Ch. 6 Pt 2 Corticospinal Tract and Other Motor Pathways
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
42 Terms
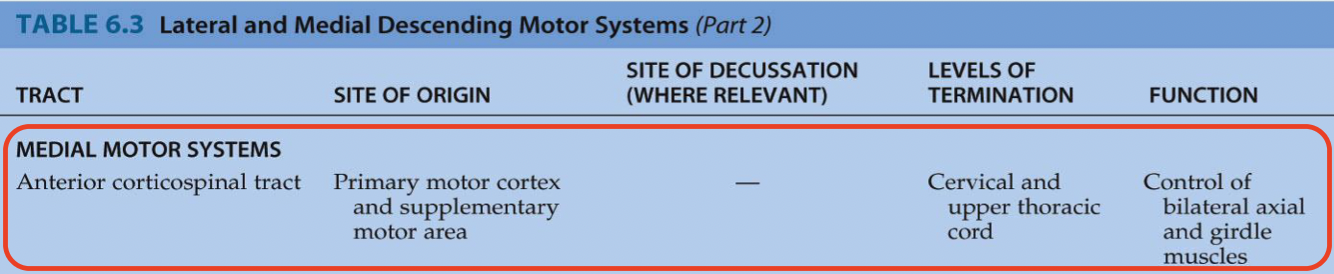
Medial motor pathways - Anterior corticospinal tract:
site of origin?
site of decussation?
levels of termination?
function?
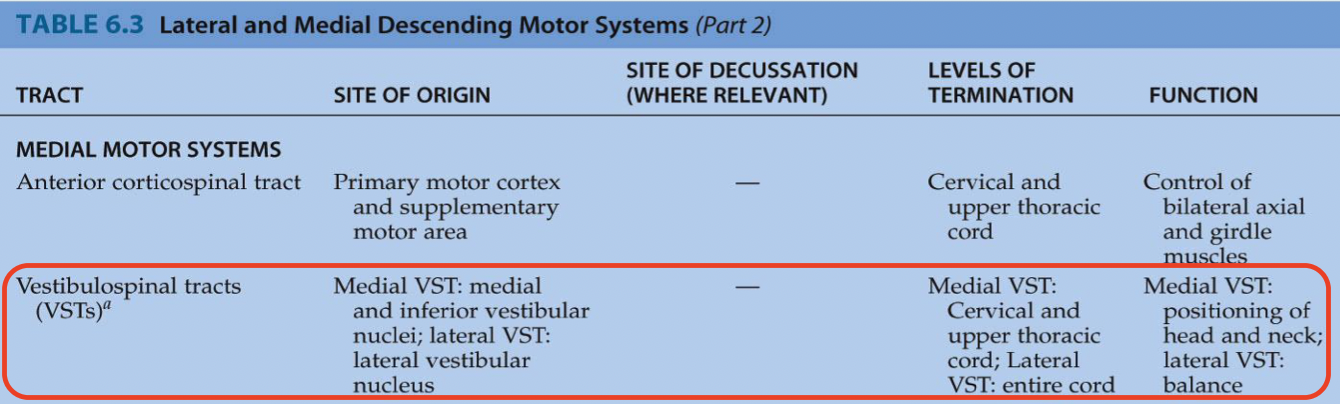
Medial motor pathways - Vestibulospinal tract:
site of origin?
site of decussation?
levels of termination?
function?
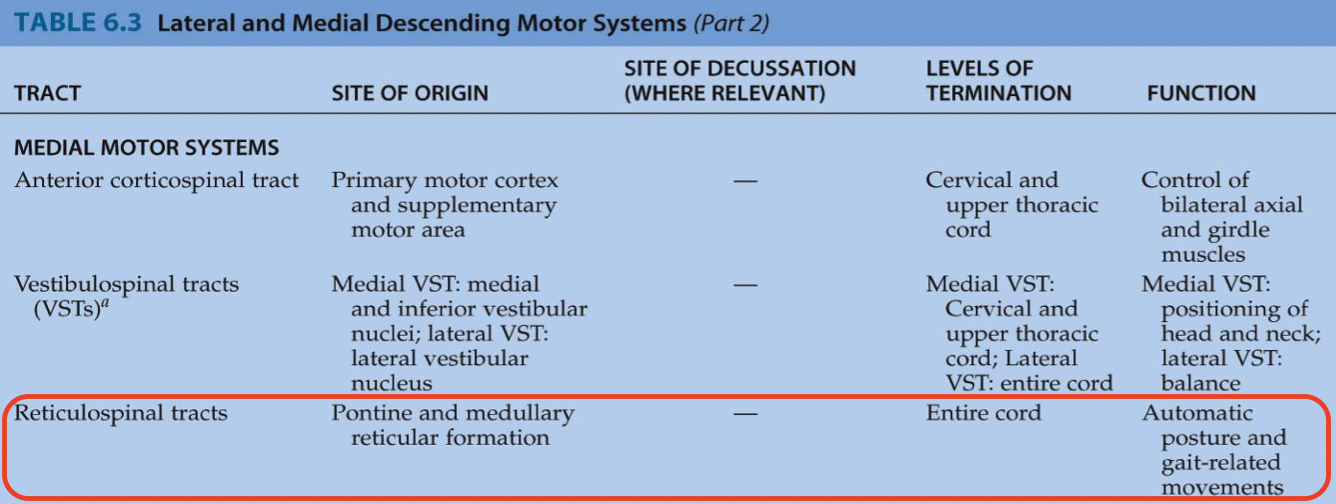
Medial motor pathways - Reticulospinal tract:
site of origin?
site of decussation?
levels of termination?
function?
Medial motor pathways - Tectospinal tract:
site of origin?
site of decussation?
levels of termination?
function?

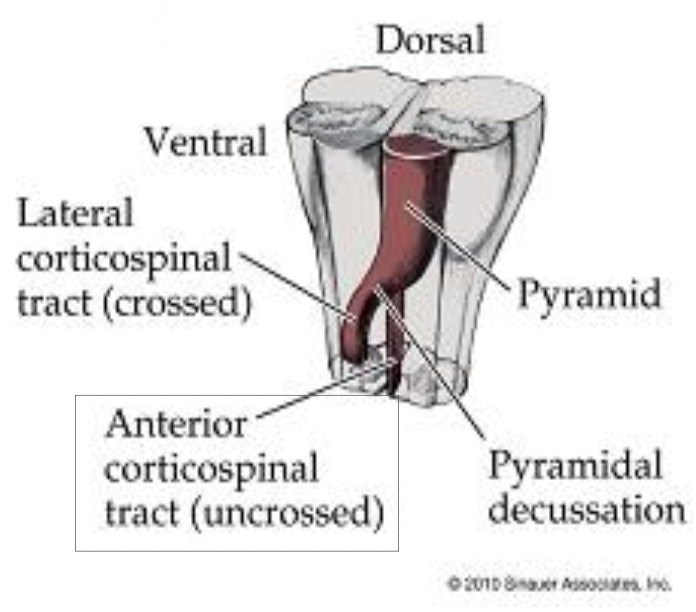
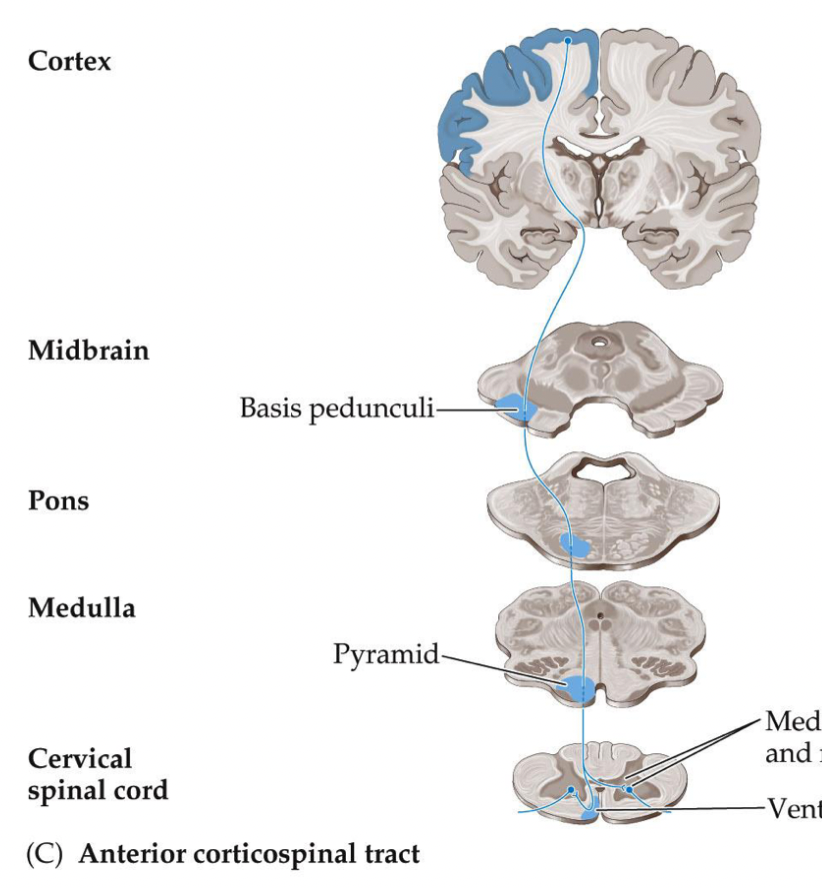
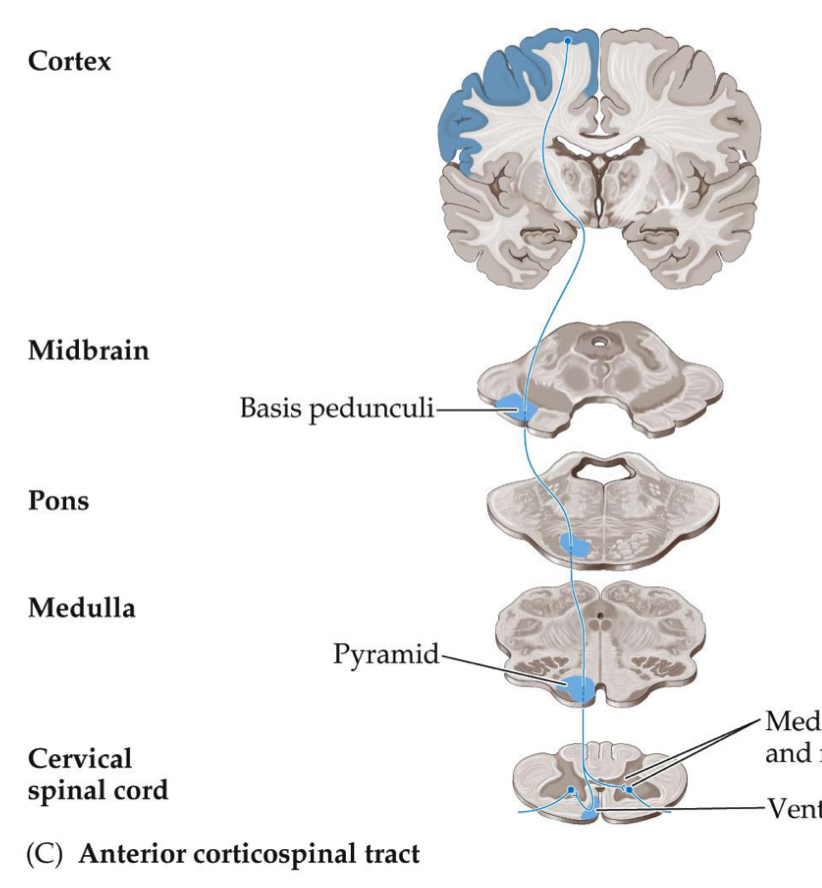
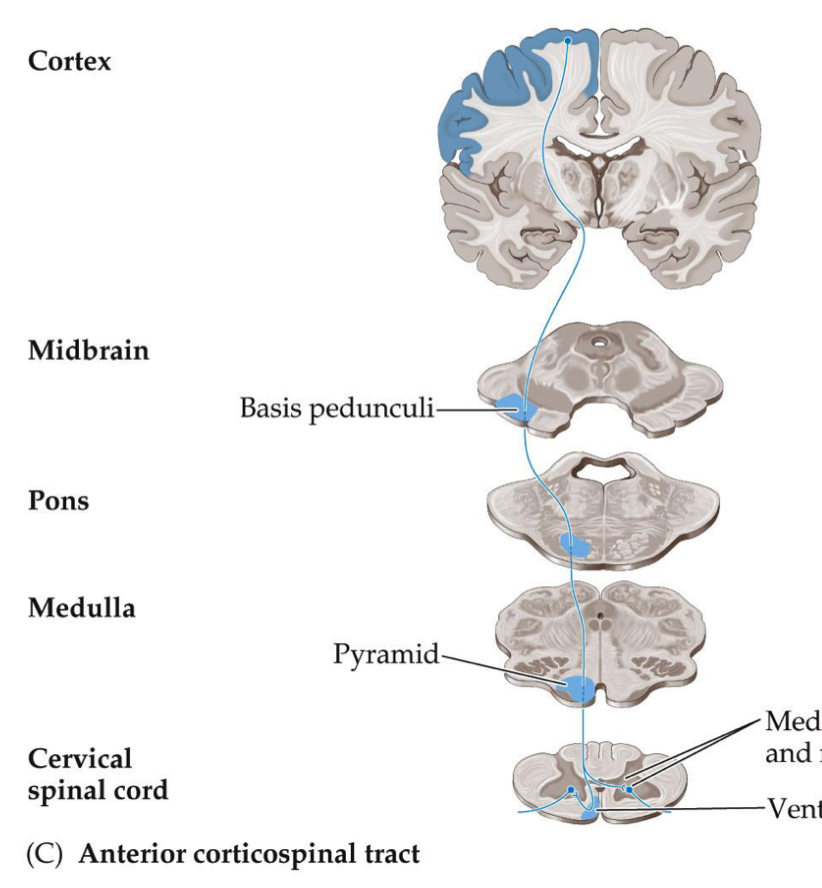
The anterior corticospinal tract has the same origin as what tract? Where is the descent the same until?
same origin as CST, descent is the same until the pyramidal decussation
The anterior corticospinal tract is formed by what axons? Explain what this means for the pathway of the axons when it reaches the “decussation”.
by the 10-15% of axons that do not cross at the pyramidal decussation
- when the axons get to the medulla, it does not cross over; it stays on the same side of the cord
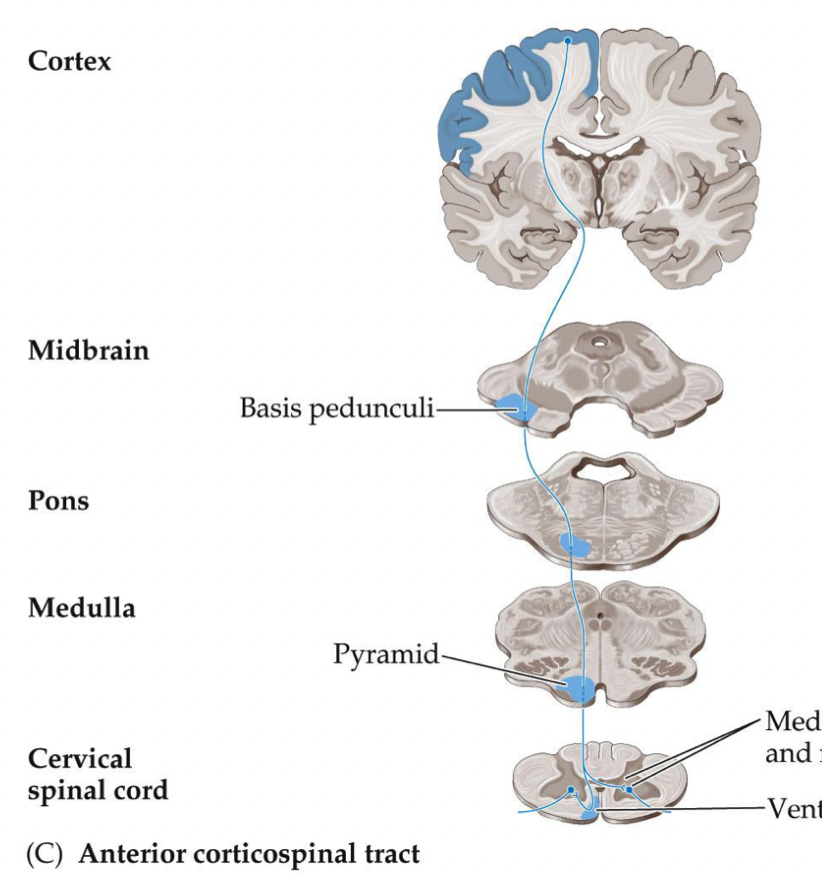
Where does the anterior corticospinal tract descend in the spinal cord? Where does it enter to synapse? Where does it end?
descends in the medial spinal cord to enter the anterior horn to synapse on LMNs
- ends in thoracic cord
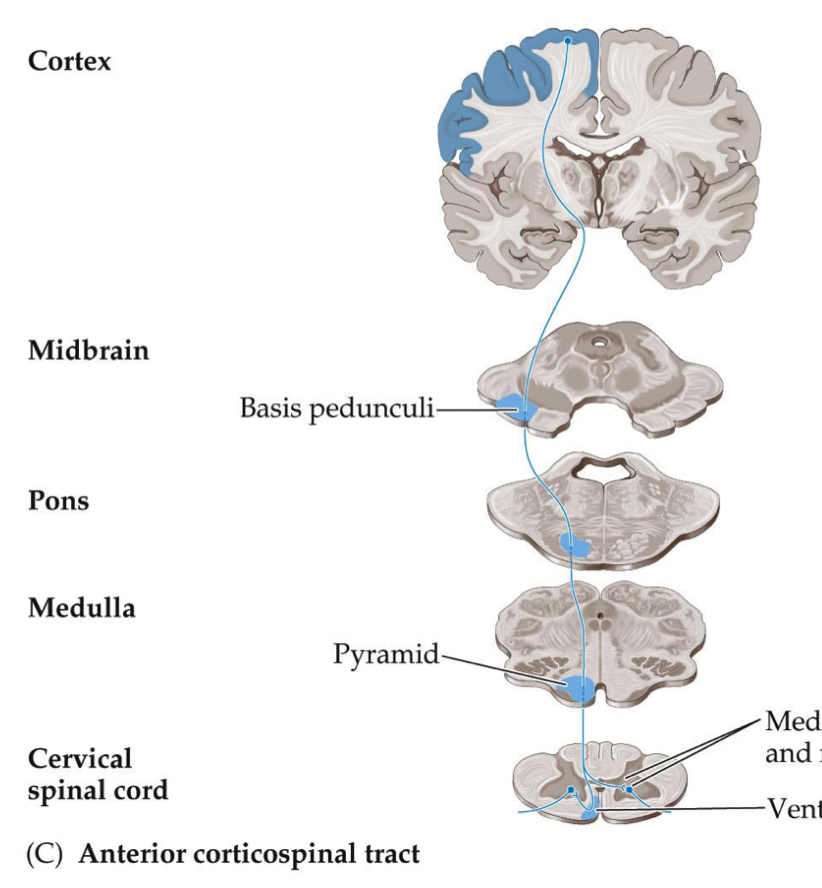
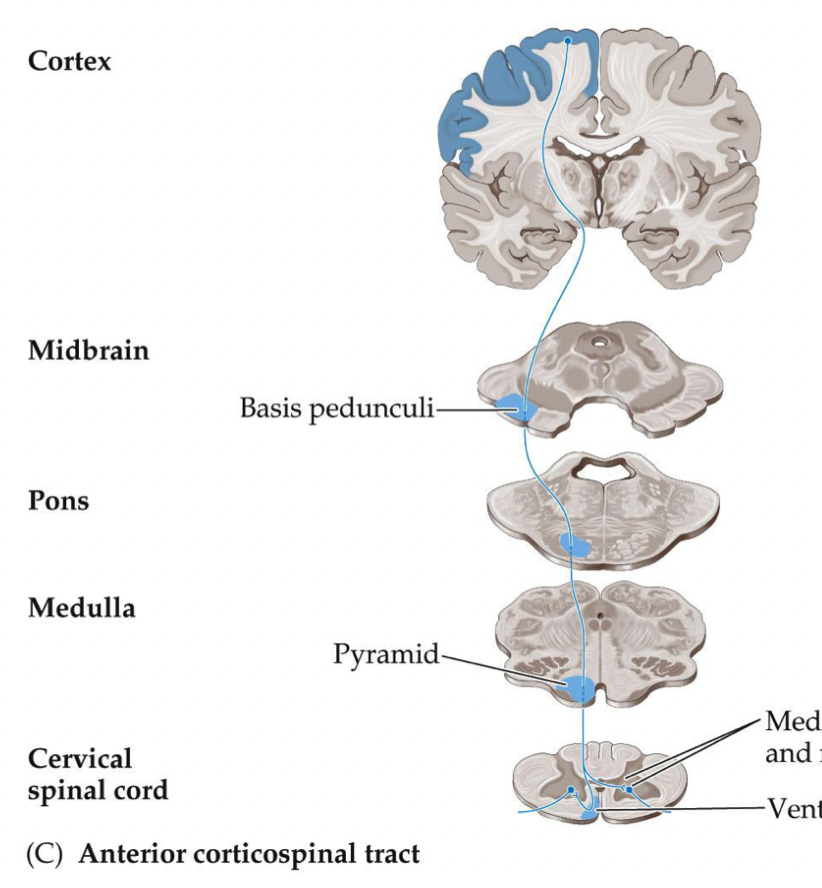
What side of LMNs does the anterior corticospinal tract synapse? What movements does it control?
- synapses on ipsilateral and contralateral LMNs, bifurcates in anterior horn
- controls voluntary movements of bilateral axial and girdle musculature (proximal muscles - neck and trunk)
Explain the physiological importance of the bifurcation of the anterior corticospinal tract in the anterior horn.
when we activate our postural muscles for example, these muscles act in pairs (erector spinae, multifidi, abdominals). you cannot activate the muscle at one specific level or side, they move together
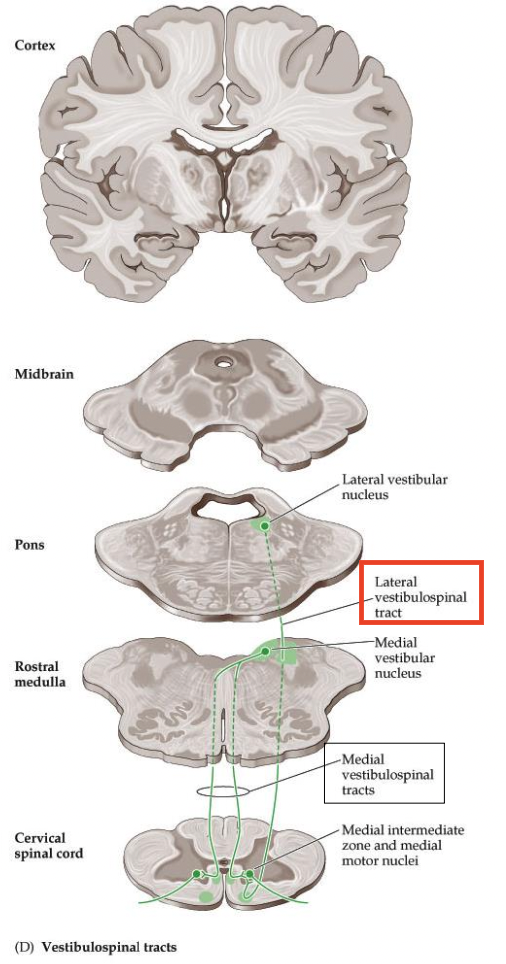
Where does the LATERAL vestibulospinal tract (VST) originate in the pons? Does it descend ipsilaterally or contralaterally?
- originates in lateral vestibular nucleus (pons)
- descends ipsilaterally in the medial SC
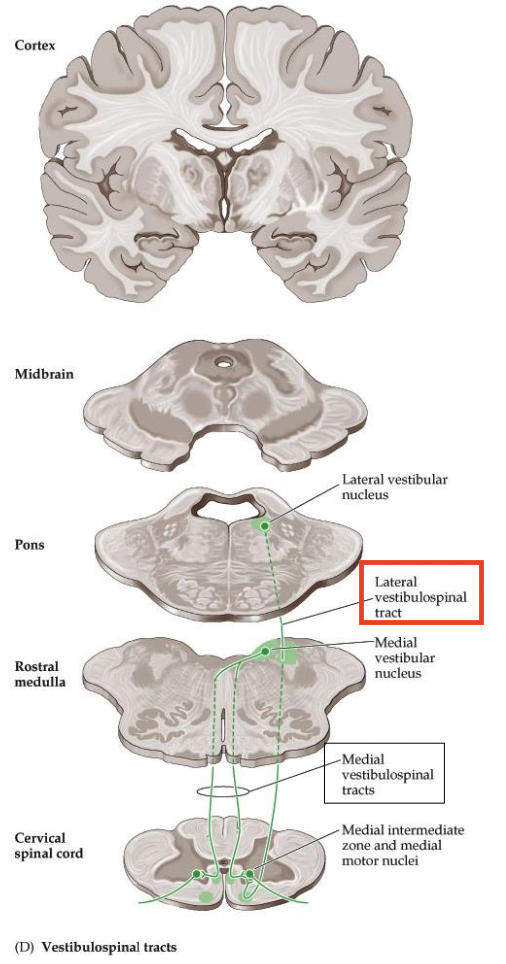
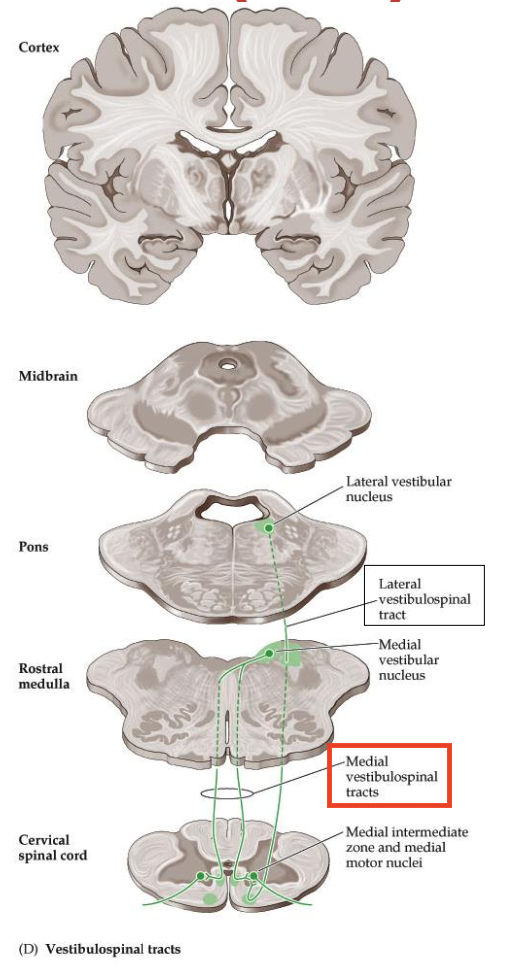
Where does the MEDIAL vestibulospinal tract (VST) originate in the medulla? Does it descend ipsilaterally or contralaterally?
- originates in medial and inferior vestibular nuclei (upper medulla)
- both, ipsilaterally and also crosses over to descend contralaterally —> descends bilaterally in the medial SC
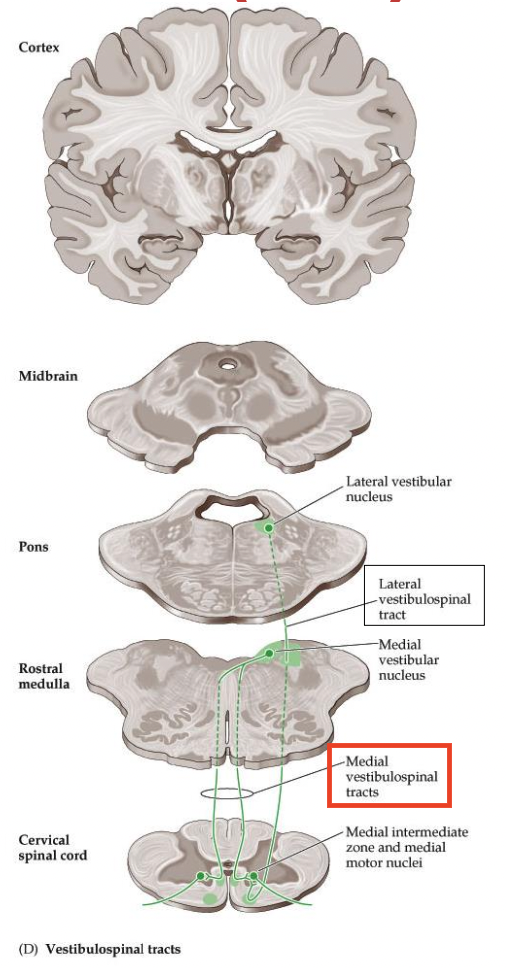
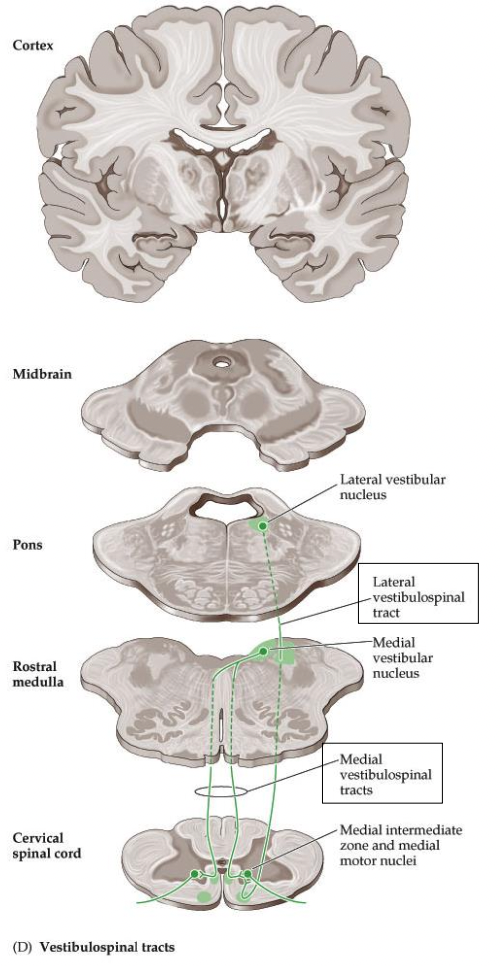
Where do both lateral and medial VST enter to synapse on LMNs?
anterior horn
What does the lateral VST run through? What is it involved in?
- runs through entire spinal cord
- involved in balance
Where does the medial VST end? What is it involved in?
- ends upper thoracic spinal cord
- involved in positioning of head and neck
Understand why the lateral and medial VST are subconscious motor tracts.
- involved in balance or positioning, so postural muscles are always on or else we fall over
- we don’t tell our muscles to contract, they do it subconsciously to keep our balance, or our head and neck upright
- we stand up statically or respond to inertia/gravity
- they could be considered voluntary because we want to stay up, but it is more of the reflexes kicking and keeping you up
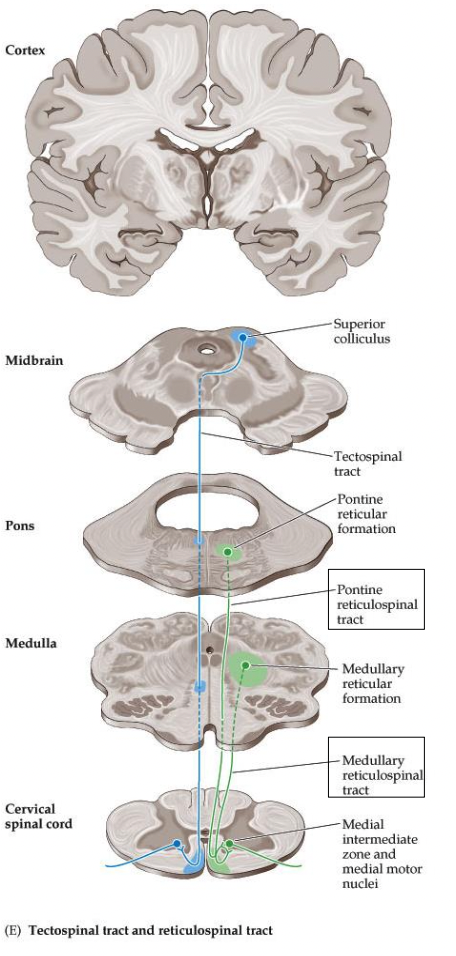
What are the two tracts of the reticulospinal tracts (RST)?
Pontine and Medullary RST
Where does the Pontine RST originate?
in reticular formation of pons
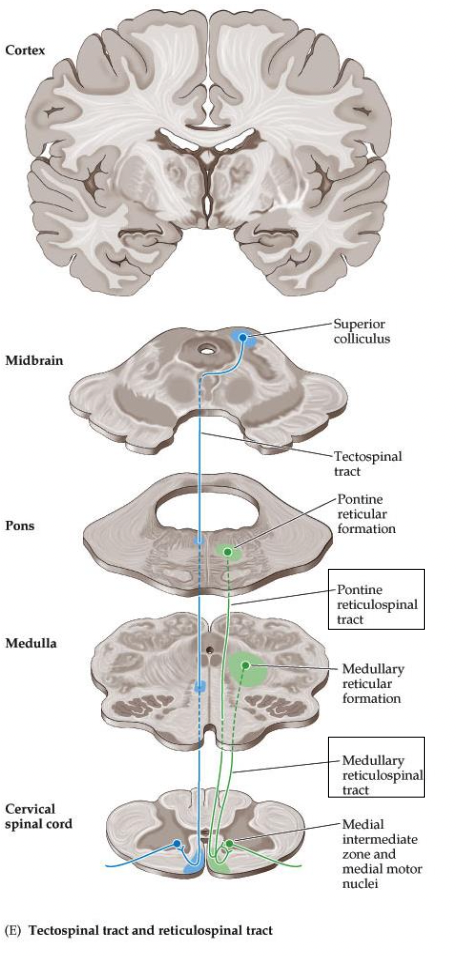
Where does the Medullary RST originate?
in reticular formation of medulla
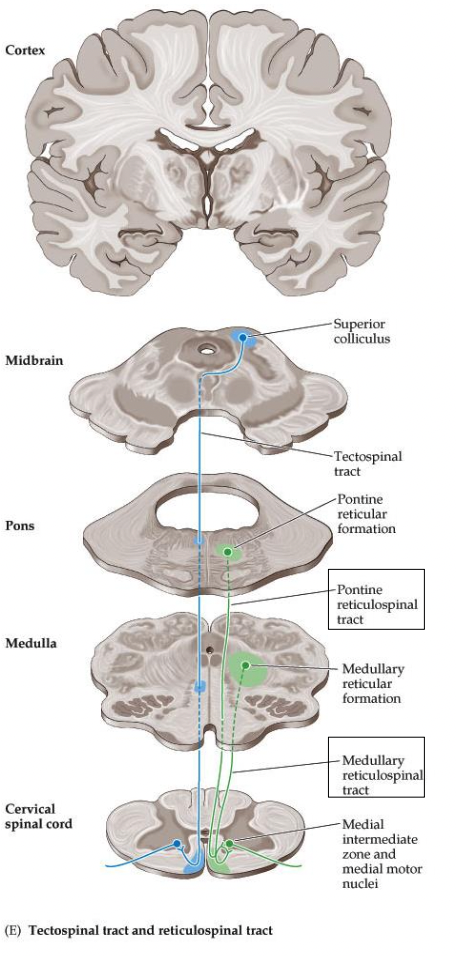
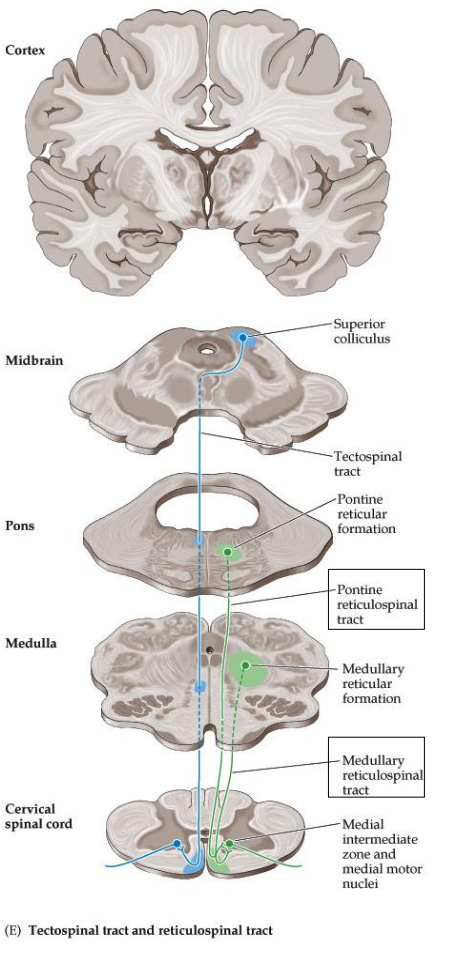
Do both tracts of the reticulospinal tract (RST) descend ipsi-/contra-laterally? Where do they enter to synapse on LMNs? How far do they run through in the spinal cord?
- both tracts descend ipsilaterally in the medial SC
- enters anterior horn to synapse on LMNs
- runs through entire spinal cord
What movements is the reticulospinal tract involved in? Give examples during gait.
automatic posture and gait-related movements
e.g. walking (not consciously telling what muscle to do)
swing phase: do not tell dorsiflexors, hip, knee flexors to bring the limb through
stance phase: knee/hip extensors to keep weight on limb
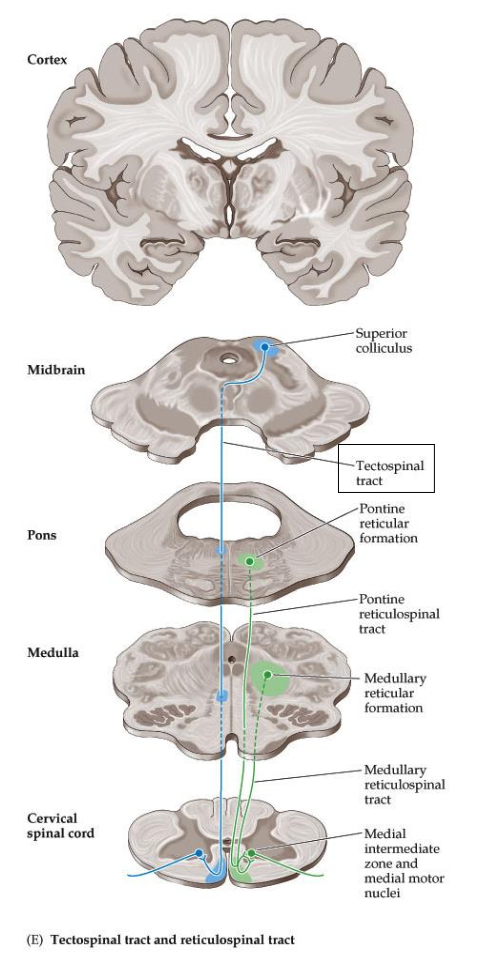
Where does the tectospinal tract originate? Where does it cross over at what decussation? Where does it descend? Where does it end?
- originates in superior colliculus (tectum of midbrain)
- crosses over right away to the contralateral side at the dorsal tegmental decussation
- descends in the medial SC to then enter the anterior horn to synapse on LMNs
- ends in cervical spinal cord
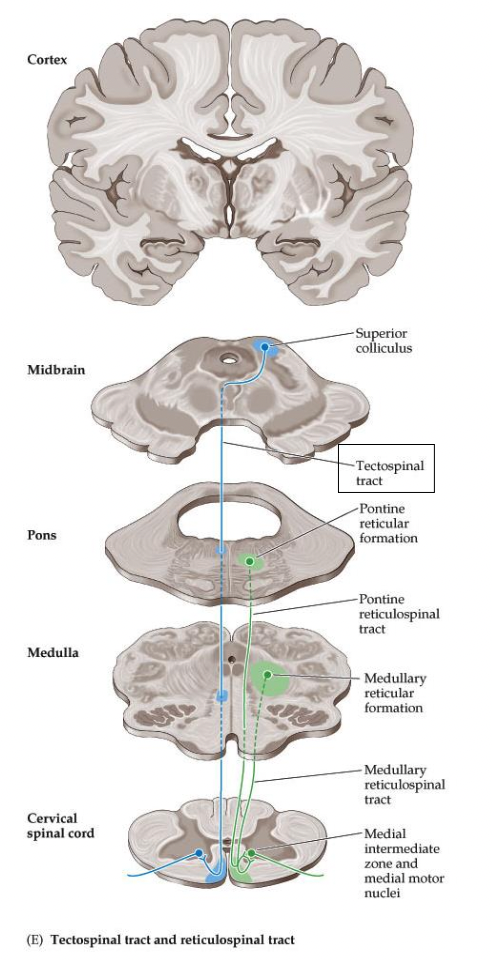
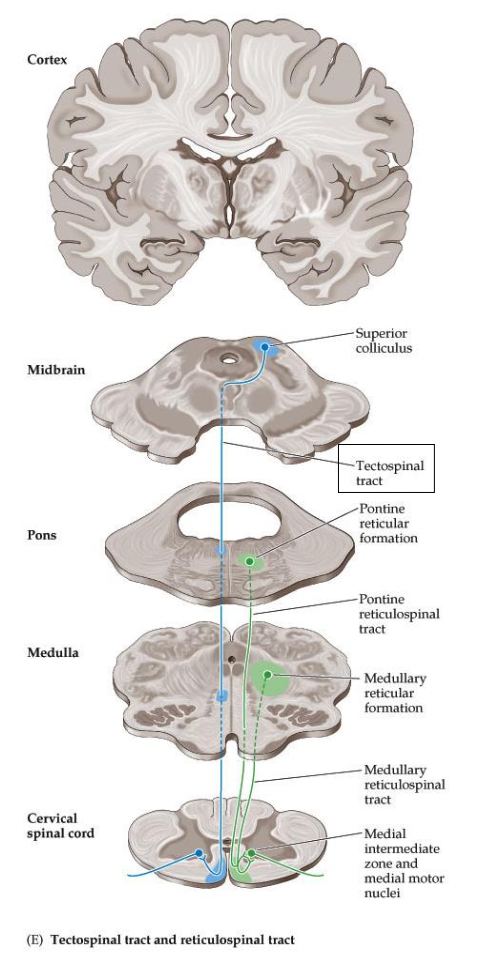
What movements is the tectospinal tract involved in?
coordination of head and eye movements (uncertain in humans)
- in response to loud sounds, flashing lights
UMN vs. LMN lesions - weakness
UMN & LMN: yes, weakness
UMN vs. LMN lesions - atrophy
atrophy -
UMN: no
LMN: yes
UMN vs. LMN lesions - fasciculations
fasciculations -
UMN: no
LMN: yes
UMN vs. LMN lesions - reflexes
reflexes -
UMN: increased
LMN: decreased
UMN vs. LMN lesions - tone
tone -
UMN: increased
LMN: decreased
Using clinical terms to describe weakness denoting the severity, “paresis” means…
weakness (partial paralysis)
ex: hemiparesis - weakness on one side of the body
Using clinical terms to describe weakness denoting the severity, “-plegia” means…
no movement
ex: hemiplegia - no movement on one side of the body
Using clinical terms to describe weakness denoting the severity, “paralysis” means…
no movement
ex: leg paralysis - no movement of the leg
Using clinical terms to describe weakness denoting the severity, “palsy” means…
imprecise term for weakness or no movement
ex: facial palsy - weakness or paralysis of face muscles
Using clinical terms to describe weakness denoting the location, “hemi-” means…
one side of body
ex: hemiplegia - no movement on one side of body
Using clinical terms to describe weakness denoting the location, “para-” means…
both legs
ex: paraparesis - weakness of both legs
Using clinical terms to describe weakness denoting the location, “mono-” means…
one limb
ex: monoparesis - weakness of one limb
Using clinical terms to describe weakness denoting the location, “di-” means…
both sides of body equally affected
ex: facial diplegia - symmetrical facial weakness
Using clinical terms to describe weakness denoting the location, “quadri-” or “tetra-” means…
all four limbs
ex: quadriplegia (tetraplegia) - paralysis of all four limbs
What is a myotome?
Know the key myotomes for the UEs and LEs
the muscles innervated by a single nerve root
~ UE: C5-T1
~ LE: L2-S1
*reminder: go over ASIA key muscles sheet in canvas*
Summary: Lateral motor systems
Control limb movements
• Lateral Corticospinal Tract (CST)
• Most clinically important motor pathway
• Controls skilled voluntary movements for UEs and LEs
Summary: Medial motor systems
• Control proximal trunk movements
• Contribute to balance and posturing
Weakness can be caused by a lesion at any level:
• ___ or ___ cerebral cortex
• UMN of ___ anywhere from ___ to the spinal cord
• LMN anywhere from ___ to the ___ nerve
• ___ junction, muscles, tendons, and/or joints
• Right or left cerebral cortex
• UMN of CSTs anywhere from cortex to the spinal cord
• LMN anywhere from anterior horn to the peripheral nerve
• Neuromuscular junction, muscles, tendons, and/or joints
Know three things that assist with localizing lesions:
1) ___ of a motor system
2) ___ of the brain and SC
3) signs of ___ and ___ lesions
1) pathway of a motor system (cortex, motor neuron, peripheral nerve)
2) somatotopy of the brain and SC (as pathways descend in SC, remember the rule)
3) signs of UMN and LMN lesions (hyper/hypo tonicity/reflexia)
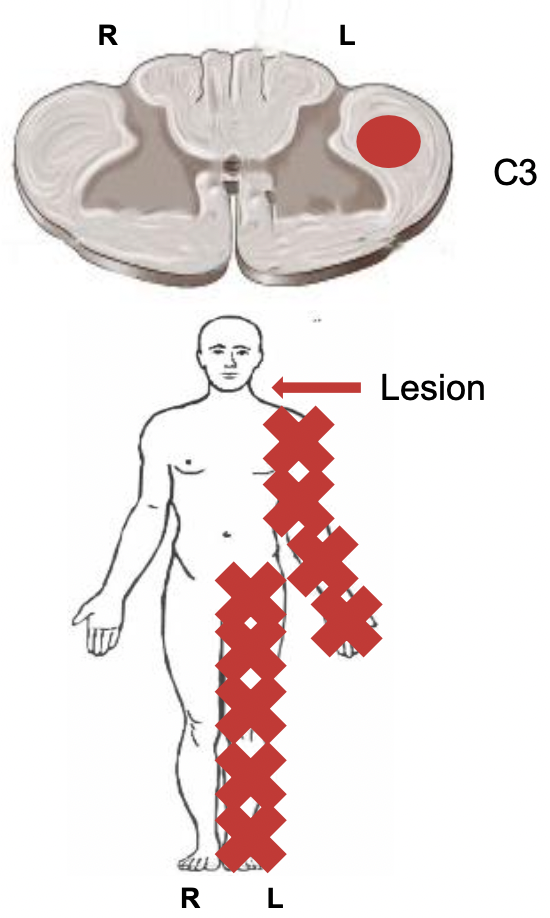
Review question: Lesion of the left lateral corticalspinal tract at C3 produces what impairments?
A lesion to the left lateral CST at C3 causes UMN signs - weakness, paralysis, hyperreflexia, and hypertonicity - in the left arm and leg (at C4 myotome and below)