Aural Rehab Final Exam
1/74
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
75 Terms
4 components of Boothroyd model of AR
sensory management, instruction, perceptual training, and counseling
Counseling (4)
-a part of a person-centered approach that helps people learn about and adjust to a disorder, condition, or situation and cope with their feelings, thought, and behaviors
-infused throughout interactions
-Goal to set clear and realistic expectations and improve quality of life
-within scope of practice to provide counseling for clients with communication disorders
informational counseling (3)
-educating patient and or families about nature and impact of HL, variety of interventions available, how interventions work to reduce negative impact
-need to assess patient and or family needs prior to making therapy plans
-establish through questionnaires
Adjustment counseling
-helping patients and or families identify and address internal barriers and external barriers
internal barriers
denial, shock, stress, perceived stigma, readiness for intervention
external barriers
how to access services, learning new info related to interventions and therapy, evaluating info, associated with ear condition: support, ongoing support to implement skills to manage adjustment and challenges to living with a HL
Person-centered care (8)
-relationship between the professions and patient-mutual trust and respect
-partnership focused on client needs
-active listening/empathic listening
-involve family and communication partners to make decisions and set goals
-clinician is genuine and transparent when interacting with clients
-clinician fully accepts and respects their client
-clinician practices empathy to understand the world as their client does
-culturally responsive care
Stages of health behavior change (5)
-precontemplation
build awareness for my need to change
-contemplation
increase my pros for change and decrease my cons
-preparation
commit and plan
-action
implement and revise my plan
-maintenance
integrate change into my lifestyle
Motivational interviewing tools (4)
-purpose is to elicit self motivational statements to make patients realize that they are using their own free will in deciding to change
-the circle (info, education, advice, encouragement, support, ongoing support)
-the line (degree of desire to change)
-the box (pros and cons)
Dynamic range (4)
-usable range of hearing
-normal hearing at 95 dB range
-difference in dB between threshold and discomfort
pure tones
speech
-challenge to address in people with HL due to smaller dynamic range, increased threshold and reduced tolerance for loud sounds
Time of HA fitting in children (3)
Best practice:
1/3/6 EHDI recommendation (1 month-all children screened, 3 months-all HL identified, 6 months-intervention)
promotes optimal opportunity for S/L development
Reality:
average age of HA fit is 9.2 months
Time of HA fitting in adults (2)
Best practice:
as soon as significant HL is identified
Reality:
Delay of up to 8.9 years until HA uptake after HL identified
Components of HAs (4)
-Microphone (converts sound from acoustic to electric)
-Amplifier
-Receiver or speaker
-Battery or power supply
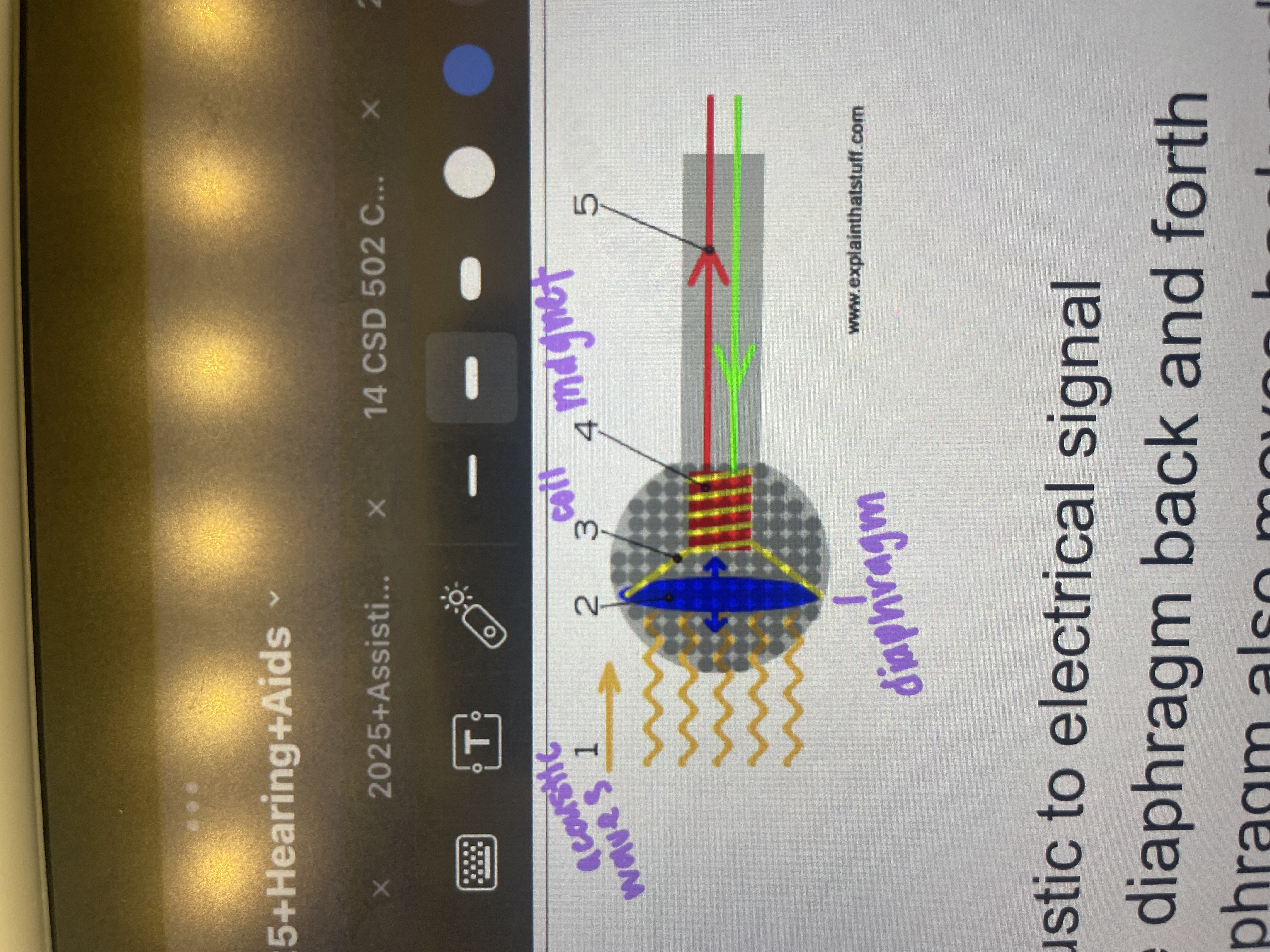
Microphone of HA (5)
-Transducer
converts from acoustic to electrical signal
-Sound waves move diaphragm back and forth
-Coil attached to diaphragm also moves back and forth
-coil wrapped at magnet
oscillating coil over magnet creates current
-Electrical signal sent to amplifier
Amplifier of HA (2)
-electronic device that increases the amplitude of the voltage (current) of signal
-generates a larger current electrical signal
Receiver of HA (2)
-Converts electrical signal (from amplifier) to acoustic signal
-Considered a small loudspeaker
Delivers signal through tubing or earmold
Battery of HA (3)
-+/- proper insertion
-Battery life
3-22 days depending on HA type, battery, HA use
Rule of thumb- larger batteries last longer
-Minimize battery drain by putting tab bag on or opening battery door when not in use
How do HA’s work?
microphone picks up acoustic signal and transduces to electrical
amplifier makes it louder and manipulates signal
receiver transduces electrical signal to acoustic and send to ear
Bone conduction aid and candidates (3)
-bypasses outer and middle ear
-delivers sound via vibration through mastoid
-candidate:
CHL
People who can’t use traditional HAs
People with drainage
no external ear (microtia/anotia)
Body aid and candidates (6)
-cord connects case to earmold worn in the ear
-worn inside a pocket
-powerful HA/low feedback
-easy to adjust controls
-AA batteries
-Candidate:
kids with severe-profound HL
Standard behind the ear (BTE) and candidates (5)
-larger controls
-2 components: unit and HA
-Can be used with assistive listening devices
-less feedback, easy to clean, fewer repaired
-Candidate:
mostly children or adults that prefer style
typically more severe-profound HL
simple dexterity
Open fit/RITE/RIC and candidates (4)
-very small BTE (less power)
-Thin plastic tubing runs from HA to ear dome
Clear tubing - open FIT
Wire inside tubing - RITE/RIC
-No earmold required (have dome)
-Candidate:
mild-moderate HL
In-the-ear (ITE) and in-the-canal (ITC) and candidates (3)
-all components housed in 1 unit
-enhanced amplification of high frequencies
-candidates:
mild-moderate HL
people who don’t want 2 pieces of HA
easiest to manipulate except for nylon thread
Completely-in-canal (CIC) and candidates (6)
-cosmetically appealing and easy to insert/remove
-reduction of occlusion effect (when ear is plugged, hear themselves louder) and feedback (HA squeals)
-sound localization improvement
-less gain needed
-Elimination of wind noise
-Candidate:
need manual dexterity to take in and out of ear
no huge fingers
mild-moderate HL
Over the counter HAs and candidates (4)
-mostly for mild (to moderate) perceived hearing loss
-do not require consultation with audiologist or other hearing health care provider
-self fit
Cost: $300-500
HA Gain (3)
-concept:
the amount of amplification a HA provides when conversational sounds enter the HA
greater the HL, the greater the gain needed from a HA. the gain in a HA can be adjusted
-affects on person with HL:
if there is too little gain, person may not perceive benefit from HL. if the gain is too high, persons may reject HA
Causes of feedback (5)
-earmold or dome fit
-wax
-internal feedback (problem with HA itself)
-External microphone covered
-Anatomically small ear canals
Real ear measurement (8)
-objective measure
tube inserted in ear canal near eardrum
HA placed on top of ear
-measures sound pressure levels near eardrum
determine if HA is delivering target gain
-not always performed-15%-20%
ask families is this was performed
really important for children! (important for speech and language. Child can’t always vocalize quality of sound)
Frequency response (2)
-Concept:
filters used to emphasize high vs low frequency HL so that it matches the shape of the audiogram. Frequency response can be adjusted
-Affects for people with HL:
if a person has a HF HL and has low frequencies included in the signal (meaning they are not filtered out), they will most likely not like the sound of the HA and could even reject it
Output limiting (6)
-Concept:
the maximum output of a HA when a loud sound enters the HA (90dB) and the volume is turned all the way up. Output can be adjusted
prevents signal from becoming to loud for persons with reduced dynamic range
addresses problems of recruitment (sounds being abnormally loud for people with SNHL) due to a reduced dynamic range
limits maximum power output (MPO)
-Affects for person with HL:
If a sound from a HA exceeds the person’s tolerance for sound, then the sound will be uncomfortable, potentially damaging and may result in a person rejecting the HA.
Concept of limited dynamic range among SNHL relates to this HA electroacoustic property
electroacoustic properties of HAs (4)
-output level (SPL)
-gain
-frequency range
-distortion
Distortion (2)
-Concept:
HAs can distort sound when amplified, but the total distortion should not exceed 4%
-Affect for people with HL:
if there is too much distortion, the individual user will complain that the HA is noisy and will not want to wear
Microphone on CI (2)
-picks up sound from environment
-Mic converts acoustic sound to an electrical signal and sends to speech processor
Speech processor on CI (4)
-Unit receives electrical signal from microphone and arranges the speech signal into a code
-Analyzes the speech signal into its frequency components of speech (high, mid, low) using band pass filtering concepts.
-sound is also being compressed here based on individual need.
-The amount of current is controlled by the program developed based on the T (threshold) and C (comfort) level responses from individual user
Transmitter on CI (3)
-coil and magnet
-unit receives the coded electrical signal from the speech processor
-sends the signal across the skin via radio frequency waves and magnet holds the coil in place
Receiver/stimulator/electrode array on CI (4)
-receives the coded electrical signal from the transmitter and sends signal to the electrode array in the cochlea
-electrode is implanted through the RW alongside the basilar membrane
-Electrical signals are allocated to each electrode based on their place in the cochlea. High freq sounds get allocated to the basal end of the cochlea, low freq sounds get allocated to the apical end
-nerve fibers get stimulated based on which electrode is activated
Why use HAT? (3)
-hearing aids are not enough
-they can help people hear better in many situations
-legislation mandates HAT in public facilities and schools
Where are HATs useful? (3)
-in noise
-distance
-reverberation
inverse square law
lose 6 dB of direct sound for each doubling of distance
Frequency modulation (FM) (7)
-enables HAs to wirelessly connect with external microphone, to improve speech signal for listener
-Uses radio waves
allocated stations for education
-transmitter
a radio station
-receiver
a radio
-individual or group (sound field amplification systems)
-FM boot
-cochlear implants
Advantages for FM (6)
-very portable
-very easy to set up and use
-offers great flexibility of movement (up to 300 feet)
-used indoors or outdoors
-appropriate for mild to profound losses
-no fluctuation in strength of signal
Disadvantages of FM (5)
-receivers are required for everyone
-receivers vary in quality and durability
-potential for outside interference
-receivers and transmitters must be on the same channel
-must be 1 free channel between systems used in close proximity
T/F: you can leave the room and still hear the presentation
True
T/F: this system can be used indoors or outdoors
True
T/F: you must have a receiver to use this system
True
T/F: you must have a hearing aid to use this system
True kind of since there are groups
T/F: you can use FM in multiple rooms in a building
True
T/F: I can use my FM receiver with your FM transmitter
False
Bluetooth (4)
-uses short range wireless technology (10 meters)
not suitable for long-range listening venues
-enables HAs to wirelessly connect with cells, TVs, computer, tablets, HA’s and CIs, or remote microphones
-very high-freq radio waves to transmit data
-creates a binaural signal in HA or CI
Remote mics (3)
-wireless system designed to help individuals hear and understand speech in noisy situations and over distances
-some RMs work together with HAs, while others are designed for those with some normal hearing
-Parts:
transmitter-includes microphone
receiver
universal
integrated
stand alone
Hard wired HAT device pros and cons (3)
-Pocket talker
-Pros:
low cost
flexible uses
easy to use
good for clinical setting or nursing home to deliver information
-Cons:
generic amplification
wired, not wireless
unable to hear other in a big conversation
Cochlear implants (3)
-electronic device that can provide a sense of sound to a person who is profoundly deaf or severely hard of hearing.
-Bypasses a nonfunctional inner ear and stimulates nerve with electrical current
-implant is surgically placed under the skin behind the ear
CI eligibility for adults (3)
-18 years of age or older
-moderate to profound SNHL in both ears
-limited benefit from amplification defined by preoperative test scores of <50% sentence recognition in the ear to be implanted and <60% in the opposite ear or binaurally with HAs
CI eligibility for children (2-17) (3)
-severe to profound SNHL in both ears
-limited benefit from binaural amplification
-speech perception tests <30%
CI eligibility for children (9-24 months)
-profound SNHL in both ears
-no medical contraindications
-limited benefit from binaural amplification after HA trial and with monitoring auditory milestones
Components of CI (8)
-microphone
-transmitter
-external magnet
-speech processor
-receiving antenna
-internal magnet
-receiver
-electrode array
How a CI works (3)
sound picked up with a microphone
sound processed through band-pass filters (sorts sound based on frequency)
Signal sent to corresponding area on cochlea (basil-high frequency, or apex-low frequency)
Pre-surgery for CI (2)
-comprehensive audiometric testing
-determining candidacy
multidisciplinary approach
decision making
fully informing patients/families
surgery for CI (5)
-3 hour procedure
-approval from 3rd party payer
-scalp shaved
mastoidectomy apporach
-Chochleostomy
electrode insertion into scala tympani
-intraoperative monitoring by audiologist
test integrity of electrode once in place
Post-surgery for CI (4)
-hook-up
mapping
-follow-up schedule
re-mapping
-therapy
-education
Possible complication of CI surgery (9)
-bleeding
-infection
-meningitis
-facial paralysis
-tinnitus, vertigo
-ear numbness
-device failure
-migration
-older devices-magnet has to be surgically removed prior to any MRI procedure
Hook-up process for CIs (6)
-3-4 week process
-mapping
process of programming the CI (external units)
establish electrical threshold current levels for each electrode (T)
establish loudness tolerance-maximum electrical comfort levels (C)
dynamic range
difference between T and C levels for all channels
recommended maps for children, adjust for the specific individual
Band-pass filtering concept with CIs (2)
-low pass and low frequencies are delivered to the apex end of the cochlea
-high pass and high frequencies are delivered to the basil end of the cochlea
Time factors that affect the outcome of CIs in children (2)
-age at time of implant
-pre-implant duration of deafness
Hearing factors that affect the outcome of CIs in children (2)
-auditory skills/hearing prior to implant
-appropriate programming
brain factors that affect the outcome of CIs in children (4)
-neuroplasticity
-medical radiological
-cognitive ability
-consistency of use
Therapy factors that affect the outcome of CIs in children (2)
-mode of communication
-quality of educational and habilitative environment
Other factors that affect the outcome of CIs in children (3)
-family and vocational support
-additional special needs
-maternal education
Time factors that affect the outcome of Cis for adults (2)
-age at time of implant
-older adult vs younger adult
Hearing factors that affect the outcome of Cis for adults (4)
-pre vs. post lingual
-etiology of HL
-residual hearing prior to implant
-appropriate programming of device
Brain factors that affect the outcome of Cis for adults (4)
-neuroplasticity
-medical radiological
-cognitive ability
-consistency of use
Therapy factors that affect the outcome of Cis for adults
access to rehabilitation services
Other factors that affect the outcome of Cis for adults (2)
-family and vocational support
-additional special needs
General expected outcomes for children (3)
-listening time
full time use by 3 months
-changes in vocalization
perception of changes in voice by 3 months
-alerts to name
25% of the time by 3 months
50% by 6 months
Concept of an imperfect signal generated by the CI (4)
-the sound produced by the CI is an electronic digitized signal that is interpretable by the brain but has limitations
-The CI uses a series of band pass filters to deliver frequency to different places along the cochlea (high freq-basal area, mid freq-middle area, and low freq-aplical area). this means that a band pass filter passes frequencies within certain ranges and rejects or attenuates others outside a specified frequency range. therefore each bandpass filter represents multiple frequencies and not just one
-there are a limited number of electrodes that can be safely activated within the small space of the organ of corti; totaling up to 22 electrodes. One electrode will receive coded information from a bandpass filter (high pass, mid pass, or low pass). This means that there is not a 1:1 correspondence between one electrode and one frequency, but rather one electrode will be stimulated by multiple different frequencies
-The combination of an artificial, digitized signal, that is band pass filtered and then sent to a fixed number of electrodes results in an adequate but less than perfect signal for a CI user to interpret