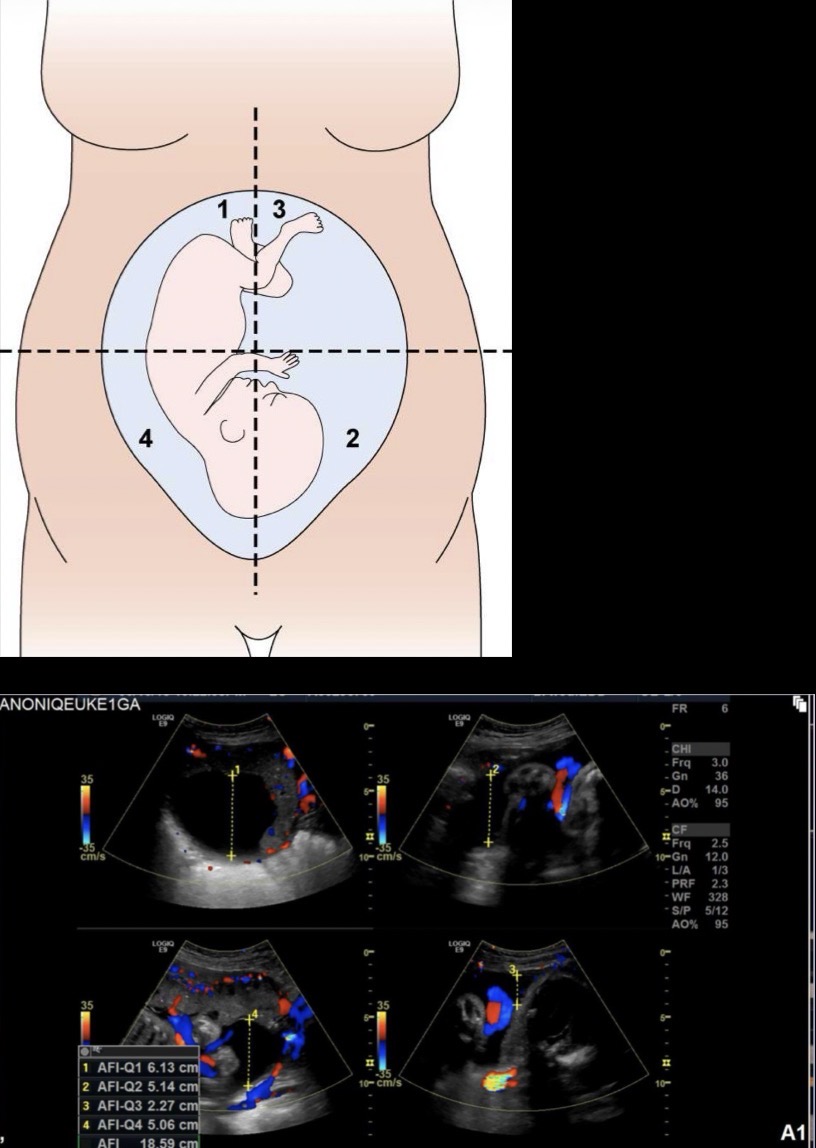
Amniotic Fluid Index
Gravid uterus is divided into 4 equal quadrants; AP diameter of deepest amniotic fluid pocket free of cord and extremities is measured in each quadrant; these 4 measurements are added together to determine the AFI (sum of 8-25cm is considered normal)
Musculoskeletal System
Bright reflection of fetal skeleton is indicated of degree of mineralization that has taken place within developing bones; density of bone attenuates sound waves, preventing through transmission
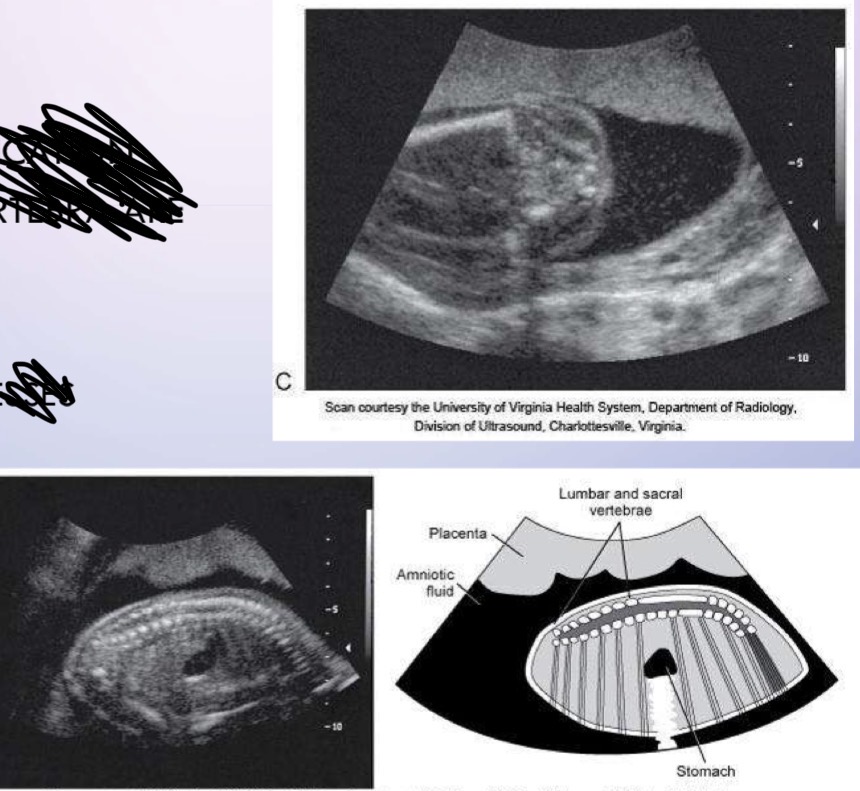
Spine
3 primary ossification centers of each vertebra are sonographically distinguishable
transverse processes
pedicles
laminae
Ribs
Bright echogenic appearance of fetal rib cage stands out against the mid/low gray of lungs and heart muscle
Skull
In almost all normal cases, the mandible, bony nasal ridge, and orbits can be visualized

Extremities
Upper and lower extremities identified; measurements of femur/humerus and hands/feed

Muscles
Normal fetal muscles appear very low gray on ultrasound; some muscles may appear anechoic especially in abdominal wall, where they can mimic appearance of ascites

Cardiovascular System
Umbilical cord: one vein and 2 arteries
umbilical vein carries oxygenated blood from placenta to fetus, where it connects with left portal vein on liver
umbilical arteries carry deoxygenated blood from fetal circulation to placenta
Ductus venosus, which shunts oxygenated blood into the IVC
Following birth: umbilical vein closes off and eventually becomes ligamentum teres
Shortly before birth: ductus venosum closes and becomes fibrous ligamentum venosum
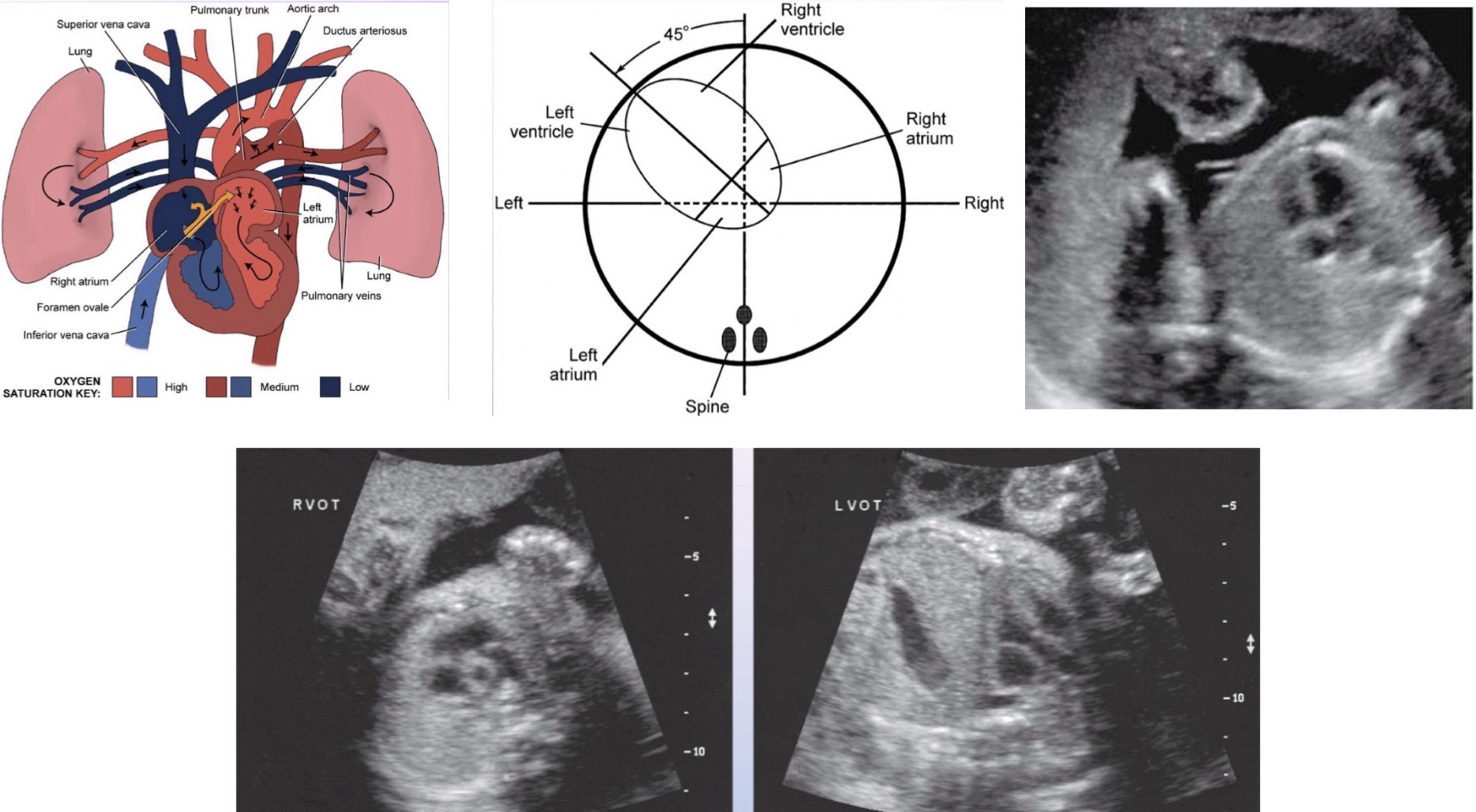
Fetal Heart
2 unique features unique to fetal heart
Foramen ovale: opening between atria of heart and allows blood to move from right to left atrial chamber
Ductus arteriosus: connects pulmonary artery and aorta and allows blood to move from pulmonary artery to aorta; closes at/shortly after birth
Axis of heart should be tilted approx. 45 degrees to anteroposterior axis of fetal thorax and pointed to left (second image)
4-chambered view of fetal heart may be seen as early as 15 weeks; chambers should appear anechoic and relatively symmetric, divided by bright atrioventricular septa (should be “broken” only as foramen ovale)
4th image is fetal heart outflow tracts
Respiratory Rate
Primitive lungs mature and become capable of functioning sometime after 25 weeks of gestation; lecithin-to-sphingomyelin ratio (LS ratio) measures ability of lungs to function; lings appear homogeneous, mid-gray echogenicity
Diaphragm: appears slightly concave with cuplike portion opening toward abdomen and arched position pointing toward thorax; it is not unusual to see diaphragm move with fetal respiration, especially during latter half of 3rd trimester

Gastrointestinal System
Foregut divides into esophagus, stomach, and duodenum in week 5; liver, gallbladder, pancreas, and sleep arise as diverticula from primitive alimentary tube; midgut splits into remainder of small bowel, ascending colon and portion of transverse colon; hindgut differentiate into remainder of transverse colon, descending colon, and rectum
Stomach
Size of stomach is variable and depends on amount of amniotic fluid swallowed by fetus; appears as anechoic structure on left side of fetal abdomen
Liver
Site of production of red blood cells; proportionately much greater in size in fetus than in adult; demonstrates as a homogeneous, mid-gray structure on right upper quadrant

Gallbladder
May be difficult to visualize after 32 weeks of gestation; it is thought that it contracts, releasing bile, as a result of initiation of gallbladder function; appears as anechoic structure on right side of fetal abdomen

Pancreas
Major parenchymal organ of gastrointestinal system; rarely visualized on ultrasound; pancreas may appear hyperechoic relative to adjacent structures and is visualized lying between anechoic fluid-filled stomach (posterior wall) and anechoic splenic vein
Spleen
Between 12-24 weeks of gestation, spleen functions as hematopoietic organ; sonographic appearance comparable to fetal liver (mid-gray and homogeneous with indistinct margins during early development

Small/Large Bowel
Normal to see small amount of anechoic fluid within small bowel and brighter areas in meconium; collapsed fetal colon typically appears hypoechoic relative to adjacent structures

Genitourinary System
Fetal genitourinary system consists of kidneys, ureters, urinary bladder, urethra, and genitalia; following 16th week of gestation, majority of amniotic fluid arises from fetal urination; normal amount of amniotic fluid implies presence of at least one functioning kidney
Kidneys
consistent recognitiion of fetal kidneys begins during 20th week; homogeneous moderate to low in echogenicity cortex; common to visualize urine-filled, intrarenal collecting structures

Urinary Bladder
By 15 weeks of menstrual age, over 90% of all normal fetal urinary bladders can be visualized; visualization is necessary to establish renal function; anechoic structure with thin hyperechoic wall in midline of pelvis; may increase and decrease in size during exam

Genitalia
Determination of fetal gender depends on visualization of either male scrotum or female labia; assignment of gender should not be made on basis of presence or absence of a fetal penis

Adrenal Glands
Triangular-shaped adrenal appears to “cap” upper renal poles; appease as low-gray organ that is typically hypoechoic relative to liver, spleen, and renal cortex

Central Nervous System
Consists of brain and spinal cord; brain is composed of 3 elements: brainstem, cerebrum, and cerebellum; meningies surround the spinal cord and brain structures; brain and spinal cord have elaborate system of circulation, ventricles, cisterns, and sinuses
Cerebellum
Composed of 2 lateral hemispheres and small central lobe, the vermis; on ultrasound, cerebellar vermis often appears as bright, reflective live dividing homogeneous, low-gray cerebellum

Ventricles
4 ventricles: 2 lateral ventricles (choroid plexus) and 3rd/4th ventricle; except for areas containing choroid plexus, ventricles are anechoic

Biparietal Diameter (BPD)
Transducer must be perpendicular to parietal bones and positioned to intersect 3rd ventricle and thalami; measure from outer anterior edge to inner posterior edge of calvarial wall (important to recognize correct plane of section to obtain accurate and consistent measurements of BPD)
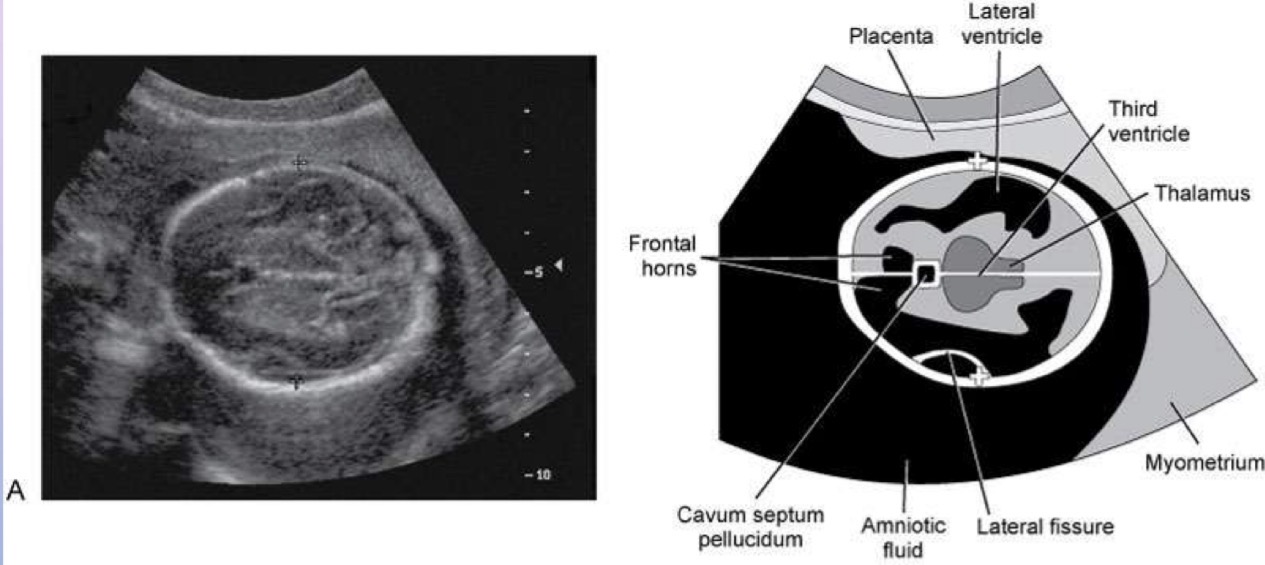
Head Circumference (HC)
Perpendicular to thalami, 3rd ventricle, and cavum septum pellucidum and tentorium; measurement is made from outer to outer edge of calvarial wall

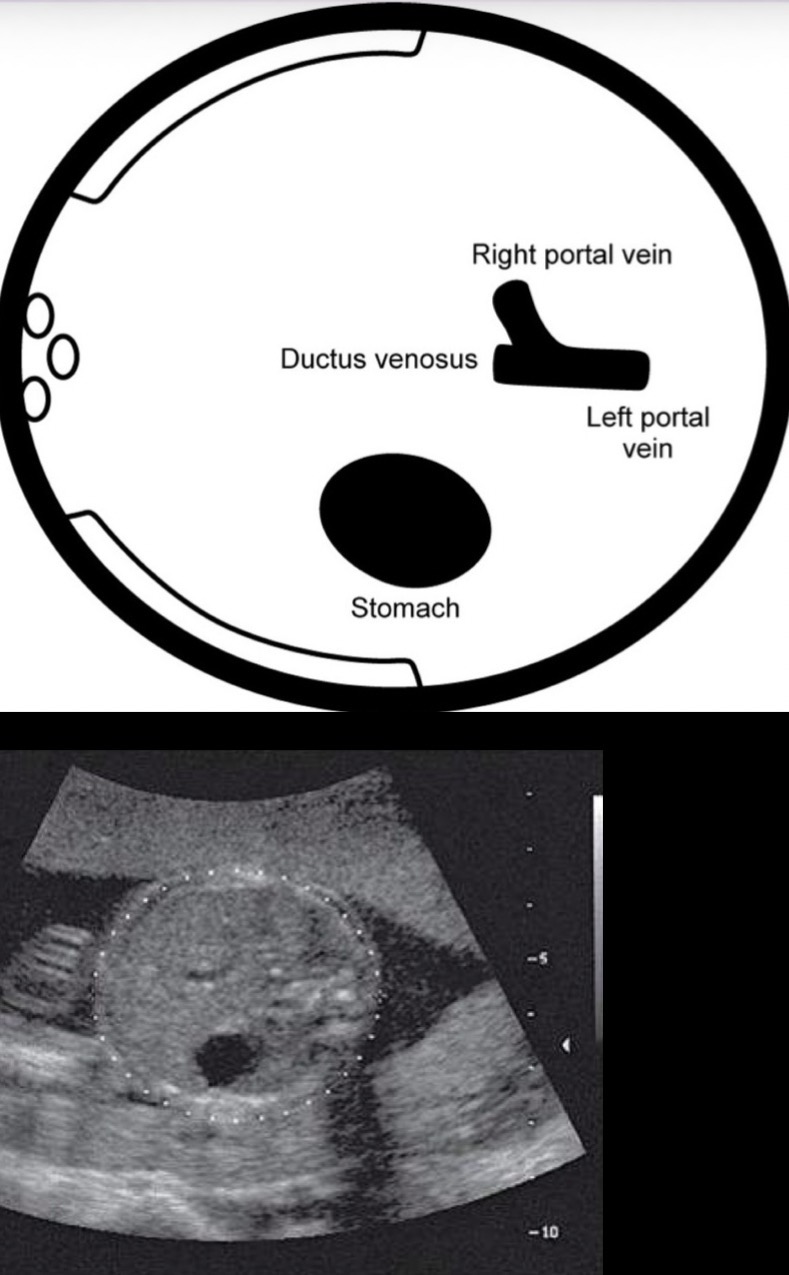
Abdominal Circumference (AC)
Axial section of fetal abdomen, where umbilical vein branches and right and left portal veins are continuous with one another; elliptical measurement cursor is fit to the skin edge (important to recognize the correct plane of section to obtain accurate and consistent measurements of AC)
Femur Length
Plane of section is long axis of the bone; measurement cursors are placed at bone cartilage interface; hypoechoic cartilaginous ends of femur are not included in measurement

Myometrial Contraction
Frequently seen on sonograms; distinguishable by their inward bulge, which does not ditrub uterine contour, and their temporary nature
Sonographic Applications
Indicated for gestational age (GA),fetal number, fetal growth, fetal presentation, discrepancy between size and dates (small/large for dates), vaginal spotting/bleeding, substance abuse/prescription drugs in pregnancy, abdominal/pelvic pain, trauma (to determine fetal wellbeing), Hx of congenital anomaly, incompetent cervix, abnormal biochemical markers, evaluation of amniotic fluid, or suspected fetal death
Normal Variants
Lemon Sign: appears as bilateral, frontal, concave scalloping of calvaria
Prominent Cisterna Magna: in absence of another malformation, this is normal finding
Choroid Plexus Cyst: in absence of other malformation, this is normal finding that usually resolves by 24-26 gestational weeks
Cavum Vergae: normal prominent posterior continuation of cavum septum pellucidi, which may simulate a dilated 3rd ventricle or arachnoid cyst
Fetal Hair: commonly seen in 3rd trimester and should not be mistaken for calverial mass or scalp edema
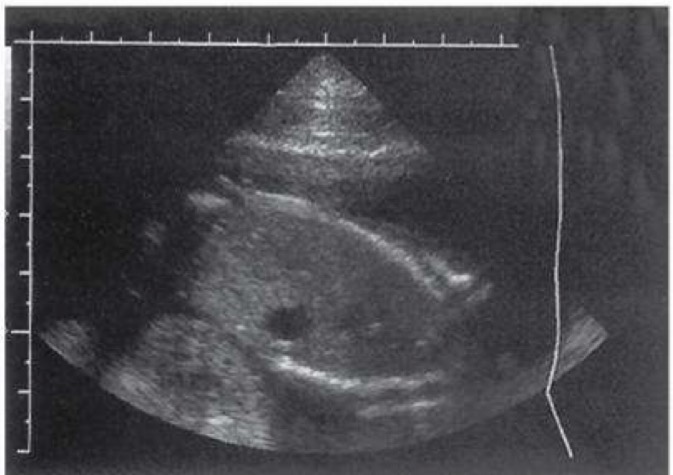
Prominent Cardiac Moderator Band: normal enlargement or prominence of moderator band can simulate ventricular thrombus or neoplasm
Echogenic Intracardiac Focus (EIF): seen as small bright echo focus in the heart on a 4-chamber heart view; if EIF is seen in isolation in a normal pregnancy, it is considered a normal benign variant; EIF’s are seen in 4-5% of normal pregnancies (what is shown in image)

Related Tests
Pregnancy Test: detects human chorionic gonadotropin (hCG) levels in urine or blood when pregnancy exists
Beta-hCG Test: blood is tested to quantitate serum level of hCG to estimate gestational age
Maternal/Parental blood typing: determines blood type and whether rh factor is positive or negative
Antibody Screen: blood test for rh factor, which is a group of autoantibodies that react with a persona own immunoglobulin
Glucose Screen: blood test for diabetes between 24-28 weeks of gestation
Amniocentesis: transabdominal/transcervical penetration of uterus and amniotic sac for aspiration of sample of amniotic fluid used for obtaining pertinent genetic information regarding fetus
CT: eval of fetal/maternal anatomy when sonographic eval is indeterminate; generally used as last resort because of radiation; most cases, use is limited to assess acute maternal abdomen
MRI: traditionally used to eval maternal anatomy during pregnancy and abnormalities such as adnexal masses, which require further characterization beyond the ultrasound findings; MRI eval of fetus is hindered by fetal motion
Lab Values
Alpha-Fetoprotein (AFP): found in maternal blood and amniotic fluid; elevated levels indicate fetal abnormalities or defects
Lecithin-to-Sphingomyelin Ratio (LS ratio): found in amniotic fluid; measures degree of fetal lung development
Triple Marker Screening (AFP,uE3, hCG): abnormal levels of AFP; unconjugated estriol (uE3); hCG are indicators of certain embryonic/fetal abnormalities, possible multifetal gestations, and (combined with maternal age) screening markers for downs syndrome