Dysphagia Exam 1
1/52
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
53 Terms
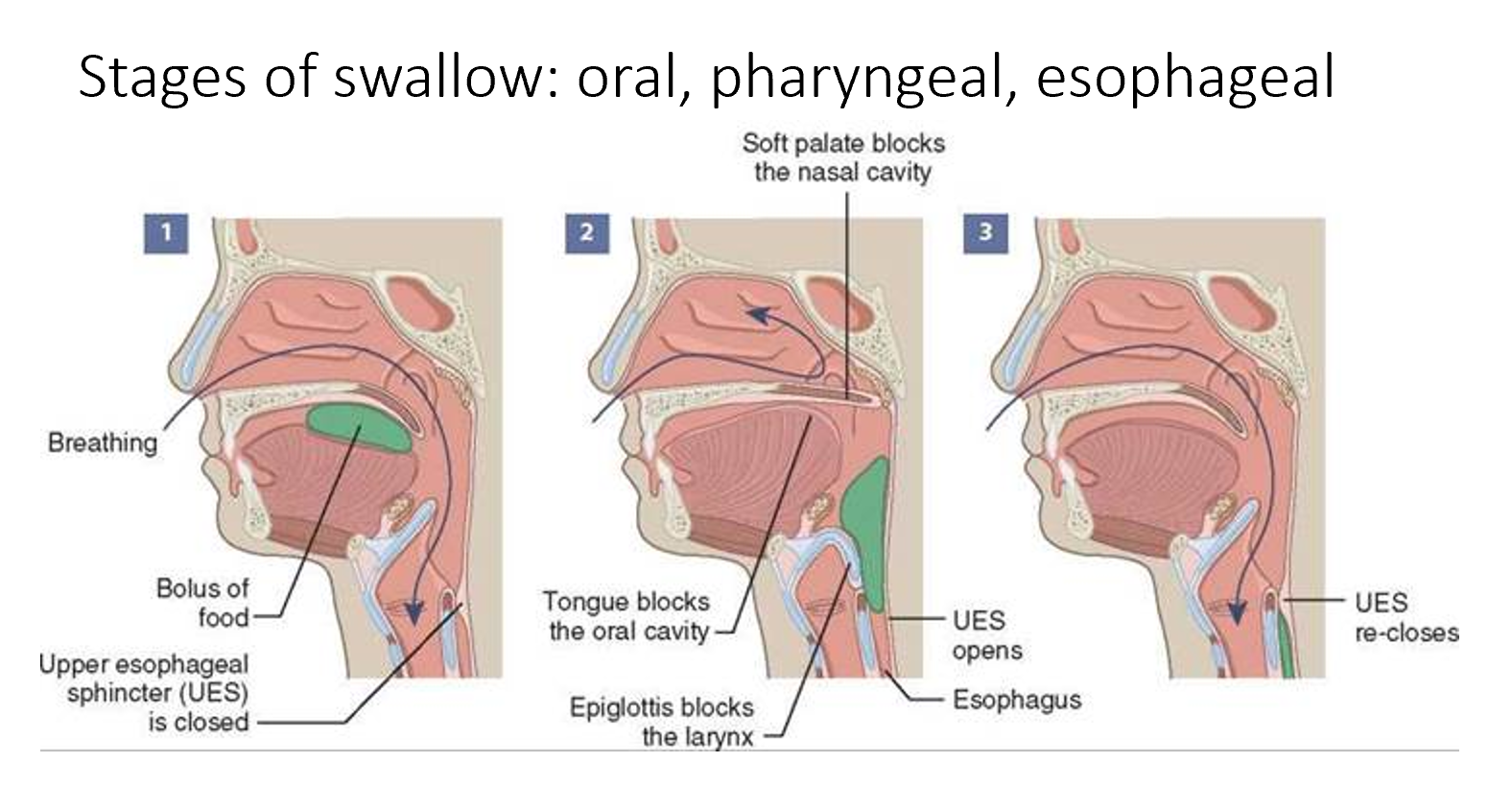
What are the phases of a normal adult swallow?
•1. Oral Preparatory Phase
•2. Oral Transit Phase
•3. Pharyngeal Phase
•4. Esophageal Phase
Who is on the dysphagia team
•SLP
•Otolaryngologist
•Gastroenterologist
•Radiologist
•Neurologist
•Dentist
•Nurse
•Dietician
•Occupational Therapist
•Respiratory Therapist
Is dysphagia a disease?
No, it is a symptom of something else
what are the big three consequences of dysphagia
•Aspiration pneumonia (respiratory compromise)
•Malnutrition
•Dehydration

What are some medical consequences?
aspiration pneumonia, cost, death, dehydration, innutrition
What is the dysphagia goal?
•Avoid aspiration
• Adequate nutrition / hydration
• Least restrictive diet
• Safety & Efficiency
Safety = risk of aspiration
Efficiency = moving the bolus through the pharynx
What is aspiration?
entry of food or liquid into the airway BELOW the true vocal folds; silent aspiration – no outward s/s
Penetration
entry of food or liquid into the larynx at some level, can be down to the cords, but not past the cords
Odynophagia
pain with swallow
Aspiration Pneumonia
Aspiration pneumonia occurs when food or liquid is breathed into the airways or lungs, instead of being swallowed
Types of dysphagia
Neurological (tbi, als, parkinsons, etc)
structural (spinal cord injury, GI, etc)
psychological (could be side effects of medicine)
Phagophobia
fear of swallowing
May be associated with panic disorders, PTSD, social phobia, or OCD
Pre-preparatory stage
smell, salivation, feeding, cognitive awareness of food
Oral preparatory phase
Oral prep stage begins with food in mouth
Bolus is chewed, manipulated and mixed with saliva
Mastication involves a rotary lateral movement of the mandible and
tongue
How does the oral prep phase work in detail?
When the upper and lower teeth have met and crushed the material, the food falls
medially toward the tongue, which moves the material back onto the teeth as the
mandible opens
• The cycle is repeated numerous times before forming a bolus and initiating the oral
phase of swallow
• Tongue mixes the food with saliva
Oral phase
Oral stage begins when tongue begins posterior movement of the
bolus.Bolus is propelled back to the pharynx by the base of the tongue by
pushing against the hard palateLabial seal is maintained to prevent food from spilling from the
mouthBuccal muscles tense to prevent pocketing
orbicularis oris
Lip closure: primary muscle. Good lip closure is
essential. Without it, bolus can leak out. Need for proper pressure.
cohesive bolus
food needs to be moved around, position
between teeth for chewing, mixing with saliva, manipulating into a
cohesive bolus and propelling it back. Bolus cohesion turns into bolus
propulsion.
Temporomandibular Joint (TMJ)
Joint between the maxilla and mandible
Joint contains an intra-articular disk which facilitates movement
between the 2 bones
Floor of mouth (submentals)
• mylohyoid, geniohyoid, anterior belly of digastric
all attach to the body of the mandible anteriorly and the body of the
hyoid posteriorly
Soft palate
moveable fold
Velopharyngeal closure (VP)
Poor velopharyngeal closure is more important for speech, not really
a great concern re: safety of swallowing
• Poor VP closure can result in reflux to nasopharynx, unpleasant but
not life threatening
Tongue propulsion
Once the bolus reaches the back of the tongue and passes into the
pharynx (through the faucial pillars) the swallow becomes reflexive
and is no longer under voluntary control
pharyngeal tongue
extends from the velum to the hyoid bone and vallecula. functions
during the pharyngeal stage
oral tongue
extends from the tip to back, adjacent to the velum, functions during
the oral stage of the swallow.
Is respiration and swallowing related?
Yes, this relation is expressed functionally because respiration is inhibited
by swallowing, and disorders of respiration often affect swallow
safety.
When does respiratory pause occur during swallowing?
Once the bolus reaches the valleculae.
When does breathing resume after swallowing?
As the bolus tail passes the PES, larynx descends, and exhalation resumes before PES closure.
Why is exhalation after swallowing protective?
It clears any material that may enter the airway.
Nasopharynx
Nose to soft palate
Oropharynx
Portion which is visible via the mouth
• Soft palate to vallecula
• Posterior and lateral walls are formed by the superior and middle
pharyngeal constrictors
Hypopharynx
Portion of pharynx inferior to the tip of the epiglottis
• Posterior and lateral walls formed by the middle and inferior pharyngeal
constrictors
Pharyngeal stage
The pharyngeal stage begins when the bolus arrives at the level of the
vallecula and ends when the PES closes.
What happens in the pharyngeal stage?
The superior, middle, and inferior constrictors contract in sequence, narrowing and shortening the pharynx. This creates peristaltic “toothpaste tube” squeezing that pushes the bolus down into the esophagus.
How does the PES/UES open during swallowing?
Normally closed → relaxes via CN X → pulled open by hyolaryngeal elevation (up & forward) → further distended by bolus pressure.
pharyngeal swallow
As the tail of the bolus passes the region of the PES, primary
esophageal peristalsis begins as the PES closes.
• The airway reopens and the hyoid bone returns to its resting position.
• These activities signal the end of the pharyngeal phase of swallow.
UES (AKA PES)
The UES is a muscular ring that separates the pharynx from the esophagus
• It prevents air from entering the gastrointestinal (GI) tract during
respiration
3 muscles of UES
• lower fibers of the inferior pharyngeal constrictor
• the cricopharyngeas =primary muscle
• the upper fibers of the esophageal muscular wall.
Esophageal swallow zones
3 main zones:
the proximal, striated muscle zone;
the body;
and the specialized smooth muscle of the
distal zone.
Bolus movement through these zones is characterized by an orderly,
ringlike progression of contractions until the bolus enters the LES and
the stomach.
Esophageal phase
the esophagus is controlled by the upper esophageal
sphincter (UES). Once the bolus has passed through the UES it is
transported down to the stomach by a series of peristaltic
contractions of the esophageal muscular wall.
thoracic esophagus
top half of the esophagus
the proximal (top) 1/3 of the esophagus is comprised of striated
muscle, the bottom 2/3 is smooth muscle
distal esophagus
bottom half of the esophagus
the proximal (top) 1/3 of the esophagus is comprised of striated
muscle, the bottom 2/3 is smooth muscle
Purpose of the larynx
• Organ of communication “voice box”
• Important regulator of respiration
• Necessary for an effective cough
• Prevents aspiration during swallowing
Viscosity
centipose cP
• How thick something is, ie drinks
• Thin 0-1 cP
• Applesauce 1500 cP
What makes straw drinking different from cup drinking?
Straw drinking requires adequate lip strength and intraoral pressure to draw fluid, airway must remain closed during sequential swallows, and brief airway openings occur between sips. These factors make it important to test with VFSS or FEES, as biomechanics differ from cup drinking.
How does aging affect swallowing?
Older adults (≥75) may show peripheral sensory changes (smell, taste) and decreased muscle strength/contractility in tongue, lips, jaw, velum, and lungs. This leads to slower but normal swallow durations. Reduced lung elasticity and respiratory control can also indirectly impact swallowing. White matter lesions may further increase swallow duration.
Presbyphagia
Normal aging may not cause dysphagia directly but can worsen conditions like neurologic disease. Some swallow functions decompensate with age, and reduced compensatory ability can heighten disease effects. Clinically, it is difficult to separate aging changes from disease-related dysphagia.
presbyphagia may lead to
impaired bolus control and transport, the
slowing of pharyngeal swallow initiation, ineffective pharyngeal
clearance, impaired cricopharyngeal opening, and reduced secondary
esophageal peristalsis, with serious consequences for independence
and quality of life.
How is swallowing controlled neurologically?
Swallowing involves both central and peripheral control. Oral swallowing is voluntary; pharyngeal is reflexive. Peripheral muscles contract sequentially but can adjust to feeding circumstances. Normally, swallowing is automatic, but it can be consciously initiated (e.g., swallowing a pill).
How is the pharyngeal swallow controlled peripherally and by the medulla?
Sensory receptors on the faucial pillars, tonsils, soft palate, tongue base, posterior pharyngeal wall, and epiglottis trigger the pharyngeal swallow. Signals travel mainly via CN IX and X to the medulla. Swallowing integrates voluntary and involuntary control of lips, teeth, jaw, cheeks, and tongue, mediated by multiple cranial nerves (IX and X).
Frailty
Frailty involves loss of physical strength and reduced compensatory ability. Cognitive frailty also includes mild mental changes (e.g., depressive symptoms) short of dementia. Frailty exists on a continuum and may or may not predict dysphagia; specific physical deficits that indicate risk for swallowing issues are currently unknown.
Characteristics that define frailty
• Hand grip weakness
• Slower than normal walking speed
• A decrease in normal physical activity
• Self-reported exhaustion
• Unintentional weight loss
• Subtle changes in cognitive status
Sarcopenia
a reduction of lean skeletal muscle mass with a marked loss of strength and speed of movement.
caused by frailness