External & Middle Ear (Exam 2)
1/35
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
36 Terms
Layers of Tympanic Membrane
-Lateral squamous epithelial
-Middle Fibrous
-Inner mucous membrane
Which layer of the Tympanic Membrane will not reform if perforated?
-Fibrous layer
How do the ossicles amplify sound?
-The size difference between the long process of the malleus and incus
-Difference in areas of the ear drum and small oval window
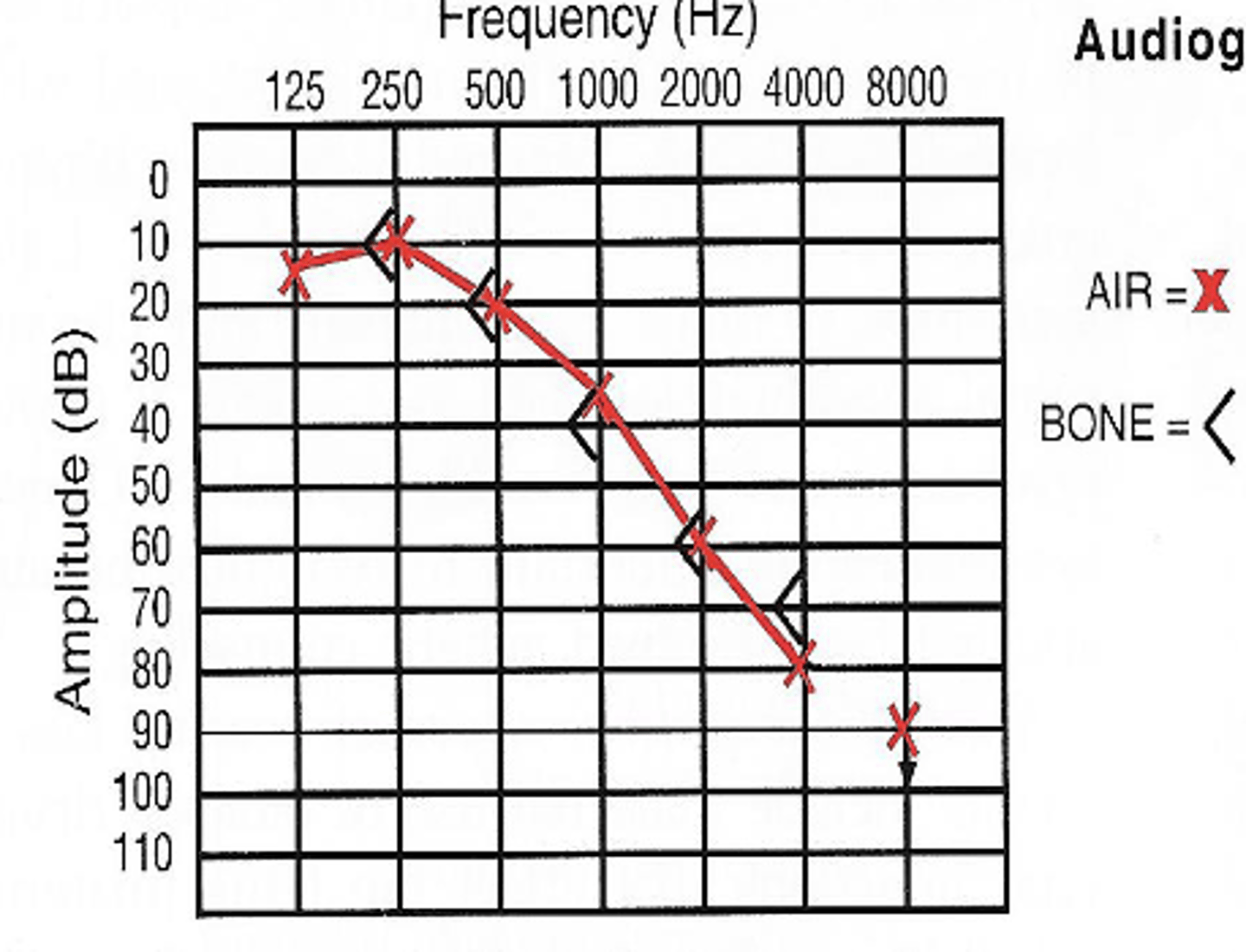
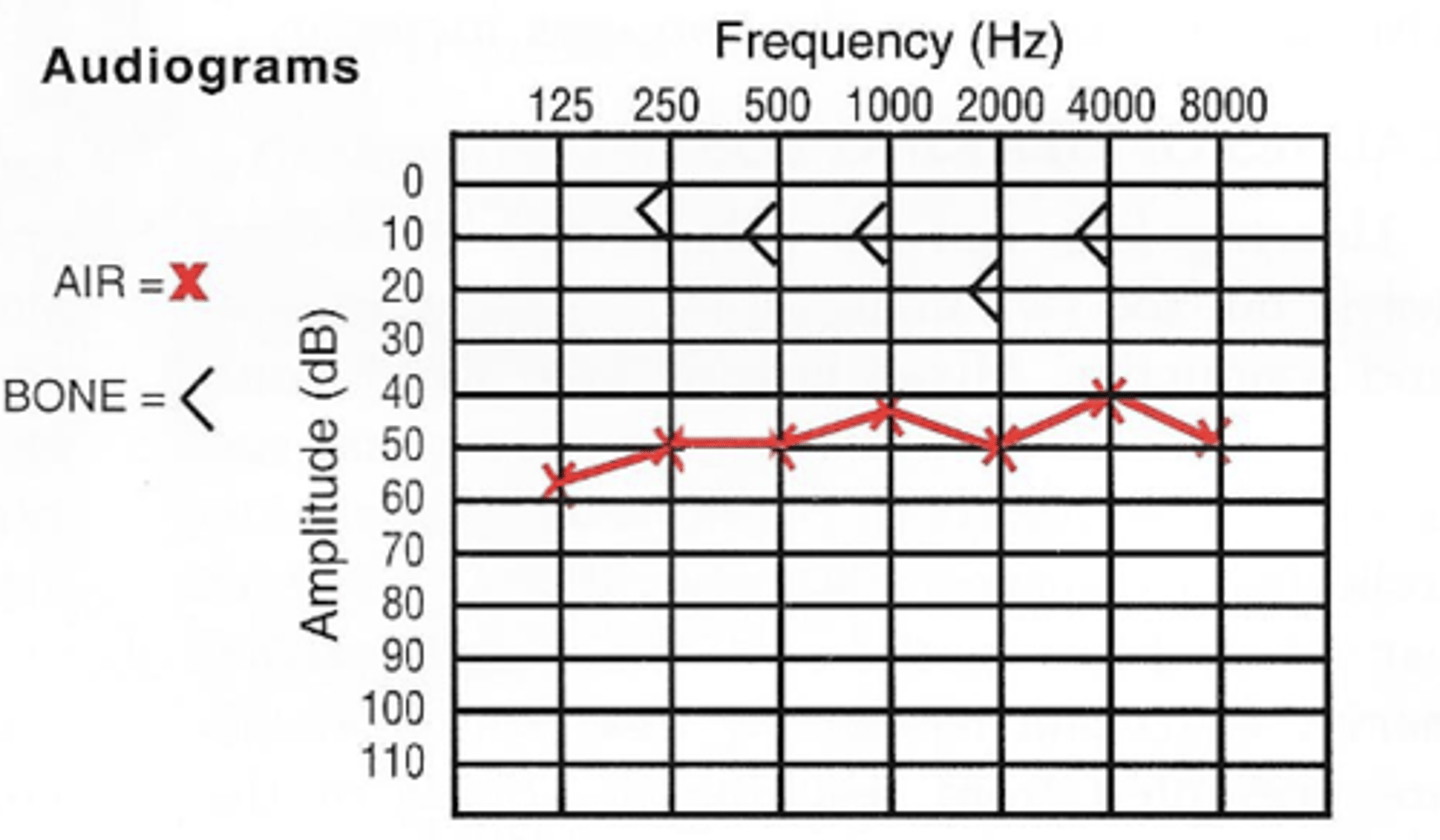
Loss mainly in higher tones; AC & BC affected equally, usually in presbycusis
What would this graph indicate?
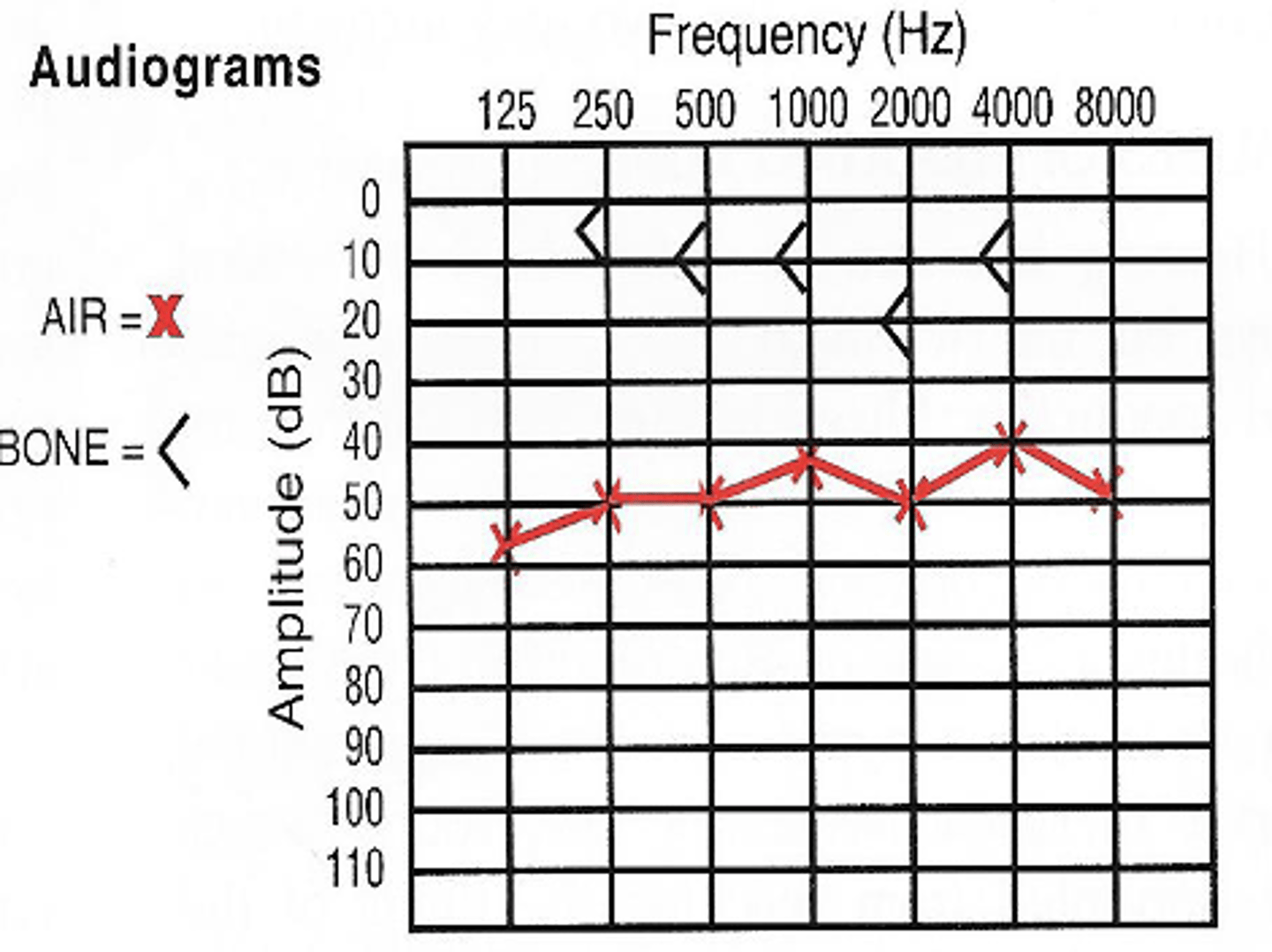
Pure conduction loss; uncomplicated otosclerosis
What would this graph indicate?
Cerumen
-Presents commonly with hearing loss
-Usually complicated when pt uses a q-tip and impacts it onto the ear drum
Cerumen Management
-May use loop or forceps
-Debrox or Peroxide (5 drops) can be curative
-Irrigation with body temp water
Foreign Bodies in the Ear
-Treat individually
-may use forceps for non-living objects
-If an insect is present; kill it first
Treatment for Cauliflower ear
-IND
-If left untreated, the cartilage will shrivel and die
Bacterial Otitis Externa "Swimmer's Ear"
-Agents: P. Aeruginosa; S. Aureus
-TX: Analgesics; topical- Cortisporin or Ofloxacin; Systemic- Phenoxymethyl PCN or Augmentin

Fungal Otitis Externa
-More common in DM
-Black thick debris
-Agents: Aspergillus Niger is MC
-TX: Acetasol plain; or Antifungal drops; Do not use steroid drops; may also mechanically remove
Image shows Acute Otitis Media
-What is this dx of the following image?
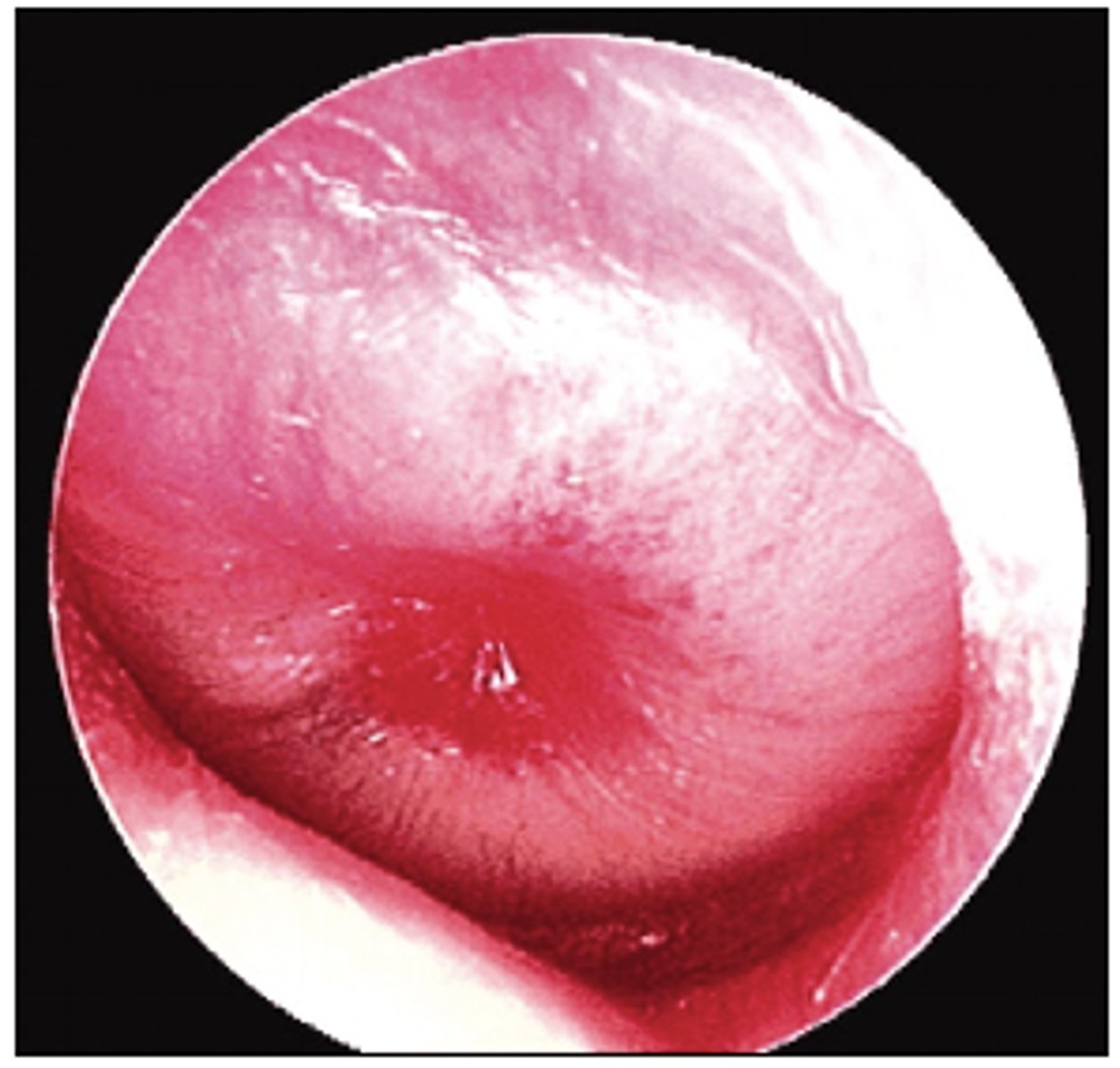
Acute Otitis Media
-Agents: Pneumococcus, haemophilus influenza, Streptococcus
-TX: culture if ear drum ruptured; PCN; Macrolides if PCN sensitive; myringotomy
When is a myringotomy indicated for acute otitis media?
-When symptoms don't resolve after ABX usually after 24 hours
Image shows Bullous Myringitis
What does the image indicate?
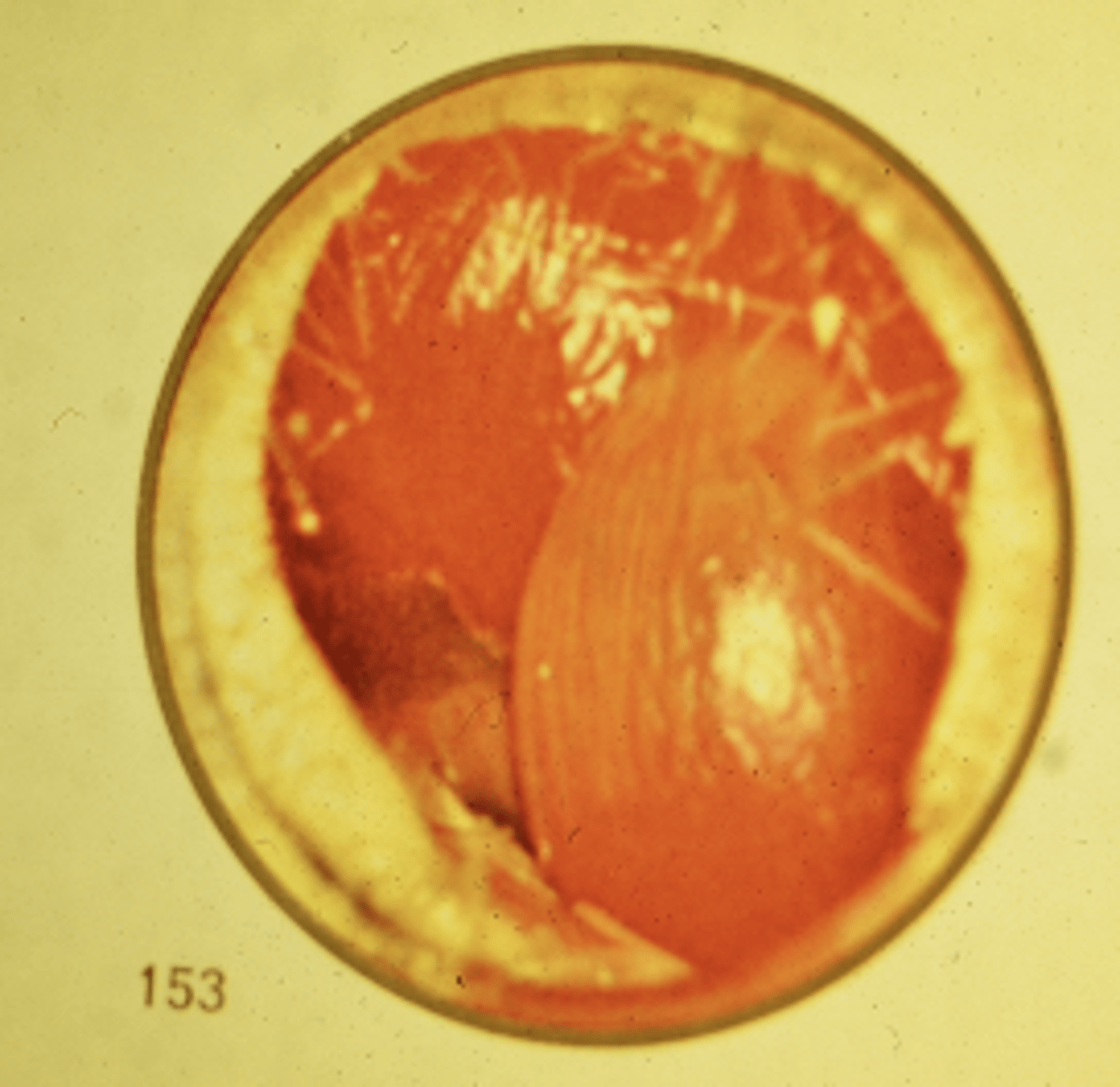
Bullous Myringitis
-Blisters and small lumps on eardrum
-May be partial hearing loss for 2-3 days
-Agents: Mycoplasma & S. Pneumonia
-TX: Oral macrolides; oral or ear drop analgesics; lancing may be necessary
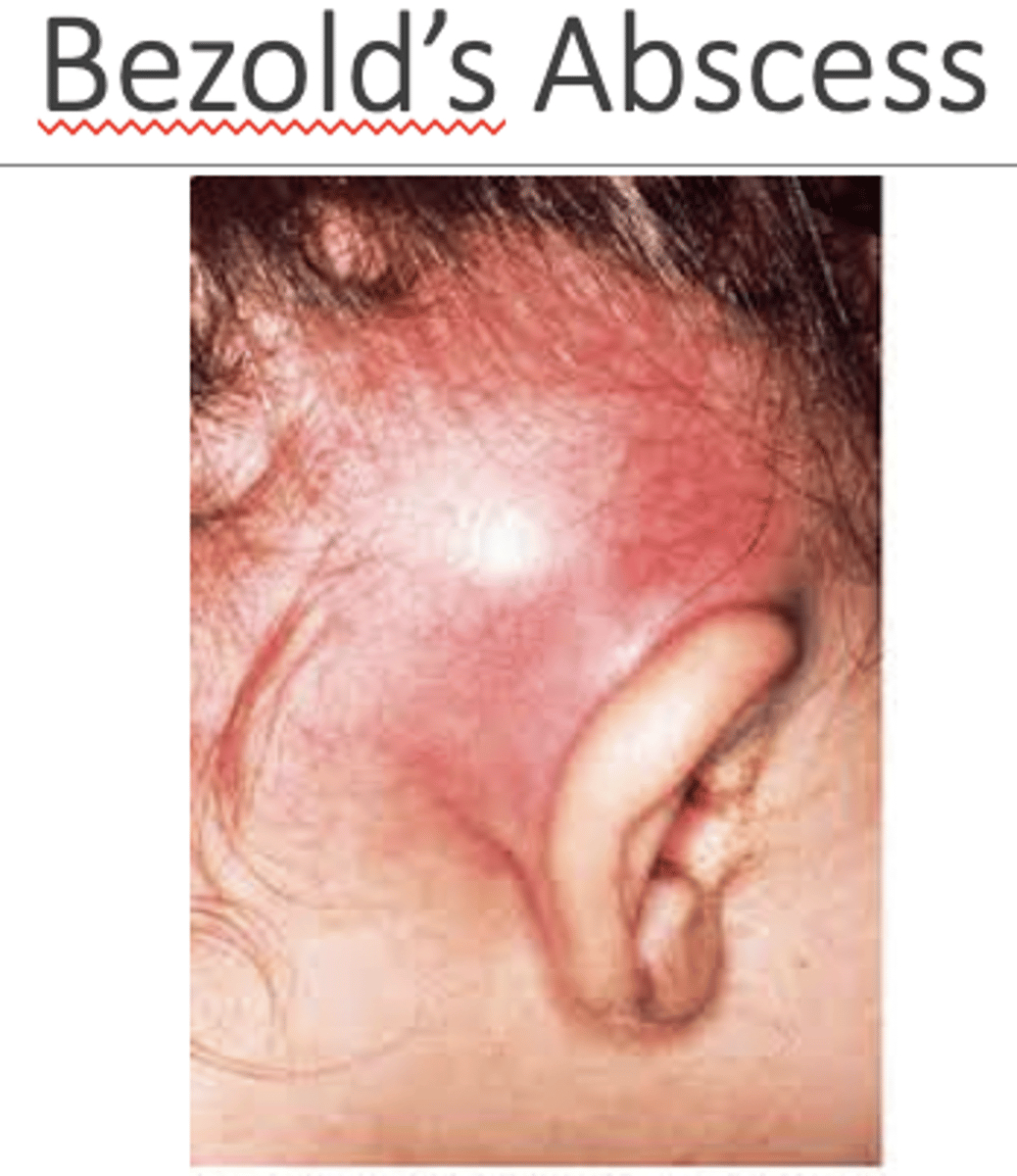
Acute Mastoiditis
-Complication of Acute Otitis Media
-Spreads to antrum of mastoid
-Agents: MC is S. Pneumo
-Symptoms: Hx of AOM; post-auricular pain; erythema; fever
-CT findings: Coalescence of mastoid air cells due to bone destruction
Acute Mastoiditis Treatment
-Based on culture; IV Vanco; if recurrent AOM- Ceftriaxone + Clindamycin
-Surgery
-Myringotomy
-Mastoidectomy: Simple- posterior canal preserved; Radical- Posterior canal sacrificed
Eustachian Tube Function
-Equalization of pressure across TM
-Protects middle ear from infection
-Clearance of middle ear secretions
-Generally closed-opens via tensor vili palatini in yawning
Eustachian Tube Dysfunction (ETD)
-Aural fullness, hearing loss, discomfort with pressure changes, Refraction of TM, Decreased TM mobility, popping sounds, tympanometric eval may be normal
ETD Treatment
-Decongestants
-Systemic steroids
-Nasal steroids (Fluticasone, Beclomethasone)
-Autoinflation
ETD Surgical Procedures
-Tympanostomy
-Balloon Tuboplasty
Barotrauma
-Ear pain/damage to the eardrum/middle ear caused by rapid changes in air pressure
-EX: during descent of airplane or deep sea dive
Treatment of Middle Ear Effusion or Hemotympanum
-Maneuvers to relieve pressure
-Pressure decreasing: Breathing through mouth, yawning, chewing, or swallowing
-Pressure increasing: pinch nose shut, hold mouth closed, blow out gently through nose
Secretory Otitis Media
-Can develop from AOM that hasn't cleared or blacked Eustachian tube
-Causes: Allergies & enlarged adenoids MC; tumors are rare; unilateral effusion in Chinese individual should raise concern
-Can occur at any age but is common in children
-Symptoms: Aural fullness, Hearing loss, lack of pain in absence of infection
-DX: Otoscopy, Tympanometry, Head & Neck exam
Treatment of Secretory Otitis Media
-Decongestants Not effective
-Autoinflation
-Steroids indicated in adult; intranasal for children and DM adults
-Myringotomy and tubes
Types of Perforation
-Central
-Marginal
Etiologies of Perforation
-Traumatic
-Result of Infection
-Acute will spontaneously close in 80% of time
Treatment of TM Perforation
-Tympanoplasty if it does not spontaneously heal
-Avoid water
Otosclerosis
-4& of population
-Occurs in families
-Manifest after puberty, pregnancy or menopause
-Symptoms: Conductive hearing loss bone impeding stapes movement
-May result in sensorineural hearing loss
Treatment of Unilateral Otosclerosis
-Do nothing, cheapest, but still have hearing loss
-Hearing aide
-Surgery: highly successful
Treatment of Bilateral Otosclerosis
-Hearing Aides
-Stapedectomies
Chronic Otitis Media Simplex
-Result of AOM which resulted in unhealed perforation of the Pars Tensa
-Perforation increases, recurring discharge
-Gradual hearing loss due to necrosis
-TX: Tympanoplasty
Chronic Adhesive Otitis Media
-if Serous otitis media not treated, drum becomes retracted
-Partial vacuum results in thinning and stretching of the TM
-TX: Myringotomy & tube
Chronic Otitis Media With Cholesteatoma
-If pars flaccida is drawn by negative pressure, it tends to form a pocket lined by squamous epithelium
-Sheds skin like onion; false tumor expands secreting acid eroding the bones
-Also from perforation of the TM of pars flaccida growing inward
-TX: surgery with mastoidectomy
Neoplasms of the ear
-SCC, BCC, melanoma
-TX: excisions