Auditory Brainstem Responses (ABRs/BAEPs/BAERs)
1/118
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
119 Terms
what does BAEP stand for
brainstem auditory evoked potential
what does BAER stand for
brainstem auditory evoked response
what are auditory brainstem responses
auditory electrical potentials generated by the auditory nerve and brainstem following stimulation to the hearing pathway
what do we assess when monitoring ABRs
integrity of the auditory cranial nerve (CN 8) & brainstem b/c these structures are at risk
what type of stimulation is used for ABRs
broad-band click
for ABRs, we stimulate at the __ & record __
distal location; proximally
sound enters the __
external acoustic meatus
sound waves cause a vibration of the __
tympanic membrane
the tympanic membrane is connected to the __
ossicles
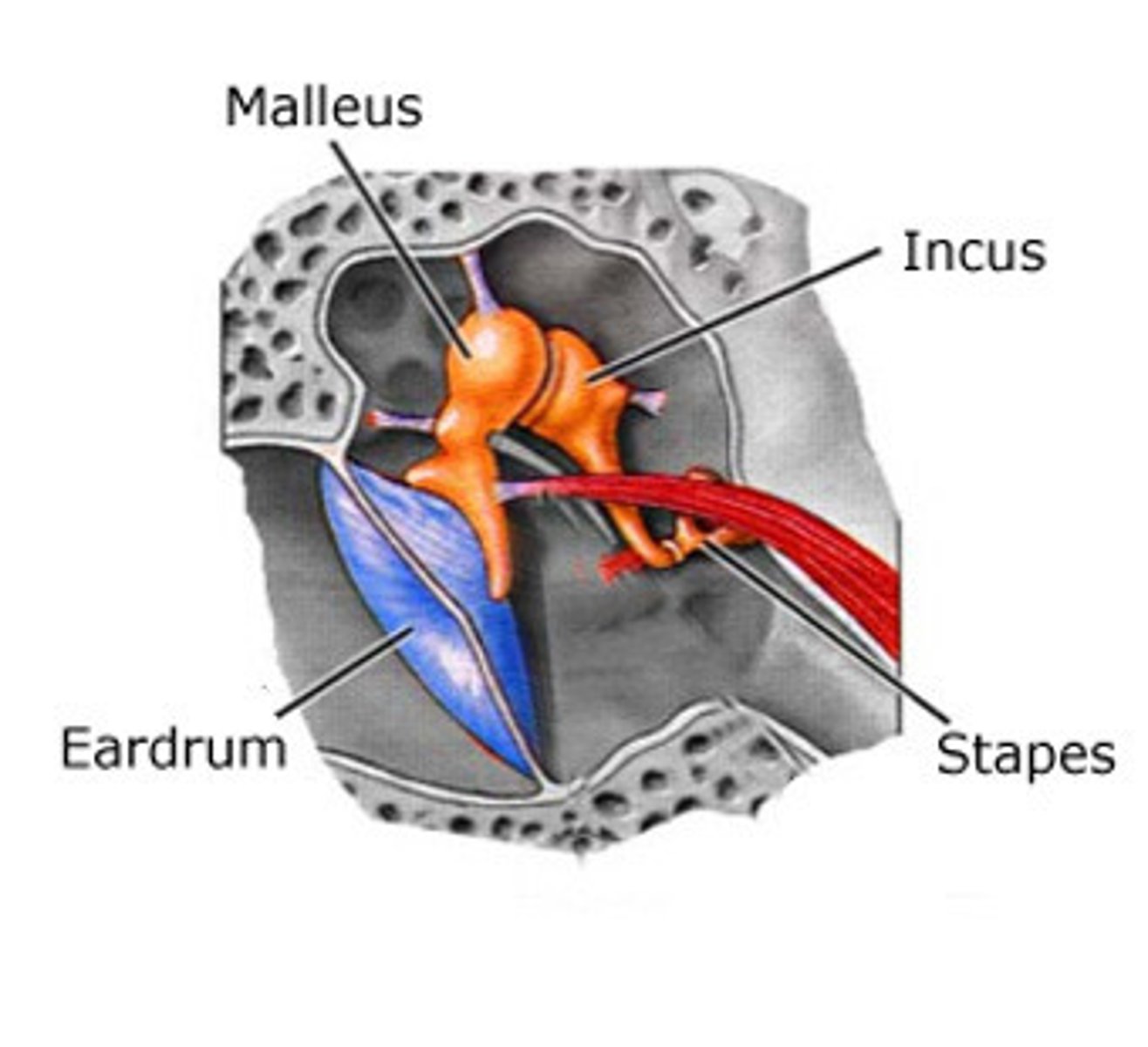
the ossicles connect to the __ via __
cochlea; oval window
___ movement leads to generation of the electrical potential that is relayed to the CN VIII
hair cell
where does the cranial nerve carry potential from? to?
from = cochlea
to = brainstem
ossicles include the __
malleus, incus, stapes
fluid movement at the oval window leads to __
depolarization
hearing pathway
sound --> tympanic membrane --> ossicles --> oval window --> cochlea --> distal auditory nerve --> cochlear nucleus --> superior olivary complex (SOC) --> lateral lemniscus --> inferior colliculus (IC) --> medial geniculate nucleus --> primary auditory cortex
cochlear nucleus
initial site that all auditory signals from CN VIII are obtained and processing begins
superior olivary complex (SOC)
contributed to the processing of sound timing & intensity --> projects UPWARDS to the pons
has CONTRALATERAL & IPSILATERAL side
lateral lemniscus
projection to higher brainstem structures & continued signal processing
on CONTRALTERAL side
inferior colliculus (IC)
receives all LOWER brainstem auditory input for processing and integration; contributes to spatial localization of sound
CONTRALATERAL
medial geniculate nucleus
processing of auditory input from BOTH ears
final processing and projection of MULTIPLE sound characteristics of the cortex
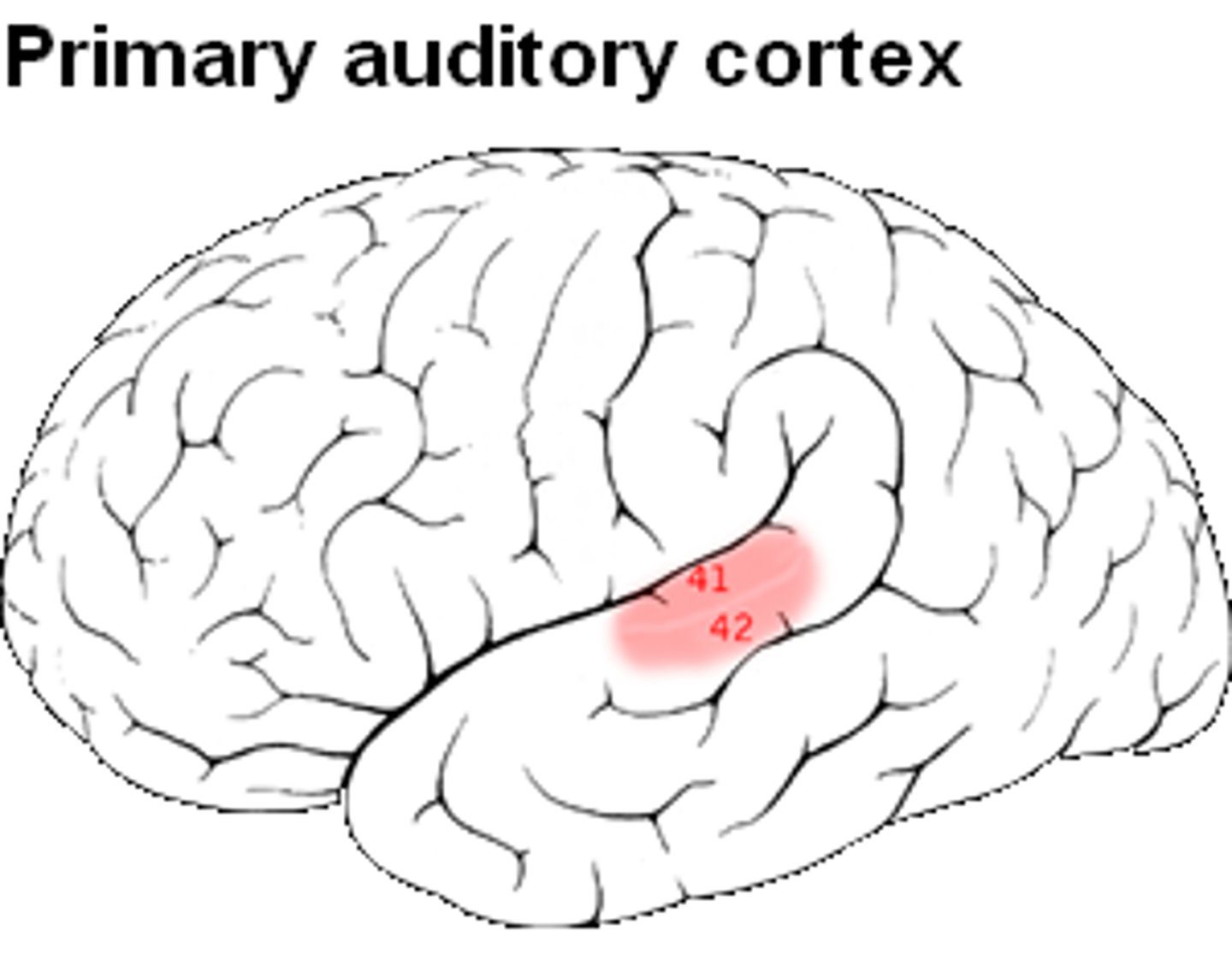
primary auditory cortex is part of the __ lobe
temporal
2 components of auditory nerve
1) distal = close to the cochlea
2) proximal = close to the brainstem
ABRs begin at the __
distal auditory nerve (AFTER the cochlea)
components of ABR come __ the cochlea
after
AFTER the sound goes through the ear pathway, it creates an __ that travels down to the __ to the __ & then to the __
action potential; cochlear nerve; brainstem; cortex
obligate ABR waveforms
wave I (WI)
wave II (WII)
wave III (WIII)
wave IV (WIV)
wave V (WV)
wave I is the?
distal auditory nerve
wave II is the?
cochlear nucleus (medulla-pons junction)
wave III is the?
superior olivary complex (medullla-pons junction)
IPSILATERAL auditory potentials are noted at BOTH the IPSILATERAL & CONTRALATERAL SOC
wave IV is the?
lateral lemniscus (contralateral)
wave V is the?
inferior colliculus (contralateral midbrain)
which wave is the MOST PROMINENT/BIGGEST
wave V
which waves are the most reliable/consistent
WI, WIII, WV
alert criteria is based on which waves?
I, III, V
which waves do we monitor
I, III, V
which waves do we not typically label even if they are presenting
II & IV
are there STANDARD latencies for ABRs
no just typical latencies
are ABR latencies shorter/longer than SSEPs?
shorter
interpeak latency for WI-WIII
~2 msec
interpeak latency for WIII-V
~2 msec
interpeak latency for WI-V
~4 msec
a tube inserts adds ___ msec to increase wave latency
0.9-1 msec
ABR amplitudes are typically __
1 uV or LESS
typical latencies:
WI
WII
WIII
WIV
WV
1.5
2.5
3.5
4.5
5.5
latencies WITHOUT tube compensation:
WI
WII
WIII
WIV
WV
2.5
3.5
4.5
5.5
6.5
WI is nearfield/farfield?
nearfield (distal auditory nerve potential)
WII-WV is nearfield/farfield?
farfield
what is the electrode that obtains a response at WI
Ai/Ac (Mi/Mc)
what is the electrode that obtains a response at WII-WV
Cz (CPz)
MPower Health ABR montages:
ipsilateral trace
contralateral trace
referential trace
non-cephalic (optional)
Ai/Mi-Cz (CPz)
Ac/Mc-Cz (CPz)
Ai-Ac (WI)
Erbs-Cz or Cs3-Cz (WII-WIV)
ACNS ABR montages (9C):
ipsilateral trace
contralateral trace
Cz-Ai/Mi
Cz-Ac/Mc
ACNS ABR montages (11C):
ipsilateral trace
contralateral trace
referential (optional)
Cz-Ai/Mi
Cz-Ac/Mc
Mi-Mc/Ai-Ac (optional)
what is the ground placed per MPower
can be placed with SSEP headpack on the shoulder/trap
what is the ground placed per ACNS
Fz
common types of surgery that may need ABR monitoring
microvascular decompression (MVD), acoustic neuroma, suboccipital craniotomy for tumor resection
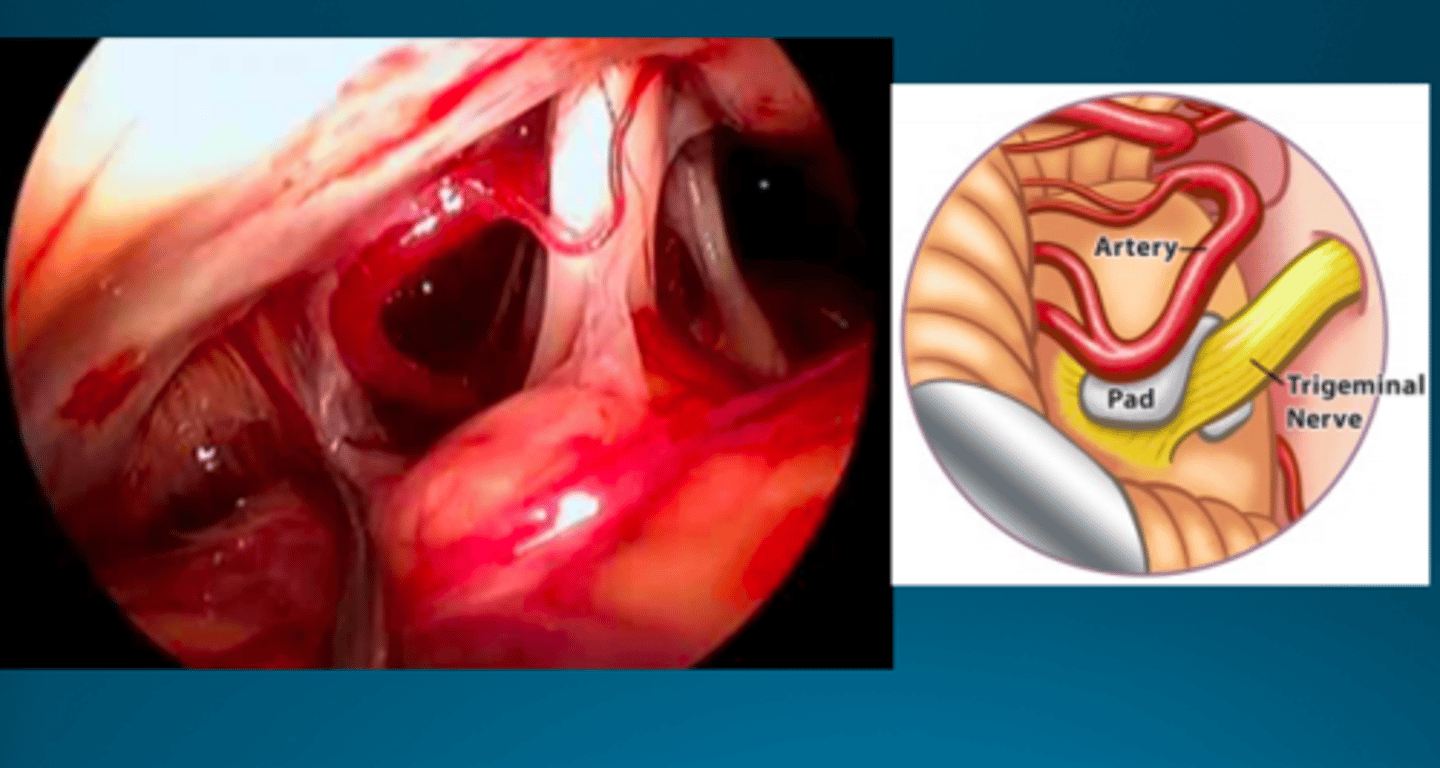
microvascular decompression (MVD)
suboccipital craniotomy approach performed to remove abnormal compression of a cranial nerve by an artery near the brainstem --> retraction on cerebellum & brainstem
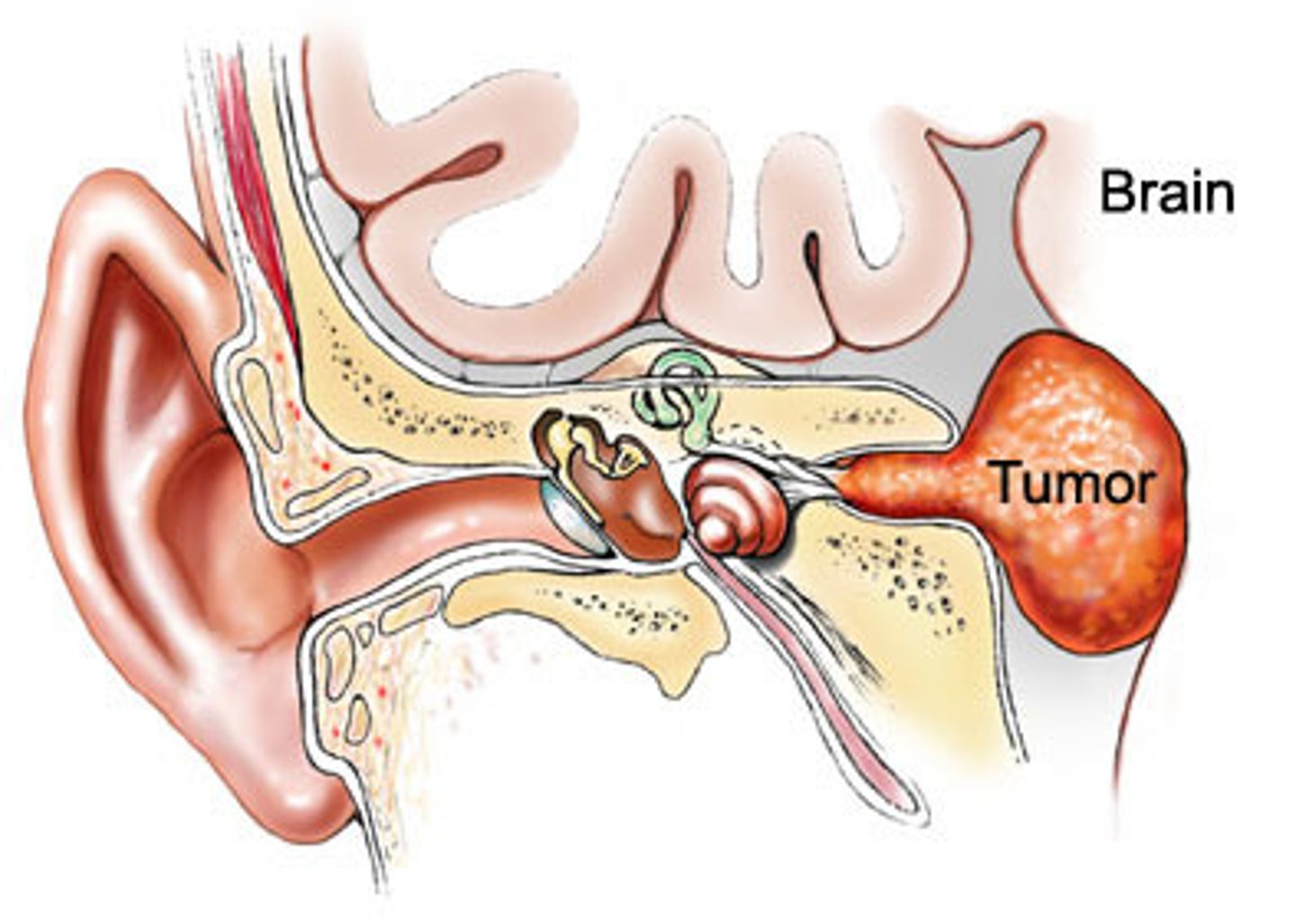
acoustic neuroma
tumor on the acoustic nerve (CN 8)
suboccipital craniotomy for tumor resection places retraction on the __
cerebellum
If the surgical approach places the auditory nerve at risk, we monitor ABRs to __
detect nerve stretch or nerve irritation --> leads to INCREASED latencies
If the surgical approach places the brainstem at risk or involves heavy retraction on the
brainstem/cerebellum, ABRs are used to __
assess brainstem integrity
CN __ is the shortest nerve
VIII
ABR kit includes?
ABR transducers
connection cable
ear inserts
tube
ABR transducer function
generates clicks using air pressure (stimulus generator)
what does the connection cable connect
ABR transducers to the base unit
what does the tube connect
transducer to the ear insert
the stimulation generated by the transducers are a series of broadband clicks that are delivered one/two ear/s at a time?
one
does the ipsilateral or contralateral ear ALWAYS get the white noise masking?
contralateral
white noise masking
prevents a crossover response from the ipsilateral ear being stimulated
what happens to the contralateral side if there is NO white noise masking
bone conduction crossover
do we run ABRs on interleaving stimulation
NO --> only ONE ear at a time
3 types of polarity
rarefaction
condensation
alternating
rarefaction polarity
produces NEGATIVE pressure at the tympanic membrane
OUTWARD pull like a suction
gives the BEST WI
condensation polarity
produces POSITIVE pressure at the tympanic membrane
gives the BEST WV
alternating polarity
alternates between rarefaction & condensation clicks
produces potentials
great for REDUCING stim artifact
stimulate one/two ears, record from one/both sides?
one; both
when we stimulate ABRs from one side, we record both __ & __ montages
ipsilateral & contralateral
in the IPSILATERAL montage, we expect to what waves?
I, III, V
in the CONTRALATERAL montage, we expect to what waves?
III & V
also gives a better separation of WIV & V --> helps identify WV
do we expect to see WI on the contralateral montage?
NO b/c the active electrode gives us a WI and Ai
interpeak latency
time between two waves
which wave will we see if there is NO white noise masking/stimulating too HIGH
I
ABR stimulation parameters
intensity = 80-100 dB SPL
contralateral masking = ½ of stim intensity
pulse width = 100 us
rep rate = 11.1-33.3 Hz
ABR recording parameters
LFF = 30-100 Hz
HFF = 100-150 Hz
amp gain = 10 uV/Div
trials = 500-3000
analysis time = 1-2 ms/div
smoothing filters = ABR1 & ABR2
dB SPL means?
decibels sound pressure level
patient set-up for ABRs
1) check ABR transducers BEFORE placing them to make sure they are working --> plug into base unit & test ONE at a time
2) check patient's ear to make sure there is NOT access cerumen
3) compress ear insert & firmly place into ear canal
4) seal around insert with bone wax
5) bend tube & secure it to the patient's skin with a tegaderm --> can use multiple layers
6) clip transducer to patient to prevent it from hanging
7) acquire baselines
1st & 2nd layer of protection around the ear for ABR set up to protect against fluid
1st = multiple tegarderm
2nd = bone wax
purpose of bone wax
helps with holding insert in place and prevents fluid from getting into the ear canal
when should ABRs be paused
when the surgeon is using bovie, bipolar, drill, burr b/c it will cause reject
effect of propofol & halogenated inhalational agents on ABR waveforms
MINIMAL latency prolongations & MINOR decreases in amp
effects of barbiturates on ABR waveforms
MINIMAL increase in latency without ANY effect on amp
does nitrous oxide have an effect on ABR waveforms
NO
effects of hypothermia on ABR waveforms
increase in WI latency; increase in interpeak latencies
significant cooling = COMPLETE LOSS of ABRs
cold irrigation in the field may contribute to __ along with __
increase in latency; facial nerve neurotonic EMG discharge
default to preferred/standard anesthetic reigmen if we are running ABRs with SSEPs or another anesthetic-sensitive modality?
preferred
what can cause a change in ABRs
mechanical trauma
thermal trauma
ischemia
mechanical trauma
stretching/cutting CN VIII or direct trauma to the brainstem
thermal trauma
CN 8 being heated up by cautery
ischemia
trauma to auditory (labyrinthine) artery or basilar artery
labyrinthine artery
perfuses cochlea
ABR alert criteria when monitoring to assess brainstem function
wave V latency INCREASE of 1 ms
DECREASE of wave III or V amplitude by 50%
report LOSS of any ABR waveforms