anticoag, anemia, sickle cell
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
MOA of Heparins
bind to AT= increase AT activity= inactivates IIa (prothrombin) + other proteases like Xa
UFH vs. LMWH
both bind to AT, but LMWHs inhibit Xa more= more predictive response
Factor Xa Inhibitors
apixaban
rivaroxaban
edoxaban
fondaparinux
Direct Thrombin Inhibitors:
dabigatran
argatroban
bivalirubin
Situations warfarin > DOAC
stroke prevention- mitral stenosis or mechanical heart valve
VTE tx- triple-positive antiphospholipid syndrome or mechanical heart valve
MORAL OF THE STORY—> MECH HEART VALVE= WARFARIN
heparin calculations use what weight
TBW
UFH dosing:
VTE pro
VTE tx
ACS/STEMI tx
VTE pro: 5,000 units SQ q8-12h
VTE tx: 80 units/kg IV bolus, 18 units/kg/hr inf
ACS/STEMI tx: 60 units/kg IV bolus, 12 units/kg/hr inf
LMWH dosing:
VTE pro
VTE tx + UA/NSTEMI tx
STEMI <75 tx
STEMI ≥75 tx
VTE pro: 40 units SQ daily, 30 units SQ q12h
CrCl <30: 30 units SQ daily
VTE tx + UA/NSTEMI tx: 1 mg/kg SQ q12h
VTE inpatient only: 1.5 mg/kg SQ daily
CrCl <30: 1mg/kg SQ daily
STEMI <75 tx: 30mg IV bolus, 1 mg/kg SQ q12h
CrCl <30: 30mg IV bolus, 1 mg/kg SQ dose, then 1 mg/kg SQ daily
STEMI ≥75 tx: no bolus, 0.75 mg/kg q12h
CrCl <30: 1 mg/kg SQ daily
LMWH dosing tips:
CrCl <30—> always only daily dosing
when in doubt—> 1mg/kg
4T
Thrombocytopenia: drop in platelets 50%
Timing: 5-10 days after hep
Thrombosis: clot?
oTher?—> can it be anything else?
4T management:
stop what?
warfarin?
restart?
which anticoags?
preference in cardiac surgery/PCI?
stop ALL HEPARINS ASAP
Warfarin
reverse w/ vit K
only restart when platelets >150
argatroban for tx asap
bivalirudin if cardiac surgery/PCI
eliquis nonvalvular AF dosing
5mg PO BID
2.5mg PO BID if—> ≥80 YO, SCr >1.5, Wt ≤60kg
eliquis DVT/PE tx dosing
10mg PO BID x 7 days, 5mg PO BID
eliquis DVT prophylaxis dosing after hip/knee replacement
2.5mg PO BID x 12 days for knee, 35 days for hip
rivaroxaban + food
doses ≥15
Xarelto nonvalvular AF dosing
CrCl >50: 20mg daily w/ evening meals
CrCl ≤50: 15mg daily w/ evening meals
Xarelto DVT/PE tx dosing
15mg PO BID x 21 days, then 20mg daily w/ food
CrCl <15: do not use
Xarelto DVT prophylaxis dosing after hip/knee replacement
10mg PO daily x 12 days for knee, 35 days for hip
CrCl <15: do not use
xarelto and funky missed dose
if on 15mg PO BID and miss dose—> take both asap do not skip
Special BBW on edoxaban
if CrCl >95: do not use for nonvalvular AF
Edoxaban nonvalvular AF dosing:
CrCl 51-95: 60mg daily
CrCl: 15-50: 30mg daily
CrCl: <15: not recommended
Edoxaban DVT/PE tx dosing
60mg daily—> must start after 5-10 days of parenteral
same dose reductions as in stroke dosing
BBW on all DOACs
pts. receiving neuraxial anesthesia or spinal puncture—> hematoma and paralysis risk
Fondaparinux CrCl cutoff
<30 is CI
DOACs and CYP interactions
eliquis & xarelto—> avoid w/ strong CYP3A4 and Pgp inducers (inhibitors for xarelto as well)
Pradaxa DVT/PE tx dosing
150mg BID —> must start after 5-10 days of parenteral
CrCl<30: avoid use
converting from warfarin to DOAC:
“READ”—> stop warfarin and convert to DOAC when…
Rivaroxaban: INR<3
Edoxaban: INR<2.5
Apixaban: INR <2
Dabigatran: INR <2
converting from DOAC to warfarin:
stop DOAC, start parenteral anticoagulant and warfarin at next dose (doesn’t apply to edoxaban)
converting from dabigatran to warfarin:
start warfarin 1-3 days before stopping dabigatran (refer to package insert)
MOA of warfarin:
competitively inhibits VKORC1—> inhibits 2,7,9,10
BBW of warfarin
bleeding. duh.
warfarin warnings
tissue necrosis/gangrene, purple toe syndrome

warfarin phamacogenomics
CYP2C9*2 or 3* alleles= increase bleed risk
goal INR
2-3 for most, 2.5-3.5 if mechanical
more potent warfarin isomer
S
Warfarin D/I
PK—> CYP2C9
decrease INR: CYP inducers (phenytoin, carb, phenobarb, rifampin, st. johns wort)
increase INR: CYP inhibitors (fluconazole, metronidazole, bactrim, AMIODARONE, tamoxifen)
PD—> anything that can increase bleed risk or clot risk like NSAIDs, SSRIs, antiplatelets, estrogens
Diet—> 5G’s, alcohol, foods with vit K (leafy green veggies)
Which anticoagulant is C/I in pregnancy?
warfarin —> (think: HD for a reason)
warfarin tab colors: 1,2, 2.5, 3, 4, 5, 6, 7.5, 10
pink, purple, green, tan, blue, peach, teal, yellow, white
Protamine dosing for UFH and LMWH reversal:
UFH: 1mg protamine will reverse 100 units, reverse amount given in last 2-2.5 hours, max 50mg
LMWH: 1mg protamine/1mg enoxaparin within last 8 hours
BBW of protamine and vit K
hypersensitivity/ anaphylaxis (warfarin IV only)
administer what with vit K?
Four Factor Prothrombin Complex Concentrate (Kcentra, Balfaxar) —> has 2,7,9,10, C,S
oral vs. IV Vit K
oral—> when no sig bleeding
IV—> major bleeding
don’t do IM or SC
Warfarin Reversal per INR:
<4.5 w/ no major bleeding: reduce/skip dose, monitor INR
4.5-10 w/ no major bleeding: hold 1-2 doses, monitor INR (maybe oral vit K if having surgery)
>10 w/ no major bleeding: hold warfarin, oral vit K, monitor INR
major bleeding: hold warfarin, IV vit K slowly + 4-factor PCC
perioperative warfarin management:
stop ~5 days before surgery
if mechanical heart valve or high VTE risk bridge w/ heparin
d/c LMWH 24 hrs before/UFH 4-6 hrs before surgery
do not bridge for low risk
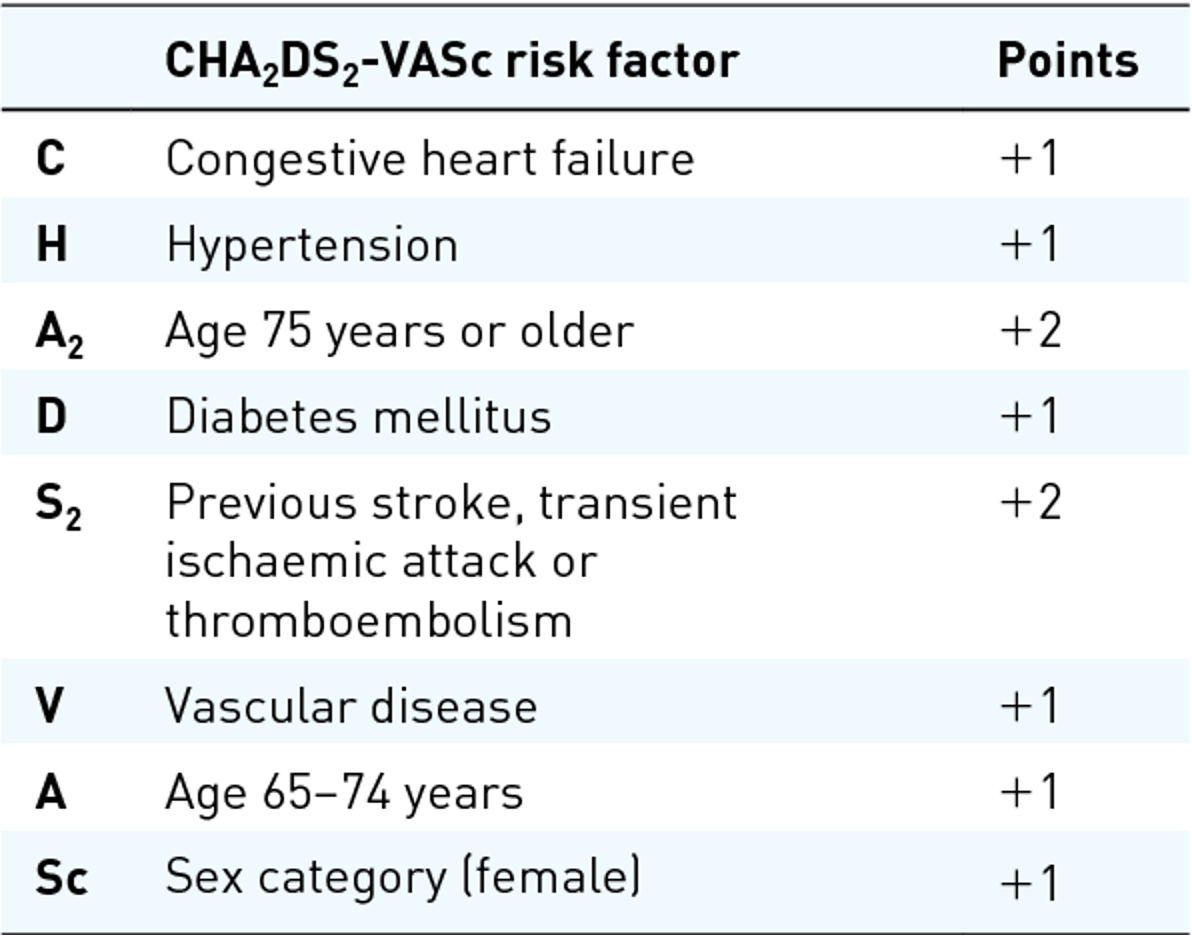
CHA-DS-VASc Scoring System:
≥2 (males) and ≥3 (females)= anticoag rec
anticoagulation for pts. with AF undergoing cardioversion
AF> 48 hrs or unknown duration= 3w before, 4w after
AF ≤ 48 hrs= 4w after
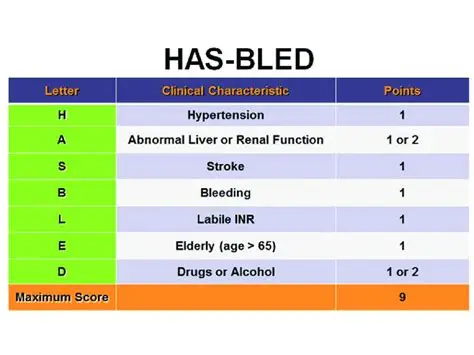
HAS-BLED Scoring System:
Anticoagulation in pregnancy:
LMWH PREFERRED
Warfarin- C/I
DOACs- not studied
VTE provoked and unprovoked tx duration:
unprovoked: 3 months+
provoked: 3 months
identifying the cause of anemia via MCV:
microcytic (<80): iron deficiency
normocytic: acute blood loss, hemolysis, CKD, malignancy, bone marrow failure
macrocytic (>100): vit b12/ folate deficiency
causes of iron deficiency anemia:
diet
blood loss (acute, chronic— heavy periods, PUD)
decreased absorption (high gastric pH—- PPI use or GI disorders)
THINK: IRON LIKES ACIDITY
increased requirements (pregnant, lactating, infants)
iron deficiency anemia tx—- oral vs. IV
oral iron—> GO TO
IV iron- due to ADRs, cost, etc.—> reserved typically for CKD or cancer
oral iron counseling:
when to take?
D/I?
BBW
ADRs
Admin: TAKE ON EMPTY stomach (unless GI upset)
take w/ vit C—> increase absorption
D/I: quinolones, tetracycline, bisphosphonates, levothyroxine, INSTIs
BBW: overdose in kids
ADRs: constipation, dark tarry stools
iron overdose antidote
deferoxamine (Desferal)
IV iron names:
Iron sucrose (Venofer)
Ferumoxytol (Feraheme)
Iron dextran complex (INFeD)
Main BBW/ warnings with IV iron
Hypersensitivity rxns—- on ALL IV iron products
BBW for Feraheme and INFeD—- must give test dose for INFeD
ESA initiated when Hgb < ___ g/dL
10
ESA d/c’ed when Hgb > ___ g/dL
11
BBW on ESAs
↑ risk of death, MI, stroke, VTE, thrombosis AKA INCREASES CLOT RISK
Epoetin brand
Epogen, Procrit
Darbepoetin brand
Aranesp
Epoetin vs. Darbepoetin
darb has 3x longer half life… allows for once weekly dosing vs. trice weekly dosing
what is hemolytic anemia?
when RBCs are destroyed prematurely (10-20 days instead of 120)
2 types of drug-induced hemolytic anemia
immune-mediated: + Coombs test
GP6D deficiency: - Coombs test
Key drugs that can cause immune-mediated hemolytic anemia:
penicillins, cephalosporins
isoniazid
methyldopa, levodopa
rifampin
quinidine, quinine
sulfonamides
Key drugs that can cause G6PD Deficiency hemolytic anemia:
Dapsone
Methylene blue
nitrofurantoin
Pegloticase, Resburicase
Primaquine, Quinidine, Quinine
Sulfonamides
ESA storage considerations
fridge
do NOT SHAKE