c-spine mobility
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
54 Terms
neck pain w/ mobility deficits - common sxs
- neck pain (central or unilateral)
- ROM and mobility restrictions
- shoulder girdle or UE pain may be present
neck pain w/ cervicogenic headache - common sxs
- Non-continuous unilateral neck pain and associated headache
- headache increased by neck movements or sustained positions
for OA and AA joints, SBing and rotation are coupled [ipsilateral/contralateral]
contralateral
primary motions of OA joint
nodding - flexion/extension (keep eyes level during rotation)
primary motions of AA joint
rotation (attempts to keep head facing forward during sidebending)
OA convex/concave
convex condyles on concave C1 (roll and glide opposite)
R SB at OA & couple movement
roll right, glide left
AND
coupled L rotation R ant, L post
AA convex/concave
convex atlas on convex axis
AA movement during R rotation
- R C1 rolls and glides posterior, inferior
- L C1 rolls and glides anterior, inferior
mid/lower cervical spine includes
C2-7
during flexion, facets are moving
superior, anterior (upglide/opening)
during extension, facets are moving
posterior, inferior (downglide/closing)
in mid/lower cervical spine, sidebending and rotation are coupled [ipsilateral/contralateral]
ipsilateral
in mid/lower c-spine, R rotation = R SBing. what's happening at the facets?
Right: inferior, medial, posterior (IMP)
Left: superior, anterior, lateral (SAL)
what's happening in upper c-spine during retraction?
flexion (roll ant, glide post)
observation - anterior
- head orientation relative to trunk and shoulders
- facial asymmetry
- bruising, swelling
- abnormal skin color
- incisions
- pupil size differences (CNS lesion)
- ptosis
observation - posterior
- head orientation relative to trunk and shoulders
- incisions
- muscle tone/symettry
- scapula position
observation - lateral
- assess cervical and thoracic curve
- CT junction
- FHP
- head on neck
- neck on thorax
- sitting posture
hypothesis with gross loss of rotation vs sidebending
- rotation = upper c-spine
- side bending = lower c-spine
if you have gross rotation ROM loss then what should you text next?
- protraction (ext)
- retraction (flex)
if there is no significant change in ROM when you do protraction and retraction then what should you suspect?
AA dysfunction
if retraction is more limited suspect
ipsilateral posterior OA joint
if protraction is more limited suspecr
contralateral anterior OA joint
if they have an opening restriction they will have painful and/or restricted...
flexion, contralateral SBing rotation
If they have a closing restriction they will have painful and/or restricted...
extension, ipsilateral side bending and rotation
c-spine capsular pattern
- equal limitation of rotation and SBing
- limited extension
- full flexion
upper trap ML
- flexion
- contralateral side bending
- ipsilateral rotation

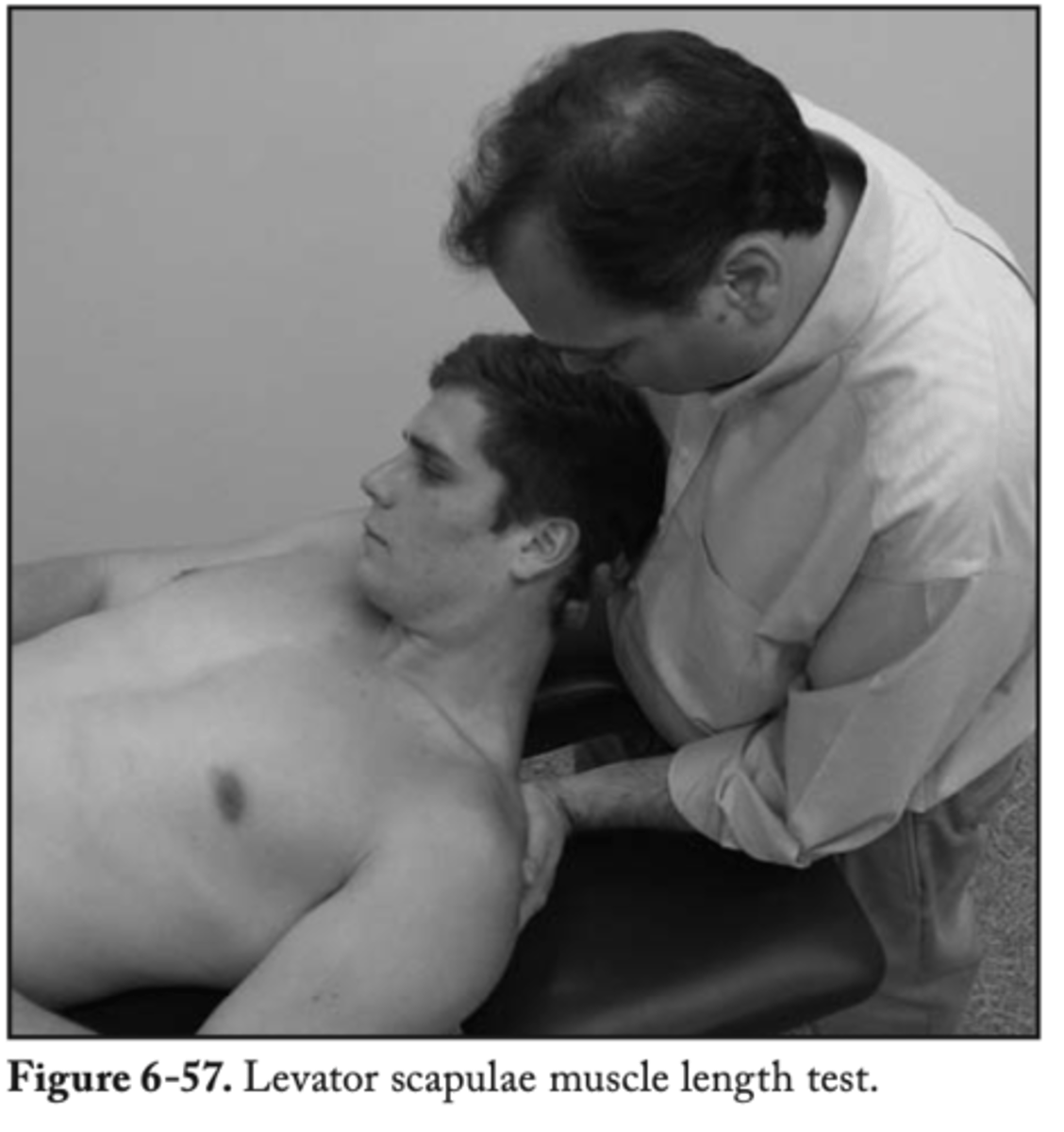
levator scap ML
- flexion
- contralateral SB & rotation
SCM ML
- contralateral SBing
- extension
- ipsilateral rotation

scalenes muscle length
- contralateral SB
- extension

OA jt assessment - left side tilt and right translation tests
- anterior glide of left OA jt
- posterior glide of right OA jt
OA jt assesment - right side tilt and left translation tests
- anterior glide of right OA jt
- posterior glide of left OA jt
OA jt assesment PPIVM
- pt supine
- put them into either flexion or extension and sidebend and translate
OA jt assessment PAIVM
- pt prone
- PT thumb on lateral mass of C1
- apply anterior force toward patient's ipsilateral eye
AA PPIVM - CFRT
- pt SUPINE
- full cervical flexion, palpate posterior arches of C1, then introduce cervical rotation
- feel for when C1 stops rotating on the contralateral side of the rotation

AA PAIVM
- pt prone with head and neck rotated 30 degrees TOWARD SIDE BEING TESTED
- PT thumb contact at TP of C2
- apply anterior force toward pts mouth
*check anterior: push contralateral C1 anterosuperior
mid/lower c-spine PPIVM
- pt supine
- perform lateral glides to one side first, then the other
- lateral glide induces relative sidebending to the opposite side of the translation force
(L lateral glide = R SBing)
mid/lower c-spine - flexion hypomobility testing
- pt supine
- head and neck flexed w/o allowing a chin tuck
- maintain flexion while producing segmental lateral glide, allowing the head and neck to sidebend
with flexion hypomobility testing, if there's restricted L SBing in flexion, that indicates...
loss of flexion on the right side of the segment (R opening restriction)
mid/lower c-spine - extension hypomobility testing
- pt supine, occiput cupped by PT
- maintain extension by pushing the superior vertebra anteriorly while producing segmental lateral glide
with extension hypomobility testing, if there is restricted L SBing in extension, that indicates
loss of L side extension (L closing restriction)
if resistance occurs before pain then what grades of mobs are indicated?
3 and 4
mid/lower cervical PAIVM
- pt prone
- PT standing at head of bed
- central: both thumbs on TP or SP of same vertebra and apply anterior force
- unilateral: thumb over thumb at TP
Pt has left side suboccipital pain and HA. The pt has a gross loss of L rotation. What are 4 possible joint dysfunctions?
1. L posterior OA
2. R anterior OA
3. L posterior & inferior AA
4. R anterior & inferior AA
Pt has left side suboccipital pain and HA. The pt has a gross loss of L rotation. If L rotation improves with protraction and worsens with retraction what is your hypothesis?
L posterior OA
if a pt has a L posterior OA what PPIVM and PAIVM would you do?
- PPIVM: flexion and R SBing
- PAIVM: C1 L TP (C0 goes posterior)
what should you do for pts with acute neck pain w/ mobility deficits?
- neck ROM
- scapulothoracic and UE strengthening
- cervical mobs
- SNAGs
what should you do for pts with subacute neck pain w/ mobility deficits?
- neck and shoulder girdle endurance exercises
- cervical mobs
- SNAGs
what should you do for pts with chronic neck pain w/ mobility deficits?
- cervical mob
- stretching & strengthening for cervical/scapulothoracic regions
- neck, shoulder girdle, and trunk endurance exercises
OA flexion mob
- PT standing at head of pt with hands around ears and thumb over zygomatic arch
- apply posterior force through pts zygomatic arch or jaw
ex: posterior problem on R --> side tilt L, translate R, rotate R
AA mob
- PT applies full cervical flexion to lock out lower c-spine then adds in rotation
- mobilizing hand at posterior arches of C1
- push anterior towards pts mouth
cervical upglide mob
- restriction in opening (flexion, contralateral SBing & rotation)
- pt supine, translate lateral
- apply anterosuperior force toward the pts contralateral eye
ex: opening problem on the R --> flex and translate R then push anterosuperior on R
cervical downglide mob
- restriction in closing (extension, ipsilateral SBing and rotation)
- pt supine, translate medial
- apply posteroinferior force toward the pts contralateral hip
ex: closing problem on the R --> ext segment and translate L then push posteroinferior on R
SNAGs
sustained nautral apophyseal glides
