Sensory pathways; pain, temperature, touch, proprioception pathway
1/86
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
87 Terms
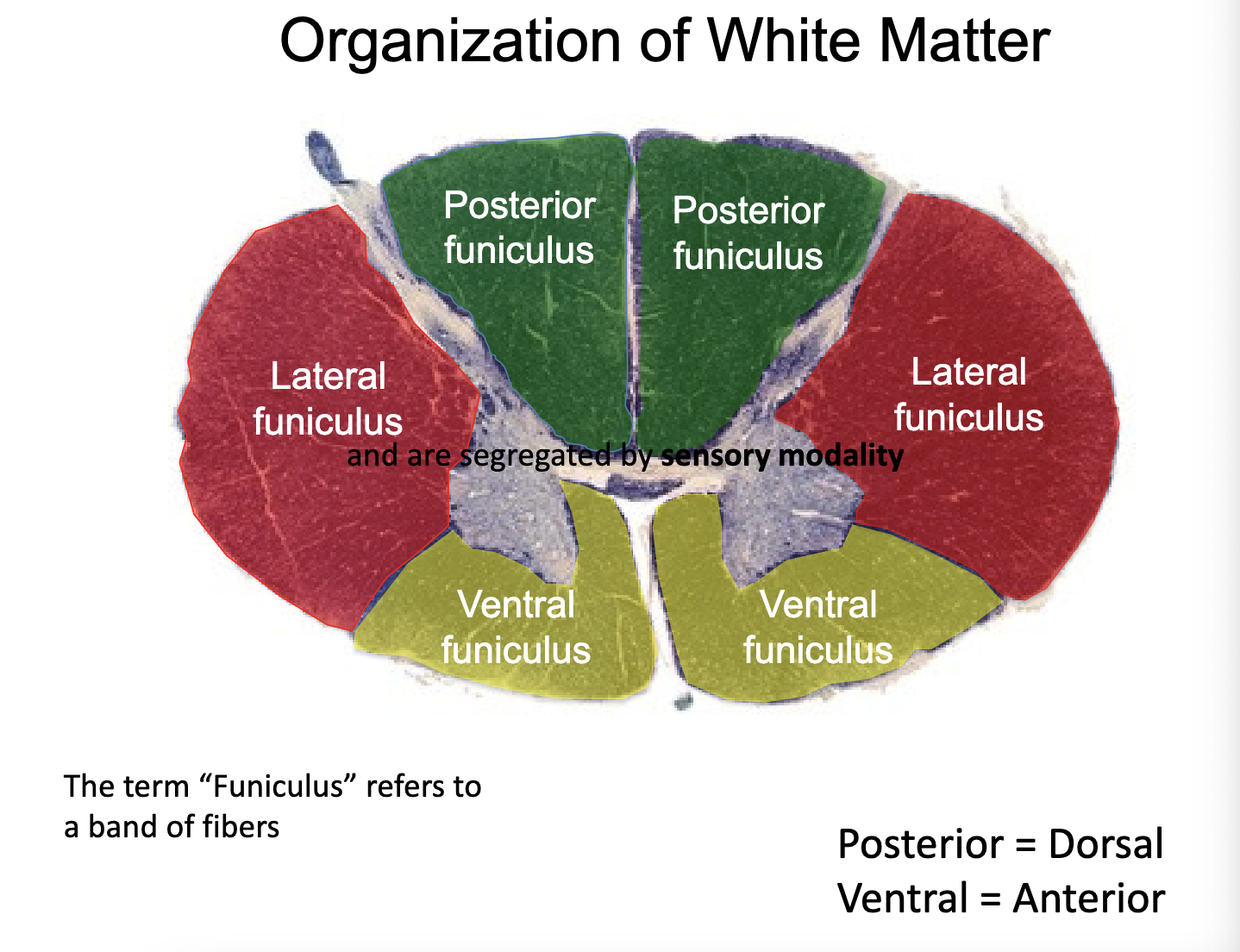
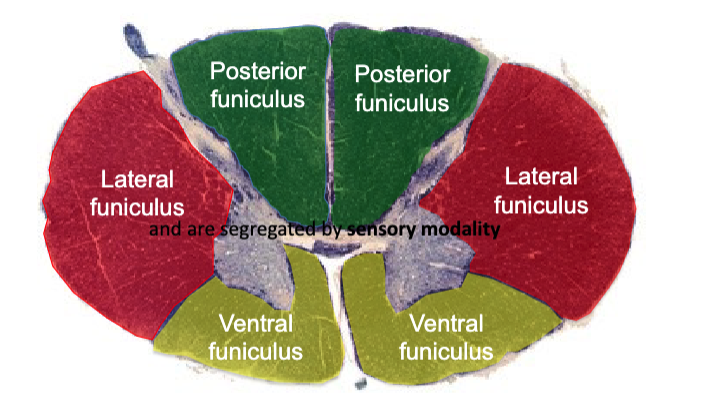
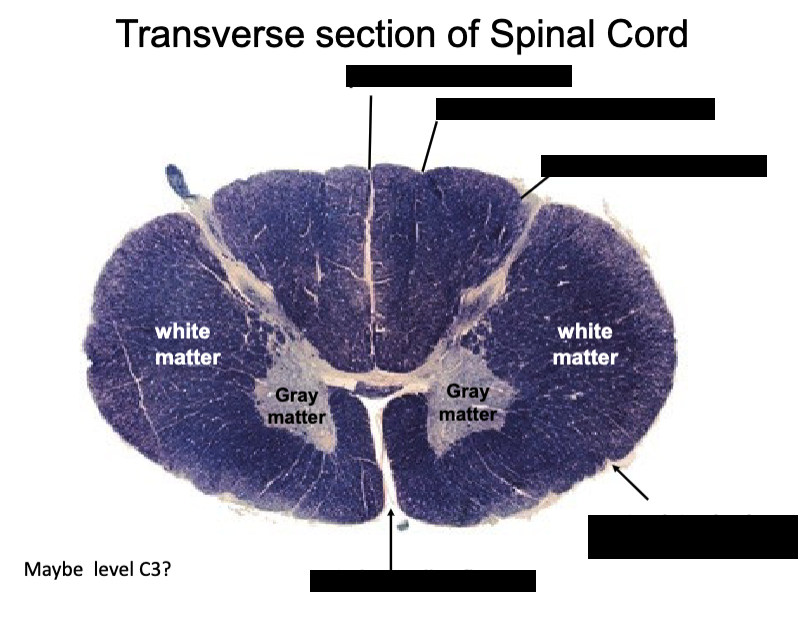
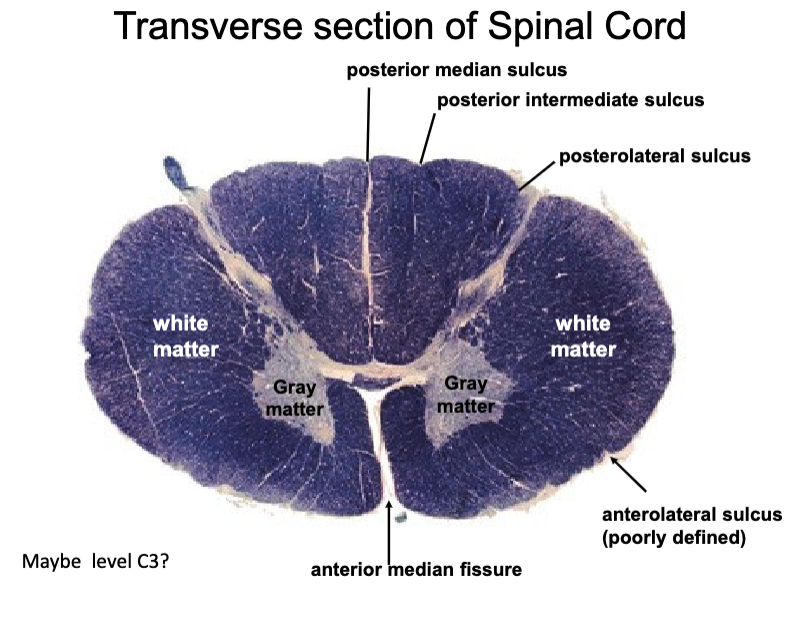
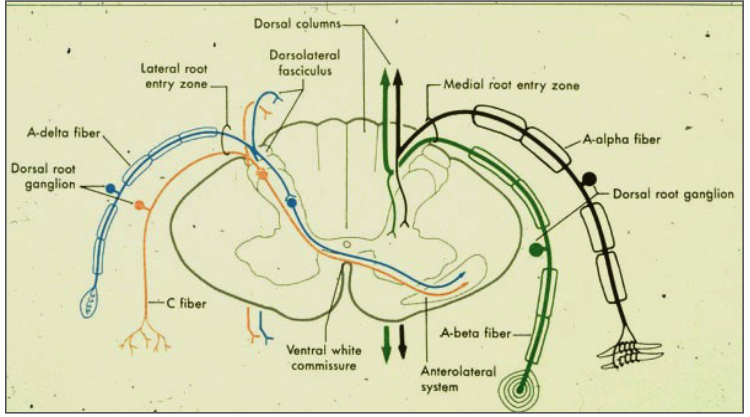
how is the white matter organized?
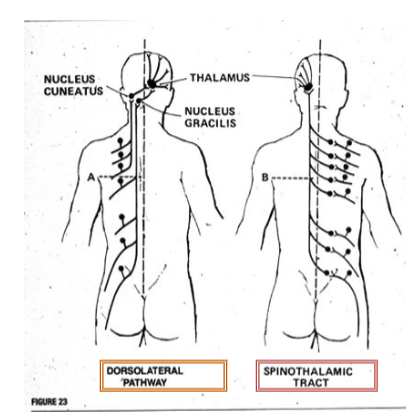
what are the two clinically testable and very important ascending pathways in the spinal cord that reach consciousness?
dorsal column / medial lemniscus pathway
spinothalamic pathway
what is the dorsal column/medial lemniscus pathway?
relays position sense vibration sense and discriminatory touch from the periphery to the cortex
what is the spinothalamic pathway?
relays pain and temperature as well as crude touch from the periphery to the cortex
what is the spinocerebellar pathways?
convey unconscious sensory information from muscles to the cerebellum
the Dorsal columns/Medial Lemniscal pathway and Spinothalamic Pathway are for conscious/unconscious perception
conscious
the spinocerebellar pathways are for conscious/unconscious perception
unconscious
Ascending tracts send sensory info up to the brain and are segregated by
sensory modality
what are the 2 components involved in the Dorsal column - medial lemniscus pathway?
- Fasciculus Gracilis
- Fasciculus Cuneatus
one deals with upper body, other deals with lower
some texts consider the spinothalamic pathway to be 2 divisions that run indistinctly next to each other. what are these 2 tracts?
(we will consider them as 1 for this course)
– Anterior spinothalamic tract (crude touch and pressure)
– Lateral spinothalmic tract (pain and temperature)
what are the 3 tracts that make up the spinocerebellar pathway?
--Posterior (dorsal) spinocerebellar tract
– Anterior (ventral) spinocerebellar tract
– Cuneocerebellar tract
The long tracts bringing information to or from the cortex must _________ during their ascent or descent because...........................
decussate (cross to the other side of the nervous system)
The left cortex deals with the right side of the body
The right cortex deals with the left side of the body
what are the different types of sensory modalities?
proprioception
muscle spindles
golgi tendon organ
touch
fine (discriminatory) vs crude
pain
temperature
t/f: Different sensory endings/structures are sensitive to specific stimuli
Different sensory endings/structures are sensitive to specific stimuli
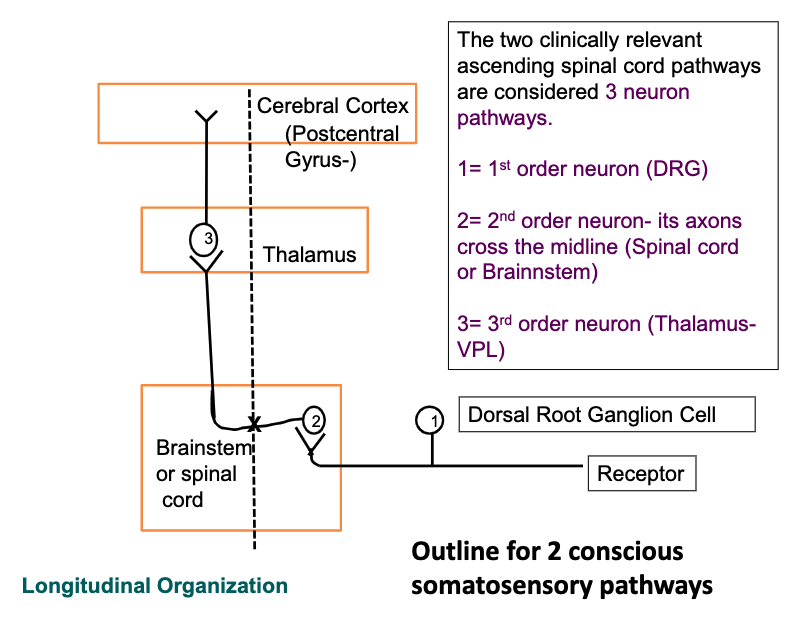
The two clinically relevant ascending spinal cord pathways are considered 3 neuron pathways. Wha are the 3 neurons?
1st order neuron → DRG
2nd order neuron → axons cross midline; in spinal cord/brainstem
3rd order neuron → thalamus
all information heading to the cerebral Cortex must stop at the _______ with one exception….?
thalamus
Olfaction
what role does the thalamus play in cortical function/activity?
gatekeeper for the cortex
All information heading up to the cortex synapses in the thalamus where it can be integrated and distributed to the appropriate cortical region
3rd order neurons
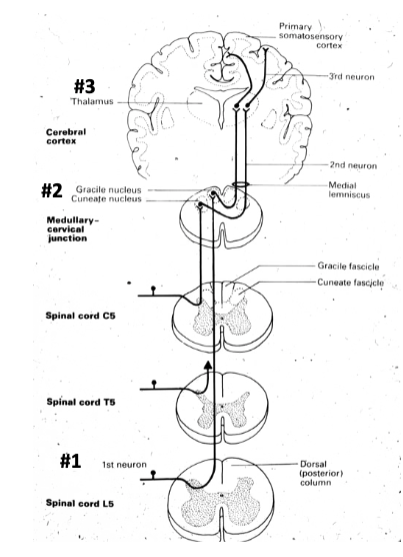
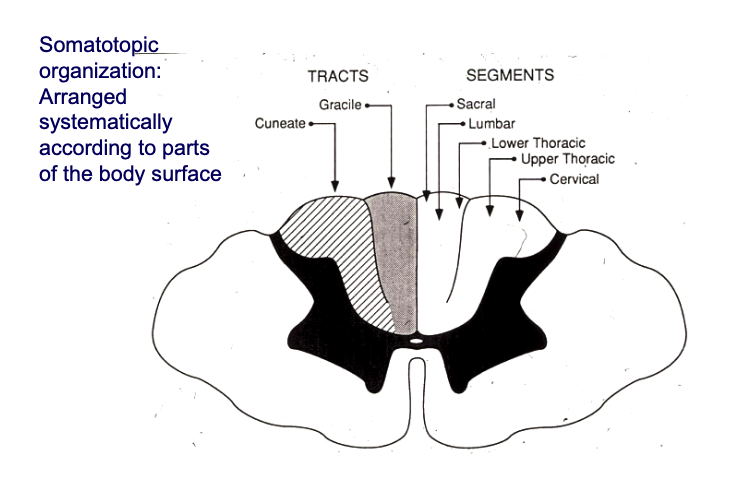
which part of the posterior column pathway is the fasciculus gracilis? fasciculus cuneatus? (which regions carry fine touch, pressure, vibration, and proprioception from which spinal levels)
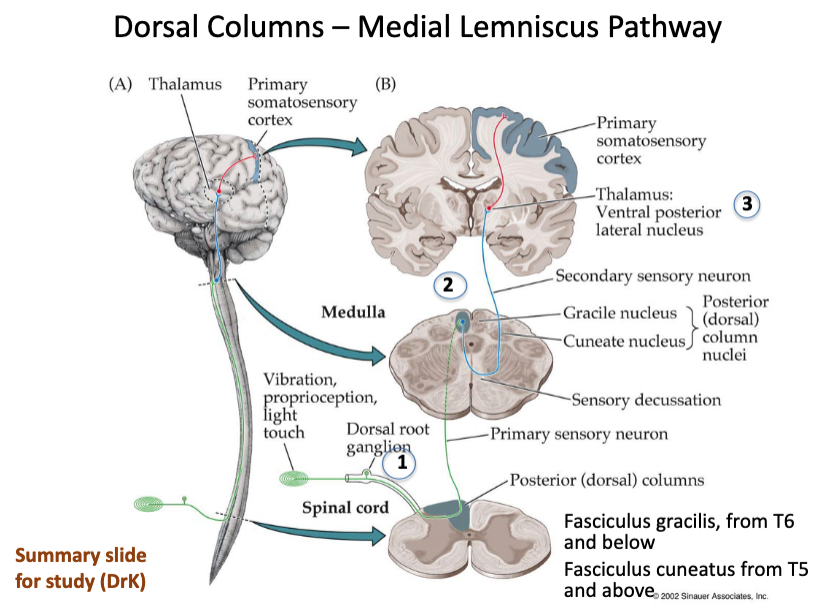
fasciculus gracilis = from spinal level T5 and above
fasciculus cuneatus = from spinal level T6 and below
which sensory modalaities are involved in posterior column pathway?
position sense
vibration sense
2-point discrimination
where does the posterior column pathway decussate?
at column medella where nucleus gracillis and nucleus cuenatus are located (2nd order neurons)
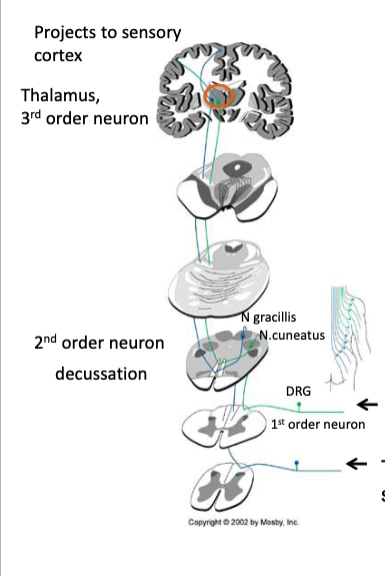
describe the posterior column (dorsal column) pathway
1 order neuron in DRG
2nd order neurons (N. gracilis and N. cuneatus) in column medulla
sensory decussation: secular neuron crosses over to opposite side to form medial leminiscus and heads up to thalamus
from thalamus, reaches up to primary somatosensory cortex
how is the dorsal column pathway somatotopically organized?
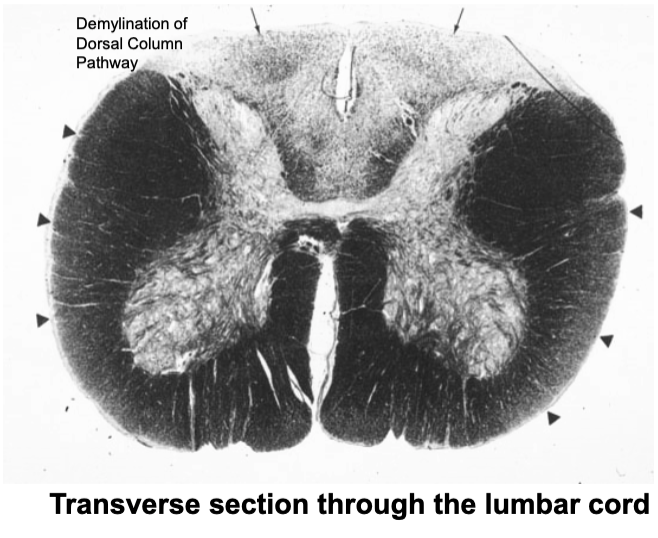
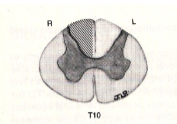
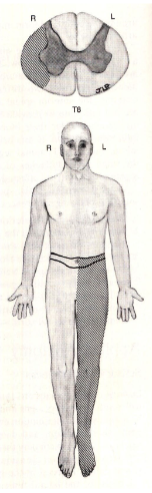
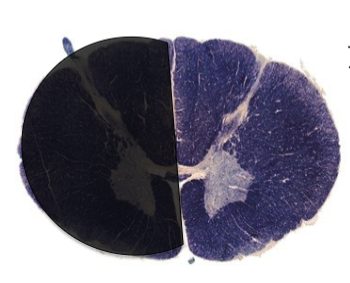
What would you expect to observe upon examination of this patient?
loss of proprioception of lower extremeties (can’t walk to bathroom in the dark unless he can see his feet)

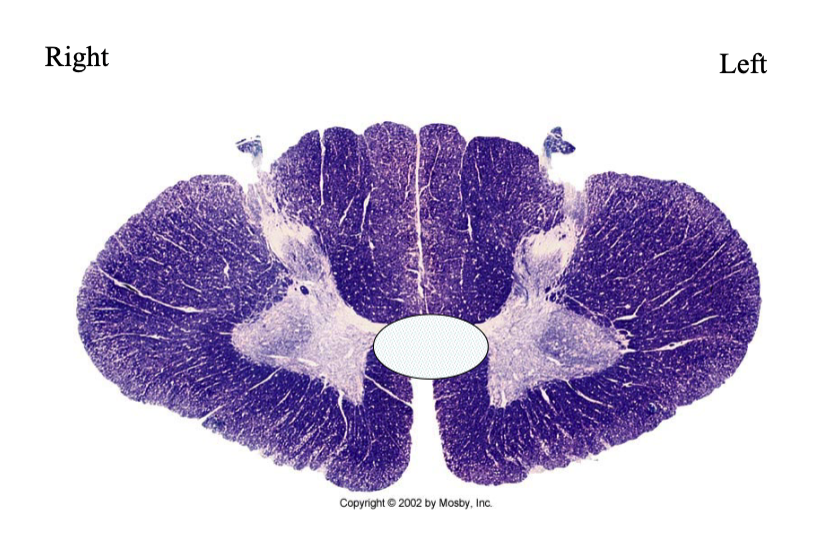
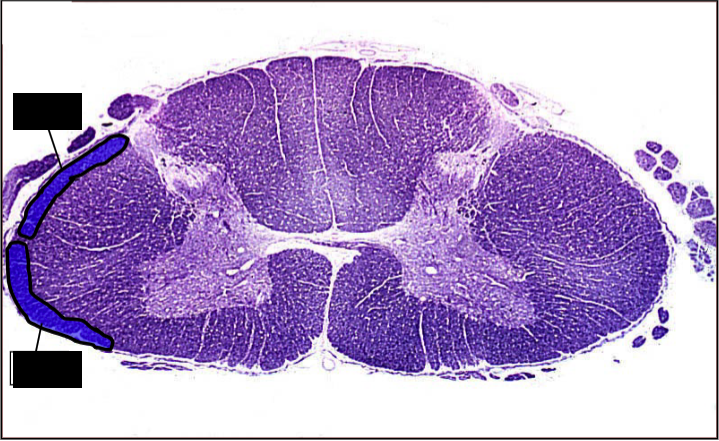
This image shows demyelination of Fasciculus Gracilis in a section through the cervical enlargement. (white region medial)
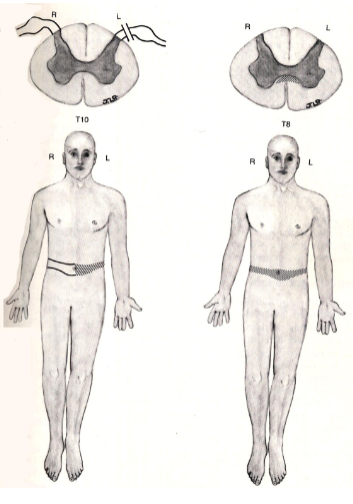
What would you expect to observe upon examination of this patient?
loss of proprioception of lower extremeties (can’t walk to bathroom in the dark unless he can see his feet)
a lesion of the fasciculus cuneatus would result in what clinical presentation?
loss of proprioception of upper extremeties
a lesion of the fasciculus gracilis would result in what clinical presentation?
loss of proprioception of lower extremeties
fine touch, pressure, vibration and proprioception are all sensations that the body is consciously/unconsciously aware of
consciously
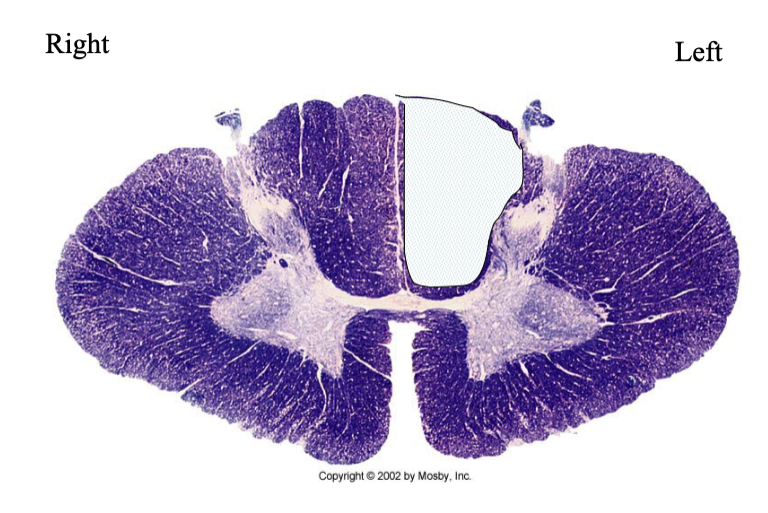
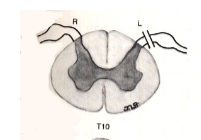
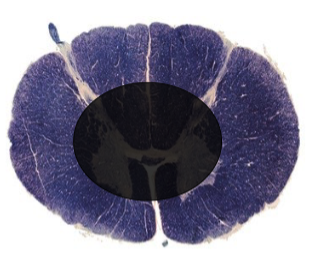
What findings would you expect to see in an individual with this lesion?
this lesion encompasses fasciculus cuneatus AND gracilis so problems with fine touch, pressure, vibration and proprioception on ENTIRE LEFT side of body
pathway must reach up to column medulla to cross
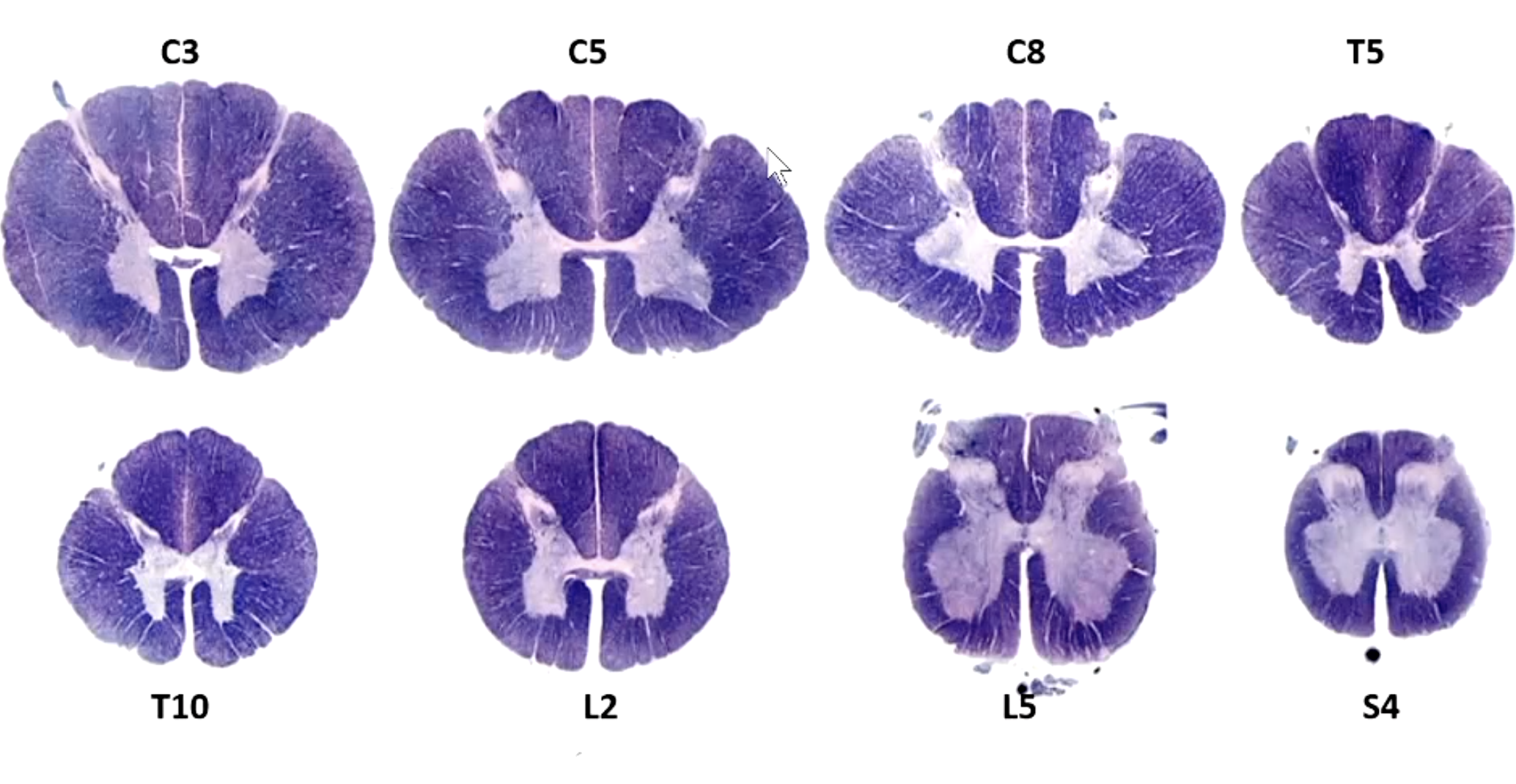
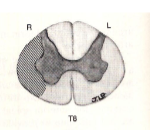
which spinal levels depicted here depict BOTH fascilicus cuneatus and gracilis? which ones only have 1
BOTH → T5 and above
only gracilis → T6 and below
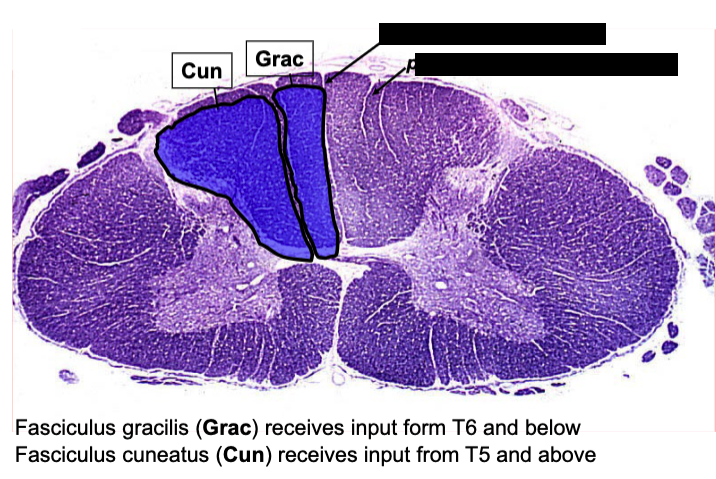
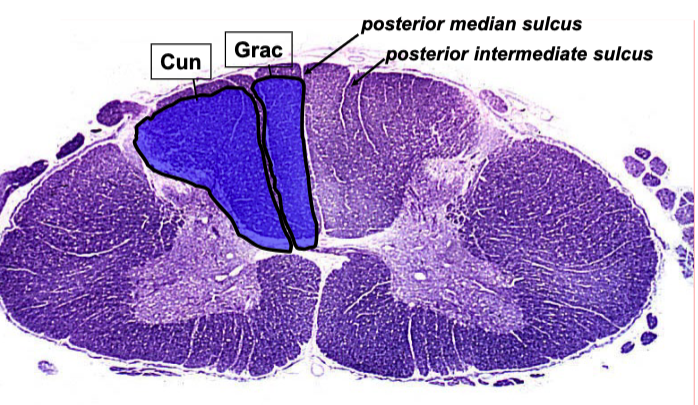
what separates fasciculus cuneatus from gracilis?
Dorsal Columns - Medial Lemniscus Pathway: function
Pressure, vibration, movement and discriminative touch: highly localized
Dorsal Columns - Medial Lemniscus Pathway: RECEPTORS & AFFERENTS
Specialized skin mechanoreceptors
Highly myelinated sensory afferent fibers
Dorsal Columns - Medial Lemniscus Pathway: FIRST ORDER SENSORY NEURON (located where?)
Located at dorsal root ganglia (DRG)
Afferent fibers enter the spinal cord.
Ascend uncrossed in the dorsal columns
- Fascilus gracilis: (Lower limbs T6 and below)
- Fasciculus cuneatus: (Upper limbs T5 and above)
Dorsal Columns - Medial Lemniscus Pathway: SECOND ORDER SENSORY NEURON (located where?)
Located at nucleus Gracilis and nucleus Cuneatus in the caudal medulla
Dorsal Columns - Medial Lemniscus Pathway: DECUSSATION (where do the fibers cross? what does it form?
Fibers cross the midline at the medulla and form the medial leminiscus
Dorsal Columns - Medial Lemniscus Pathway: THIRD ORDER SENSORY NEURON (where is nucleus located? where do fibers project up to?)
Ventral Nucleus in the thalamus, projects to Primary sensory cortex
Dorsal Columns - Medial Lemniscus Pathway: FINAL DESTINATION
Postcentral gyrus (primary sensory cortex), parietal lobe
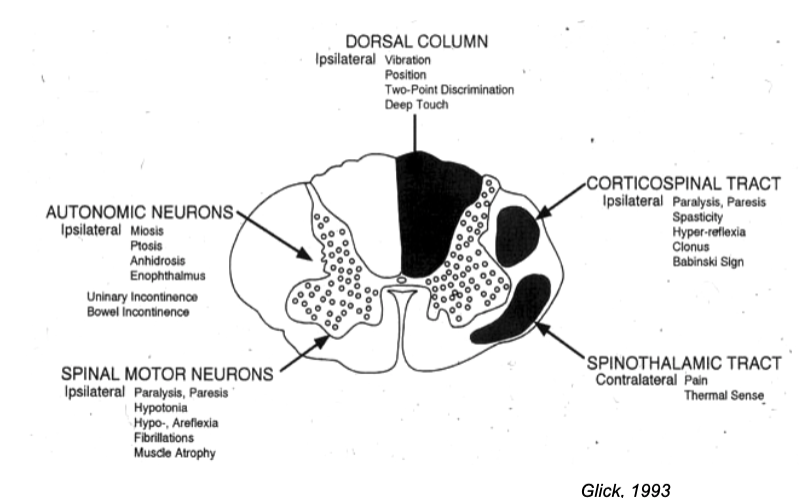
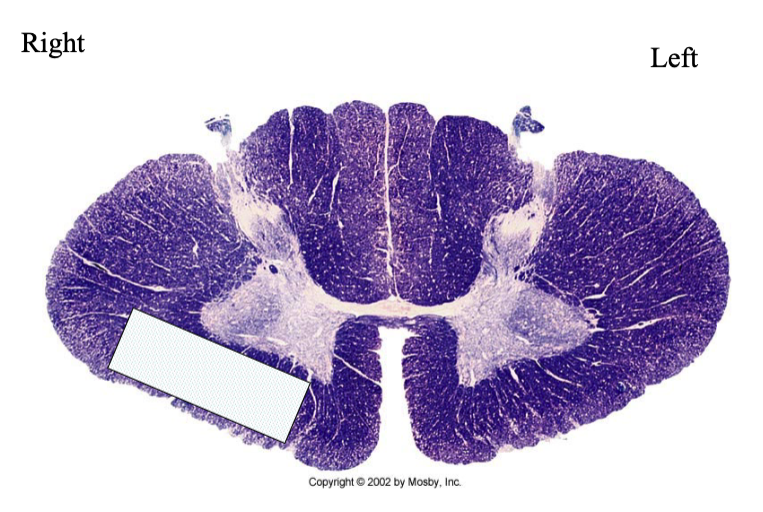
what tracts/pathways are located where?
spinohalamic pathway: sensory modalaties
-Localization of pain and temperature
-Crude touch
spinothalamic pathway:
location of 1st order neuron? 2nd? 3rd?
1 st order neuron in DRG
2 nd order neuron in dorsal horn
3 rd order neuron in thalamus (VPL)
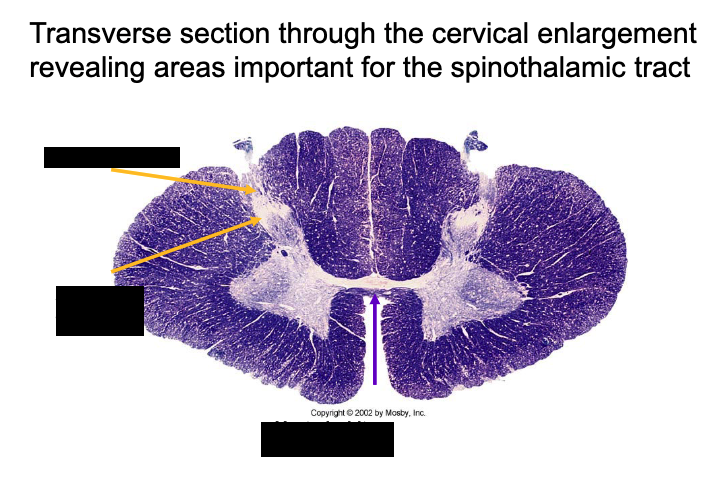
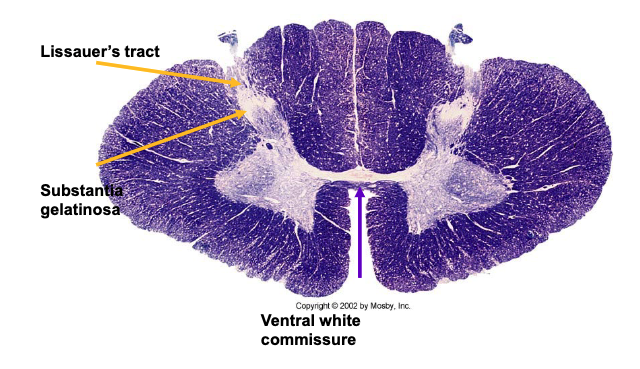
what type of lesion would knock out the ventral white commisure needed for spinothalamic pathway to cross over?
central cord lesion (affects both sides)
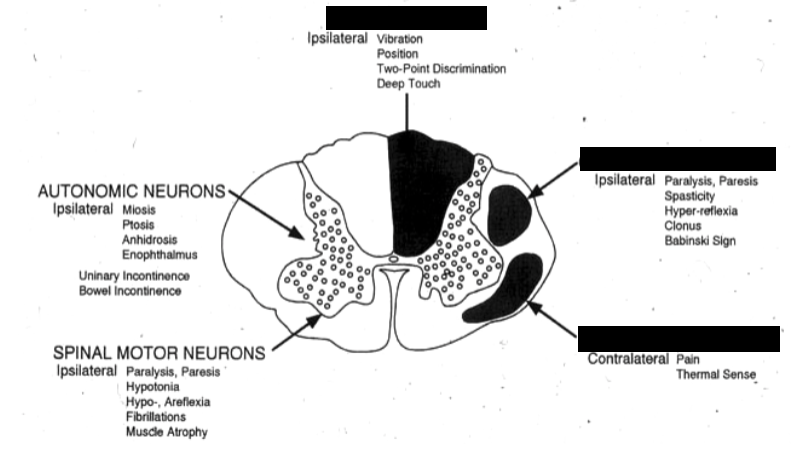
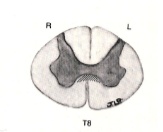
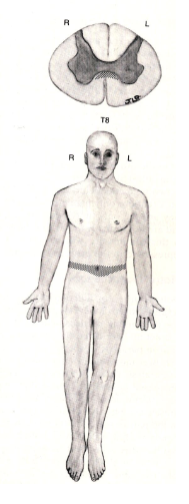
Lesion Diagram: What would you expect to see on examination of this individual
loss of pain and temperature on LEFT side of body (spinothalamic pathway)
which pathway would result in ipsilateral deficit vs contralateral?
dorsolateral pathway = ipsilateral deficit
spinothalamic = contralateral
which pathway has heavily myelinated axons? which one has poorly myelinated axons?
dorsal solumn = heavily myelinated
spinothalamic = poorly myelinated or unmyelinated
t/f; Long Tract Lesions cause deficits at the level of the lesion and above.
FALSE
at the level of the lesion and below
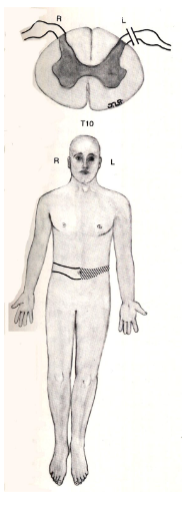
a lesion here would result in what clinical presentation?
(dorsal column)
deficit in position sense, vibration sense, discraminatory touch on the same side of body at the level of lesion and below
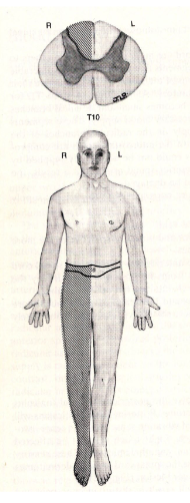
a lesion here would result in what clinical presentation?
(spinothalamic)
deficit in pain/temperature on opposite side of body at the level of lesion and below
what is suspended sensory loss?
caused by lesions that do not involve the long tracts and therefore they reveal a band-like distribution of deficit
a lesion here would result in what clinical presentation?
information from DRG can’t enter the cord
all sensory information from left side blocked
suspended sensory loss of both dorsal column and spinothalamic pathway
a lesion here would result in what clinical presentation?
lesion in ventral white commissure
can’t get spinothalamic information in and across from either side
bilateral sensory loss
What is lesioned here? What findings would you expect in this individual?
(ventral white commissure)
bilateral loss of pain and temperature at the level of the lesion only
describe the spinothalamic tract (anterolateral system)
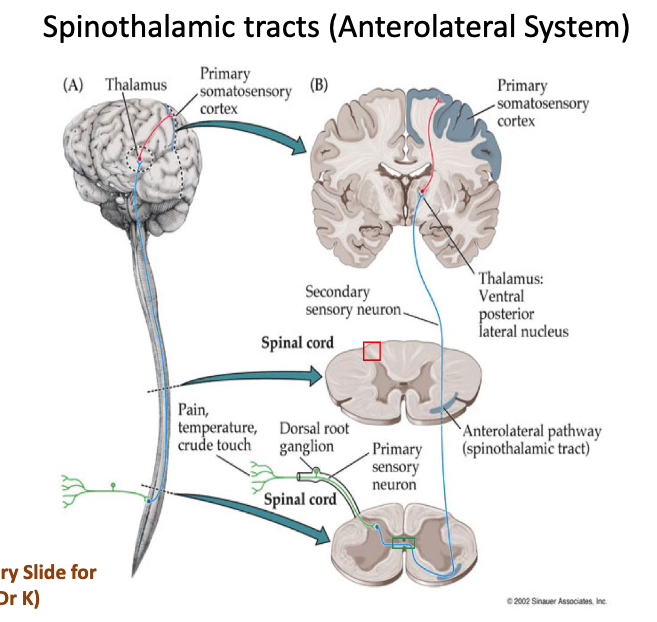
spinothalamic tract (anterolateral system): FUNCTION
Pain and thermal sense – Lateral spinothalamic
Crude touch – anterior spinothalamic
spinothalamic tract (anterolateral system): RECEPTORS & AFFERENTS
Free nerve endings in skin regions or thinly myelinated sensory afferents
spinothalamic tract (anterolateral system): FIRST ORDER SENSORY NEURON
Located at dorsal root ganglia (DRG)
Afferent fibers enter the spinal cord and
Project to lamina II-V (Substantia Gelatinosa, n. Proprius
spinothalamic tract (anterolateral system): SECOND ORDER SENSORY NEURON
Located in lamina II-V
spinothalamic tract (anterolateral system): DECUSSATION
Fibers cross the midline usually 1-2 spinal segments above
entry and ascend in the anterior (crude touch) or lateral (pain/temp) spinothalamic fasciculus.
Terminates in the thalamus
spinothalamic tract (anterolateral system): THIRD ORDER SENSORY NEURON
It is located in the ventral nucleus in the thalamus, and projects to the primary sensory cortex
spinothalamic tract (anterolateral system): FINAL DESTINATION
Postcentral gyrus (primary sensory cortex), parietal lobe
what are some other ascending pathways that head to the cerebellum?
Dorsal (posterior) spinocerebellar pathway.
Ventral spinocerebellar pathway
Cuneocerebellar Pathway
(these all end ipsilaterally in the cerebellum)
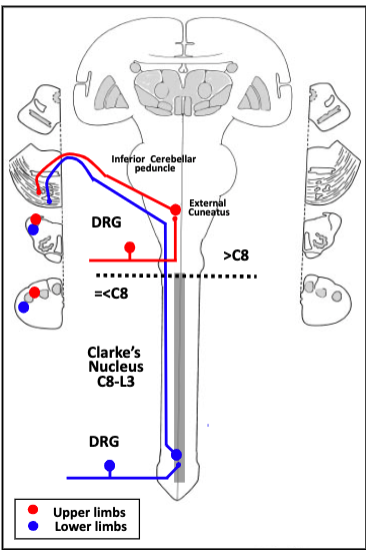
Dorsal Spinocerebellar/Cuneocerebellar (DSC): FUNCTION
Conveys muscle sense information which is used by the cerebellum to coordinate movement and posture. It collects information about individual muscles
Dorsal Spinocerebellar/Cuneocerebellar (DSC): RECEPTORS & AFFERENTS
Muscle spindles and golgi tendon organs
Thick and highly myelinated afferents
Dorsal Spinocerebellar/Cuneocerebellar (DSC): FIRST ORDER SENSORY NEURON
Located at the dorsal root ganglia (DRG), afferent fibers enter the spinal cord and stay in the same side
Dorsal Spinocerebellar/Cuneocerebellar (DSC): SECOND ORDER SENSORY NEURON
Afferent fibers project to the ipsilateral
C8: Clarke’s Nucleus (Nucleus Dorsalis) in Lamina VII
C8: External Cuneatus, in the medulla, this tract is called Cuneocerebellar
Output fibers from 2nd order sensory neurons project to the cerebellum via lateral funiculus
Dorsal Spinocerebellar/Cuneocerebellar (DSC): DECUSSATION
Fibers do not cross the midline and stay always in the same side
Dorsal Spinocerebellar/Cuneocerebellar (DSC): FINAL DESTINATION
Cerebellum
walk through the dorsal spinocerebellar/cuneocerebellar (DSC) pathway
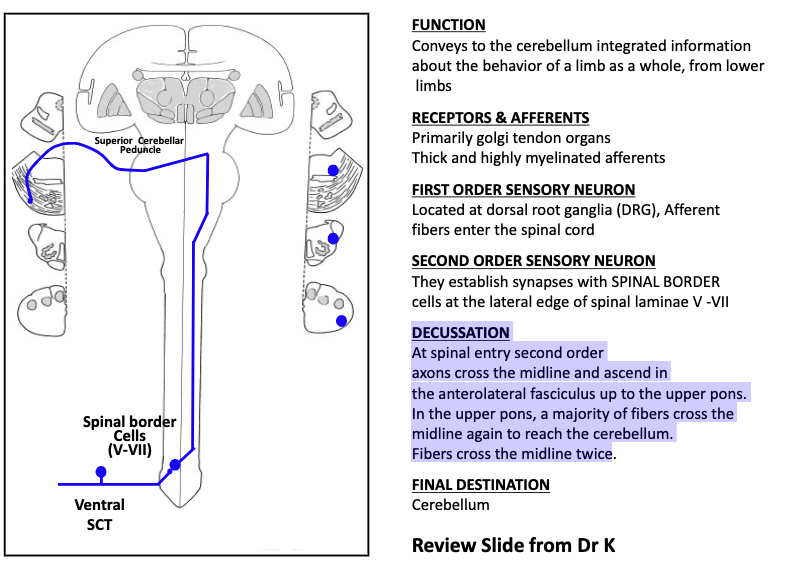
Anterior Spinocerebellar Tract (VSC): function
Conveys to the cerebellum integrated information about the behavior of a limb as a whole, from lower limbs
Anterior Spinocerebellar Tract (VSC): receptors & afferents
Primarily golgi tendon organs
Thick and highly myelinated afferents
Anterior Spinocerebellar Tract (VSC): FIRST ORDER SENSORY NEURON
Located at dorsal root ganglia (DRG)
Afferent fibers enter the spinal cord
Anterior Spinocerebellar Tract (VSC): SECOND ORDER SENSORY NEURON
They establish synapses with SPINAL BORDER cells at the lateral edge of spinal laminae V -VII
Anterior Spinocerebellar Tract (VSC): DECUSSATION
At spinal entry second order axons cross the midline and ascend in the anterolateral fasciculus up to the upper pons.
In the upper pons, a majority of fibers cross the midline again to reach the cerebellum.
Fibers cross the midline twice
Anterior Spinocerebellar Tract (VSC): final destination
cerebellum
walk through the anterior spinocerebellat tract (VSC)
Spinocerebellar Pathways: Dorsal and Ventral Spinocerebellar tracts + Cuneocerebellar tract convey conscious/unconscious muscle sensory information
unconscious
which pathways are involved?

what is anterior cord syndrome?
Rare, after occlusion of the ant. spinal artery
Symptoms:
MOTOR: Bilateral paralysis or weakness
FINE TOUCH: Normal
PAIN/TEMP: Bilateral loss

a lesion here would cause…?
anterior cord syndrome
what is posterior cord syndrome?
Rare, after occlusion of the post. spinal artery
Symptoms:
MOTOR: Normal
FINE TOUCH, VIBRATION: Bilateral loss
PAIN/TEMP: Normal
a lesion here would cause…?
posterior cord syndrome
what is central cord syndrome?
damage to the central area of the spinal cord
It first damages crossing fibers
Symptoms:
MOTOR: Progressive bilateral paralysis by direct damage on motor neurons
FINE TOUCH: Normal
PAIN/TEMP: Immediate bilateral loss
a lesion here would cause…?
central cord syndrome
what is Brown-Séquard Syndrome?
Also called lateral spinal hemisection
Symptoms:
MOTOR: Ipsilesional paralysis (same side lesion)
FINE TOUCH: Ipsilesional loss
PAIN/TEMP: Contralesional loss
a lesion here would cause…?
Brown-Séquard Syndrome
what are some types of incomplete lesions?
central cord syndrome
posterior cord syndrome
anterior cord syndrome
Brown-Séquard Syndrome