Equine Reproduction and Neonatal Care
1/36
Earn XP
Description and Tags
Flashcards covering vocabulary from a lecture on Equine Reproduction and Neonatal Care
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
37 Terms
Equine Reproduction
To produce a live foal, successful breeding, conception, implantation, gestation, parturition, and survival of the neonatal period must occur.
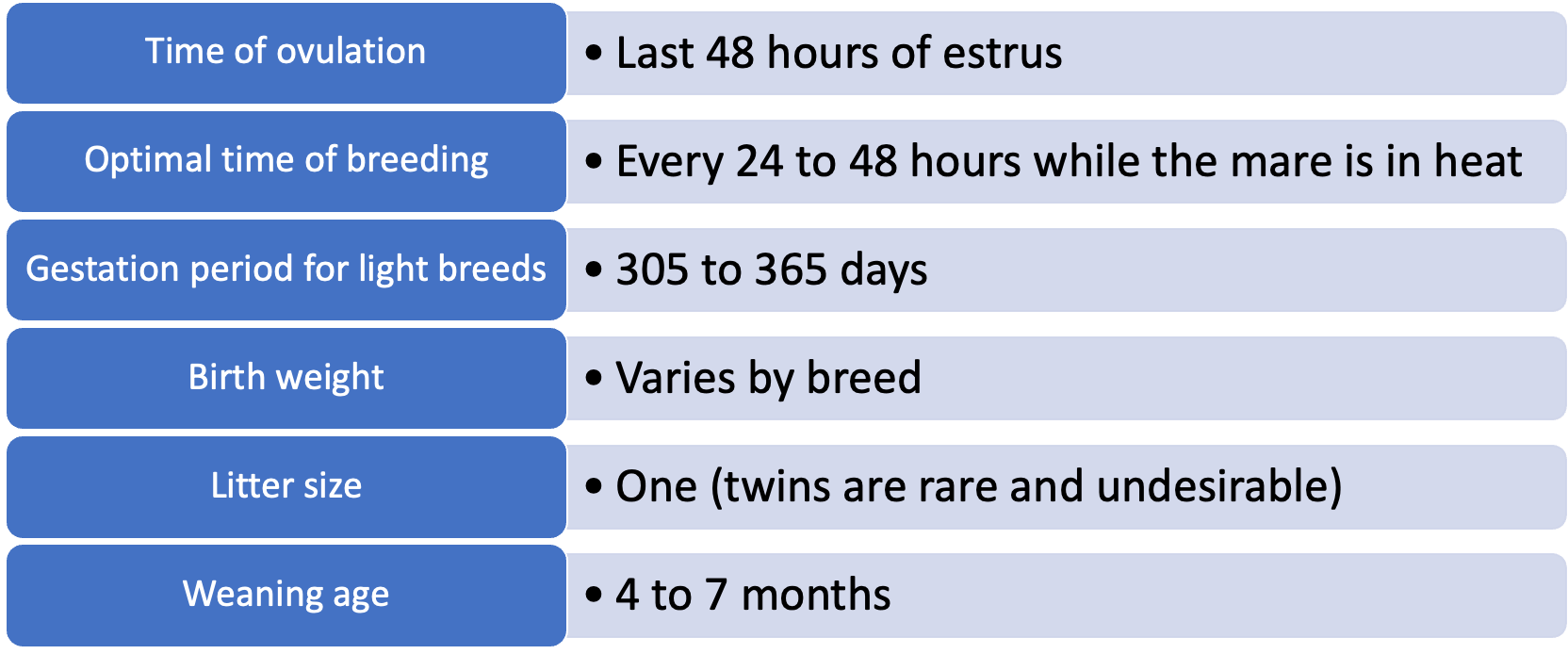
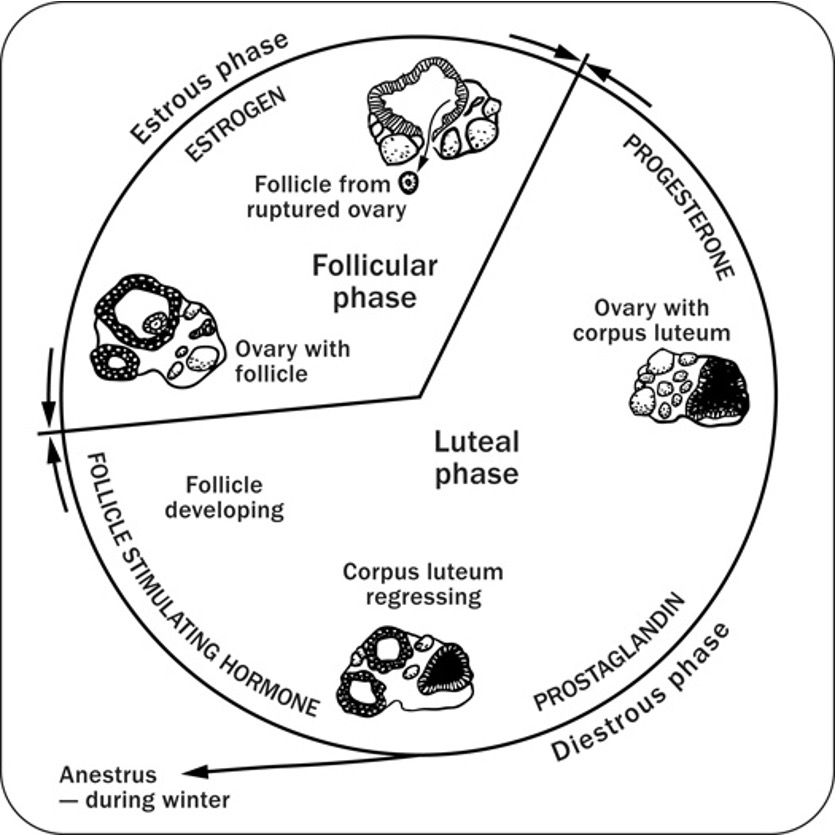
Type of equine estrus cycle
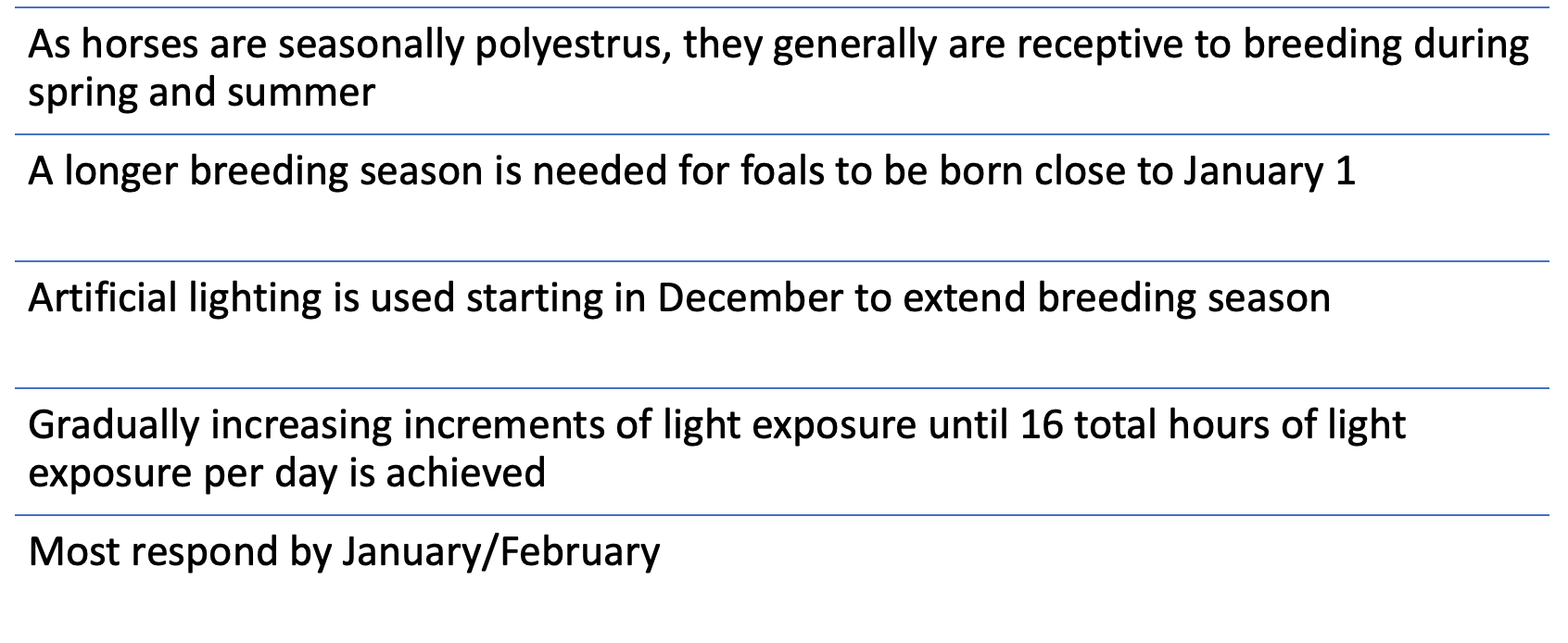
seasonally polyesterous
Female and male horses reach puberty at
10 - 24 months
Frequency of equine estrus
15 - 26 days
duration of equine estrus
2-12 days (average 5-7)
Equine Breeding Data
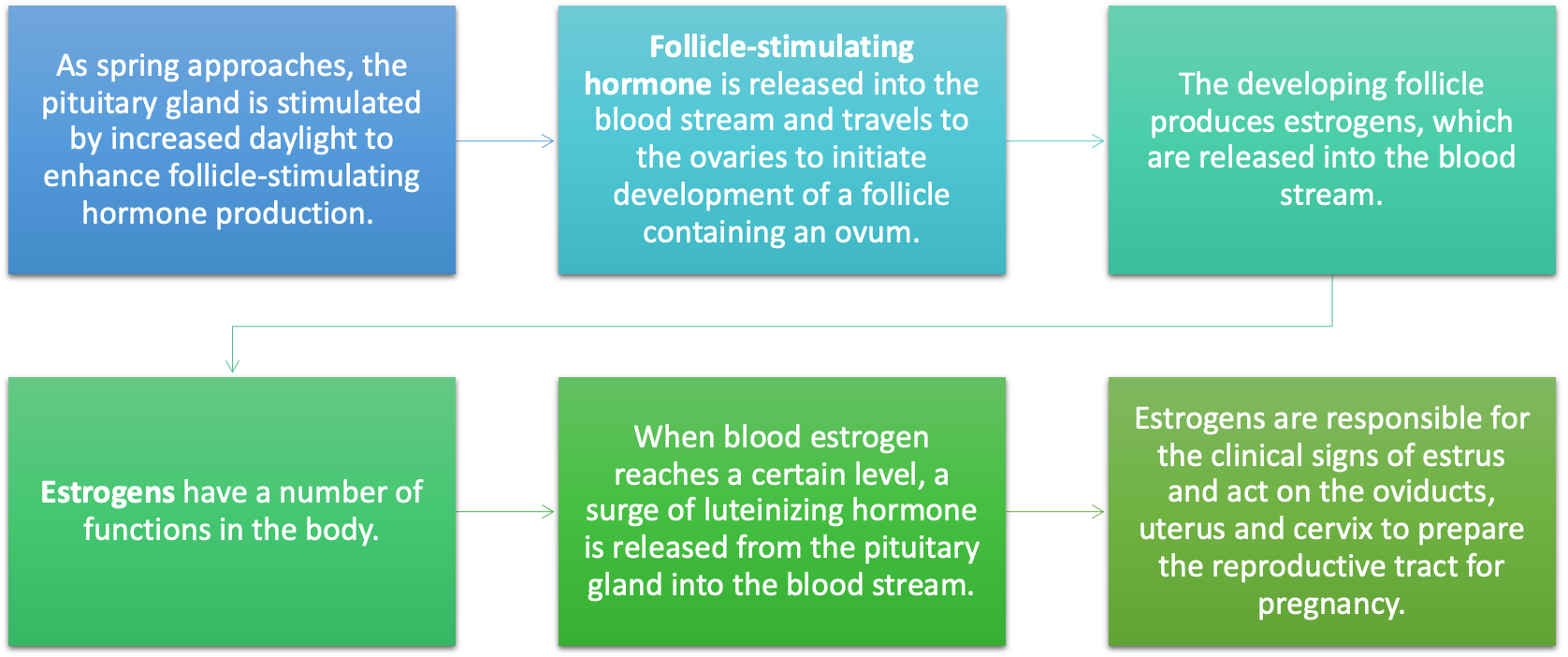
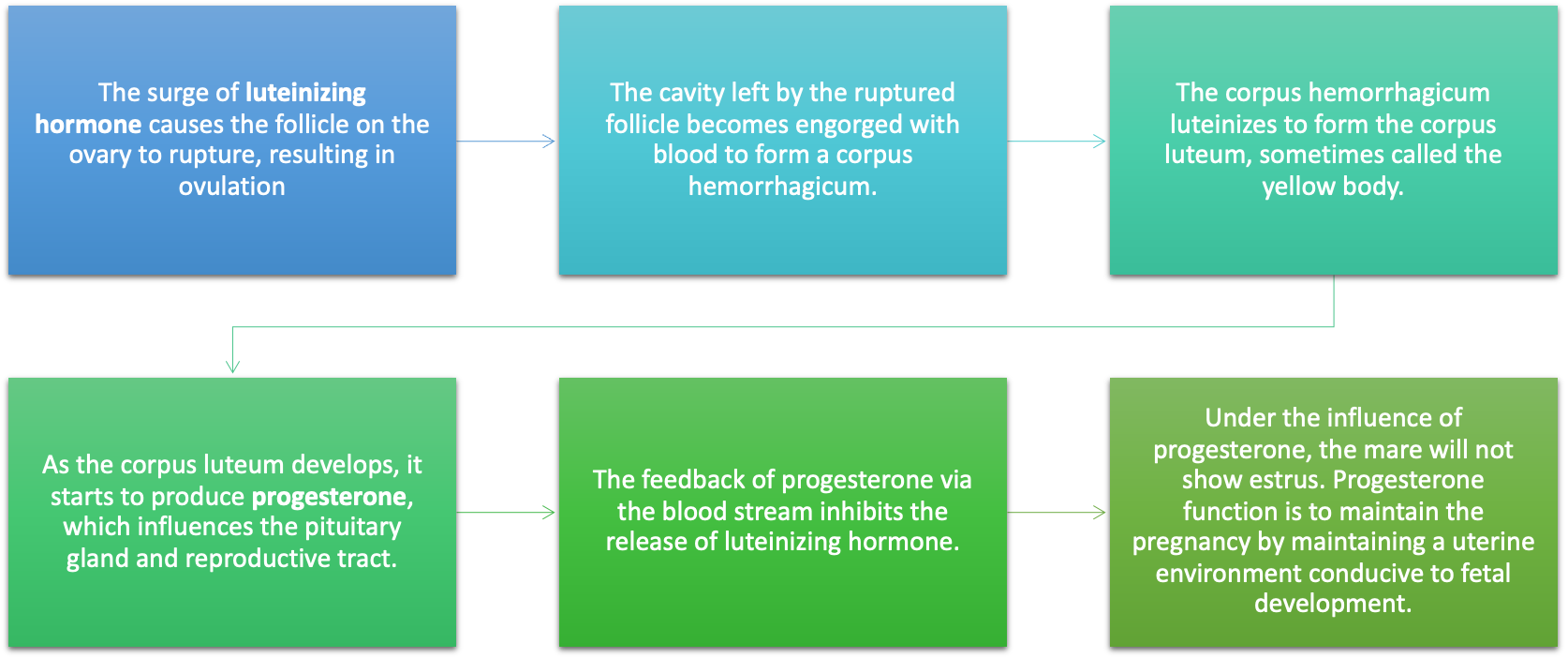
Luteinizing Hormone
Hormone that causes the follicle on the ovary to rupture, resulting in ovulation.
Corpus Luteum
Forms from the cavity left by the ruptured follicle and produces progesterone, maintaining a uterine environment conducive to fetal development.
Female Reproductive Examination
Rectal palpation (less accurate as early follicles are inside the ovary) or Ultrasound (US)
Ovaries, uterus, and cervix
US can be much more accurate for the estrous cycle, diagnosing pregnancy, twins, and fetal sexing
Female Reproductive Examination
Visual exam
Vulva; vagina and cervix (need speculum and light)
Female Reproductive Examination
Uterine Culture
Most common reason for infertility in mares is a bacterial infection of the uterus and these infections are usually “silent”
Female Reproductive Examination
Endometrial biopsy
able to assess the probability mare can support a pregnancy
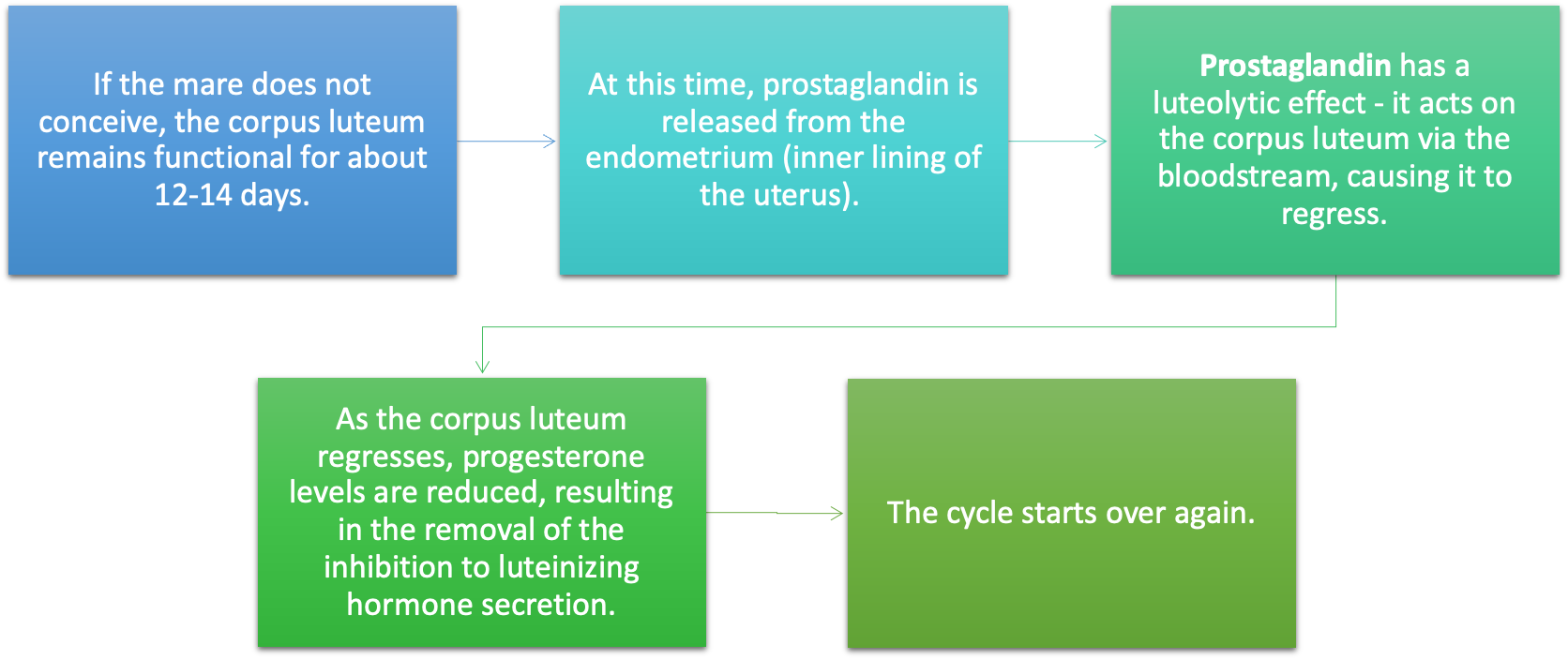
Prostaglandin
Hormone released from the endometrium that causes the corpus luteum to regress if the mare does not conceive.
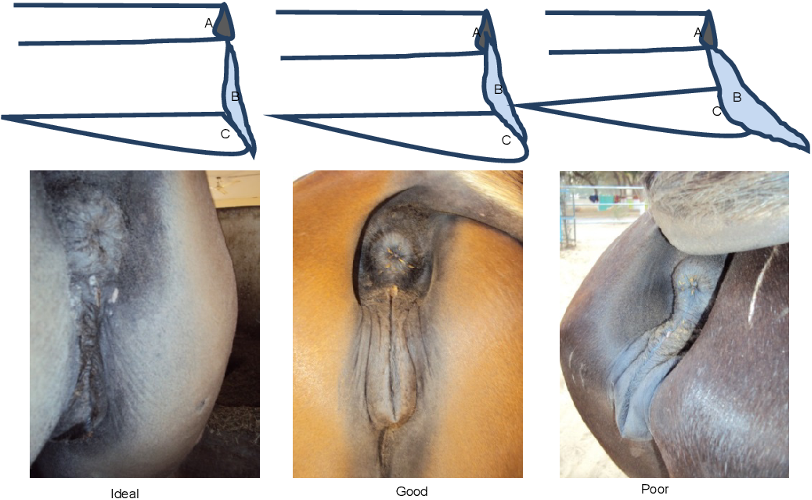
Windsucker
in mares and fillies is a condition that is only visible in the female gender, where the air gets sucked into the vagina due to the vulva lips not sealing the entrance of the vagina properly.
Poor conformation also makes horses more prone to infections due to fecal matter dropping on labial folds
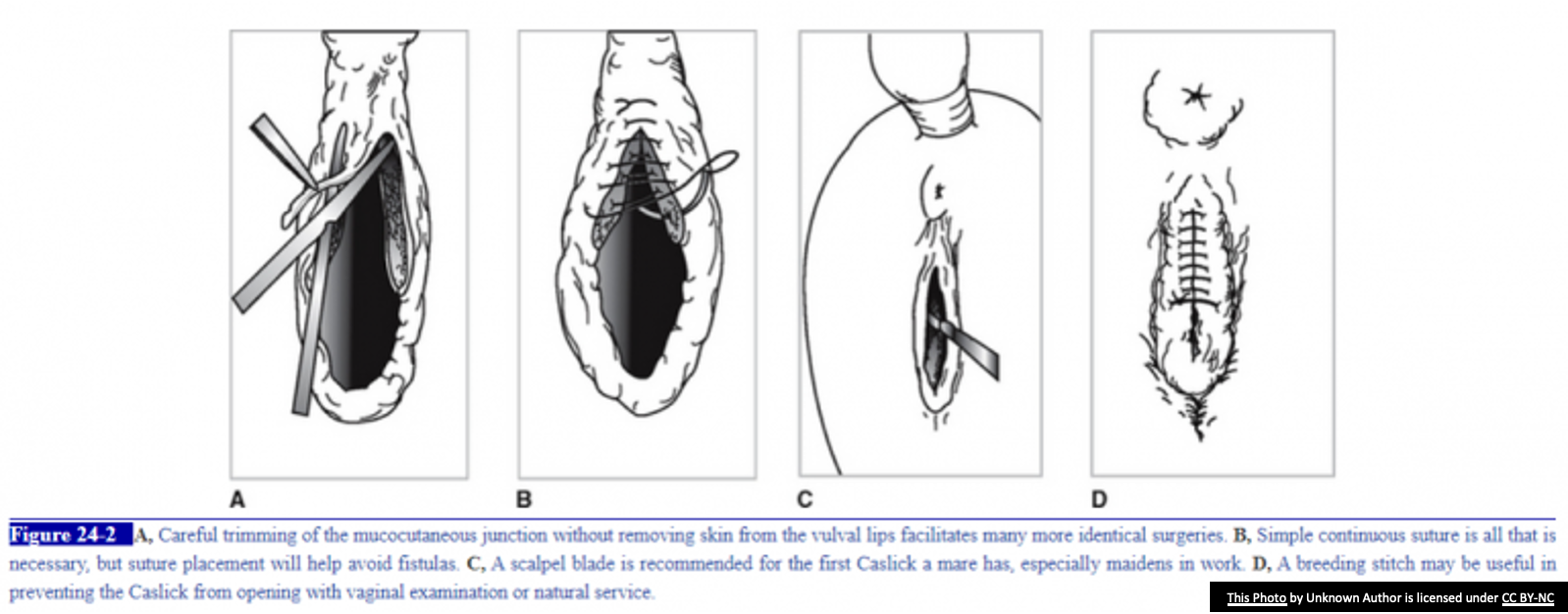
Surgical correction using Caslick procedure
Caslick's Procedure
Procedure where the dorsal 2/3 of the vulva are sutured closed to prevent wind-sucking in mares.
Must be removed during breeding or prior to parturition
Clinical Signs of Impending Parturition in Mares
Swelling of the vulva and possible discharge, udder enlargement, waxing of teats, and changes in rectal temperature.
Edema of the legs; plaque of edema ventral abdomen (not helpful for prediction of time of foaling)
Udder enlarges 2-4 weeks before foaling
Waxing of teats 24-48 hours before foaling, not all mares wax
Vulva swells with possible discharge
Rectal temperature – if nighttime temperature is not higher than morning temperature, foaling MAY occur within 36 hours
Calcium level in mammary secretions can be tested; test kits available; under 400ppm unlikely to foal; over that usually foal within 48 hours; or within another 48 hours after
Stage 1 of Parturition
Preparatory Stage
Lasts 2-4 hours
Restlessness, pacing, sweating-particularly neck, shoulders and flank
Disinterest in food
Stage 2 of Parturition
Delivery of the foal
Lasts 20-30 minutes
Begins with “water breaking” (8-20 Liters of fluid)
Fetus delivered in “head-dive” position
Stage 3 of Parturition
Should occur within 2-4 hours
Placenta passes
If not within 4-6 hours, considered retained and need to contact veterinarian
Dystocia
Incidence is low compared with other large domestic species
When it does occur, consequences often disastrous, and a live foal is not often achieved
Most common cause is fetal malposition
If a foal is not delivered within 20-30 minutes of water breaking, contact veterinarian – Considered an EMERGENCY
Dystocia treated: Mutation (manual reposition fetus)/traction, Fetotomy, C-section
C-section has high complication rate and is generally last resort
Essential Aspects of Neonatal Foal Care
First 4-5 days of life
2% of all foals born alive do not survive past 48 hours
Once delivery has occurred, the following needs must be addressed:
Oxygenation/pulse assessment
Temperature regulation
Care of the umbilical cord and umbilicus
Nutrition and nursing
Bonding of mare and foal
Passage of meconium
Adequacy of passive transfer of antibodies
Oxygenation
Clear away nostrils
Foal placed sternal with head/neck extended, body rubbed vigorously
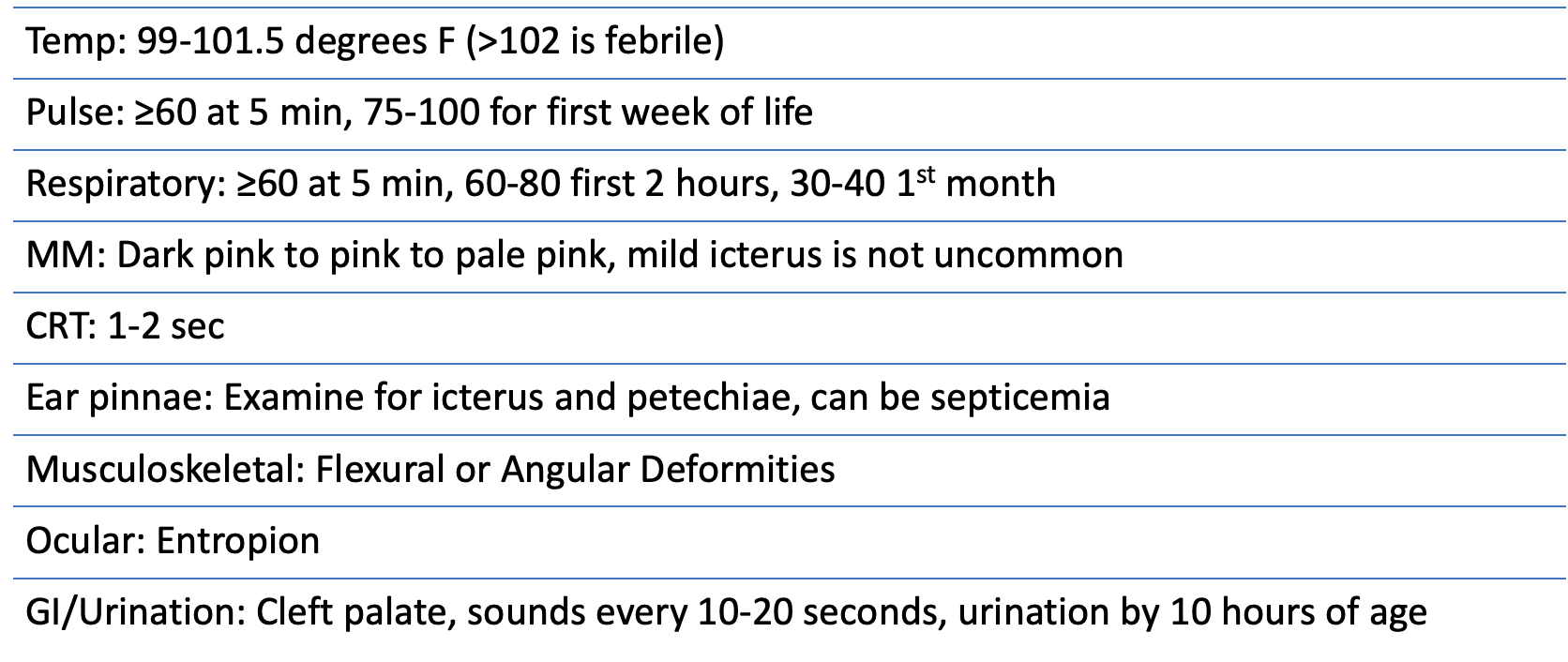
RR at least 60 bpm at 5 min after delivery, staying around 60-80 bpm first hour, then decline to 30-40 bpm for first few weeks of life
If not breathing after 1 minute, resuscitation can be done
Close one nostril and breathe into the other, watch for chest rise, and open both nostrils for exhale
Continue rate 20-30 per minute
Can insert a nasotracheal tube through one nostril, inflate the cuff, and ventilate with Ambu-bag
Pulse Assessment
Should be at least 60 bpm at 5 minutes after birth
Usually elevates >100 bpm over first hour, then declines to 75-100 bpm first week of life
If the pulse rate or respiratory rate is less than 60 per minute at 5 minutes after birth, contact veterinarian immediately
Temperature Regulation: temp ranges between 99-101.5
Drying the foal is the first step in warming the body
Deep bedding and prevent drafts
Heat lamps (no closer than 4 feet), warm water pads or bottles, and blankets can be used
Care of Umbilical Cord and Umbilicus
Should not be cut unless necessary, usually breaks naturally when mare stands
Do not apply traction on cord
Umbilical stump should be dipped in 2% chlorhexidine solution 2-3 times a day for first week
Nutrition/nursing
Should be standing and nursing within 60-180 minutes (2 hours average)
Foals nurse every 1-2 hours (often more frequently)
Death may occur in foals with blood glucose level less than 40 mg/dL
Bonding of mare and foal
Allow them to spend most of their time with little interference
Imprinting can be done in gentle manner with mare always present and close as possible
Passage of Meconium
Meconium is from the fetus swallowing amniotic fluid
Can be hard and difficult to pass and cause straining (tenesmus)
Common practice to give warm water or human pediatric fleet enema
Most pass in first 9-12 hours of life
If not seen by 24 hours, or if colic behaviors seen, contact vet
Adequacy of Passive Transfer of Antibodies
Should receive within first 12 hours (best absorbed first 6 hours)
Test kits available to check immunoglobulin G levels of foal
Physical Exam of the Neonatal Foal
Limb deformities
Club foot
Valgus deformity
Flexor Tendon Laxity
Varus deformity

Neonatal Diseases
High risk foals
Mares with illness during pregnancy
Dystocia
Lactation issues with mare
Premature or dysmature foal
Twin foal
Orphaned or rejected foal
Failure of Passive Transfer
C-section delivery
Dummy Foal (Neonatal Maladjustment Syndrome)
Term for foals with behavioral and neurological abnormalities not attributable to other disorders.
Have difficulty standing or are unable to stand
Have opisthotonus (severe flexion of the body)
May be blind and disoriented
Suffer seizures
May be stuporous
Some are mild cases and are much more difficult to diagnose
SCID Foals (Severe Combined Immunodeficiency)
Genetic condition in Arabian horses where foals cannot produce functioning T-cell and B-cell lymphocytes.
Seen in Arabian and part-Arabian horses
Inherited as an autosomal recessive mutation
Unable to produce functioning T-cell and B-cell lymphocytes
Illness begins to be apparent as maternal antibodies decrease (around 2 months)
Usually foals die by 5 months of age
DNA test available for breeders as two carriers have a 25% chance of producing a SCID foal
Arabian Horse Association Code of Ethics requires disclosure of known carriers