Truelearn NPTE study guide
1/321
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
322 Terms
What is the rancho los amigos scale?
a scale to determine cognitive function following TBI
Level I: no response to pain, touch, sound, or sight
Level II: generalized reflex response to pain
Level III: localized response, blinks to strong light, turns toward/away from sound, responds to physical discomfort, inconsistent response to commands
Level IV: confused/agitated; alert, performed motor activities but behavior is non-purposeful, extremely short attention span
level V: confused/non-agitated; gross attention to environment, highly distractible, inappropriate verbalization
Level VI: confused/appropriated. inconsistent orientation to time and place. consistently follows simple directions
level VII: automatic/appropriated. skilled noticeably deteriorated
Level VIII: purposeful/appropriate
Lymphedema stage 0
Latency;
has no outward swelling and the body can continue to respond appropriately to lymphatic load
Lymphedema stage I
reversible;
-has soft or pitting edema
-no skin changes
-negative stemmers sign
lymphedema stage II
spontaneously irreversible;
-swelling that can no longer pit (no indentation)
-skin changes are present; hard with decreased mobility
-fibrotic tissue with brawny, hard swelling
- positive stemmers sign (inability to lift a skin fold to the second toe)
-frequent infections
lymphedema stage III
lymphostatic elephantiasis;
-positive stemmers sign
-non-pitting edema
-much greater skin volume; skin changes more pronounced and hard with little mobility
-darkened skin with papillomas (benign skin growths), deep skin folds, hyperkeratosis
-infection is common
Spinalthalamic tract relays which types of information in the spinal cord?
-pain (fast nociception- localized well defined pain; A delta fibers)
-crude touch
-temperature
dorsal column-medial leminiscus(DCML) tract relays which type of information in the spinal cord?
-light touch (discriminative)
-conscious proprioception
-vibration
spinocerebellar tract relays which type of information in the spinal cord?
unconscious proprioception
anterior spinalthalamic tract relays which type of information in the spinal cord?
slow nociception - diffuse, and poorly localized pain; C fibers
lateral corticospinal tract relays which type of information in the spinal cord?
voluntary fractionally movement to limbs and multi-joint movement or fine motor
medial corticospinal tract relays which type of information in the spinal cord?
motor to axial and abdominal muscles
the gracile fasciculus relays which type of information in the spinal cord?
part of DCML that relays light touch and proprioception to lower leg
the radial nerve innervates what muscles?
triceps, brachioradialis, supinator, extensor carpi radialis longus and brevis, extensor carpi ulnaris and finger extensors
The results of a MMT are 5/5 for all motions except elbow extension, which is 1/5, elbow flexion is 4-/5 supination is 4/5, wrist extension is 1/5, and finger extension is 1/5. which of the following is most likely the explanation for the weakness?
radial nerve injury
3 multiple choice options
what muscles would be weak with a median nerve injury?
wrist and finger flexors
what type of glide at the hip would improve hip extension ROM?
grade 4 anterior glide
3 multiple choice options
what type of glide at the hip would improve hip flexion ROM?
grade 4 posterior glide
3 multiple choice options
common fibular (peroneal) nerve innervates which compartments of the leg?
anterior and lateral compartments of lower leg
grade 3 mobilization to the distal femur in a posterior direction results in an increase of what ROM?
knee extension
when a patient performs forward flexion, a rib hump on the right side is revealed. this means the vertebrae is rotated __ and protrudes ___ on the right side of the body
to the right; posteriorly
3 multiple choice options
what are the symptoms of systemic lupus erythematous
-malaise
-fever
-skin lesions (butterfly rash across the cheeks/nose)
-chronic fatigue
-arthritis
-arthralgia
-anemia
-commonly have Raynaud phenomenon
what is the common clinical presentation of scleroderma?
-skin becomes firm and edematous
-fibrosis of skin, joints, blood vessels, organs
-commonly accompanied by Raynaud phenomenon
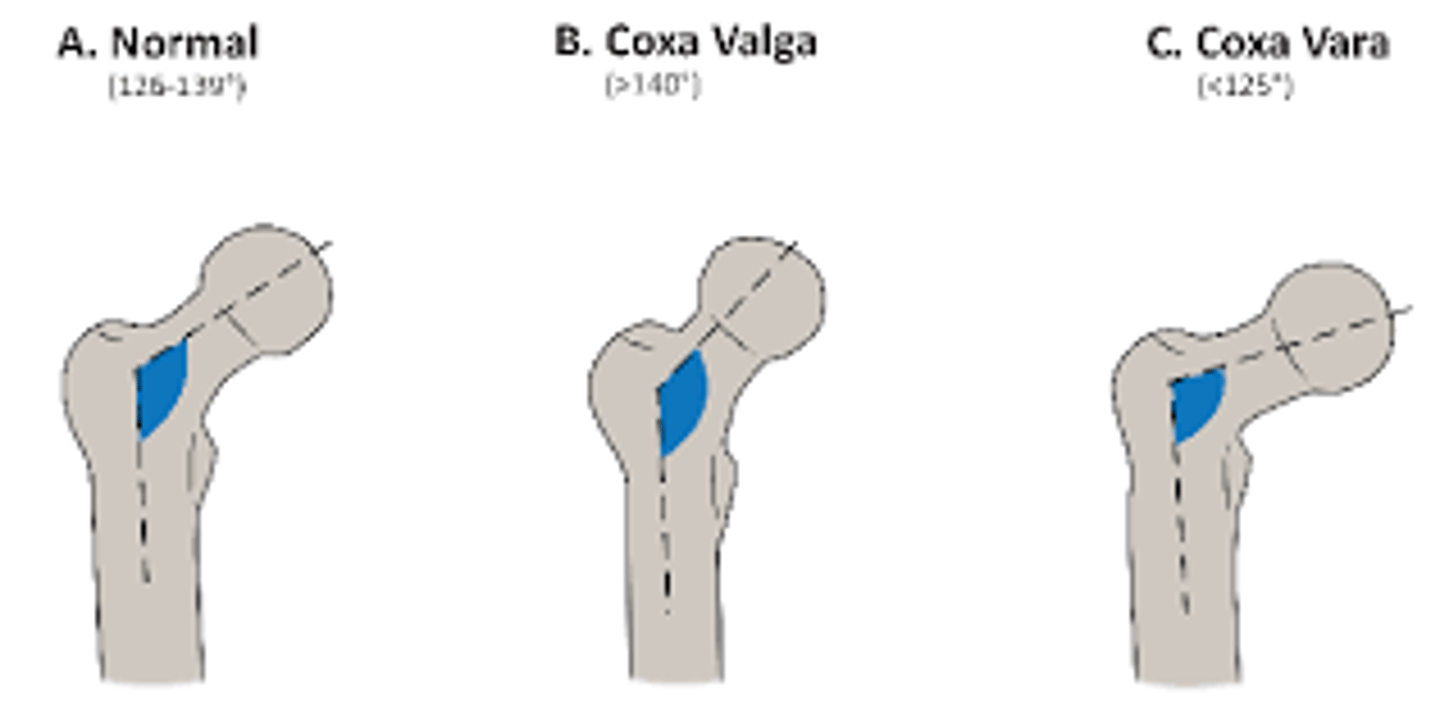
when the angle of inclination is >140 degrees, this is termed as?
coxa valga
3 multiple choice options
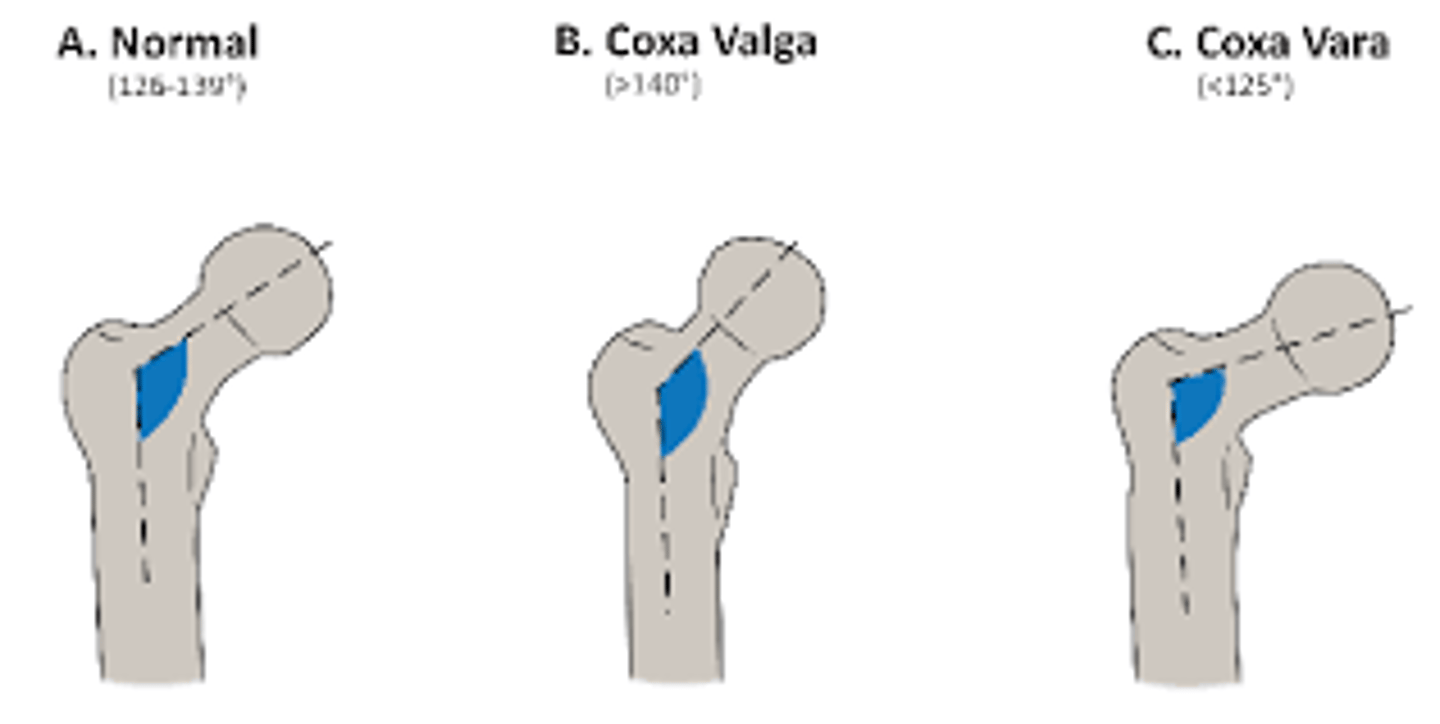
when the angle of inclination is <125 degrees, this is termed as?
coxa vara
3 multiple choice options
describe stage 1 of pressure ulcer
non blanching erythema; intact epidermis
describe stage 2 of pressure ulcer
partial thickness ulcer involving epidermis and dermis; blanchble
describe stage 3 of pressure ulcer
-full thickness ulcer extending through dermis in to subcutaneous tissue
-blisters and weeps
-does not blanch
-less painful than stage 1&2;
- diminished sensation to light touch and pin prick
-requires surgery
describe stage 4 of pressure ulcer
-Full-thickness tissue loss with exposed bone, muscle, or tendon;
-often undermining
what are the characteristics of superficial burn
-<3 days to heal
-blanching present
-pink, red, wet
-sensation intact and painful
-does not blister or scar
what are the characteristics of partial thickness burn
-3-7 days to heal
-pink, red, edema
-blanches
-blisters and weeps
-more painful than stage 1
-intact to light touch
what are the characteristics of deep partial thickness burn
-2-6 weeks to heal
-blisters and weeps
-skin is white and waxy
-does not blanch
-less painful than stage 1&2
- diminished sensation to light touch and pin prick
-requires surgery
what are the characteristics of full thickness burn
-requires surgical intervention (time to heal depends)
-white, waxy, leathery, dark eschar
-high risk for infection
- absent sensation to light touch and pin prick
-large areas require skin graft
what is the proper splint position to immobilize the wrist, MCP, and IP joints following a fracture?
wrist: 0-30 of extension, MCP: 70-90 flexion, and IP: full extension
3 multiple choice options
what are the pathological changes in a patient with multiple sclerosis
demyelination and plaques in the white matter
3 multiple choice options
two-point discrimination is the most defined and should be tested on which area of the body?
distal upper extremities
3 multiple choice options
what is the BEST instructions to give to a patient for pursed-lip breathing?
expiration should be twice as long as inspiration
3 multiple choice options
describe the characteristics of inflammatory phase in wound healing
-prepares the wound for healing;
-redness, edema, warmth, and pain;
-typically lasts 1-6 days
describe the characteristics of proliferative phase in wound healing
-the rebuilding of damaged structures;
-inflammatory response subsides;
-epithelialization, collagen production, wound contraction, and neovascularization occur simultaneously
-occurs between 3-20 days
describe the characteristics of maturation phase of wound healing
-scar is remodeling with changes in size and form
-scar tissue matures and strengthens
-typically lasts between 9 days and 2 years
abnormal kidney function is determined by ___?
elevated blood urea nitrogen and creatine levels
3 multiple choice options
the apprehension test involves a ___ directed force to the posterior humeral head, and stresses the ___.
anterior; anterior structures (glenohumeral ligament, anterior capsule, labrum)
3 multiple choice options
what are symptoms of complex regional pain syndrome (CPRS)?
severe pain/hypersensitivity when touched lightly, vascular changes, limited PROM
what causes scapula winging?
tight pec minor and weak serrates anterior
what is the most common DMARD?
methotrexate
3 multiple choice options
what is the effective doses to administer iontophoresis
effective drug delivery: 40 - 80 mA-min;
treatment dosage example: 2 mA x 20 min
where does the left middle cerebral artery provide blood supply?
the lateral convexity of the cortes areas- controls right upper extremity motor and sensory function, expressive and receptive language, loss of visual field
what impairments are present with left middle cerebral artery stroke?
right upper extremity weakness and aphasia
what impairments are present with right middle cerebral artery stroke?
loss of visual field, homonymous hemianopsia, spatial neglect
what impairments are present with left middle cerebral cortex damage?
apraxia
what is apraxia
inability to perform motor activities upon command while sensory and motor systems are still intact
what is hemianopsia
cut in a visual field that may occur after a stroke
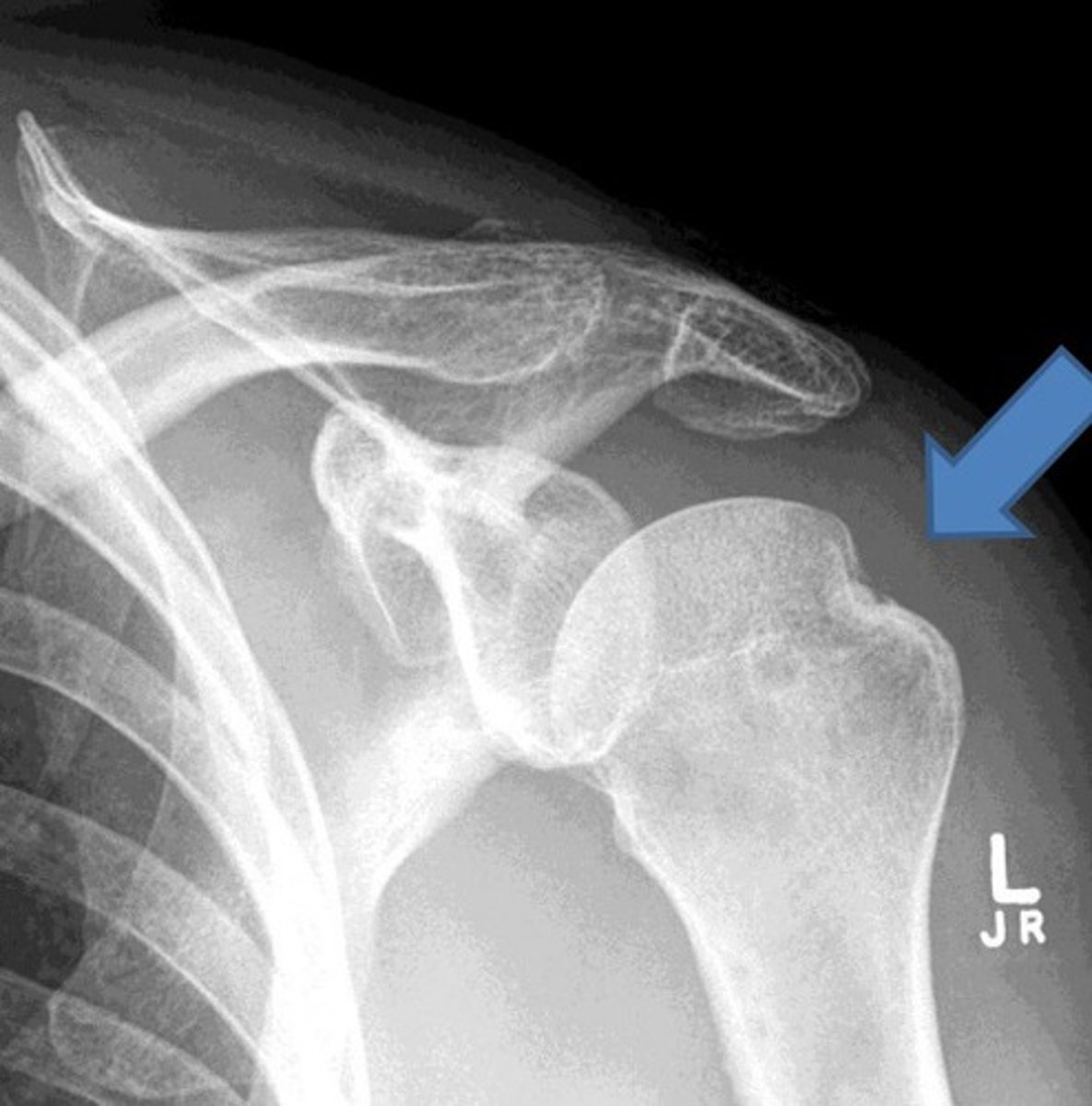
what is the most common shoulder dislocation?
anterior
3 multiple choice options
what is a hill-sachs lesion?
compression fracture of posterosuperior humeral head; when humeral head anteriorly dislocates, humeral head strikes against the front of the glenoid
what is a reverse hill-sacs lesion?
part of the anteriormedial potion of the humeral head fractures due to a posterior dislocation of the shoulder
what is a bankhart lesion?
part of labrum tears during anterior dislocation of shoulder

what is a bony bankhart lesion?
a piece of the anterior inferior glenoid is fractured during anterior dislocation of shoulder

tightness in the posterior capsule presents as limited PROM of which motion?
internal rotation
tightness in the inferior capsule presents as limited PROM of which motion?
abduction
tightness in the superior capsule presents as limited PROM of which motion?
adduction
tightness in the anterior capsule presents as limited PROM of which motion?
external rotation
what are intrinsic cues (sensory events occurring during movement)
-visual
-vestibular
-proprioceptive
-cutaneous
what are extrinsic cues?
-auditory
-tactile
-visual
what kind of intervention does mid portion achilles tendinopathy respond best to?
slow, controlled, eccentric loads; lowering into dorsiflexion off a step; improve dorsiflexion ROM, plyometrics once reduction of pain and strength is built
cholecystitis symptoms worsen when eating what types of foods?
fatty foods
what is a clinical sign/symptom of peptic ulcer disease?
dark, tarry-looking stool
what is indicative of an inverted t-wave?
ventricular repolarization
what conditions would an inverted t-wave appear on an ECG
myocardial ischemia, ventricular overload, hypertrophic cardiomyopathy, acute cerebrovascular events, myocarditis, pericarditis, PE
what drugs are used to treat seizures
barbiturates, benzodiazepines, and hydantoins
what nerve roots are affected for erbs palsy and what motions do they exhibit?
C5/C6 nerve.
-shoulder internal rotation and adduction with wrist flexion and finger extension ("waiters tip")
-increased risk during breech vaginal delivery, with use of forceps, weight over 8 lbs
what nerve roots are affected for klumpke's palsy and what motions do they exhibit?
-C8/T1 nerve roots
-MCP extension, flexion of phalangeal joints ("claw position")
- affects muscles of hand and sensation of medial arm
what is Huntingtons disease? s/s?
neurodegenerative disease due to genetic abnormality on chromosome 4>breakdown of basal ganglia> too much dopamine
-causes sx to present in ages 30-40yrs
-leads to death within 10-20yrs of dx
s/s:
-movement dysfunction ( chorea): fidgety, uncontrollable writhing movements
-hyperkinesia - quick mvmnts
-ataxia
-cognitive sx (executive function, inattention, depression, psychosis )
-spasticity
-clonus
What is Alzhiemer's Disease? s/s?
-slow degenerative disease causing progressive loss of memory, cognition, and language
-accumulation of hyper-phophorylated Tau protein and extracellular amyloid- plaques causing loss of nerve cells.
s/s: primary sx-progressive memory loss
-dx in 60 yrs +
What is Korsakoff's syndrome? s/s
-neurological condition caused by chronic alcoholism
-confabulation, decreased short-term memory, decreased long term memory
What is Parkinson's disease?
-Movement disorder caused by the death of cells that generate dopamine in the basal ganglia and substantial nigra.
-dx in 60+ yrs
-s/s: resting tremor,
-bradykinesia- slowed movement
-rigidity
-resting tremor
-facial weakness/rigidty
-shuffling gait
-difficulty initiating movement
-cognitive sx
-reduction in capacity for language
-balance deficits
what are common spastic gait abnormalities?
can be unilateral or bilateral-
-stiff-legged
-circumduction
-scissoring
-toe-walking
-decreased arm swing
-unsteady and falling toward side of greater spasticity
-localized in unilateral or bilateral corticospinal tracts
- commonly seen with cerebral palsy, multiple sclerosis, spinal cord lesions, and cortical, subcortical, brainstem infarcts.
what is ataxic gait?
describes as wide-based, unsteady, staggering side to side
-falling toward side of worse pathology.
-can be detected with tandem gait testing
-seen in pts with cerebellar dysfunctions
what is vertiginous gait?
Unsteady, wide-based walking with swaying and falling, worsened with eyes closed and feet together
-seen in pts with ischemic of vestibular nuclei, BPPV, Menderes disease
what is anterograde amnesia
unable to recall recent memory, able to recall older information and memory
-typically from damage to frontal or temporal lobes of brain
what is retrograde amnesia?
inability to recall past memories
what is post-traumatic amnesia?
causes both retrograde and anterograde amnesia; the time between the injury and when the patient is able to recall recent events
what is transient global amnesia
temporary loss of the ability to form new memories or recall recent memories that occurs without a clear neurological explanation
what type of diagnostic tool is used on infants to determine if they are having seizures
electroencephalograms
which gait parameters are WNL in patients with mid-stage Parkinson's disease
speed, stride length, double limb support
what are the symptoms of a failing ventriculoperitoneal (VP) shunt for CSF?
-headaches
-cognitive difficulties
-nausea
-vomiting
-drowsiness
(emergent situation!!)
what is summed feedback of motor learning?
feedback given after a set number of trails, such as every 3rd attempt
what is constant feedback in motor learning?
PT gives feedback after every trial
what is faded feedback in motor learning?
feedback is given initially after every trial and then less often such as every 2nd trial, then every 4th trial
what is bandwidth feedback in motor learning?
feedback given only when the patient makes an error that is outside acceptable performance
what is MOI to the cervical spine would result in complete bilateral loss of motor, pain, and temperature below the level of lesion with vibration preserved throughout?
hyperflexion - anterior cord syndrome
3 multiple choice options
what is MOI to the cervical spine would result in motor loss with greater involvement of UE>LE?
hyperextension - central cord syndrome
3 multiple choice options
what is MOI to the cervical spine would result in unilateral loss of motor and sensory function on the ipsilateral side of lesion, loss of temperature and pain on the contralateral side
Ipsilateral penetration - unilateral hord hemisection
2 multiple choice options
what score is considered fall risk on the TUG?
>14 sec
what score is considered fall risk on functional reach
<10 inches
what score is considered fall risk on BERG
< 45/56
what score is considered fall risk on 5x STS
>16 sec
what score is considered fall risk on 30sec STS
for ages 60-64:
<12 female
<14 male
what is the number one most effective intervention to treat uterine prolapse?
kegel exercises to strengthen pubococcygeal muscles
which motions at the ankle isolate the common peroneal (fibular) nerve during SLR test?
PF and INV PIP
3 multiple choice options
which motions at the ankle isolate the common tibial nerve during SLR test?
DF and EV (or toe ext) TED
3 multiple choice options
which motions at the ankle isolate the common sural nerve during SLR test?
DF and INV SID
3 multiple choice options