NR 283 Final Exam (2026 2027)||| questions and answers with rationales/graded A+/2026 update/100% correct /instant download
1/138
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
139 Terms
What regulates the release of hormones?
feedback systems
Positive Feedback
tells a hormone to make more
Negative Feedback
stops making a hormone
Secreting Cells
what is pumped out of the cells (ADH released from the posterior pituitary gland)
Receiving Cells
what cells the hormones target (ADH targets the kidney)
Why are hormones are released?
-altered cell environment (increases intake of glucose leads to a release of insulin)
-maintaining levels of other hormones (cascades trigger the release of other hormones, ex: TRH)
-neural control (autonomic NS - not in control)
Non-steroidal hormones
-water soluble, can float around blood stream with no issues since the blood stream is made up of water, but cannot get through phospholipid bilayer - which is why we need receptors on the cells and second messengers (proteins that live inside the cells to help get the message to the nucleus)
-ex: insulin: freely moves around bloodstream but has to connect with a second messenger
Steroidal Hormones
-lipid soluble, fatty hormones floating around bloodstream cannot float around easily so they need carrier proteins to carry them. When they get to the cell, they dont have any issues getting into the cell they can deliver the message straight to the nucleus
ex: sex hormones (estrogen, testosterone)
regulation
refers to the receptivity of cells, how open is that cell to allow a hormone in
Upregulation
if we starve a cell of a hormone, they will be much more likely to get a hormone in
-this is why type II diabetes can be reversible, if the cells haven't seen insulin in a while, the pancreas isn't overworking to pump out insulin
Downregulation
-happens with type II diabetes, have tons of glucose in bloodstream, in response the pancreas (beta cells) pump out insulin, in a normal state the pancreas is able to pump out insulin, but since there is so much excess glucose in the blood, insulin comes to the cell receptor and they wont let glucose in because they have become sensitized.Now it will take more insulin to do the same job.
-also happens with narcotic addiction
Thyroid Cascade
thyroid hormone helps us make ATP, the target cells for thyroid hormone is every cell in the body so it affects many things.
-need more ATP? positive feedback loop is started. Hypothalamus release TRH which reaches pituitary gland and then releases TSH, TSH reaches thyroid and the thyroid gland release TH and then goes to target cells (all cells in the body), once we have enough, negative feedback loop is initiated to stop making TRH
Cause of Endocrine Disorders
-autoimmune
-most common cause is a tumor on gland (pituitary)
-target cell resistance (type II diabetes)
-congenital defect
-hyperplasia (increase in cell number - goiter)
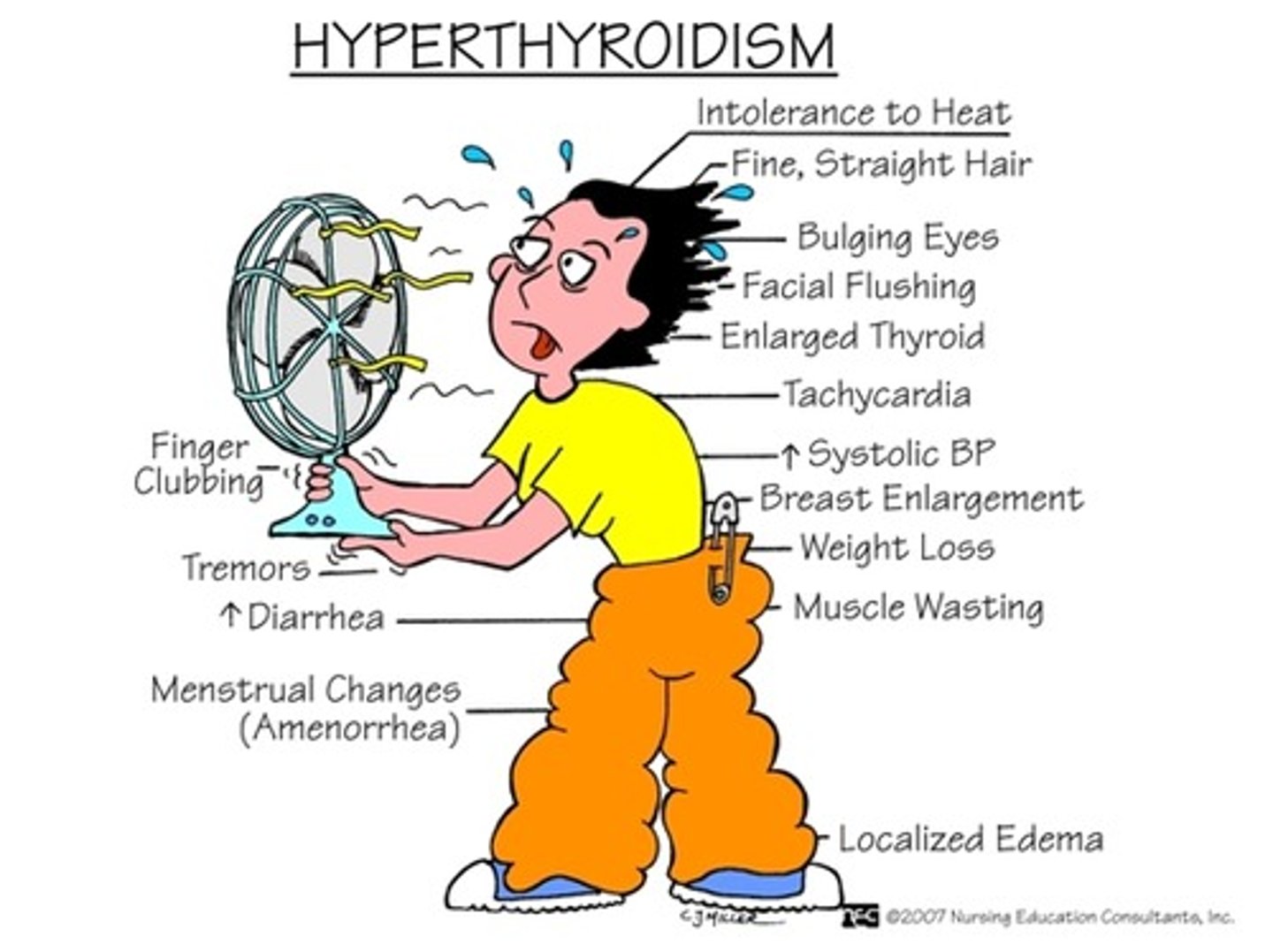
Hyperthyroidism
(graves disease)
-only affects women, autoimmune
-body produces antibodies (normally fight infection), but this AB's instead will go to the thyroid and will mimic the cascade. They tell the thyroid to produce more thyroid hormone, even when negative feedback is taking place
-Sx: exophalmos (bulging of the eyes caused by inflammation from cell mediators), toxic goiter, symptoms are also due to everything speeding up (hot because of increased metabolism which makes more ATP - ATP releases heat, shaky: everything is moving fast through body, weight loss: crazy fast metabolism, tachycardia, increased BP: thyroid hormone helps maintain BP
-Tx: iodine (kill part of thyroid) or surgically remove part of thyroid
Hypothryoidism
-common, autoimmune
-thyroid does not make enough TH
- AB's are attacking the thyroid so it is not able to make as much TH
-usually affects women
-Sx: due to lowered metabolism, everything slows down. Cold: not making a lot of ATP, super tired, apathy (disinterest)
-Tx: synthroid which acts as a superficial TH, easy treatment that has to be regulated very closely as metabolism needs change
SIADH
-syndrome of inappropriate antidiuretic hormone
-high levels of ADH (ADH helps keep water)
-if we have too much ADH, we have too much water in the blood stream, end of with tons of water and not enough sodium
-hyponatremia: imbalance of water to salt, brain is super sensitive to this, the brain will know that this is off
-problems happen from being in a hypo-osmolar state (not enough solutes in blood)
-ADH works on last part of nephron so it gets the last say on deciding on how much water to pull back
-causes: tumor on pituitary gland, occasionally after surgery
-Sx: irrational thirst: ratio of solute to water is off so the brain wants us to drink more water, but we already have all this water in the bloodstream. Anorexia and GI problems: wont want to eat when carrying around all this extra water. Dyspnea: extra fluid in blood stream so increase in hydrostatic pressure, fluid could exit into lungs.
-Severe Sx: changes in LOC, confusion, lethargy, muscle twitching, convulsions
-NOT A SODIUM PROBLEM, this is a water problem
-Tx: IV fluids or a hypertonic solution, important to give fluids slowly since a if there is a sudden increase in solutes, water will be attracted from the brain cells so they will shrink and die and will put you into a coma OR water can be rushed into the brain cells too quickly and the brain can burst or die, which leads to coma or death
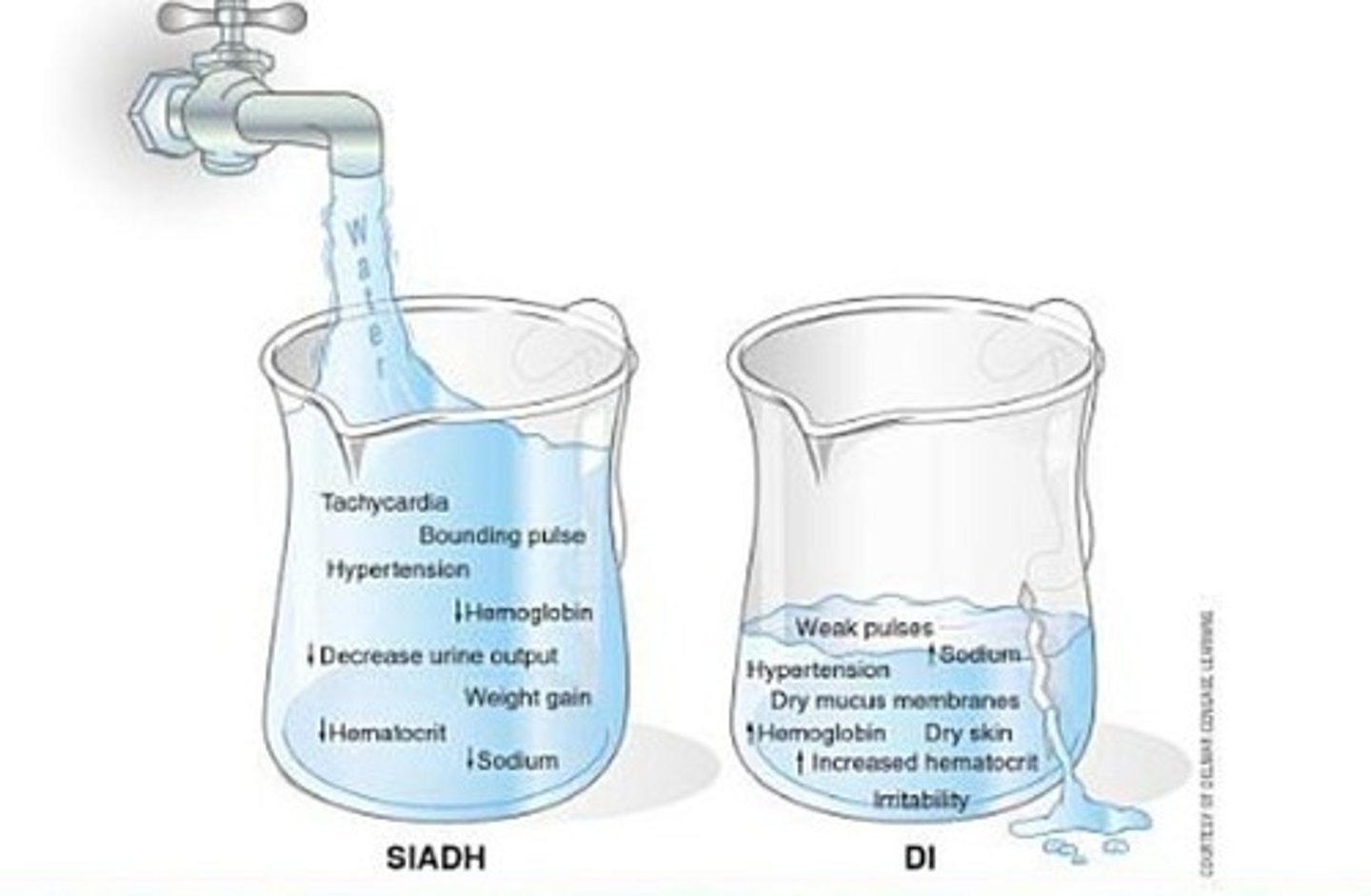
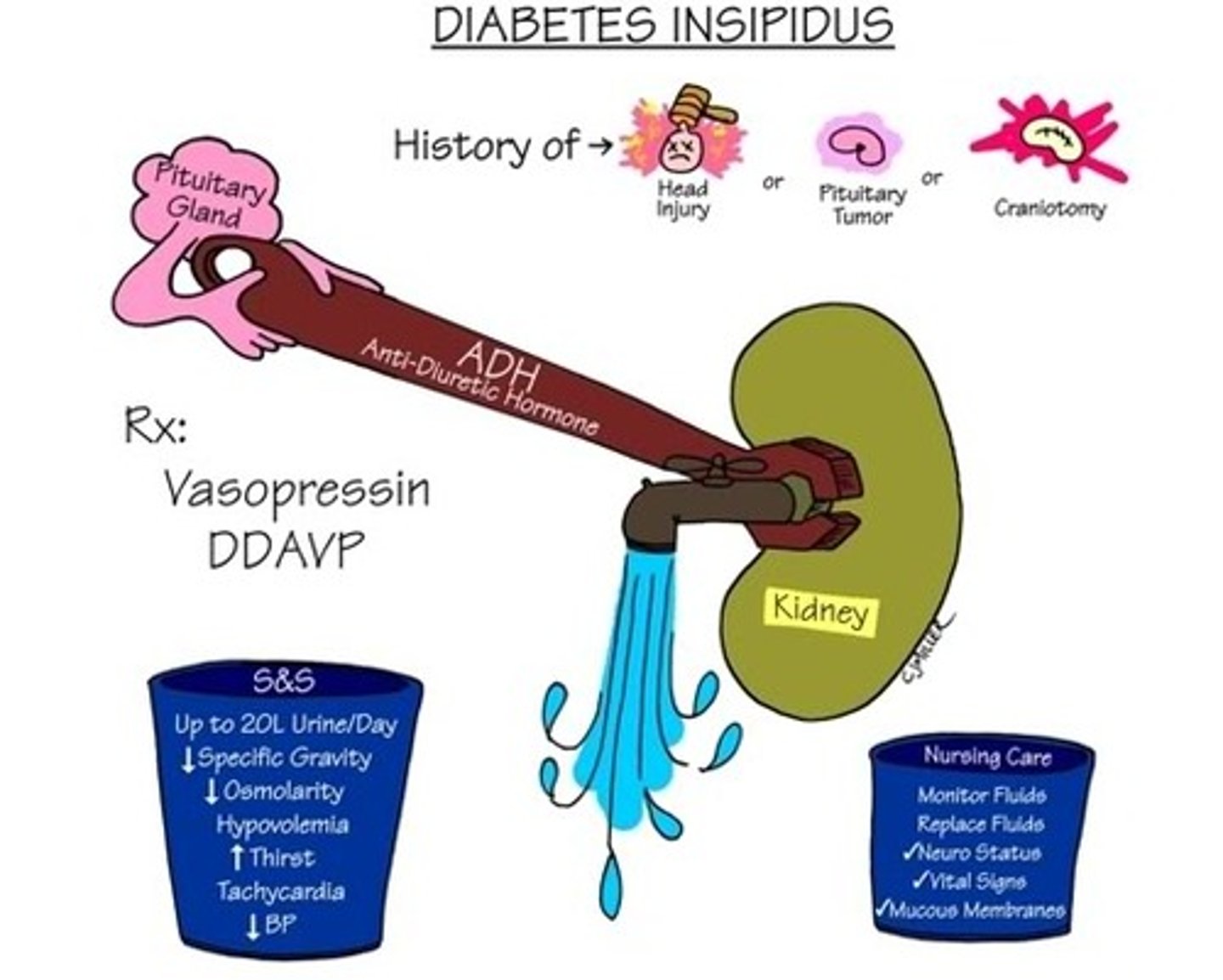
diabetes insipidus (DI)
-rare
-causes by trauma, tumor on pituitary, craniotomy
-Sx: polyuria (frequent urination) and polydipsia (increases thirst)
-not enough ADH so dumping tons of water into urine, so pt. is severely dehydrated. All of the water is exiting through the kidneys and now have an inability to concentrate urine (ability to pick and choose what we want in the nephron)
-increased plasma osmolality: blood vessel with not enough water and tons of solutes, hyperosmolar state, blood is thick and viscous, syrupy due to lots of solutes
-hypernatremia not related with intake of salt, all a water problem
-Sx: increased thirst due to losing a lot, urinating at night, can lose up to 20 L of urine in a day (hypovolemic), tachycardic: super dehydrated so heart has to work harder and there isnt a lot of volume
tx: vasopressin (artificial ADH)
Diabetes
-common
-important to note that insulin is dangerous
-beta cells in pancreas produce insulin
-normally: when there is glucose in the blood, insulin gets released from the beta cells into the blood stream. insulin acts a key to get glucose inside the cells. insulin is water soluble so it needs a second messenger to take it to the nucleus.
-hyperglycemia: tons of sugar in blood
-type 1: dont make enough insulin
-type 2: insulin resistant, down regulation
-Diagnose: hemoglobin A1C or HbA1c - draw blood and look at RBC's, look at how blood sugar levels have fluctuated in the last 3 months, want this to be below 7.
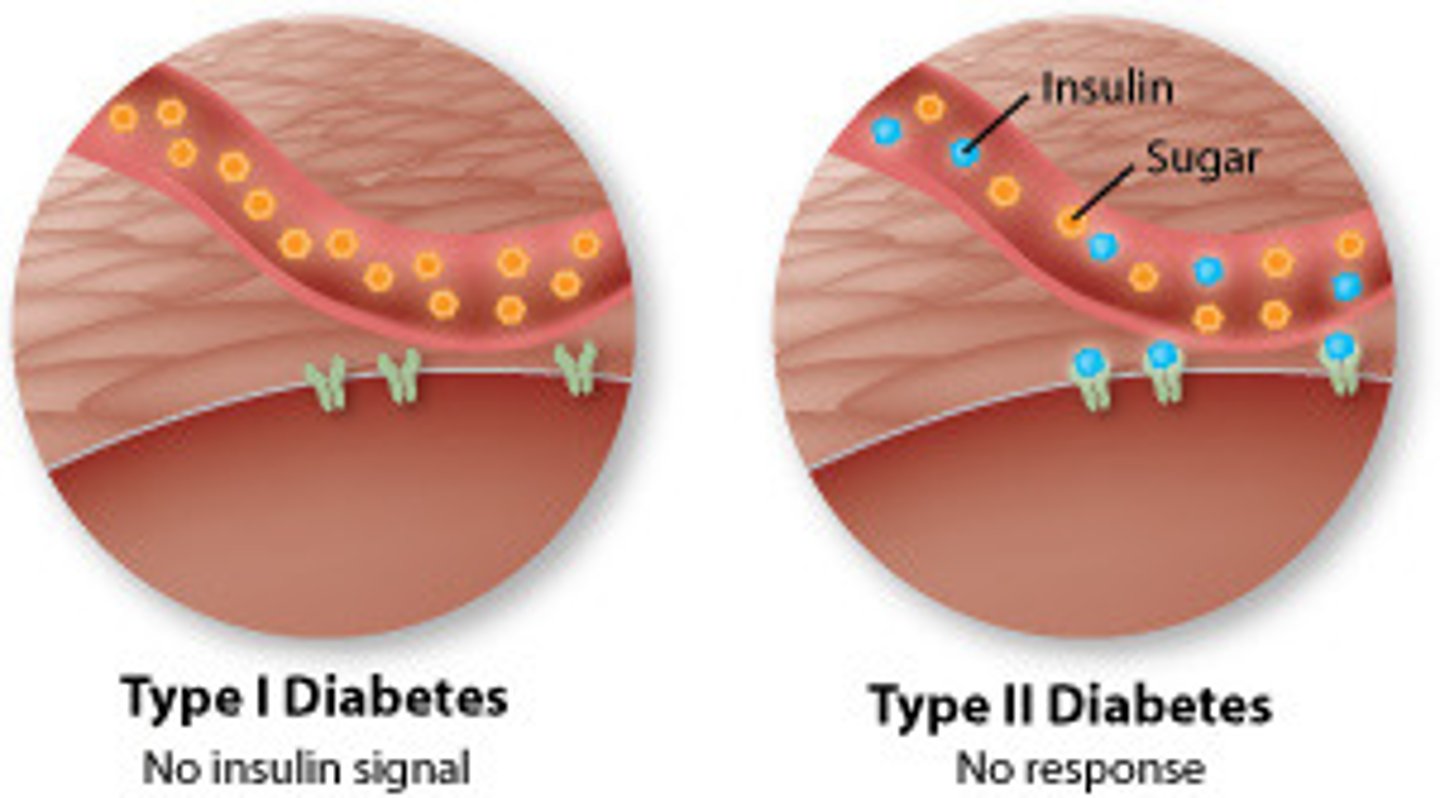
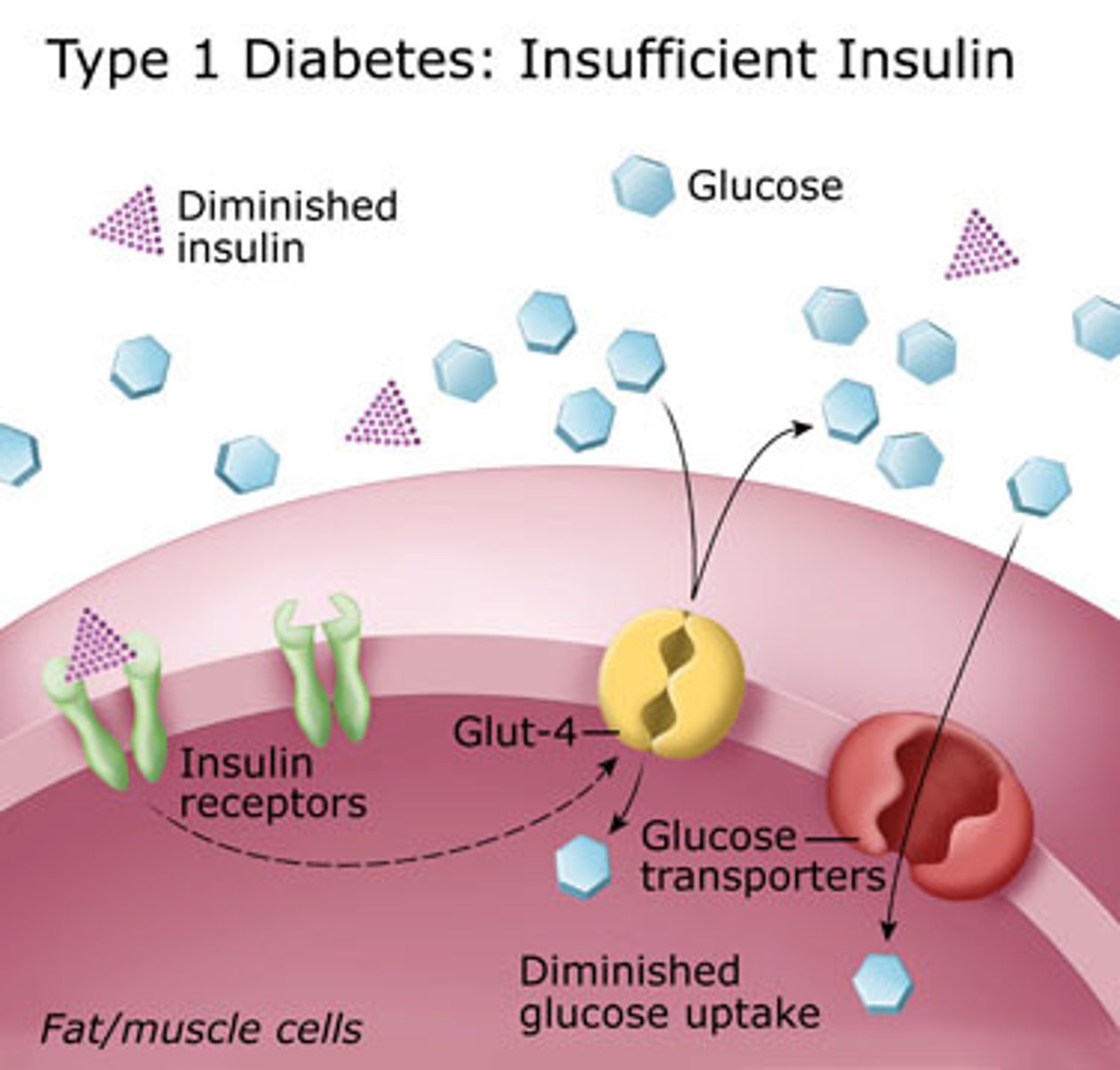
Type 1 Diabetes
-insulin deficient
-hypoglycemia that is caused by autoimmune
-childhood disease
-For some reason our body produces AB's that attack pancreas and we stop making insulin. We become deficient, lose ability for beta cells to pump out insulin. If we don't have insulin we end up with tons of glucose molecules in blood stream and none of it is making it into cells
-RF: family history, environment, asians, african americans
Sx: 3 p's, weight loss initially since sugar is not entering into cells, starving, fatigue (no ATP), increased infection (bugs love sugar), rapid onset.
-will need external insulin forever
3 P's of diabetes
-polyuria: increased urination due to body trying to get rid of excess sugar, kidneys are helping out, trying to get rid of sugar molecules, but its not a good thing for glucose to up in urine and nephron (indicator that something is off)
-polyphagia: increased hunger - glucose is not making its way into cells, staying in blood stream so cells are starving
-polydipsia: increased thirst - a lot of solutes in blood (syrup blood), brain is going to increase thirst mechanism to try and balance osmolality of the blood, also due to increased urination
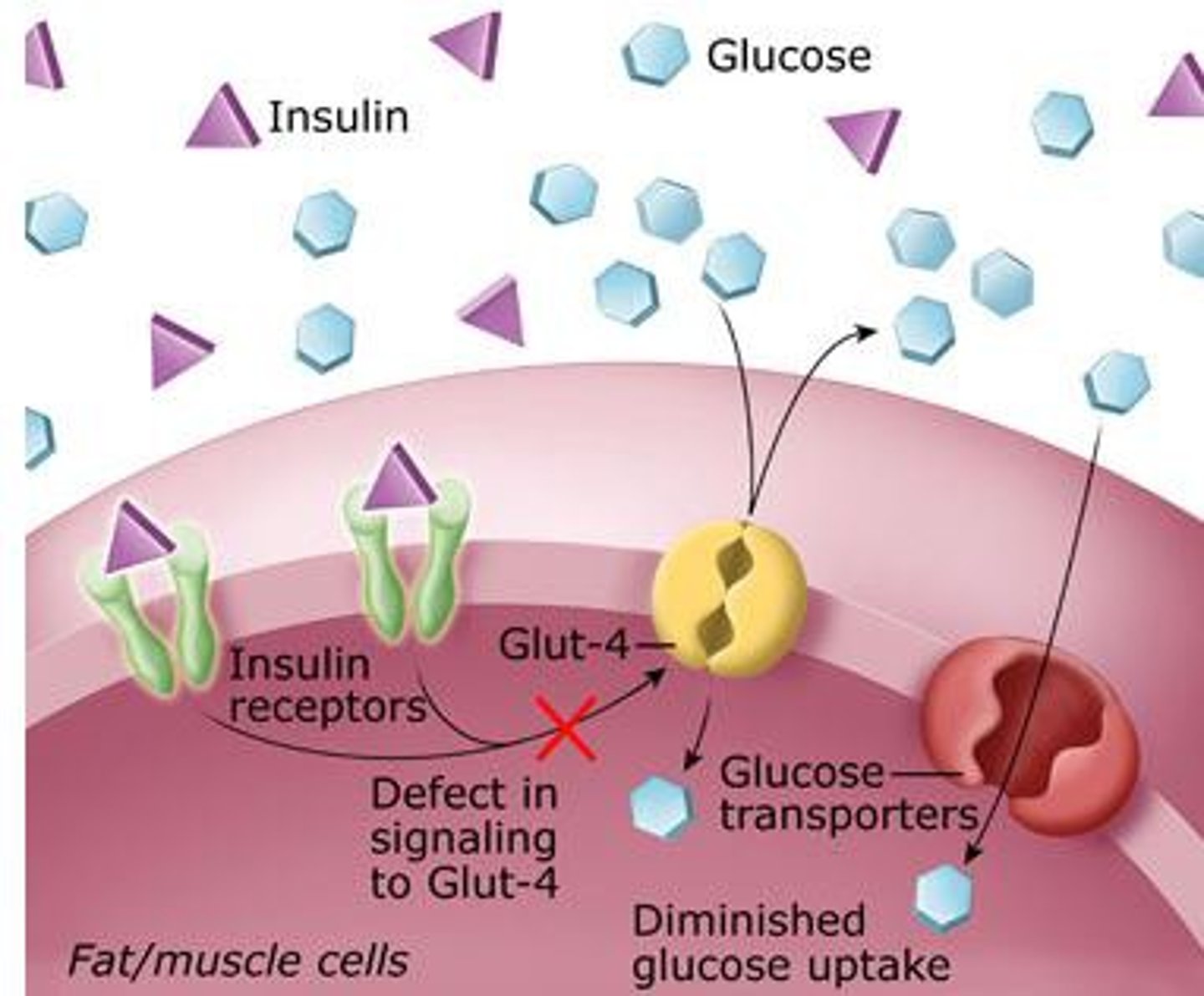
Type II Diabetes
-problem is insulin resistance, pancreas is pumping out so much insulin to make up for tons of glucose and cells are super tired of seeing insulin, cells become insulin resistant
-RF: lifestyle related, obesity, age, HTN (blood moving to quickly, epithelial injury damage - glucose damaging to body because all of the complications that come from diabetes are from how damaging this molecule is, as glucose is rocketing through a blood vessel at a fast rate and it stabs the side of a blood vessel and causes damage and can start atherosclerosis, also has issues getting through kidneys and tiny arteries
-decreased insulin secretion: diabetes is a progressive problem - can move forwards or backwards
-Tx: strict diet or oral medication: glycerides, metformin (helps pancreas to produce more insulin or on cells themselves to be become more receptive - can still move backwards and cure yourself of diabetes)
-once you become insulin dependent and cant go backwards and need insulin for life, pancreas has quit and pancreas does not work anymore so resembles type 1.
Sx: 3 p's decreased energy, obese, recurrent infections (bacteria loves sugar), FBS is greater than 125 mg/dl
Acute complications of diabetes
-Slightly incorrect dose of insulin can drop blood sugar so low so they can slip into a coma and die (hypoglycemia) - insulin shock - too much insulin, rapid onset (sweaty, irritability, confusion, seizures, coma)
-Diabetic ketoacidosis: crazy high blood sugar (600, 700)
-Occurs from too little insulin and body is starving and we go into backup metabolism - break down fats and proteins and get ketones. Ketones are extremely acidic cant live on this alone. When we get super high levels of ketones then you end up in metabolic acidosis - DKA is most common cause. Body compensates by respiratory system - deep, rapid respiration (kussmaul respirations) using accessory muscles to blow of CO2, sweet smelling breath or urine or sweat from ketones (acetone production which is super sweet), will all this acidity you have CNS depression
-Causes: type 1 diabetic about to be diagnosed (come into ED lifeless - cells have been starving for so long, so body has to do backup metabolism, type 2 that doesn't follow diabetic diet, diabetics who are sick (vomiting, flu) - so don't take insulin. Metabolic needs change when you are sick.
chronic complications of diabetes
• Acute retinopathy
• Diabetic nephropathy
• Neuropathy:
• Nerves are not functioning anymore (cut off or eaten away)
○ Tends to happen first in feet and hands (numbness and tingling sensation)
• Danger: don't inspect feet often, can step on something and they don't feel it, bugs love sugar so they can get an infection, an ulcer, can get gangrene - end up with amputations
• Heart attack: all due to atherosclerosis due to so much glucose (throwing stars)
• Stroke: atherosclerosis
• Peripheral vascular disease: atherosclerosis
• Glaucoma/cataracts: tiny vessels behind eyes can get clogged and damaged
• Infection
Nephron
-putting things in and out of fridge:
- Put everything into glomerulus, then everything gets thrown into nephron with the exception of large molecules that should into go into nephron (blood and albumin) - too large and damage glomerulus. Everything gets pumped into glomerulus and goes into nephron as filtrate. First function is filtration. Can manage ability to pull things into nephron (glomerular filtration rate GFR). Proximal tubule: sodium, potassium, water, take everything out of fridge. Next go to reabsorption - hey I actually want to keep some of that potassium and sodium, putting things back into fridge, starts in proximal tubule and finished up in loop of Henle. Loop of Henle is water reabsorption and does it passively - osmosis. Distal tubule: third function: secretion, bodies last effort to get rid of toxins, deposit urea into collecting duct - active process - active transport - ATP. ADH acts on distal tubule and collecting duct - last say on how much water we want to keep. Whatever is left after this process makes urine
-Easiest way to measure kidney function is serum blood tests: are my kidneys filtering out toxins. Filters out metabolic waste - breakdown of macros,. Proteins create biggest amount of waste products like uric acids. We can measure levels of those toxins in the blood. If kidneys are filtering great, should have low levels of those toxins. If kidneys aren't working good, all serum tests will be elevated.
Serum Blood Tests for Kidney Function
-BUN (blood, urea, nitrogen) - waste products
-creatinine
-uric acid (healthy kidneys can get rid of)
Function of Kidney: remove metabolic waste
-when protein is broken down, we get ammonia, the liver is supposed to turn this into urea. It is the kidney's job to get rid of urea. Urea gets deposited into collecting duct. FAILURE: high level of urea in blood (uremia). Urea is a form of ammonia, if you have high levels of this in the blood stream then you can get encephalopathy (brain poisoning). Even though the liver can perform conversion, the kidneys dont do their job of getting rid of it.
Function of Kidney: secrete erythropoietin: stimulates production of RBC's
Need this hormone to tell bone marrow to make RBC's. FAILURE: not making a lot of RBC's which leads to anemia (fatigue, pallor, tachycardia - impaired O2 transport)
Function of Kidney: activation of vitamin D
Vit. D is important to help absorb calcium for bones. FAILURE: cant absorb calcium which leads to bone loss or osteoporosis. Calcium is also important for cardiac muscle contractions so if kidney fails then you have weak cardiac contractions. Calcium acts as an insulator so that nerves have an appropriate response, if they dont have enough then there will be neuromuscular dysfunction (spasticity, tetany). If you have too much calcium you have muscle weakness and depressed neuromuscular activity (not enough reaction)
Function of Kidney: fluid and electrolyte and pH balance
hormones that regulate fluid: aldosterone (keeps salt), ADH (keeps water) electrolytes (most dangerous is potassium). pH: kidneys and hydrogen ion/bicarb. FAILURE: kidneys end up keeping everything. Nephrons shut down progressively. Dont have the ability to decide what is sending out in body. Instead of picking and choosing, you keep everything. Keeping lots of ADH/Aldosterone = edema. High potassium = arrhythmia's. High H+ ions = metabolic acidosis.
Function of Kidney: Regulate blood pressure
RAAS system. FAILURE: kidneys want a precise amount of O2 and blood flow. When they dont get this the RAAS system is getting triggered every time so we always have HTN.
Function of Kidney: remove drugs and toxins
nephrotoxic drugs: generally really serious antibiotics "mycin" drugs. NSAIDS filtered here. FAILURE: drug toxicity and drug interaction. Can damage kidneys by just abusing NSAIDS.
Kidney pain is felt:
flank pain
Bladder pain
by groin/low back pain
Dysuria
painful urination
Hematuria
blood in the urine
Proteinuria
protein in the urine
Incontinence types:
urge (gotta go now, pregnancy), stress, mixed (both stress and urge), functional (something wrong with nerves in bladder)
Oliguria
Decreased urine output
Polyuria
increased urine output
Anuria
absence of urine
Obstruction in Kidney
• Primarily talking about stones, most common, generally idiopathic.
• Other things that can obstruct: tumor, enlarged prostate, scarring/stenosis (narrowing) of ureter.
• RF: stone (calculi or nephrolithiasis), age (before 50), men (usually because they don't drink as much water), fluid intake, pregnancy, diet
• Stones mostly made up of calcium, salts (something crystallizes and forms an object)
• Should not stop eating calcium
Some people don't have stone inhibitors (enzymes that help inhibit the crystallizing process)
• High pain
• Symptoms: horrible flank pain, so bad you throw up, hematuria: the stone is scraping the inside of ureter, still will feel the urge to pee.
• Tx: has to be resolved because urine can turn around and go back to where it came from, always have risk of nephrons failing. If we don't resolve a stone, then this whole system of the nephrons can fail us. Have to be able to get filtrate out of body. Occasionally there can be an infection, can potentially travel to the kidney (unlikely since we resolve them)
• Hydronephrosis: fluid sitting in kidneys
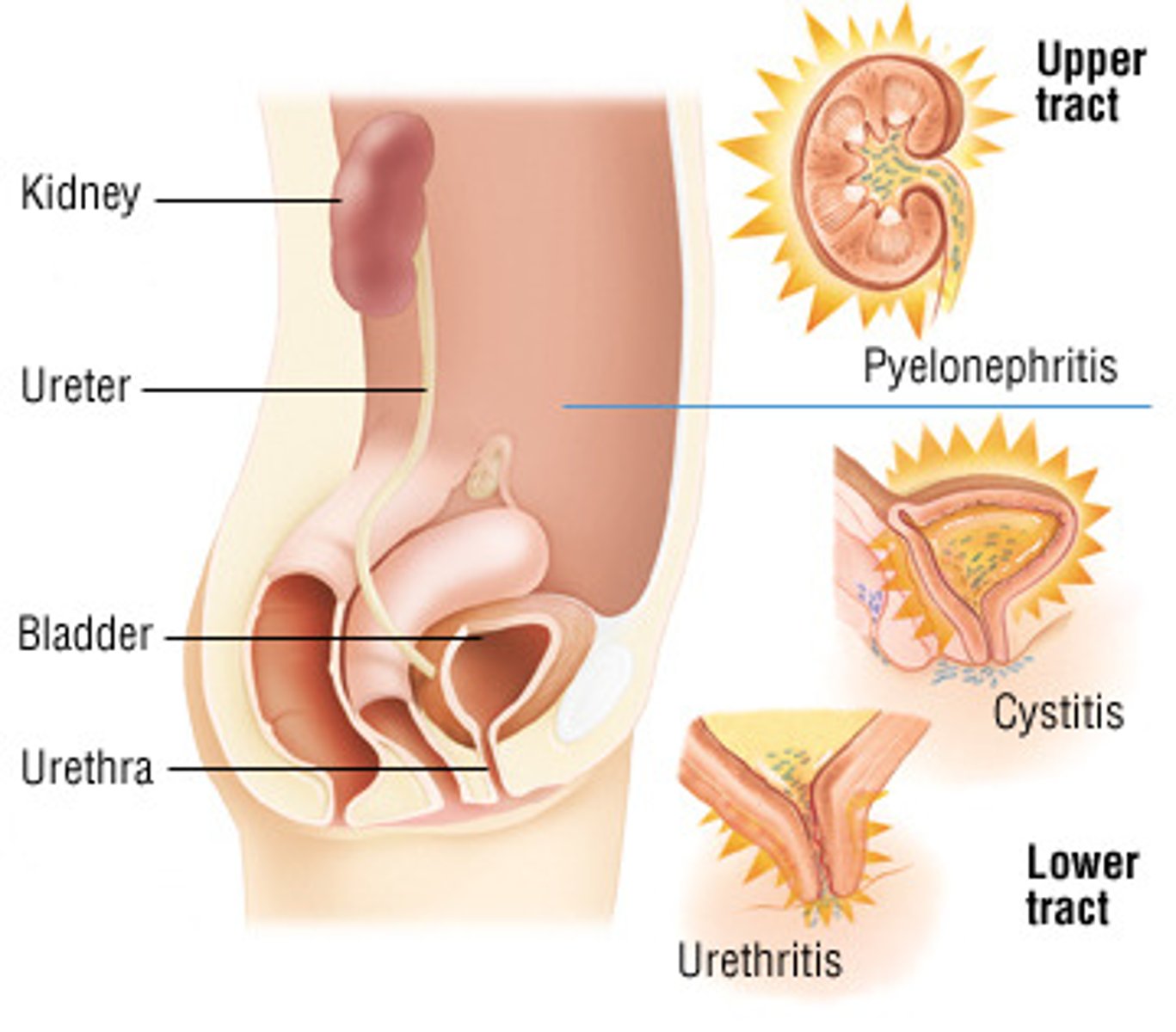
Infection in Kidneys
• Inflammation of the urinary epithelium.
-In the bladder: acute cystitis (UTI)
- Pyelonephritis
• RF: elderly ( incontinence, poor hygiene), women (shorter urethra), pregnancy ( pH changes to be more alkalotic, and we need a little bit of acidity to kill bacteria), diabetes (sugar - bug love it)
• Symptoms: burning, urgency, frequency, dysuria (pain), possible to get a low grade fever with UTI and high fever with pyelonephritis, groin pain with UTI, with pyelonephritis will be flank pain, hematuria, only pee a little
• Tx: antibiotics, if you catch it early (cranberry juice can change acidity and kill bacteria), important to tell pt. to take prescription for entire time (if don't, you don't kill all of the bacteria, resistance will build so will need a stronger antibiotic)
• Elderly: even though most at risk are typically asymptomatic but they get confused, they wont experience all the dramatic symptoms, get mistake for symptoms of aging (dementia, etc)
• Complications: when elderly get a UTI, they can die from that one infection because they didn't get tx when they should have, but the infection that started in the bladder makes it way up to kidneys (pyelonephritis) more dangerous, kidney's have direct blood supply so once bacteria is there then bacteria can go into blood stream (sepsis)
• Pyelonephritis: bacteria in kidney's, high fever, typically admitted in a hospital, IV, antibiotics, can potentially shut kidneys down temporarily
• Can get UTI's easily in a hospital from catheter's.
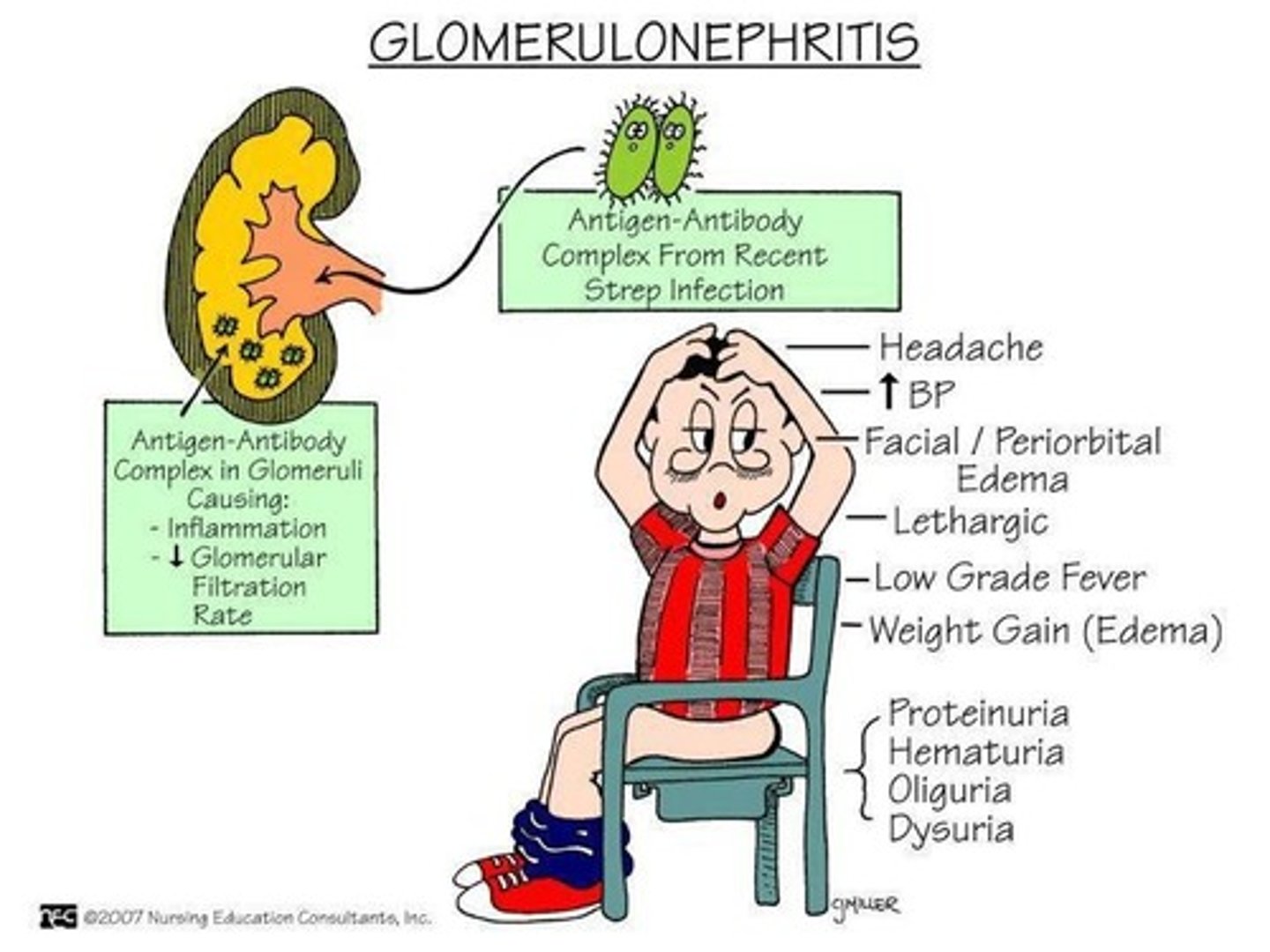
glomerulonephritis
• Inflammation of the glomerulus
- Caused by: streptococcus OR weird immune mechanism (type 3 hypersensitivity - antigen antibody complex, form a complex and this complex travels around the body and causes inflammation and one of the places is in the glomerulus, it punches holes in the glomerulus which causes proteins and blood to travel through which shouldn't)
• Sx: hypertension, due to RAAS., protein and blood loss
Acute Kidney Injury (AKI)
• Temporarily injury to kidneys, where one shuts down temporarily. Not a chronic problem, not anything wrong (diabetes), could happen in a moment (boxer and someone punches you in the kidney), hopefully with some rest, kidney function is restored, but AKI can progress to chronic
• See the stages of CRF really fast, decreased GFR (nephron isn't able to decide what should we send into bladder), accumulation of waste products (creatinine and urea , not able to get rid of toxins), all of these symptoms are the same with CRF, also see hyperkalemia, increased serum levels (BUN, uric acid, creatinine)
• Danger, can lead to chronic. Kidneys are so damaged we cant rebuild.
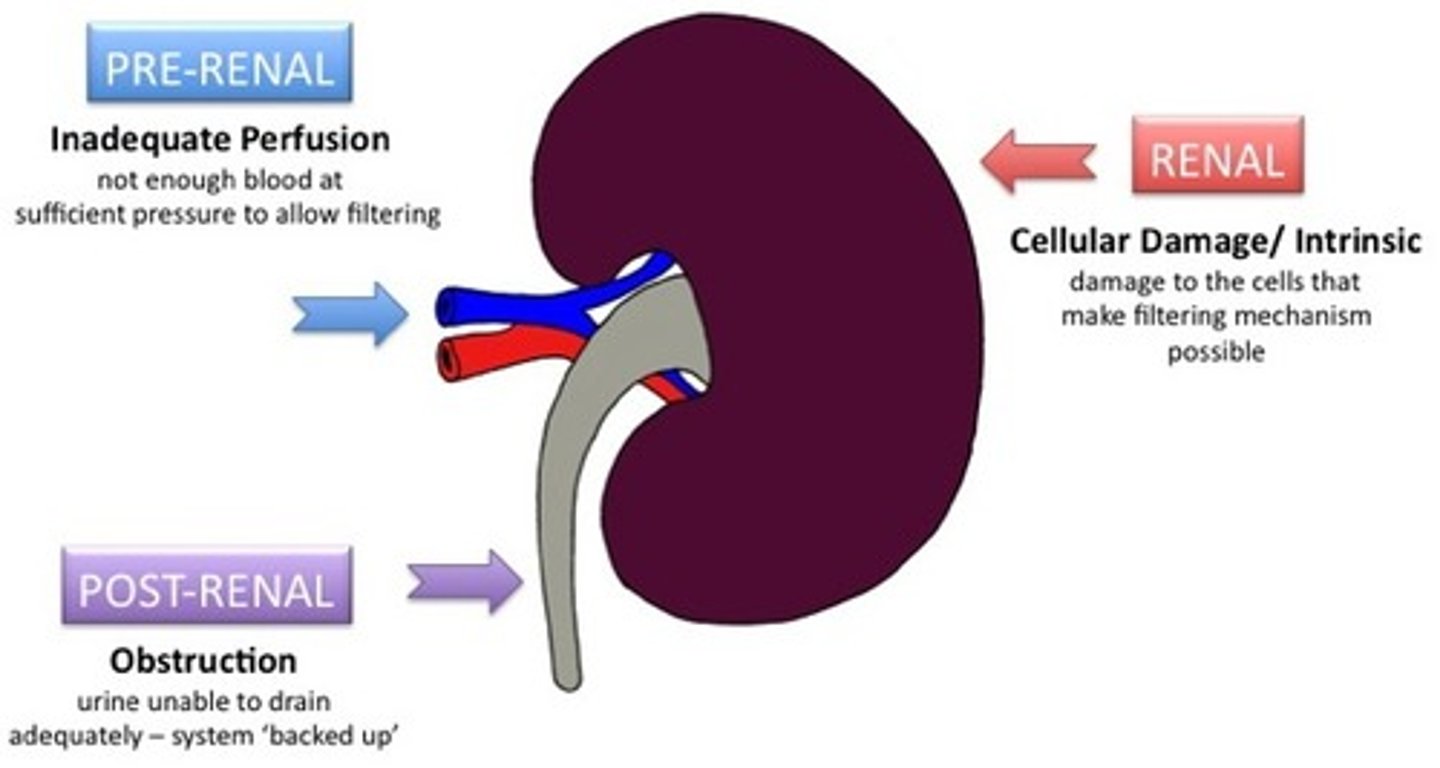
• Causes:
○ Prerenal injury: problem happens before the kidneys, sudden severe drop in BP (shock, arrhythmia, potential illness ) - not having enough blood flow
○ Intrarenal: problem is in the kidney's, inflammation, glomerulonephritis, nephrotoxin drugs (mycin, NSAIDS)
○ Postrenal: below kidneys (enlarged prostate, kidney stone that is not resolved, tumor in bladder)
Stages of Renal Failure
1• Decreased reserve: 60 % loss of nephrons, 1st stage of renal failure, only sign with will see if slight decrease in GFR, slight increase in creatinine, rarely catch it here
2• Renal insufficiency: 75% loss, change in blood chemistry, decrease GFR, failure to concentrate urine (losing everything in urine), second stage, will experience like turning on a faucet (water, waste products, electrolytes, cant perform reabsorption), lose everything initially. Osmotic diuresis. Deceased erythropoiesis: anemia, HTN due to RAAS
3• End stage renal failure (90% loss) not holding onto everything, not making urine, keeping everything, high level of uremia in blood -> encephalopathy, GFR is negligible, fluid, electrolytes and waste are all retained, edema, hyperkalemia, uric acid and urea, retained, H+ retained -> metabolic acidosis, (NEED DIALYSIS or transplant)
Chronic Kidney Disease (CKD)
• Progressive loss of function associated with systemic disease or AKI that doesn't resolve is the causes
• Diabetes is a common cause, HTN - triggering RAAS system over and over again, autoimmune diseases (lupus), nephrotoxins
• Fluid and electrolytes imbalances (edema, arrhythmias, metabolic acidosis)
• Bone loss because cant activate vit D
• Decrease in muscle mass (proteinuria, losing protein in urine)
• Glucose intolerance: diabetes
• Dyslipidemia: too much LDL, not enough HDL
• HTN - RAAS
• Fluid overload: aldosterone, ADH, everything has shut down, so now keeping everything
• Anemia: decrease erythropoiesis
• Immune suppression: antibodies are made up of proteins, losing proteins in urine so we aren't able to synthesize immunoglobulins or AB's
• Neurologic dysfunction: encephalopathy, buildup of urea
• Gastritis: inflammation, metabolic acidosis (increased acid all over), h. pylori (inflammation makes it multiply like crazy)
Function of Bones
protection, help with blood cell production, store calcium and regulate calcium levels, support and movement
Osteocytes
primary bone tissue cell, responsible for spongy appearance of bone
Osteoblasts
builds up bone and increases bone density and forms bone matrix
Osteoclasts
decreases bone density, reabsorbs bone matrix
Calcitonin
regulates osteoblasts
Parathyroid Hormone
stimulates osteoclasts
Bone remodeling
process of osteoblasts and osteoclasts working together
Stem cells
live in bone marrow, undifferentiated (doesnt have a job yet), can turn into an RBC, WBC, or platelet
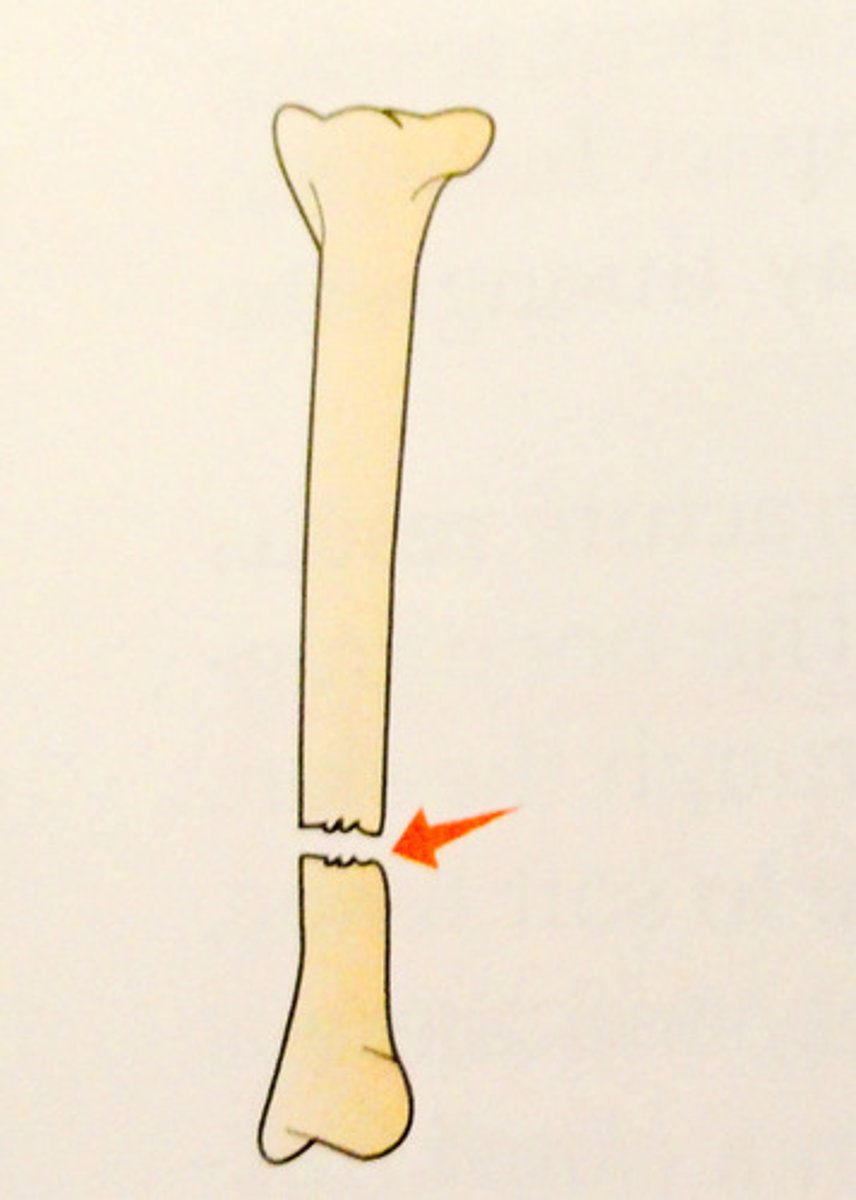
Transverse Fracture
complete fracture that is straight across the bone
Spiral Fracture
twisting motion in arm causes this, indicative of abuse

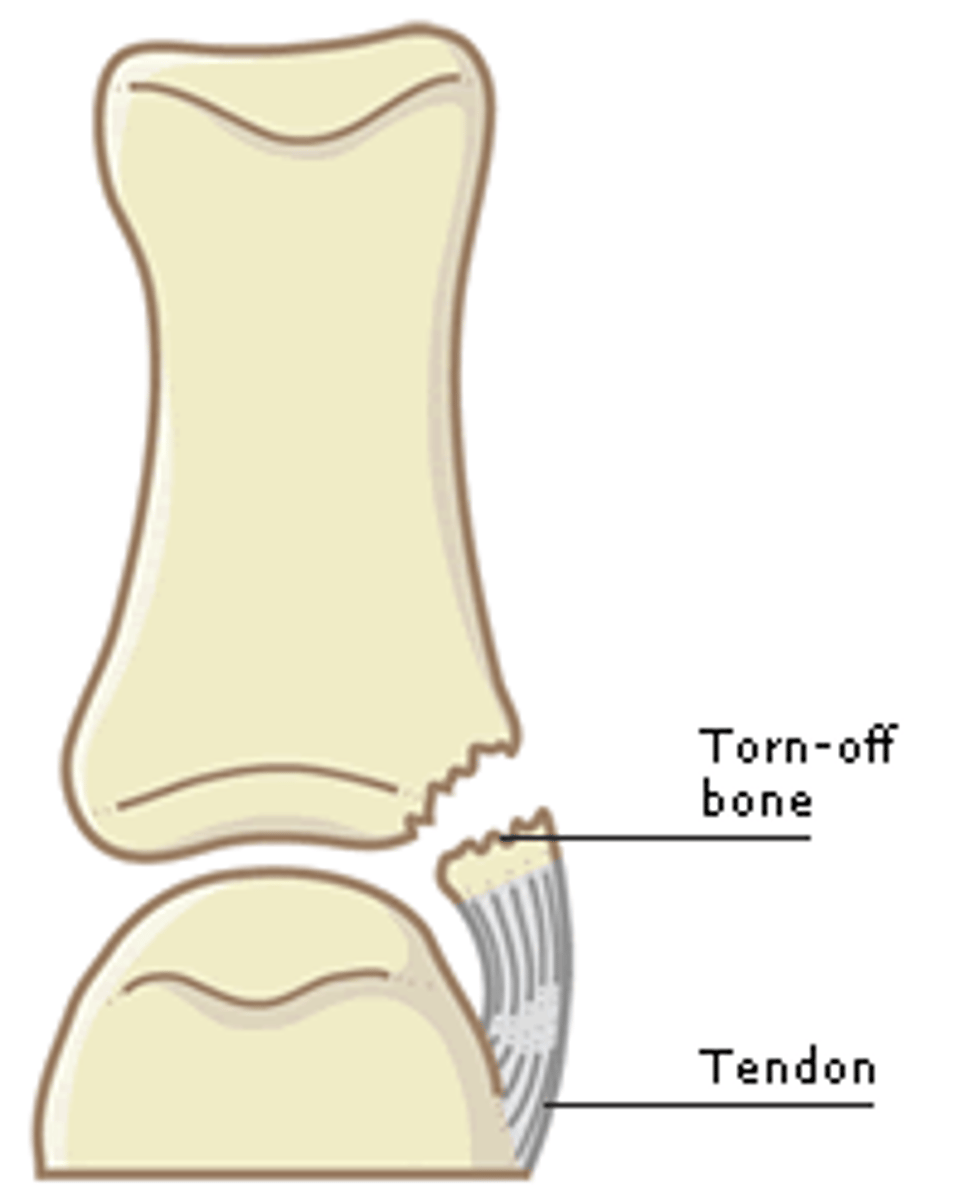
Avulsion Fracture
knobby part of bone breaks off (wrists, ankles)
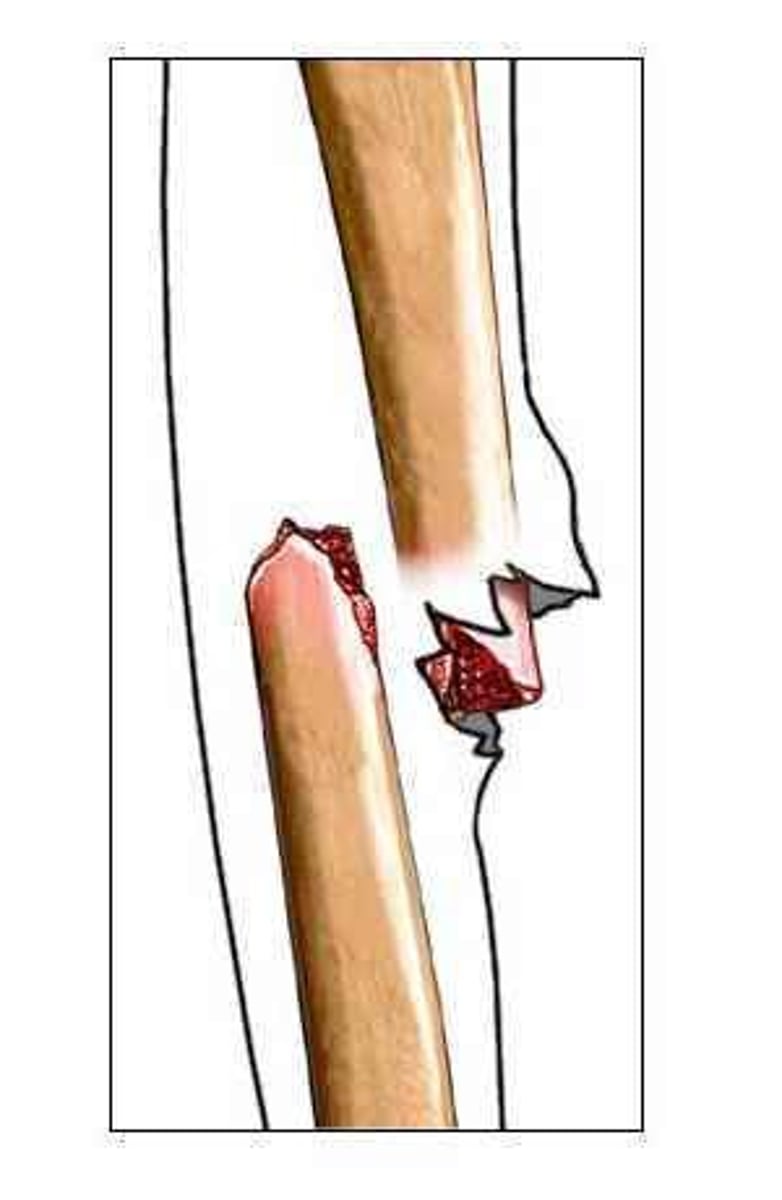
Greenstick Fracture
bone splinters, happens in children, not a clean break

Open fracture
skin is broken
Closed Fracture
skin did not break

Tendon
connects muscle to bone
ligament
connects bone to bone
Sprain
tear in a ligament
Strain
tear in a tendon
RICE
important to reduce inflammation (supposed to be acute). Ice helps with vasoconstriction so we have less water leaving the capillaries and going to the injured site. Compression to help push the fluid back to where it came from and to get rid of edema.
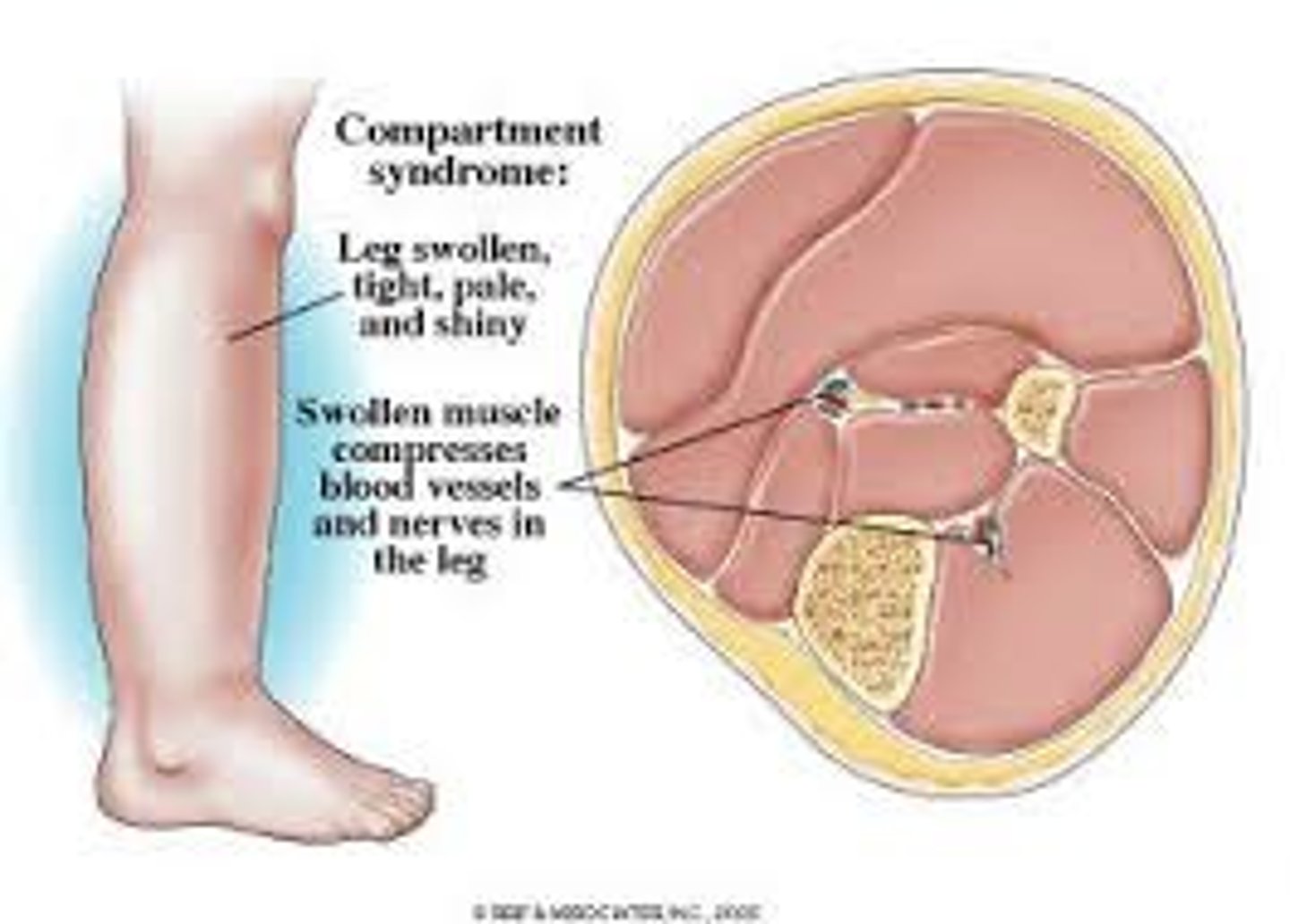
Compartment Syndrome
-increases pressure in muscle compartment, burst blood vessel is a common cause (something leaking that shouldn't be, and in a muscle compartment there is nowhere for the fluid to go)
-need to get rid of compression to avoid necrosis
-cause: trauma, snake venom
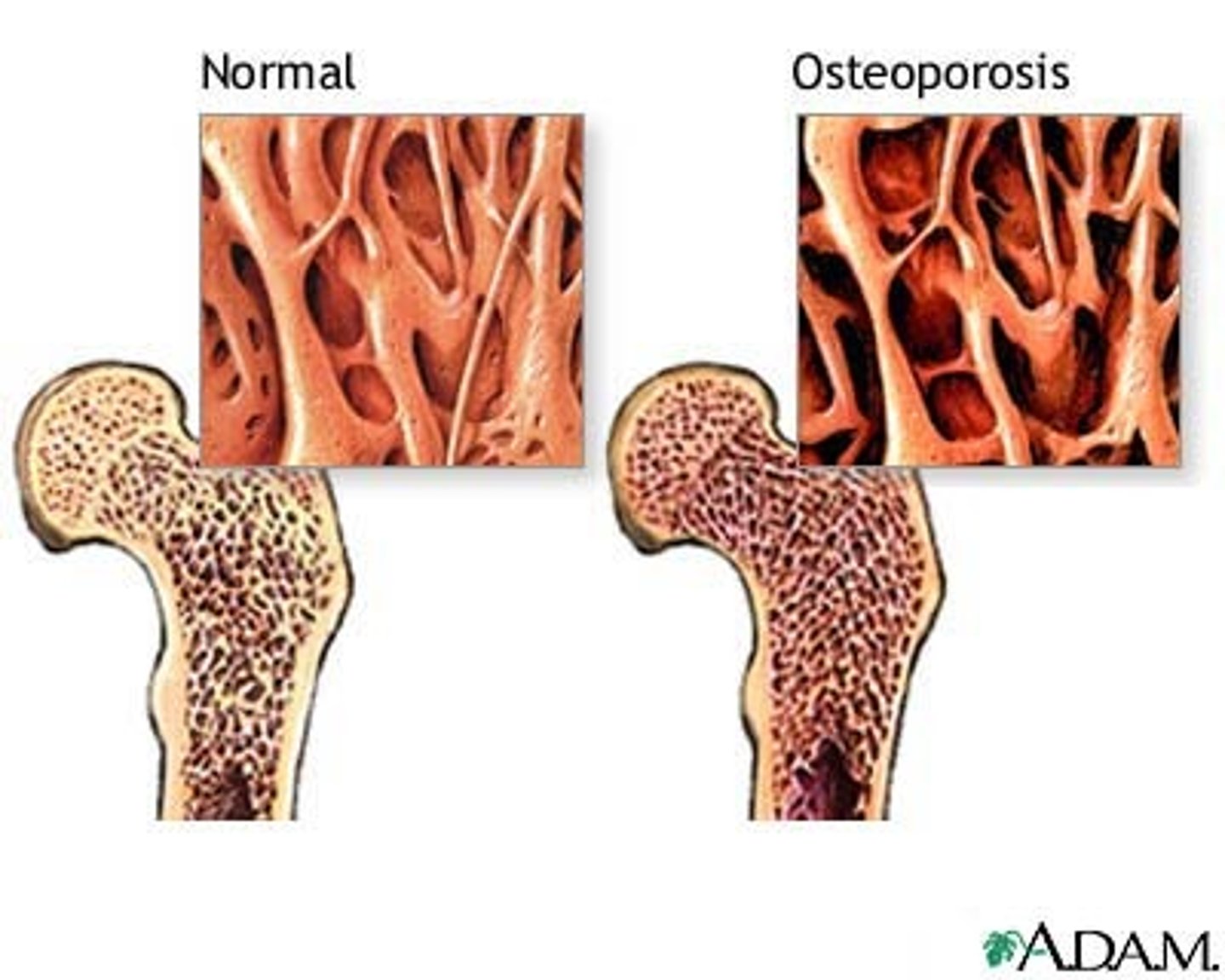
Osteoporosis
• Decreased bone mineral density
• Osteoclasts have gone crazy
• Breaking down bone matrix
• One potential Cause: parathyroid hormone going crazy
• Another cause: not enough calcium
• Chronic renal failure: since liver cant activate vitamin D cant absorb calcium
• White women most at risk
• Multifactorial
• Menopause is a big risk factor: when you go into menopause, estrogen is a protective factor of osteoblasts, so when we lose that estrogen, the osteoblasts aren't protected anymore
• At risk for fractures easily
Osteoarthritis
• Affects athletes or someone who has suffered from obesity
• Affects load bearing joints, knees, ankles, elbow
• Loss of cartilage
• Bones do a grinding motion and form a bone spur, osteoblasts will try to help and rebuild, we don't do this effectively since we are constantly breaking down bone that we are trying to build
• Pain, joint stiffness, limited ROM
Not an inflammatory process
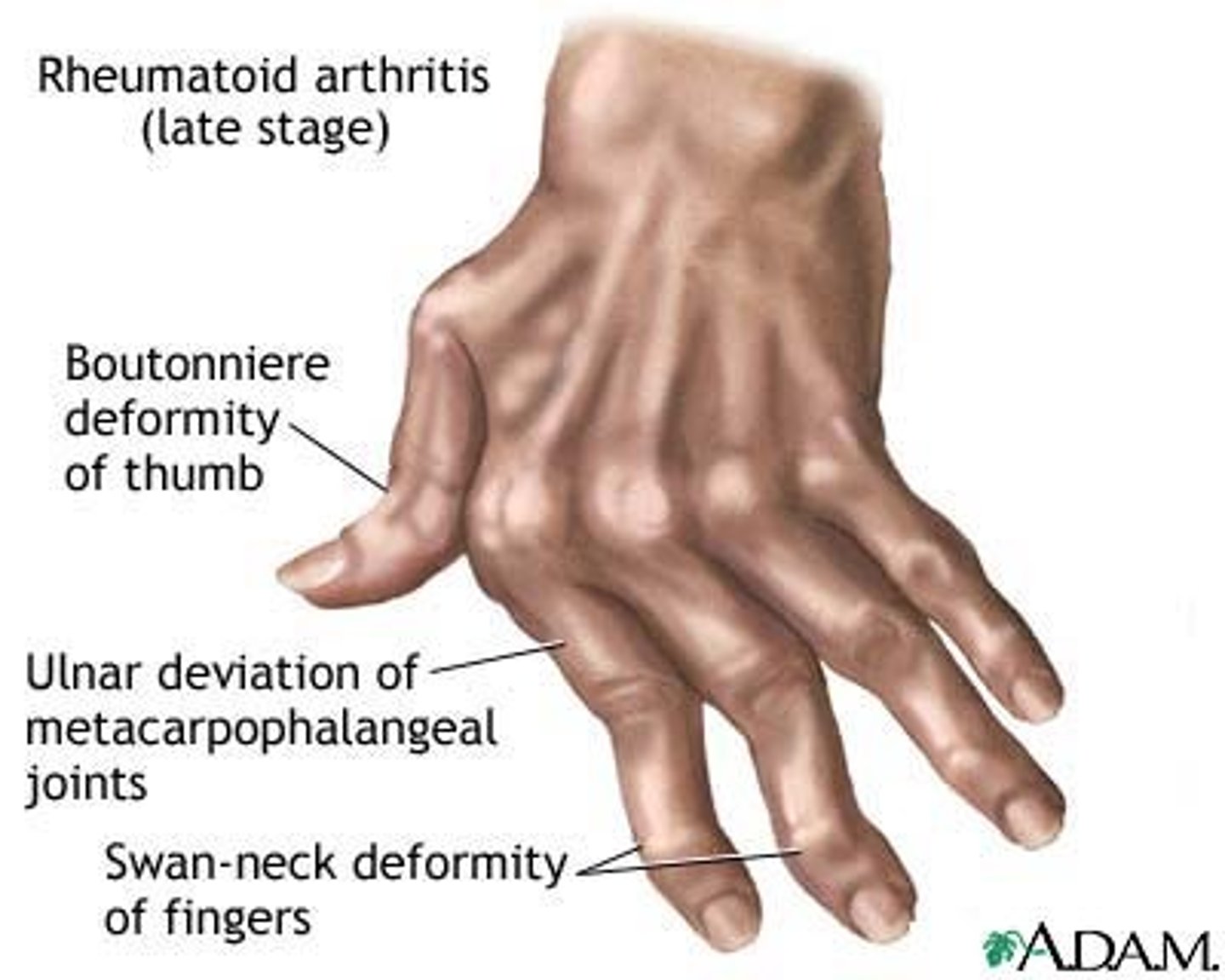
Rheumatoid Arthritis
• Autoimmune disease, don't know the cause
• Chronic inflammatory process that stays present in affected joints
• Hinge and synovial joints are affected
• Joints become frozen in place
• First white blood cells come to area, lots of neutrophils that fill synovial fluid, triggers inflammation. Now have potent chemical mediators doing their job over and over again. Cytokines released and are typically messenger cells. Cytokines here do damage. Attack synovial membrane and that breakdown of where we can hold synovial fluid is what forms a pannus. Pannus grows its own blood vessels and starts getting bigger. T cells get involved and T cells trigger fibroblasts which make fibrous or scar tissue. Now we have a joint where capacity to deal with cushion has shrunk, now have fibrous tissue and scar tissue over joint, can have bone on bone, bones can fuse together (ankylosis) now have a joint that loses function since it is so painful and so inflamed. Finally frozen all together.
• RF: RA factor that works against IgG (fights infection, most prominent)
• Typically affects joints symmetrically
• Sx: fever during an exacerbation (systemic inflammatory process), pain, stiffness, joint tenderness, joint deformity (from all the extra fluid and inflammation, pops the bones out of alignment).
• Complications: rheumatoid nodules or cysts can break off and go to other places in body (heart, lungs).
CNS
brain and spinal cord
PNS
cranial nerves and spinal nerves
-afferent: sensory impulses toward CNS
-efferent: away from CNS and toward muscle and organs
-somatic: voluntary control
-autonomic: involuntary
-sympathetic or parasympathetic
Neuron
-primary cell of nervous system, dendrites act as antennas for the cell, synapses are the spaces between the neurons
Spinal Cord
-cervical, thoracic, lumbar
-worse to have a higher spinal cord injury due to brain or everything below it can become affected
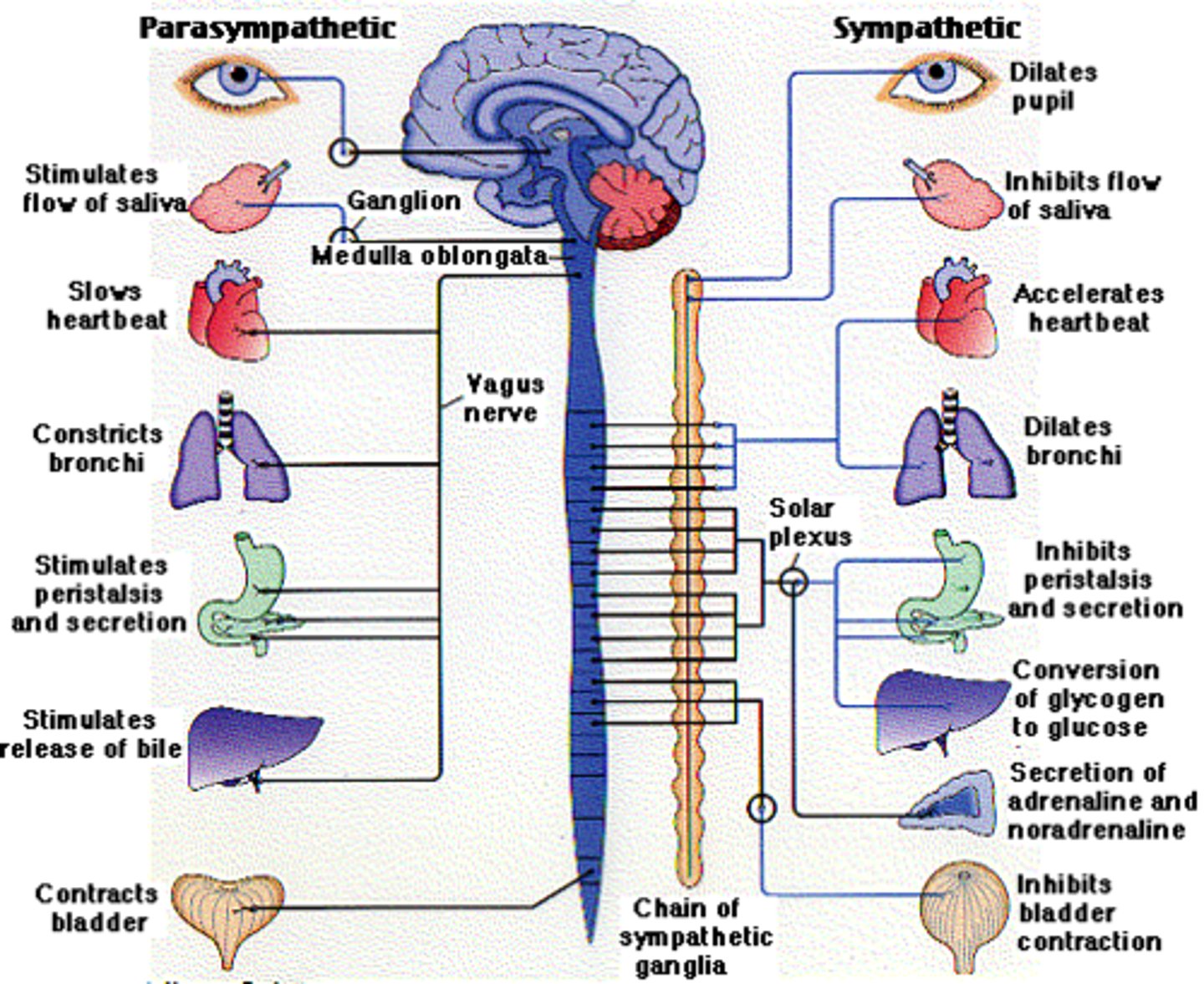
Parasympathetic
rest and digest
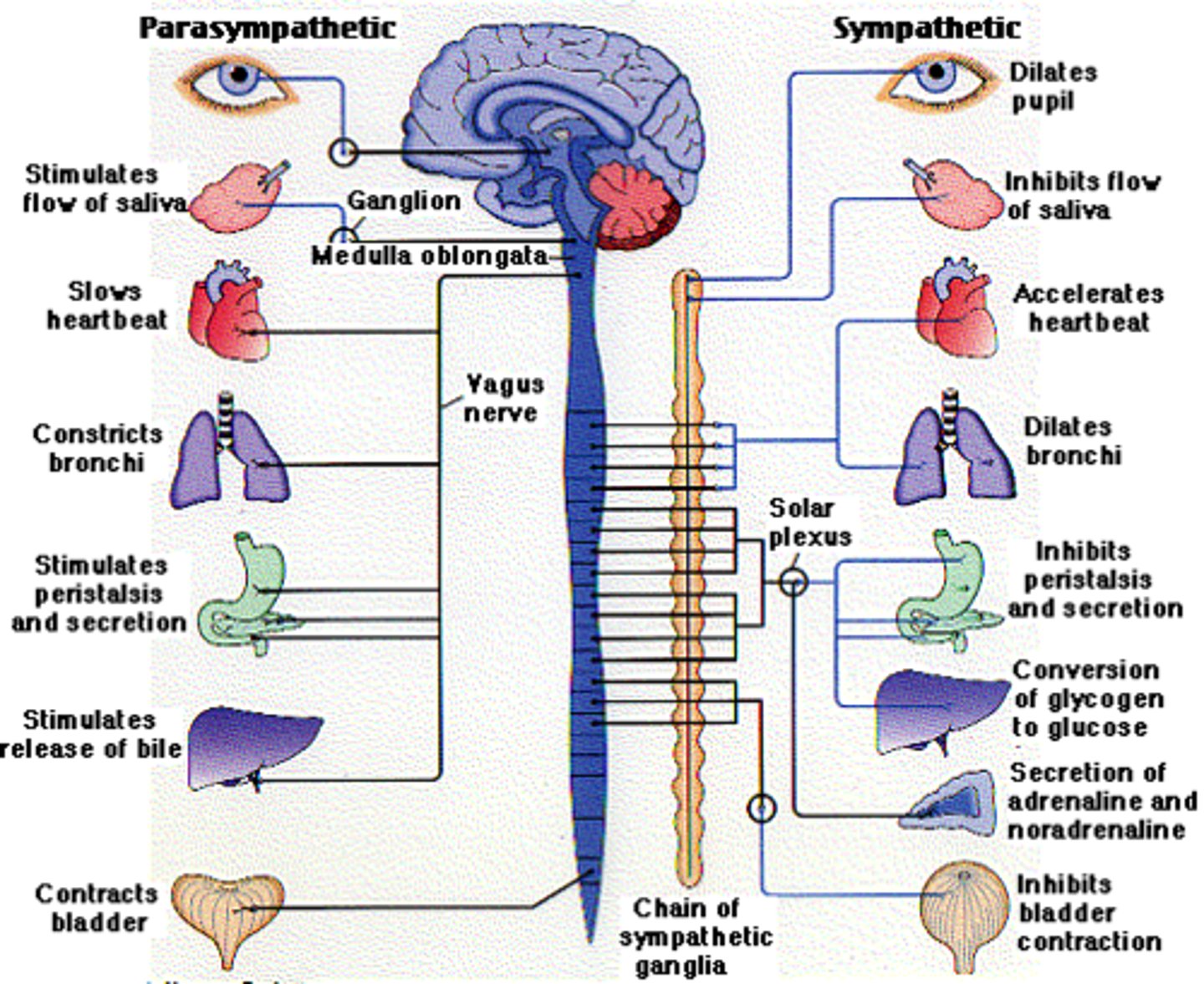
Sympathetic
fight or flight
Pain
-subjective
Pain transduction
ability for the body to sense pain, with dendrites
Pain translation
happens in the brain, brain gets signal and decided what to do with it, interpret info and decide what to do
Pain transmission
ability to transmit signals on afferent and efferent pathways
Pain perception
happens in brain, how you experience pain, unique to every person (how one person thinks of shots)
Pain threshold
happens in brain, the moment at which you consider a stimulus to be painful. Most of us dont think getting BP hurts, but a shot does, is the same person to person
Pain tolerance
happens in the brain, the point at which you must remove a painful stimuli, different from person to person
Pain modulation: excitatory
lower pain threshold, stimulation inflammation to lower threshold to protect injury. Ex: sunburn: lowered threshold so you feel pain easier, when someone slaps your back
Pain modulation: inhibitory
GABA and serotonin block pain translation (how we interpret it in the pain), hormones will decrease message, only happens if you don't have an epidural. Translation gets interpreted and brain says that pain isnt that bad.
Pain modulation: Endogenous opioids
endorphins: natural happy hormones that flood your system, prevent transmission of pain signals
Pain modulation: segmental pain inhibitors
massage, rubbing muscle fiber is going to speak louder than nociceptor that is saying "pain"!
Pain modulation: diffuse noxious inhibitory control
deep massage or acupuncture: stub toe and hit table or dig nails in skin, pain inhibiting pain - focus on that
Pain modulation: expectancy-related cortical activation
placebo: expect it to work so you feel better
Acute Pain
-protective, less than 3 months
Somatic Pain
skin, joints, muscles
Visceral Pain
internal organs
Referred Pain
heart attack, also feel pain in arm and jaw, removed from point of origin
Chronic Pain
more than 3-6 months, no benefit in the body
-all about neurons
Neuropathic Pain
dysfunction with neurons or nociceptors, extremely hard to diagnose
What part of the brain regulates temperature
hypothalamus
Hypothalamus
thermostat of the body, keeps body temp at 36.2 - 37.7. 38 degrees C is a fever.
Fever
○ Resetting thermostat
○ Meet a pyrogen: something that tells hypothalamus to initiate a fever. Inflammation releases pyrogens.
○ Benefits of fever: kills microorganisms. Decreases level of minerals they need for replication - cant replicate. For viruses since they hijack our cells, the high temp change causes lysosomes to break down and blow up to prevent spreading. Lysosomes hold acidic enzymes to burst in viral cells to kill them.
○ Increases speed of immune response
Temp of 105.8 or more
causes nerve damage
Temp less than 95
depresses CNS
Hyperthermia
• Heat stroke
• Compensatory mechanisms have failed
• No wet skin, dry
• Body has done everything it can to get rid of heat and its failed
• Cerebral edema (brain is sensitive to water and salt) major water and sodium depletion. If we don't have enough sodium, then water rushes into cells. Pt can slip into a coma, and then cells go into denaturing process.
• Sx: hypovolemia (tachycardia, hypotension, decrease RR) not enough volume in blood stream. Skin is hot and dry, confused, out of it
- Give IV fluids