Lecture 28: Vestibular Disorders
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
Anatomy of peripheral vestibular system
- Semicircular canals
- Otolith organs
Semicircular canals
- Anterior
- Posterior
- Horizontal
Otolith organs
- Saccule
- Utricle
Benign paroxysmal positional vertigo (BPPV)
- Peripheral vestibular disorder
- Most common disorder resulting in dizziness in older population
- Mechanical disorder caused by otoconia displaced from the macula of the utricle.
Causes of BPPV
- Infection
- Head trauma
- Vestibular weakness
- Advancing age
BPPV symptoms
- Vertigo
- Nausea (w/ or w/o vomiting)
- Nystagmus
BPPV vertigo
- With change in head position such as when turning over in bed, getting into or out of bed
- When bending over/coming up
BPPV nystagmus
- Involuntary, rapid and repetitive movement of the eyes
- Most important symptom
Types of BPPV
- Canalithiasis
- Cupulothiasis
Cupulolithiasis
- Immediate
- Persistent in duration
- Nystagmus = no change in intensity
Canalithiasis
- Latency with (1- 40 seconds)
- Short in duration (< 1 min)
- Nystagmus = fluctuates in intensity
What is a similarity between cupulolithiasis and canalithiasis?
Both have nystagmus
Which canal(s) result in a torsional/rotational nystagmus?
Anterior and posterior SCC
Which canal(s) result in a horizontal nystagmus?
Horizontal SCC
Dix hallpike test procedure
- Head turned 45 deg toward affected ear while in seated
- Patient quickly moved into supine position with head extended 20-30 deg off the table and rotated 45 deg toward the ear
Is Dix hallpike an assessment or intervention?
Assessment
Dix hallpike is assessing which canal?
Anterior and posterior
Posterior canal results in what kind of nystagmus?
Up beating torsional toward side of head rotation
Anterior canal results in what kind of nystagmus?
Down beating torsional to side of head rotation
Posterior SCC canalithiasis is treated by what?
Epley maneuver
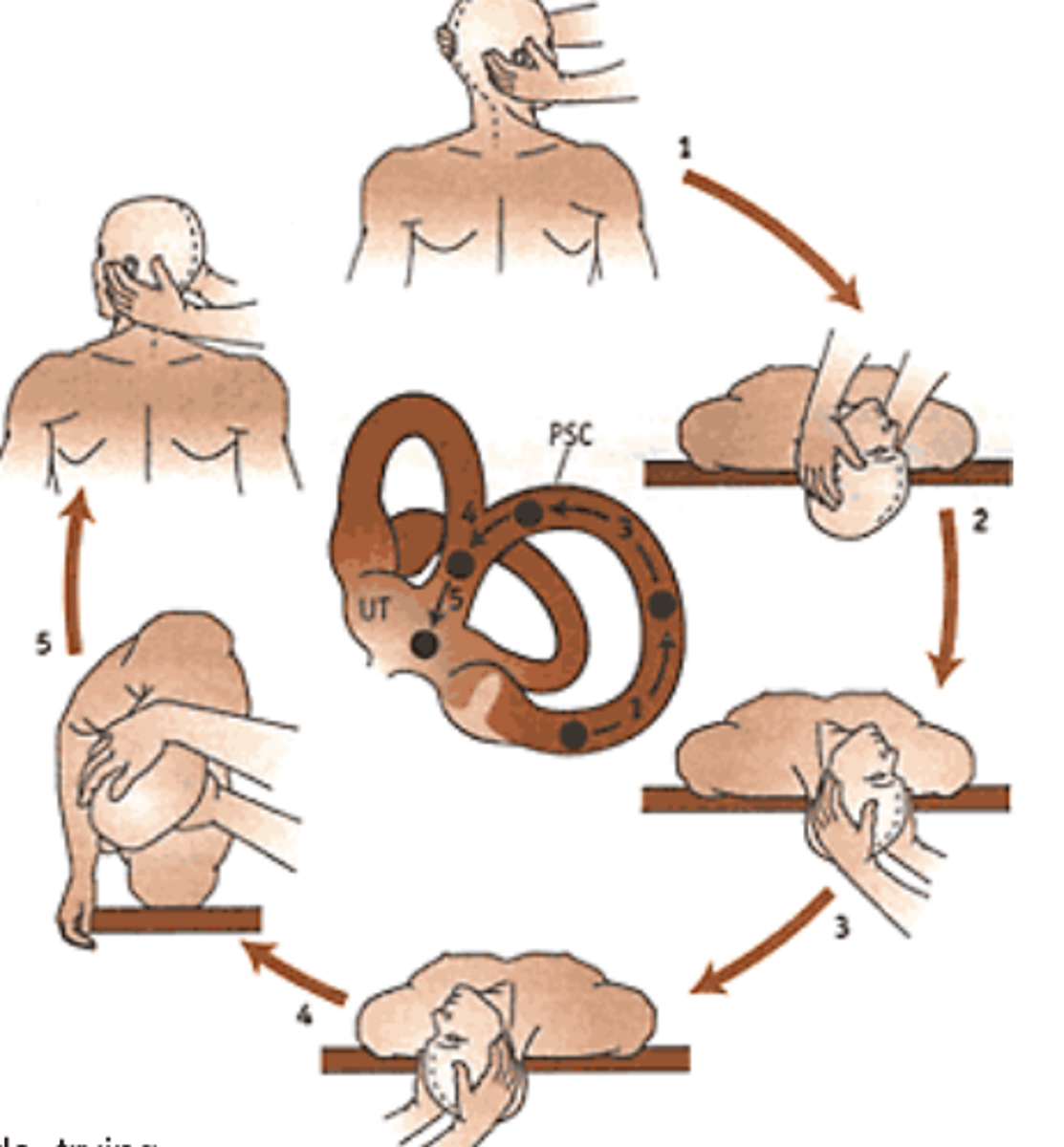
Epley maneuver
- Series of 4 head positions
- Maintain each for 1-2 minutes or until vertigo and nystagmus has stopped
- Add about 30 more seconds to ensure the otoconia stay put
Epley maneuver procedure
- 45 deg to more symptomatic side and 30 deg below horizontal
- Rotate 45 deg to other side keeping 30 deg declination
- Roll to sidelying (uninvolved side), nose down
- Slowly sit up, maintaining head position flexed (chin tucked) and rotated
- Slowly return the head to upright and remain sitting 3-4 min, then repeat until no symptoms are seen
A therapist is examining a patient's vestibular dysfunction. Thepatient is asked to assume a long sitting position. The patient's head is turned toward her left side while she is in a sitting position. The therapist then quickly moves the patient backward so that the head is extended over the end of the table approx.30 degrees below horizontal. This maneuver causes dizziness and vertigo. The repeat test to the right side did not produce any symptoms. The therapist reports these findings as:
A. Positive right Dix Hallpike test
B. Positive sharpened Romberg test
C. Positive left Dix Hallpike test
D. Positive Positional test
C. Positive left Dix Hallpike test
In vestibular, whichever side they turn the head, is the side that has the problem.
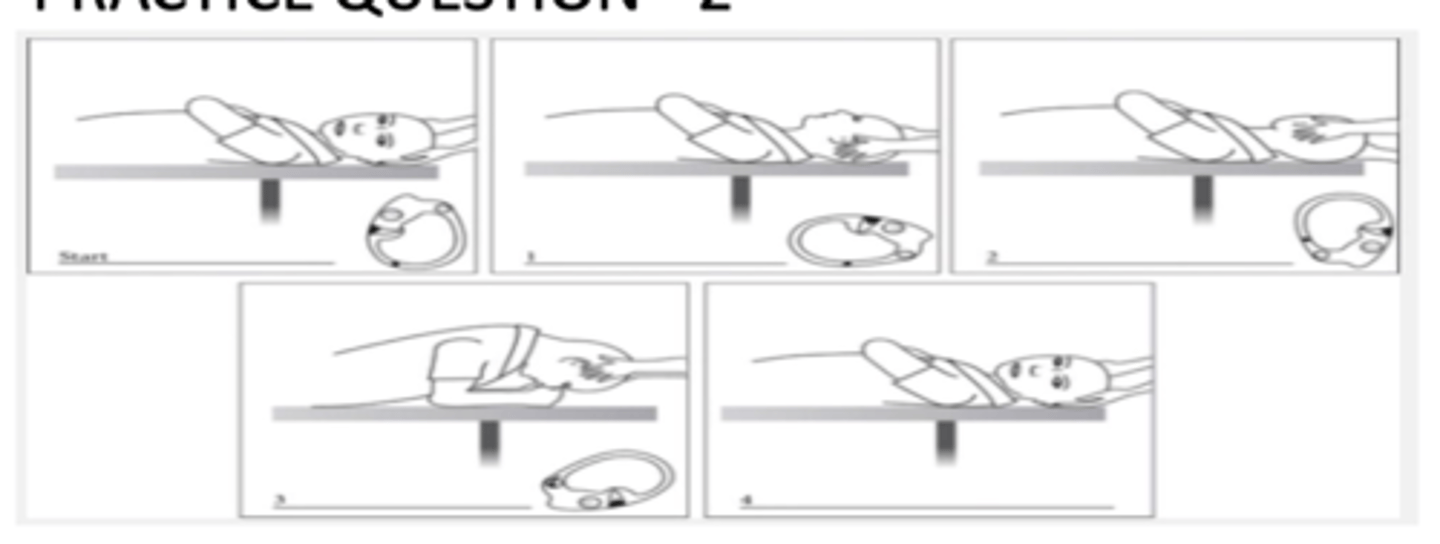
The physical therapist is performing the shown technique on a patient to treat his vertigo. What would be the most likely diagnosis for this patient?
A. Posterior semicircular Canal BPPV in Right Ear
B. Horizontal semicircular Canal BPPV in left Ear
C. Horizontal semicircular Canal BPPV in Right Ear
D. Posterior Semicircular Canal BPPV in Left Ear
B. Horizontal semicircular Canal BPPV in left Ear
This is BBQ roll. Left ear involved because it is the first side down.
What test is used to assess horizontal canal?
Supine roll test
What is the supine roll test used to determine?
Whether is it canalithiasis versus cupulithiasis
What is a positive supine roll test?
Horizontal nystagmus without torsion
Does geotropic nystagmus indicate canalithiasis or cupulithiasis?
Canalithiasis
Does ageotropic nystagmus indicate canalithiasis or cupulithiasis?
Cupulithiasis
Geotropic nystagmus
- Towards the ground
- Involved ear (to treat) is the side with more intense nystagmus
Ageotropic nystagmus
- Away from ground/airplane
- Involved ear is side with less intense nystagmus
A PT is evaluating a patient for loss of balance and dizziness. On assessment the patient presented with geotropic nystagmus which was stronger on the left side. Which of the following is the MOST likely diagnosis for this patient?
A. Left sided HC canalithiasis
B. Right sided HC canalithiasis
C. Left sided HC cupulolithiasis
D. Right sided HC cupulolithiasis
A. Left sided HC canalithiasis
Geo = canalithiasis
Ageo = cupulothiasis
What is the treatment for geotropic horizontal canal BPPV?
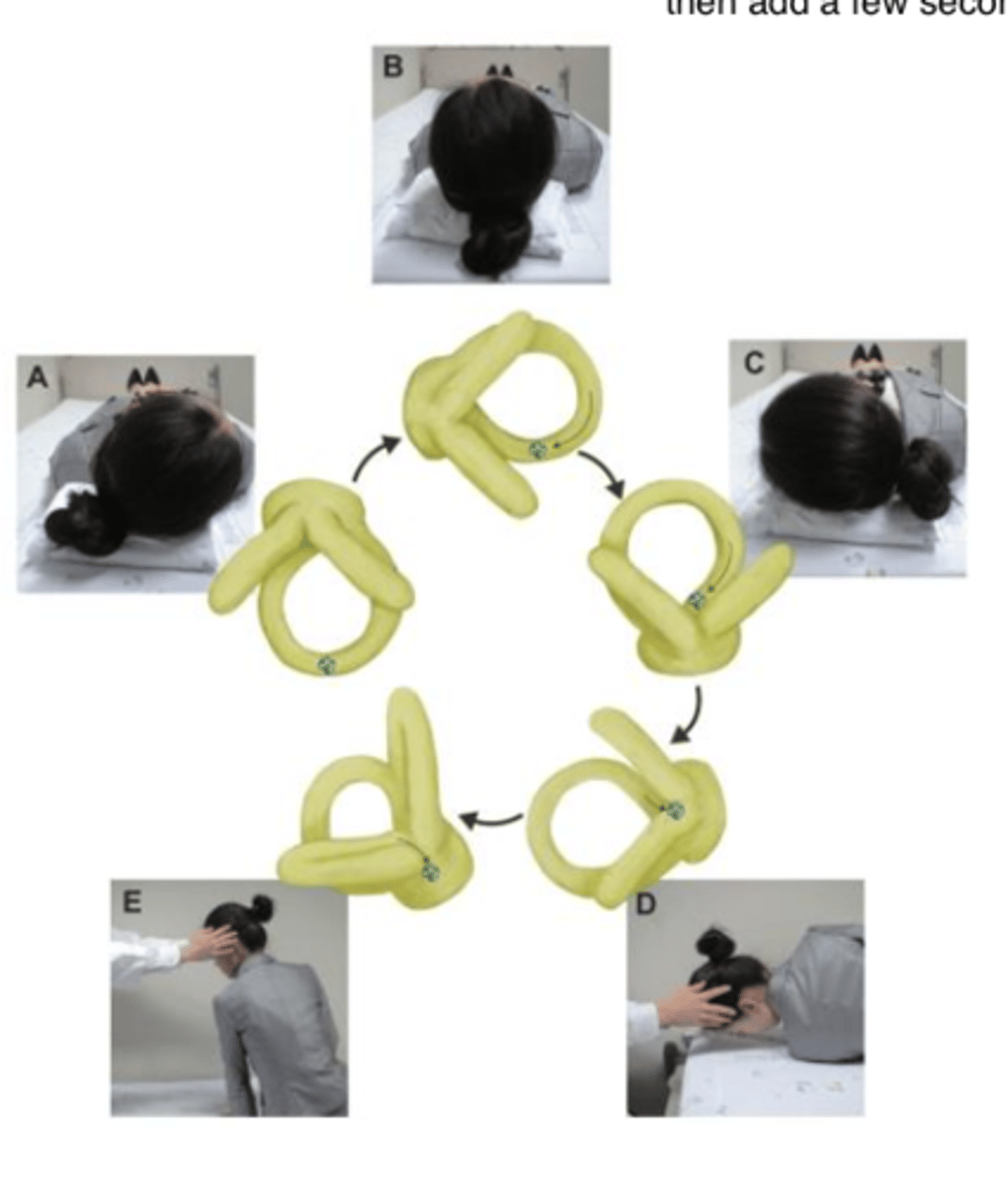
Barbecue roll
Barbecue roll procedure
- Patients head should be in 20 deg of cervical flexion
- After head turning toward the involved ear, head is then turned 270 deg toward unaffected side through a series of stepwise 90 deg turns before resuming sitting position
- Each position should be maintained for at least 15 sec or until induced nystagmus and vertigo are resolved
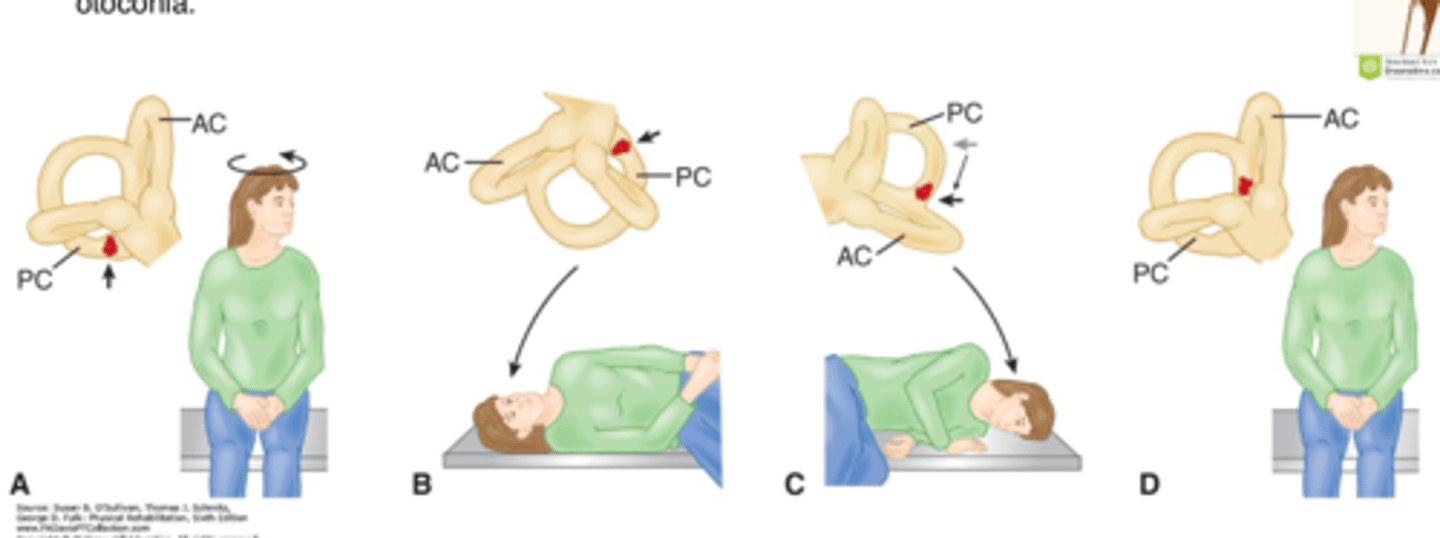
Treatment of cupulolithiasis
Liberatory (Semont) maneuver
Liberatory (Semont) maneuver procedure
- Head rotated 45 deg to OPPOSITE of involved side first (Example: to the L)
- With assistance, pt is then moved from sitting to R side lying and stays in this position for 1 min
- Patient then rapidly moved 180 deg, from R side-lying to L side-lying
- Head should be in original starting position, L rotated (nose down in final position)
- Otoconia have been dislodged from the cupola. After 1 min, return to sitting
Treatment of posterior BPPV home exercise program
Brandt-Daroff exercise
Brandt-Daroff exercise
- Patient brought into side-lying position with the head rotated toward other side
- Patient instructed to rapidly lie on their side, sit up, lie on the opposite side and then sit up again
- Each position maintained for at least 30 seconds or until vertigo stops
- Repeat this 10-20 times, three times a day until patient is without vertigo for 2 consecutive days
A physical therapist is visiting a 32-year-old female with diagnosis of BPPV in the clinic. What Techniques are the best way to treat Benign Paroxysmal Positional Vertigo?
A. Epley Maneuver and Semont Maneuver
B. Canalith Repositioning Maneuver and Gaze Stability Exercises
C. Brandt- Daroff Exercises and Gaze Stability Exercises
D. Epley Maneuver and Habituation Exercises
A. Epley Maneuver and Semont Maneuver
Habituation exercises are not used for BPPV. They are used for uniltaleral hypofunction. Gaze stability exercise are also used for unilateral hypofunction. Epley are semont are used for posterior BPPV. But Epley is for canalithiasis and Semont is for cupulothiasis.
Summary treatment: Canalith repositioning maneuver "Epley"
- BPPV due to canalithiasis
- Posterior SCC most common
- Both anterior and posterior
Summary treatment: liberators/semont manuever
- BPPV due to cupulolithiasis
- Posterior SCC most common
- Both anterior and posterior
Summary treatment: Brandt-Daroff exercises
- Persistent/residual or mild vertigo (even after CRM)
- For the patient who may not tolerate CRM
- To treat posterior SCC BPPV
Summary treatment: BBQ roll
Horizontal canal BPPV
Summary treatment: Gufani maneuver
Lateral BPPV
Central vestibular pathology
- CNS
- Brain stem vascular disease
- Arteriovenous malformations
- Acoustic neruomas
- Tumors of the brain stem and cerebellum
- MS
- Vertebrobasilar migraine
Presentation of central vestibular disorder
- Severe ataxia
- Abnormal smooth pursuit and abnormal saccadic eye movement tests
- Usually no hearing loss
- Diplopia, altered consciousness, lateropulsion
- Acute vertigo not usually suppressed by visual fixation
- Pure vertical/pendular nystagmus
Peripheral vestibular pathology
- Inner ear and vestibular nerve
- BPPV followed by uncompensated Meniere disease
- Vestibular neuritis
- Labyrinthitis
- Perilymphatic fistula
- Acoustic neruoma
Presentation of peripheral vestibular disorder
- Mild ataxia
- Normal eye movement
- Hearting loss, fullness in ears, tinnitis
- Sx of acute vertigo usually suppressed by visual fixation
- Acute vertigo usually intense
- Upsetting or downbeating torsional nystagmus
A PT is assessing a patient with chief concerns of dizziness and loss of balance. Presence of which of the following findings during assessment will MOST likely lead the therapist to refer the patient to a physician?
A. Mild Ataxia
B. Positional testing reproducing the nystagmus
C. Vertigo suppressed by visual fixation
D. Pendular nystagmus
D. Pendular nystagmus
With CNS involvment
- Would have severe ataxia
- Vertigo NOT suppressed by visual fixation
Both CNS and PNS involvement would result in positional testing reproducing the nystagmus
Smooth pursuit
Slow and smooth movements of the eyes to follow a moving target in the environment
Saccade
- Rapid, jerky movements of the eyes to bring the image of the target onto the fovea
- I.e. rapid movement of the eye between fixation points
Abnormal smooth pursuits and saccades indicates
Central vestibular pathology
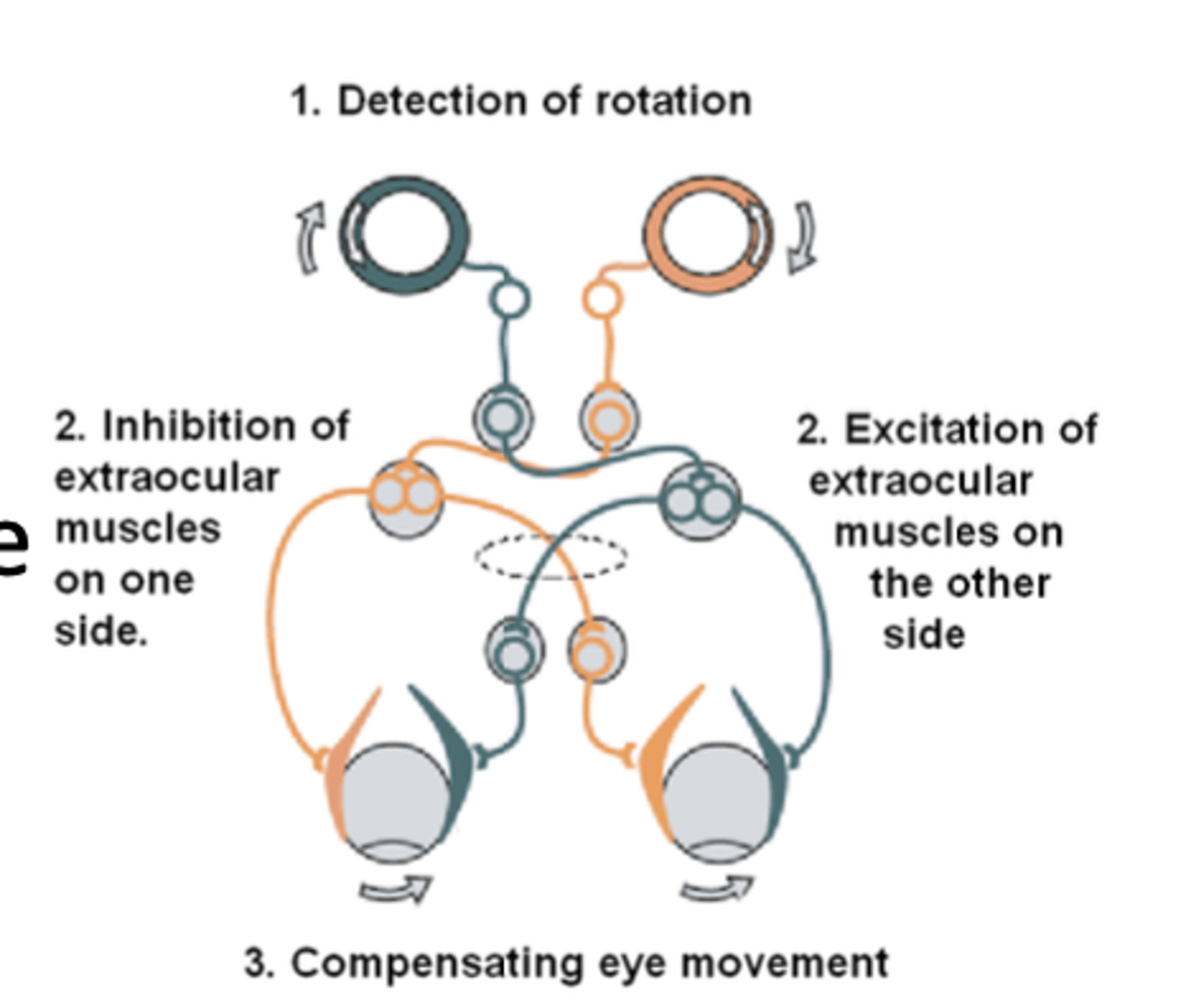
Vestibular ocular reflex (VOR)
- Allows for head/eye movement coordination
- This reflex supports gaze stabilization through eye movement that counters movement of the head
Is VOR intact in BPPV?
Yes
Impaired VOR
Head movement/velocity does not equal eye movement/velocity
Retinal slip
- Difference between eye velocity and head velocity
- Eyes lag behind, causing blurring of vision with head or eye movement
- Retinal slip of a few degrees results in significant decreases in vision and postural control
- When slip occurs = dec visual acuity, blurry vision (horizontal) or jumpy vision (vertical)
3 systems needed for balance
- Inner ear/vestibular
- Sensory receptors in legs
- Vision/eyes
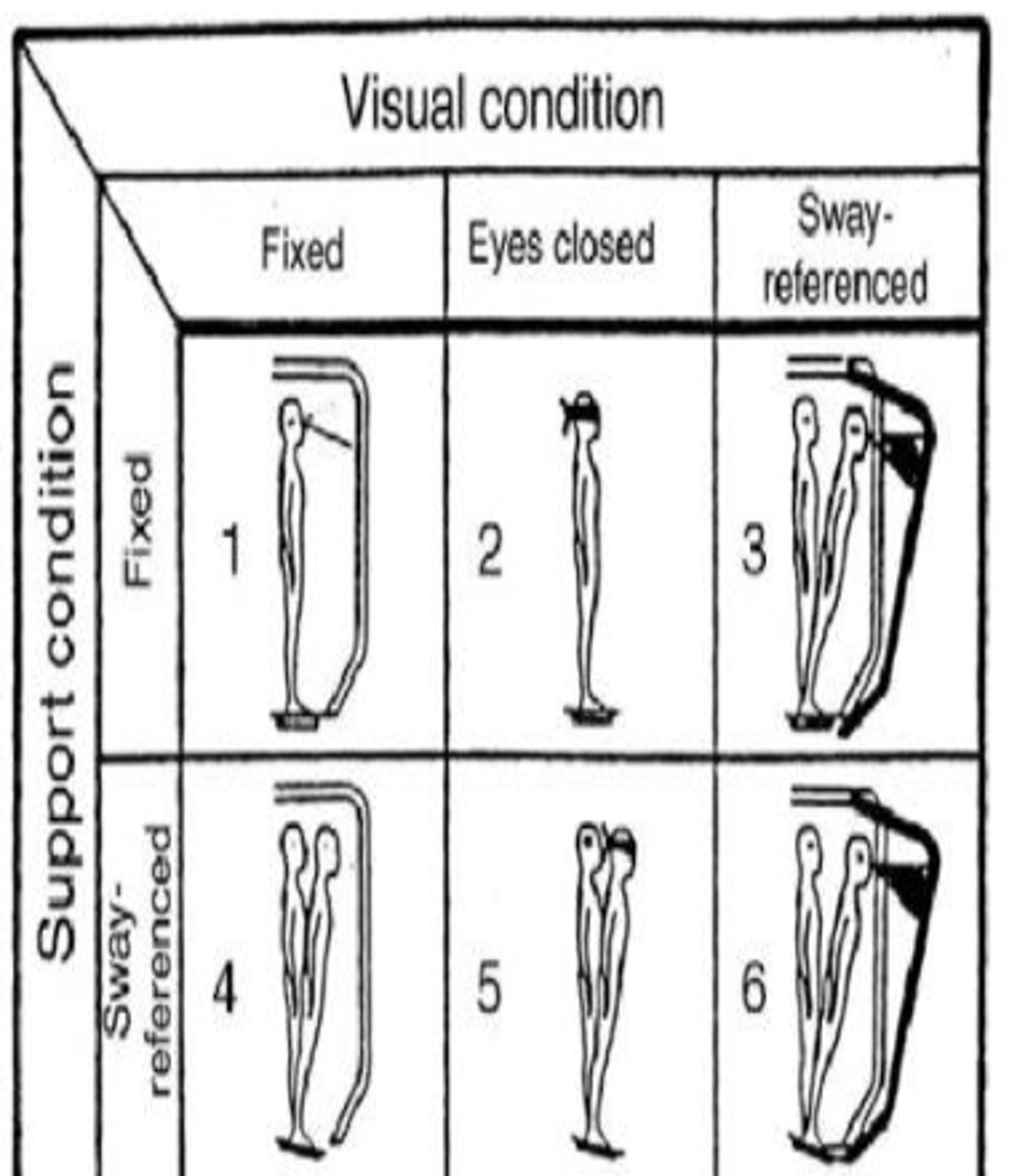
What does CTSUB stand for?
Clinical test of sensory interaction on balance
Order of recruitment of these balance systems
- Vision
- Somatosensory
- Vestibular
CTSIB: Condition 1
- Eyes open, firm surface
- Vision: eyes open
- Surface: fixed
- Disadvantaged system: none
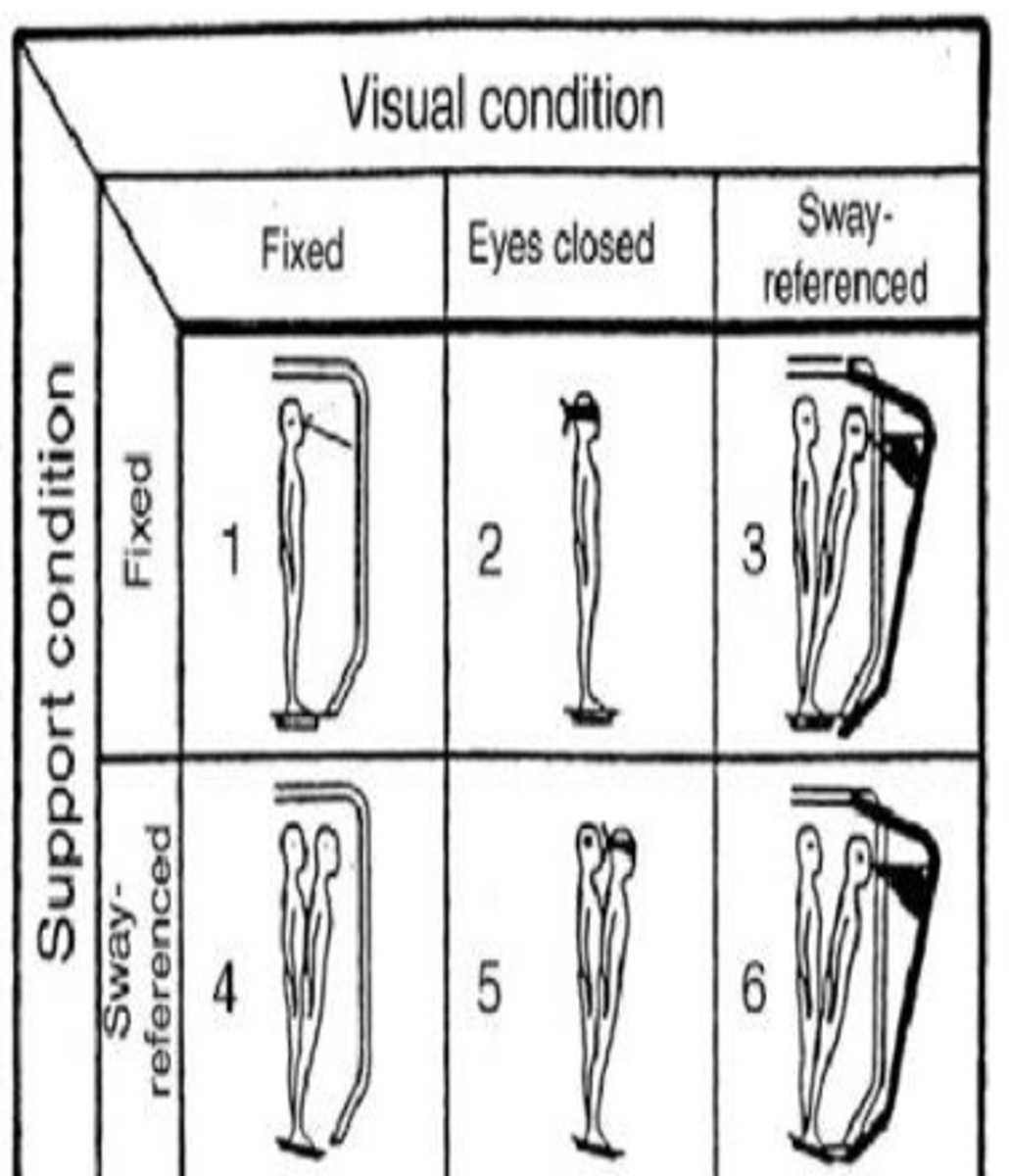
CTSIB: Condition 2
- Eyes closed, firm surface
- Vision: eyes closed
- Surface: fixed
- Disadvantaged system: vision absent
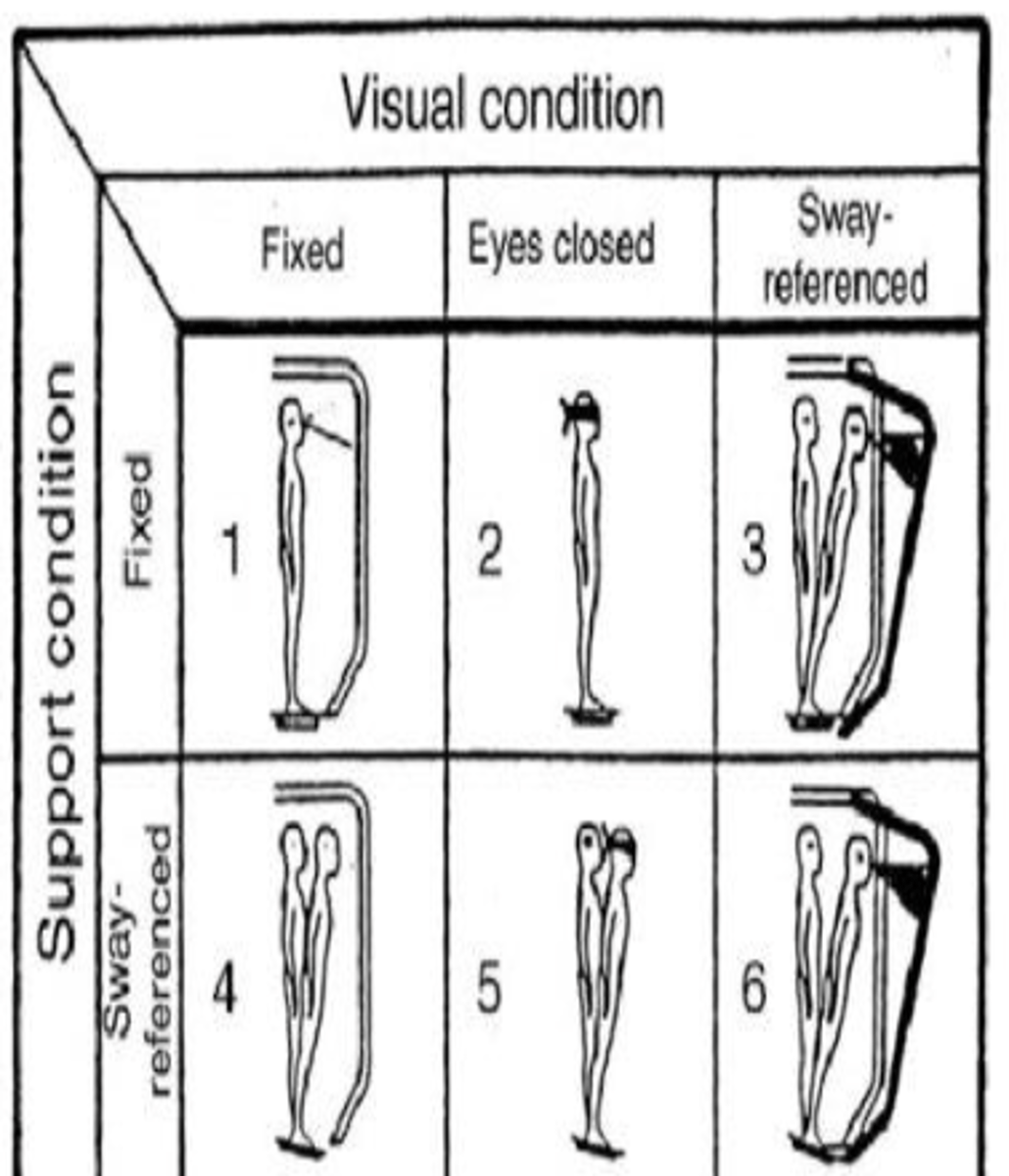
CTSIB: Condition 3
- Vision: sway referenced
- Surface: fixed
- Disadvantaged system: vision incorrect
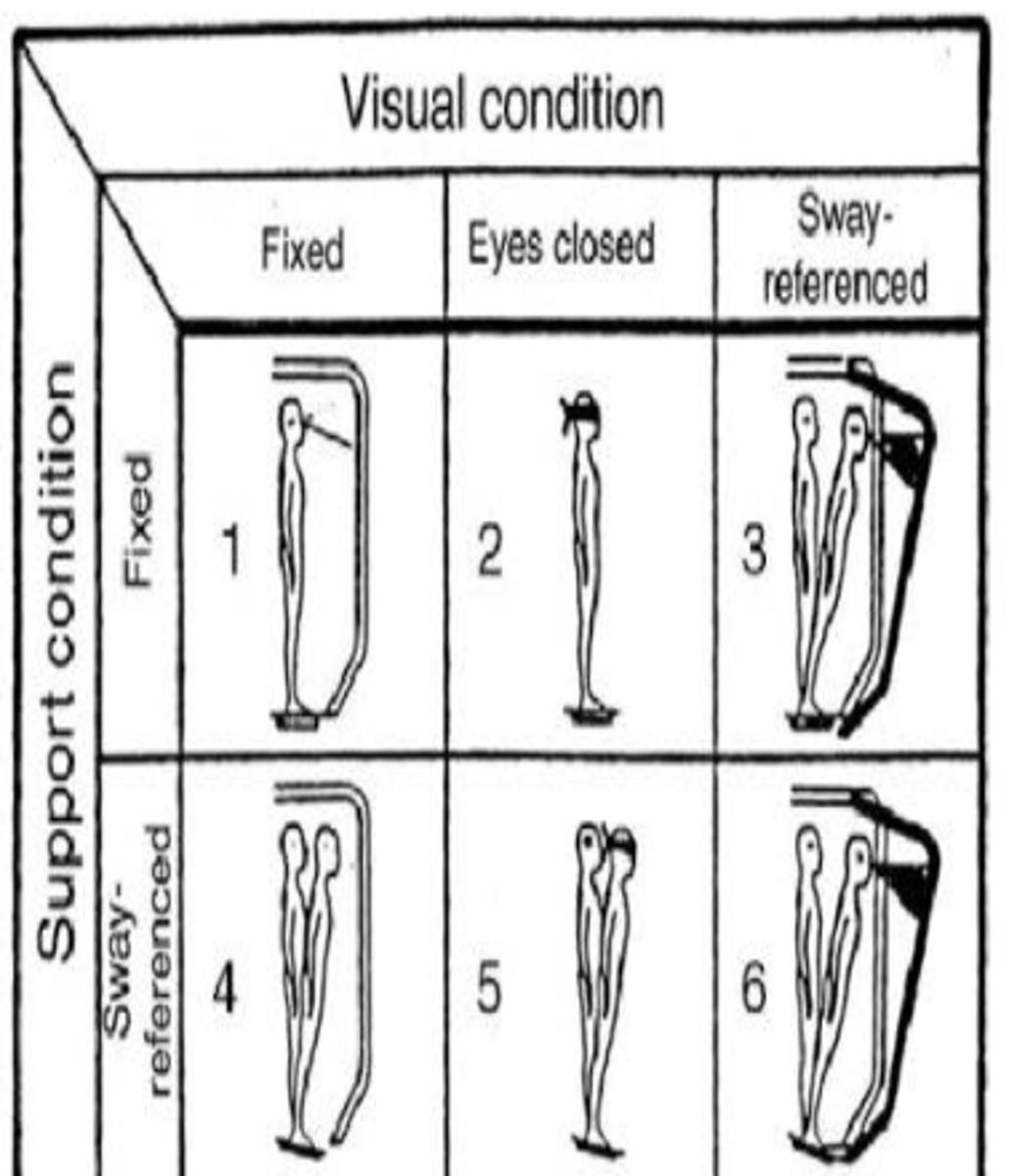
CTSIB: Condition 4
- Eyes open, foam surface
- Vision: eyes open
- Surface: sway referenced
- Disadvantaged system: somatosensory absent
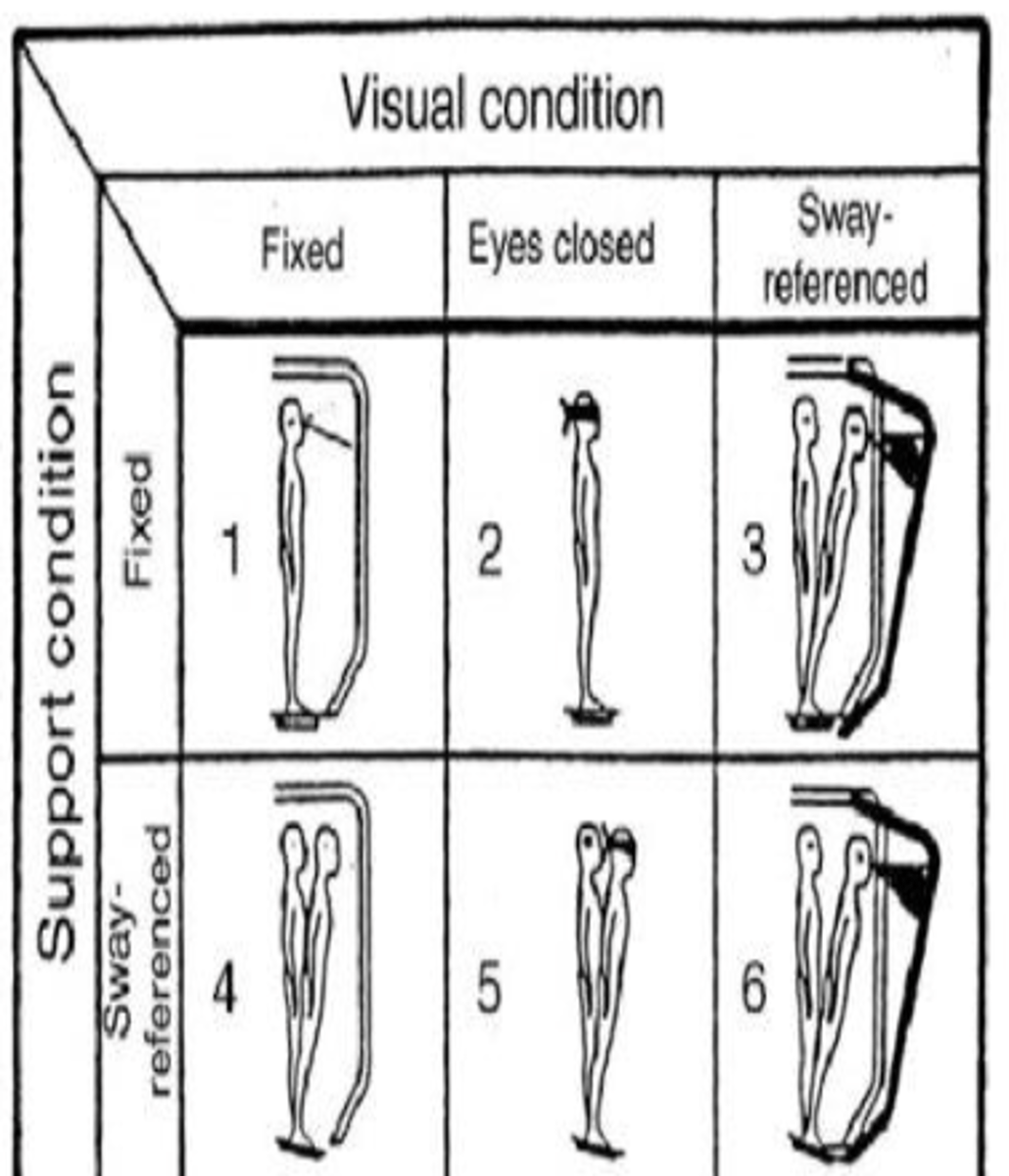
CTSIB: Condition 5
- Eyes closed, foam surface
- Vision: eyes closed
- Surface: sway referenced
- Disadvantaged system: somatosensory and vision
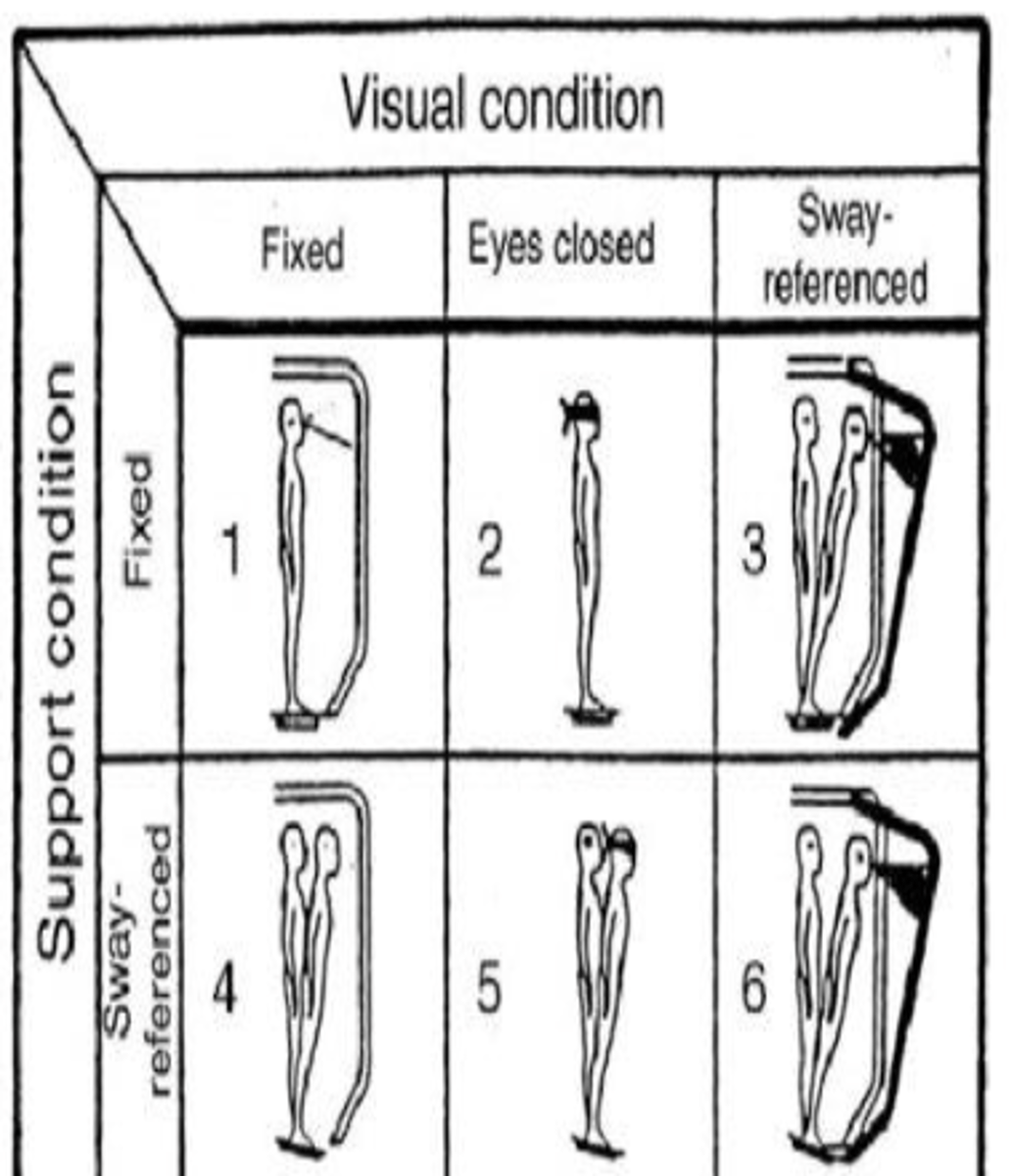
CTSIB: Condition 6
- Vision: sway referenced
- Surface: sway referenced
- Disadvantaged system: somatosensory absent, vision incorrect
Which systems are available in condition 1?
All 3
If patient is having difficulty with condition 1, which systems may be affected?
All of them
Which systems are dominant in condition 2?
- Somatosensory
- Vestibular
- Vision is removed
If patient is swaying in condition 2, which system is affected?
Somatosensory
Which systems are dominant in condition 4?
- Vision
- Vestibular
- Somatosensory removed
If patient is swaying in condition 4, which system is affected?
Vision
Which systems are dominant in condition 5?
- Vestibular dominant
- Somatosensory and vision removed
If patient is swaying in condition 5, which system is affected?
Vestibular
If a patient is dependent on vision, which conditions would they be unstable in?
2, 3, 5, 6
Because the eyes are closed or conflict between vision and vestibular system in these conditions
If a patient is dependent on somatosensory, which conditions would they be unstable in?
4, 5, 6
Because foam/ compliant surface present
If a patient has weakness or loss os vestibular system, which conditions would they be unstable in?
5, 6
Because their somatosensory and visual systems are not available
A patient reports feeling off balanced when walking on a crowded beach during the day where he has to look out for people as he walks. The Physical Therapist should suspect that the patient would have difficulty in which of the following conditions during testing with the CTSIB?
A. Condition 2 (ECSS)
B. Condition 6 (VCMS)
C. Condition 4 (EOMS)
D. Condition 5 (ECMS)
B. Condition 6 (VCMS)
Crowded beach and looking out, what does that make the patient do = visual conflict. Eyes are open, but there is a visual conflict more so due to the volume of people.
A patient presents to the clinic and scores poorly in conditions 4,5,6 on the CTSIB test. At which of the following is the appropriate conclusion?
A. Patient is dependent on vision for balance
B. Patient is dependent on somatosensory system for balance
C. Patient is dependent on vestibular system for balance
D. Patient's somatosensory system is affected
B. Patient is dependent on somatosensory system for balance
If patient was dependent on vision, they would have difficulty with conditions 2, 3, 5, 6. If the patient was dependent on vestibular system, they would be unstable on conditions 5, 6. Cannot infer that something is affected. CTSIB looks at which systems they are dependent on.
Unilateral vestibular hypofunction (UVH)
- Impairment of balance system in the inner ear
- Peripheral vestibular system is not working properly in one ear (viral insults, trauma, vascular events)
Symptoms of UVH
- Dizziness or vertigo
- Poor balance, especially with head turns
- Blurred vision, especially when turning your head quickly
- Nausea
- Trouble walking, especially outdoors, in dark rooms or in crowded places
Causes of bilateral vestibular hypofunction (BVH)
- Ototoxicity
- Meningitis
- Autoimmune disorder
- Head trauma
- Tumor on 8th CN
Symptoms of BVH
- Oscillopsia (vision blurring with head movements)
- Disequallibirum
- No nausea
- Gait ataxia
Otitis media
- Infection of the middle ear
- Causes fever and ear pain
Ototoxicity
Ear poisoning caused by drugs
UVH intervention
- Adaptation --> gaze stabilization exercises
- VOR x1
- VORx 2
VOR x1
- Target is stable
- Head movements while eye stay focused on target
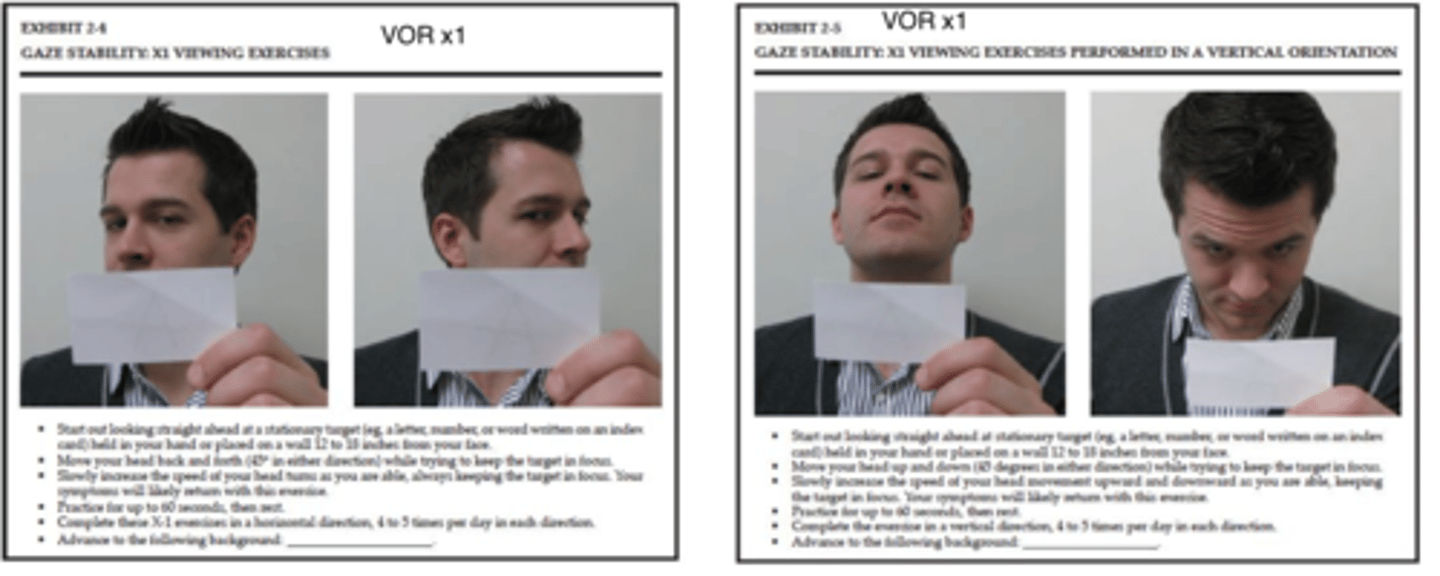
VOR x2
- Progression of x1 viewing
- Target and head/eyes move in opposite directions
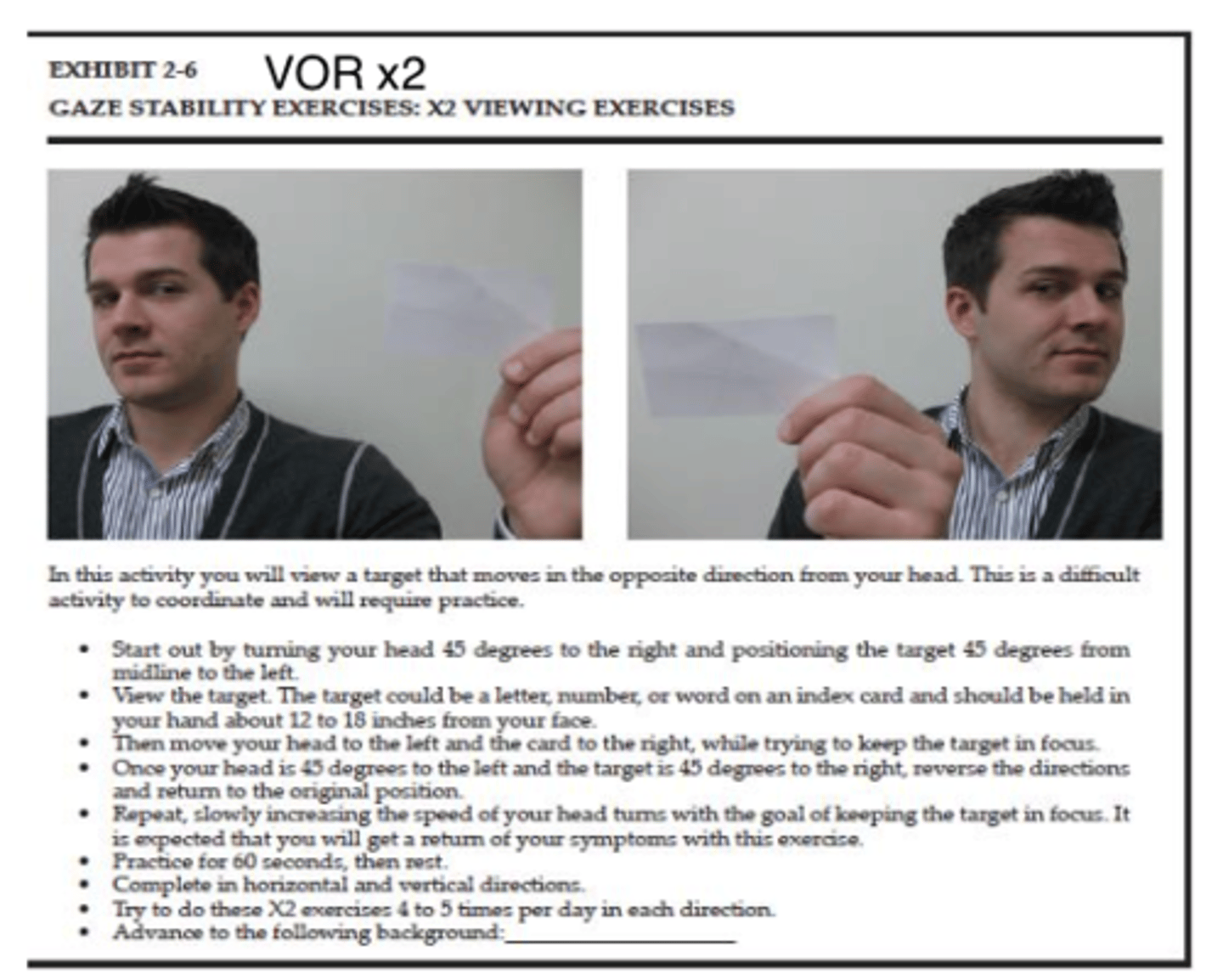
How to progress BVH interventions
- Progress to increasing the distance used to see the target
- Then use a busy background (checkerboard, Venetian blinds)
- Progress to doing this in standing
A Physical Therapist has determined that a patient has unilateral vestibular hypofunction. What would be the MOST appropriate INITIAL home exercise to provide to the patient?
A. Brandt-Daroff Exercises
B. VOR x2 Walking
C. Walking towards a busy wallpaper
D. VOR x1 sitting
D. VOR x1 sitting
UVH = gaze stability exercises.
VOR x1 because asking for initial intervention. Brandt-daroff = BPPV exercises.
A patient present to a clinic with complaints of dizziness and vertigo in some positions. On examination, the PT found that pt has his head tilted to one side, conjugate eye torsion, and an abnormal weight shift to one side. These signs are MOST consistent with what condition?
A. Unilateral vestibular hypofunction
B. Otitis media
C. Ototoxicity
D. Malingering
A. Unilateral vestibular hypofunction
Malingering = pt thinks they have something when they really dont. Otitis media has to due with middle ear and fullness in the ear. Ototoxicity = drug involvement.
Head tilted, abnormal shift, something unilateral.
A patient referred for vestibular rehab presents with spontaneous nystagmus that can be suppressed with visual fixation, oscillopsia, and a loss of gaze stabilization. Additional symptoms found during examination are disequilibrium, an ataxic wide-based gait with consistent veering to left. Based on these findings, the patient is MOST likely to have which condition?
A. BPPV
B. Acute UVH
C. Acoustic neuroma
D. Meniere's disease
B. Acute UVH
With BPPV, they cannot suppress the nystagmus. We know the cause of the nystagmus = misplaced otoconia.
C & D = with respect to one side involved, wide based gait and veering, and feeling wobbly = acute UVH.