Test 1
1/333
Earn XP
Description and Tags
Chapter 17-20
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
334 Terms
Prefixes and Suffix for Blood
Prefixes
“heme-”
“hemo-”
Suffix
“-emia”
Functions of blood
Transport
Oxygen and nutrient delivery to tissues
Waste removal from tissues
Hormone transport from endocrine organ to target organs
Maintenance
Body temperature
pH
Fluid Volume
Protection
Blood clotting
Infection
Waste products removed by blood
CO2
Nitrogenous Waste
Uric Acid
Urea
How does blood function to maintain body temperature?
Blood is mostly water, water absorbs heat
Moves blood
Closer to skin if hot (heat radiates)
Deeper if cold (less heat lost and preserves vital organs)
Bloods maintenance of fluid volume
effects blood pressure
maintain correct amount of fluid in tissues
Abnormal increase of fluids in tissues = edema
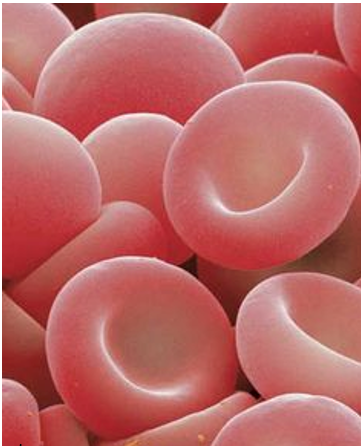
Characteristics of Blood
Scarlet to dark red in color
Can vary due to amount of oxygen
Total amount: 5.25L (in an average 150lb-180lb person)
pH range: 7.35-7.45
Considered neutral range for blood (even though its slightly basic)
Maintained by urinary system and lungs
Viscous due to erythrocytes
Blood is thicker than water

Which drop of blood has more oxygen?
The lighter one on the left
the darker the color the less oxygen

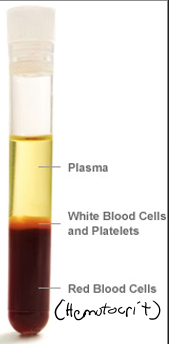
Blood Composition
Blood Plasma
Blood Cells
Erythrocytes (RBC)
Leukocytes (white blood cells)
Thrombocyte (platelets)
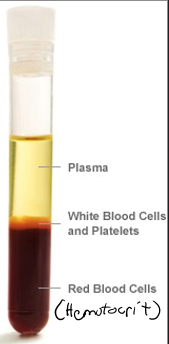
Blood Plasma
Fluid (non-living) portion of blood
When blood is centrifuged, it is the clearish yellow portion
Composition
90% water
6 solutes found in plasma
Electrolytes
Nitrogenous substance (urea, uric acid, etc)
Organic nutrients (glucose, amino acids, triglycerides, etc.)
Respiratory gases
Hormones
Plasma proteins
Every night owl really hates possums
Plasma Proteins
huge compared to other solutes in plasma
make up most of the mass of plasma
Most produced by liver
Several types of plasma proteins
Albumin
Fibrinogen
Globulins
Albumin
specific type of plasma protein
major transport protein of blood and contributes to water content in blood
attracts water
What would happen to water content of the blood plasma if albumin were absent?
decrease in blood volume blood pressure would decrease
cause H2O to leave blood and fallow the high salt concentration into tissues
Fibrinogen
specific type plasma proteins
soluble protein that functions in blood clotting
Globulins
general class of plasma proteins
transport proteins, antibodies (immune defense), etc
What do all blood cells have in common
short-lived
non-mitotic
Types of blood cells
Erythrocytes (red blood cells)
Transports oxygen
False cells: no nucleus therefore no mitosis
Leukocytes (white blood cells)
Protection and defense
Thrombocytes (platelets)
Blood clotting
False cells: no nucleus therefore no mitosis
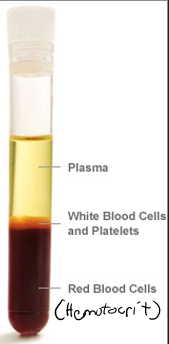
Hematocrit
portion of total blood volume made up by erythrocytes
composition of blood that is only red blood cells
Males ~ 47%
Females ~ 42%
If too low will lead to hypoxia and anemia
Hematopoiesis
production of blood cells (all 3 types) in red bone marrow
All blood cells arise from hematopoietic stem cell (hemocytoblast)
Hematopoietic stem cells eventually become ”committed” to forming a certain type of blood cell
Once committed, the cell cannot become any other cell type
Red marrow produces billions of new blood cells per day!!
Fairly efficient
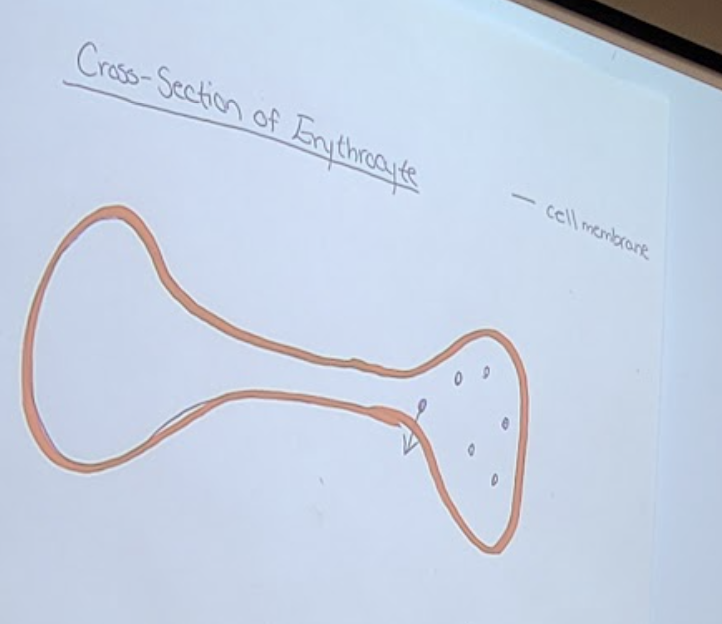
Erythrocytes
RBCs
Blood cell type responsible for respiratory gas transport
Nuclei and most organelles removed during cell development
Increase the open space for hemoglobin to filled
Features that make erythrocytes ideal for gas exchange
Large surface area relative to volume
Oxygen has to cross the membrane
Gives more space for oxygen to cress
Flattened disc-shape
Oxygen closer to the membrane to leave
Anaerobic mechanism of energy production by RBC
RBCs use glycolysis
Do not use any of the oxygen they carry
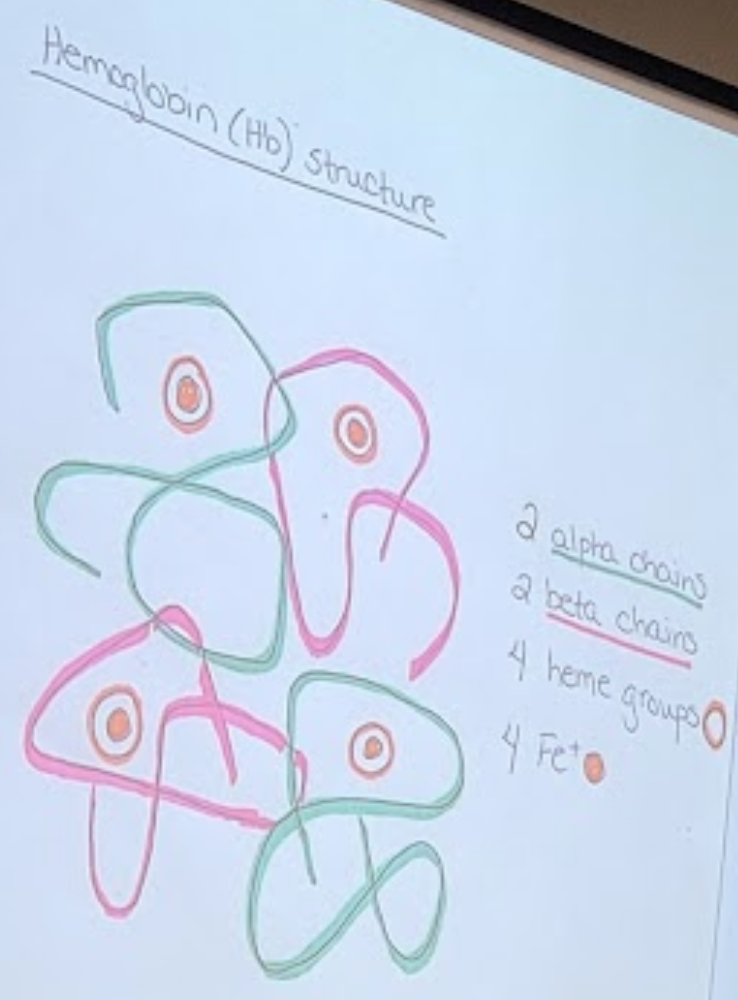
Hemoglobin
Hb
Protein responsible for O2 transport in blood
Is composed of heme pigment bound to globin protein
A globin protein is made up of 2 alpha chains and 2 beta chains
Each chain binds to 1 heme group
Each heme group has Fe+ ion at center
Each Fe+ can bind one molecule O2
1 hemoglobin can bind to 4 oxygen molecules
250 million hemoglobin in 1 RBC = 1 billion oxygen molecules
Bind and breaks free of oxygen very easily allowing easily oxygen transfer to and from tissues
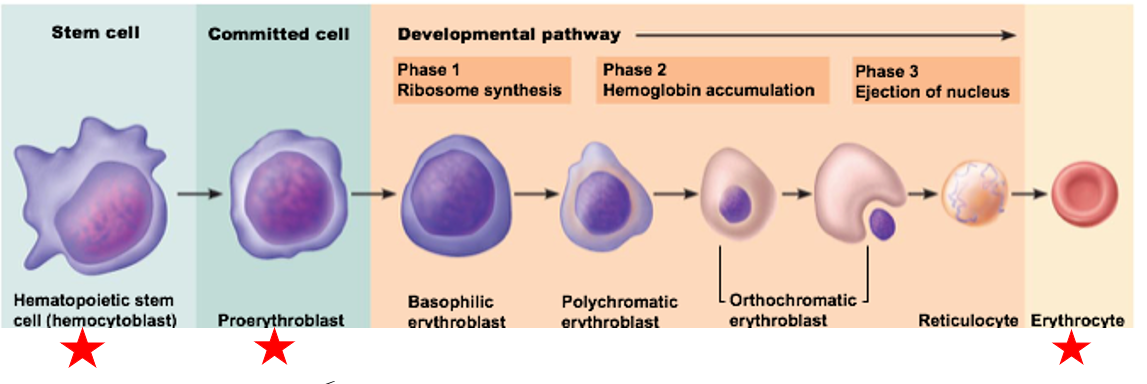
Erythropoiesis
the production of red blood cells
Hematopoietic stem cell “commits” to a proerythroblast
Strictly regulated process
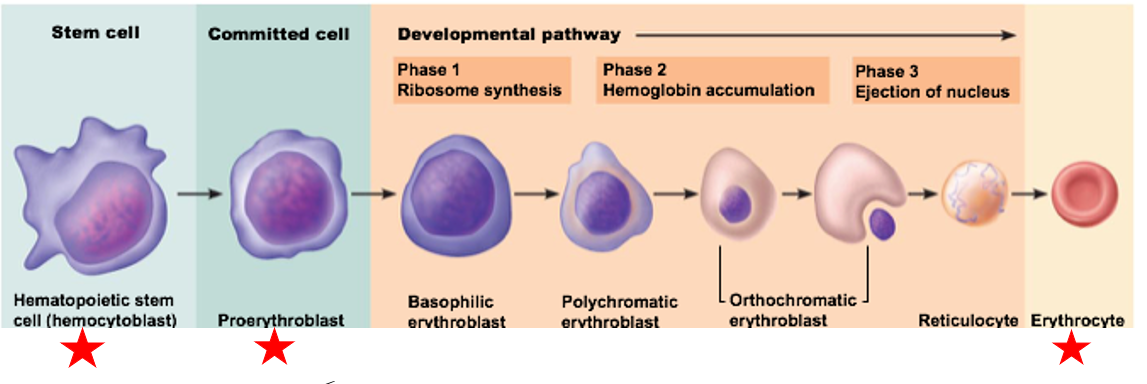
Steps of erythropoiesis
Starts with stem cell (Hematopoietic stem cell/hemocytoblast)
Commits/differentiates (Proerythroblast)
Developmental pathway
Becomes Erythrocyte
has nucleus for a lot of the steps
nucleus directs development and differentiation
kicks out nucleus at end of developmental pathway
How is erythropoiesis controlled
Hormonal control
Erythropoietin
Testosterone
Dietary needs must be met also
Erythropoietin affect on erythropoiesis
EPO
directly stimulates erythrocyte production
produced and released by kidneys
only simulates cells already committed to becoming erythrocytes
small amount almost always present in blood to set basal rate of production
increase of EPO is negative feedback mechanism
excessive oxygen supply suppresses EPO release
Testosterone affect on erythropoiesis
enhances production of EPO
Males generally have more erythrocytes and Hb than females
Helps males be better athletes with more oxygen to expend
Dietary needs for normal erythrocyte production
General nutrients: amino acids, lipids, carbohydrates necessary for cell synthesis
B-complex vitamins: B12 and folic acid
Necessary for normal DNA synthesis
Iron
65% of body’s iron supply is in Hb
Remainder stored in liver, spleen, etc.
“Free” iron bound to protein transferrin—erythrocyte takes up iron as needed
Iron cannot circulate on its own and unbound
Iron is toxic in high amounts
Death of Erythrocytes
Average lifespan: ~120 days
Over time, Hb begins to degenerate & RBC becomes less flexible
Macrophages engulf & destroy cell
Heme group splits free from globin protein
Heme broken down to bilirubin in the liver & excreted to intestines → leaves body in feces
Globin proteins broken down to amino acids & released to circulation
Fe2+ saved for reuse
temporarily bonds to transferrin
Why do RBCs need to be flexible
blood vessels can be very tiny
need to be able to fold in half to fit
if cannot fold are more likely to block blood flow
Bilirubin
substance created by the break down of heme from erythrocytes destroyed by macrophages
produced in liver and excreted to intestines
leaves body in feces, gives the brown color
Homeostatic Imbalances of erythrocytes
anemia
too few erythrocytes
polycythemia
too many erythrocytes
Anemia
insufficient oxygen supply to meet body needs
not really disease or disorder…more a symptom
Symptoms: paleness, cold, short-of-breathe, tired
Causes of Anemia
Blood loss (hemorrhage)
Acute hemorrhagic anemia: severe, swift blood loss (bleeding to death, requires blood transfusion)
Chronic hemorrhagic anemia: slow, persistent blood loss (long term, usually internal)
Ex: ulcer bleeding, hemorrhoids
Inadequate erythrocyte production
iron-deficiency anemia (nutritional origins - usually due to diet)
renal anemia - kidney failure (little/no EPO release)
Excessive erythrocyte destruction/deformation
autoimmune
Ex: sickle-cell anemia
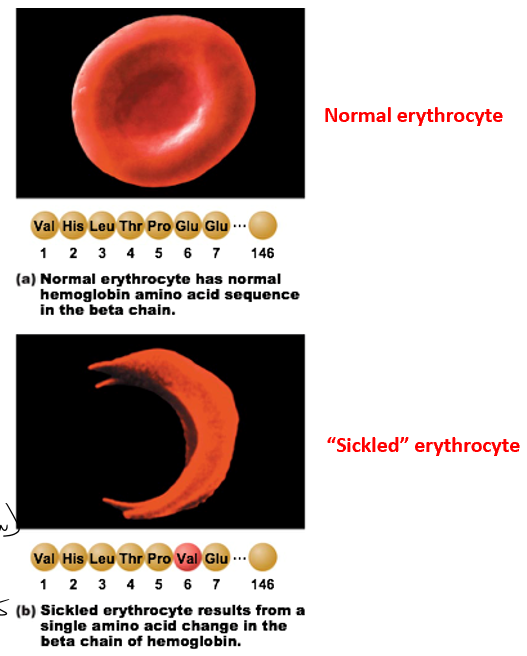
Sickle-cell anemia
erythrocyte deformation
genetic condition
single point mutation
change in confirmation of protein
different shape and less flexible
pulls on cell membrane
Hypoxic condition
Circulation problems
Can hook together
Forming clots
Symptoms: pale, short of breath, pain (not enough blood blow), cold hands and feet
No cure, treat symptoms
Nitroxide
dilate vessels for easier blood flow
Polycythemia
increased number of erythrocytes
blood is thicker
harder to pump → heart works harder
increased blood pressure
increased risk of heart diseases and heart attack
Types
Polycythemia vera
secondary polycythemia
temporary polycythemia - blood doping
Polycythemia vera
hematocrit level ~80% (almost double - blood is practically sludge)
blood volume doubles - vascular system engorges with blood and impairs circulation
effects
increased blood pressure
increased risk of heart attack
increased risk of stroke
increased risk of kidney issues
treatment
therapeutic phlebotomy (routinely get blood drawn/removed)
chemotherapy drugs to kill RBCs
Aspirin
Secondary Polycythemia
Increased EPO release due to low oxygen availability
Caused by: high altitude living, etc.
composition increases to 50% because of less oxygen being available
will take care of itself if individual moves to lower elevation
Temporary Polycythemia - blood doping
Individuals (usually professional athletes) inject synthetic EPO/oxygen carriers or use of blood transfusions
autologous transfusion (from same individual) harder to trace
Risks: stroke, heart failure
Body compensating for blood loss
Body compensates for blood loss 2 ways:
Decreasing blood volume to injured blood vessel(s)
rapid constriction
Increasing red blood cell production by red bone marrow
kidneys stimulated to release increased amounts of erythropoietin
Only for regular scraps and cuts
The body can only compensate so much
Losing 15-30% total blood volume leads to weakness
slow and sluggish and tired
decreased nervous system
30%+ loss leads to severe shock (possibly death ← Hypovolemic shock)
Organs (BRAIN) are not getting oxygen
Blood pressure drops, blood flow slows and eventually stops
Whole blood transfusions are rare
More often, red cell transfusions are used
Blood transfusion
not 1 size fits all
Erythrocytes have very specific extracellular markers called antigens
ABO antigens, Rh antigens, etc. etc.
allows our immune systems to identify our cells as us
more than 20 to 30 types of antigens but most are very rare or benign
Transfusions between two people with different antigens usually cannot occur
Medical field is mostly concerned with ABO Blood groups & Rh Blood groups
generally strongest immune response if mismatched
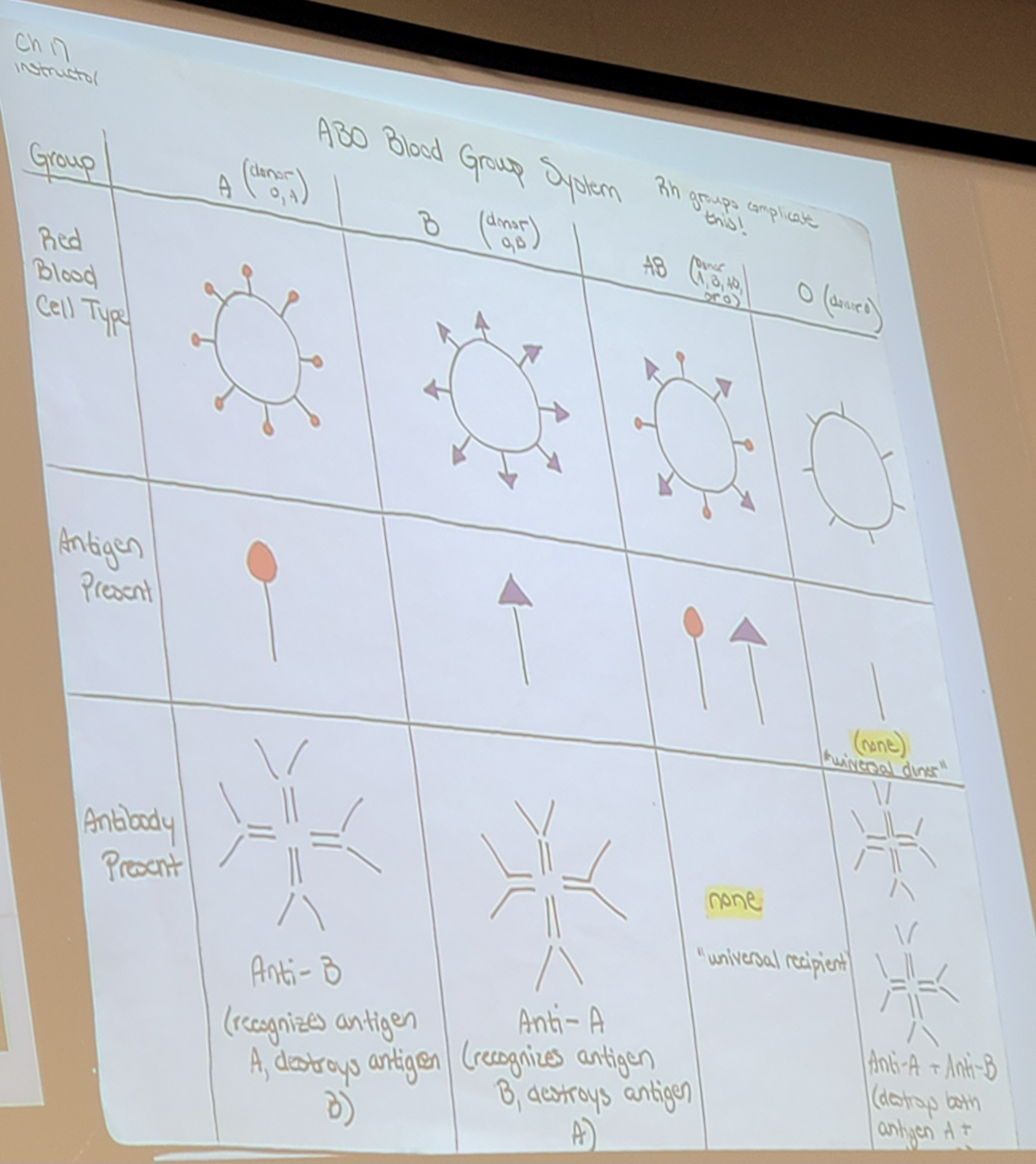
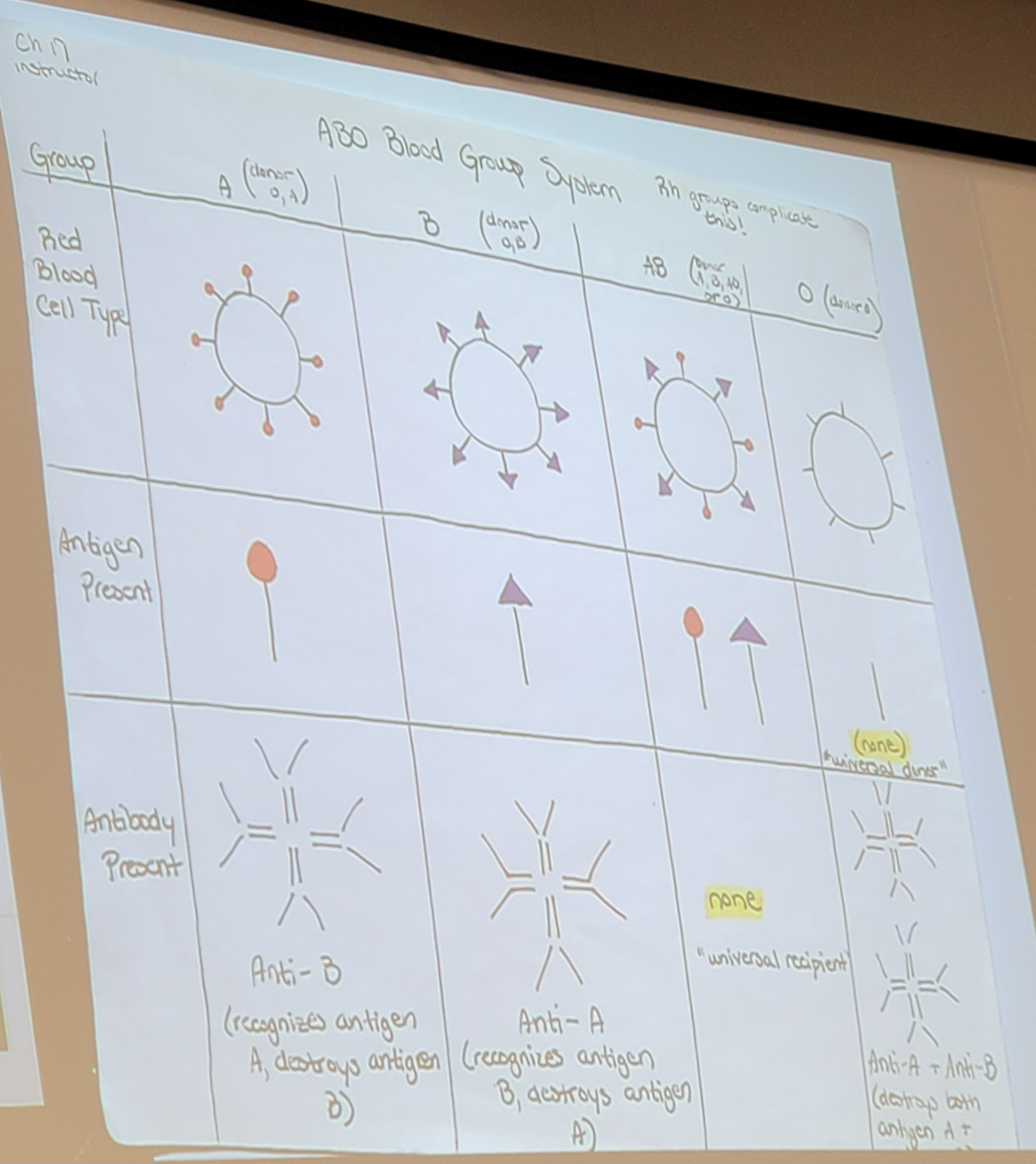
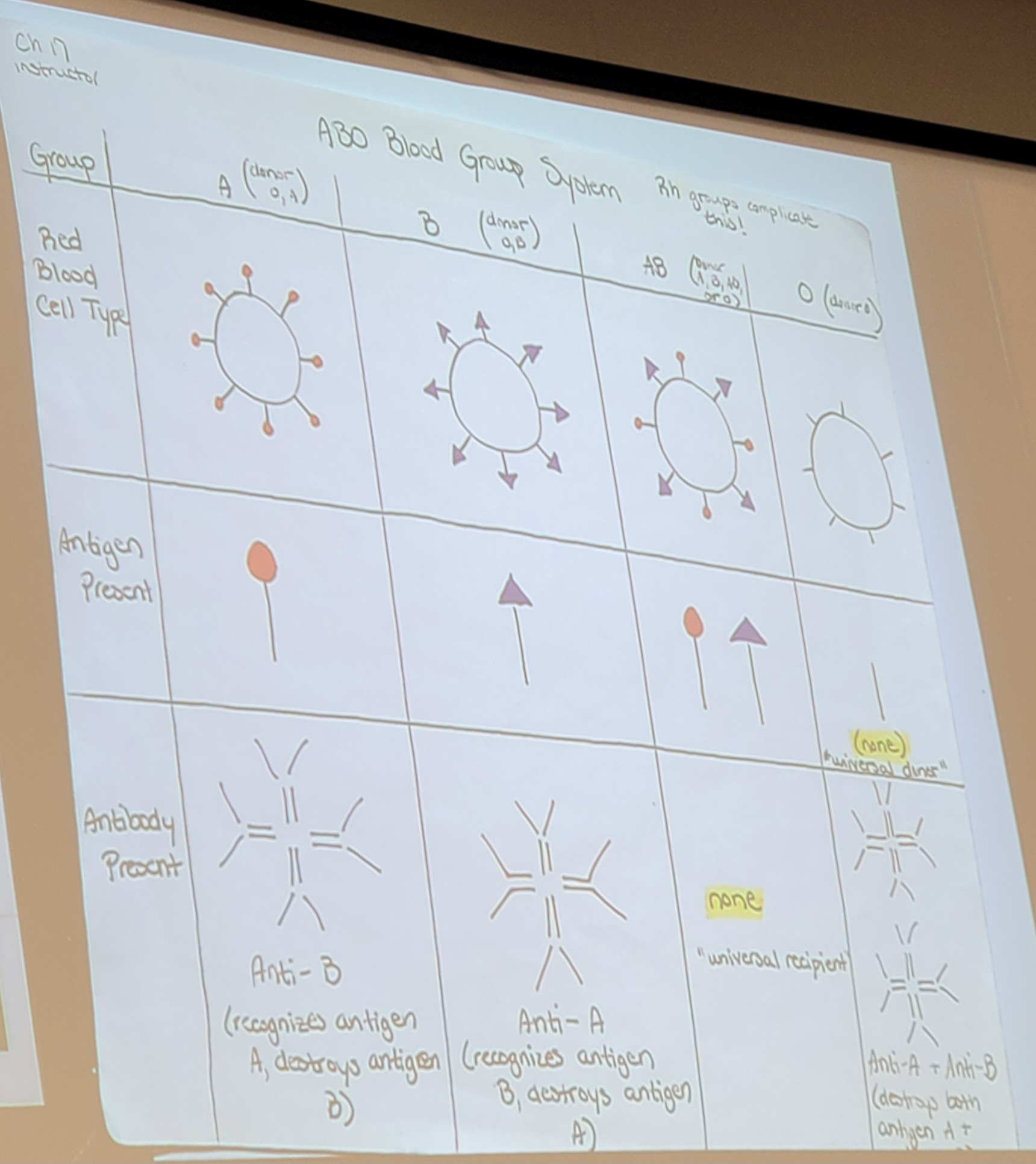
ABO Blood Groups
Blood type A: have “A” antigen
Blood type B: have “B” antigen
Blood type O: do not have any antigen
Blood type AB: have “A” and “B” antigen
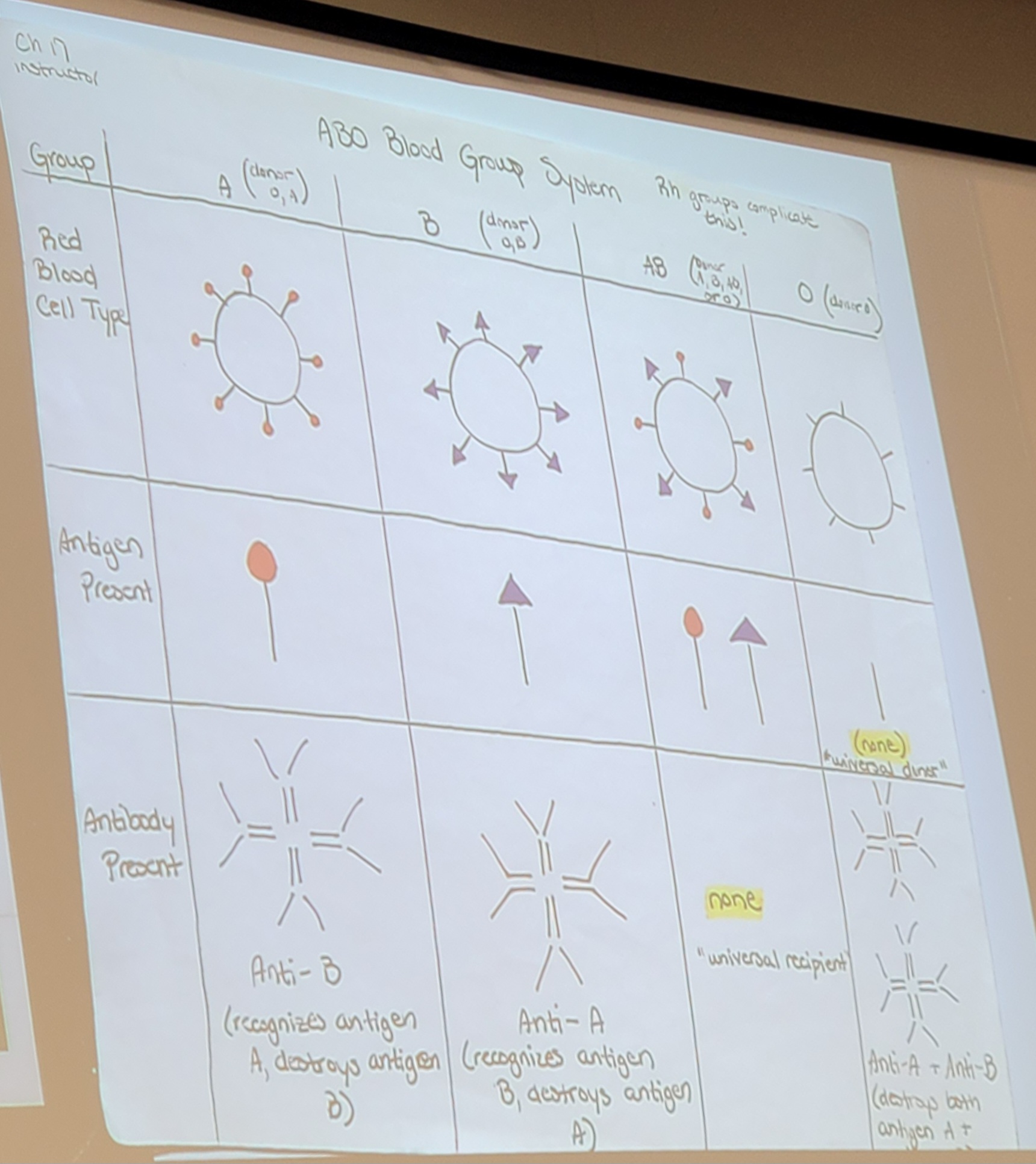
Agglutinins
immune system antibodies that will attack mismatched blood cells
work as red flags
Person with Type A blood has anti-B antibodies
Person with Type B blood has anti-A antibodies
Person with Type AB blood has neither type of antibody
Person with Type O blood has both anti-A and anti-B antibodies
Donation rules
A can receive A, O
B can receive B, O
AB can receive A, B, AB, O
O can receive O
Rh Blood Groups
Five antigens make up this blood group → C, D, E, c, and e
D antigen is Rh+
C, E, c, or e antigen is Rh-
Donation rules
Rh- can only receive Rh-
Rh+ can receive Rh- and Rh+
Blood types are identified as a combination of ABO blood groups and Rh blood groups
Blood acceptance practice
A- ←→ B-
A- ←→ A+
A- ←→ O-
A- ←→ AB-
A- → B-
No: A blood can not be given to anti A
A- ← B-
No: B blood can not be given to anti B
A- → A+
Yes: A blood can be given to anti B, - can be given to +
A- ← A+
No: A blood can be given to anti B but, + cannot be given to -
A- → O-
No: A blood cannot be given to anti A anti B
A- ← O-
Yes: O blood can be given to anti B, - can be given to -
A- → AB-
Yes: A blood can be given to anti none, - can be given to -
A- ← AB-
No: AB blood cannot be given to anti B
Transfusion Reaction
Mismatching blood types can lead to transfusion reaction
Antibodies attack “foreign” donor blood cells (immune system tries to kill what doesn’t belong)
Foreign erythrocytes are clumped together via agglutination → clumps of RBCs will ”clog” blood vessels
like shooting fish in a barrel
“Foreign” blood cells will eventually start to lyse → releases free hemoglobin to blood stream
Results: Free hemoglobin does not bind to oxygen outside of the cell, Decreased oxygen transport & hemoglobin causes damage to kidneys (clogs them)
Type O blood
”universal donor”
O- is the most universal
can donate to anyone
Neither antigen is present on blood cell surface
Most common
Worst receiver, can only receive O
Type AB blood
”universal recipient”
AB+ is the most universal
can receive from anyone
Neither antibody is present
Least common
Worst donor, can only donate to AB
Leukocytes
White blood cells (WBCS)
responsible for defending the body
Characteristics of Leukocytes
Not restricted to the blood vessels (can leave)
Use vessels as transport to various parts of the body
Can leave vessels via capillary walls
Uses blood as highway then squeezes through blood vessel wall straight to the infection or bacteria
This way can get to the problem before it infects the blood
Can be produced very quickly
the number in the body can double within 2-3 hours
Leukopoiesis is very fast
Prevents spread of infection
Average lifespan: 13-20 days
if used, lifespan is even shorter
many die in battle
Categories of leukocytes
granulocytes
agranulocytes
Granulocytes
type of leukocytes
spherical in shape, large, and packed with granules
granules full of different substances
looks grainy under microscope
Types of granulocytes
Neutrophils (bacteria killer)
Eosinophils (parasite killer)
Basophils (have histamines)
Neutrophils
Type of granulocyte
bacteria killer
50-70% of total leukocyte population
Chemically attracted to sites of inflammation - Chemotaxis
granules contain defensins - antimicrobial protein
kill of bacteria by punching holes in membrane
water rushes into the cell, cell swells and burst open
Can become phagocytic
breaks them down with digestive enzymes
Eosinophils
Type of granulocyte
Parasite killer (like worms ewwwww)
2-4% of leukocyte population
lysosomes in cell contain digestive enzymes
Do not have enzyme that kills bacteria
digestive enzymes released will digest body wall of parasitic worms
only effects worms
Steps of getting infected by tapeworm
consume under cooked meat (eggs are in the meat)
eggs develop to larvae in lungs
coughs up the larvae and end up swallowing them
larvae go through digestive tract
hook on to the walls of small intestine
worms steal nutrients

Basophils
Type of granulocyte
0.5-1% of leukocyte population
have histamine-containing granules
Histamine release causes vasodilation & attracts other leukocytes to area
Tigger itch receptors
Blood vessels widen, so WBCs transport there faster
more WBCs better fight of illness
Explain how seasonal allergies work
basophils are being dramatic
think pollen will kill you
has full histamine response
itchy, red eyes, sneezing, puffy, etc
Agranulocytes
Type of leukocytes
lack visible granules
mainly just nucleus
Types of Agranulocytes
Lymphocytes
T-lymphocytes
B-lymphocytes
Natural Killer cells
Monocytes
Lymphocytes
Type of agranulocytes
25% of leukocyte population
Hang out in lymphatic system
migrate into and out of blood continuously
Types
T-lymphocytes (T-cells)
B-lymphocytes (B-cells)
Natural Killer cells (NK)
Between T-cells and NK cell about 12 types of cancer are killed in a person lifespan
T-lymphocytes
T-cells
act against virus-infected cells and tumor cells
specifically infected own body cells or cells that have grown into tumors
B-lymphocytes
B-cells
produce antibodies released into the blood
attach as red flags to ID things that should be destroyed
Natural Killer Cells
NK cells
act against virus-infected cells and tumor cells
same function as T-cells
Monocytes
Type of agranulocytes
3-8% of leukocyte population
Differentiate into macrophages as they leave bloodstream and enter damaged/infected tissue
actively phagocytic
destroy bacteria, viruses, sources of chronic infection
more or less specialized
Leukopoiesis
production of leukocytes
takes place in red bone marrow
Stimulated by 2 chemical messengers
Interleukins
Colony-stimulating factors
e.g: erythropoietin
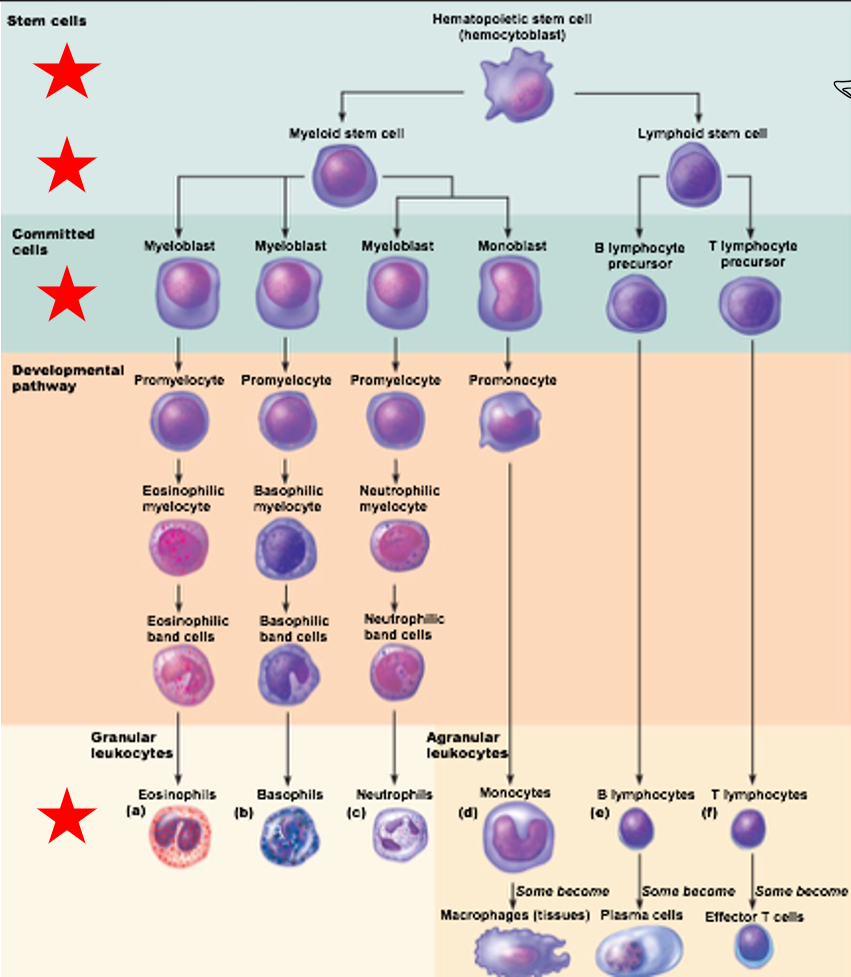
Leukocyte differentiation
Leukocyte differentiation
Hematopoietic stem cell can form either
Myeloid stem cell
Commits to either myeloblast or monoblast
Lymphoid stem cell
Commits to either B-lymphocyte or T-lymphocyte precursor cells
Steps of leukocyte differentiation
Start with Stem Cells - Hematopoietic stem cells (hemocytoblast)
Slightly differentiate - Myeloid stem cells or Lymphoid stem cells
Cells commits
Myeloid Stem Cells to Myeloblast or Monoblast
Lymphoid Stem Cells to B lymphocyte precursor or T lymphocyte precursor
Developmental Pathway
Final Stage
Granular leukocytes form from Myeloblast
Eosinophils
Basophils
Neutrophils
Agranular leukocytes form from Monoblasts, B lymphocyte precursors and T lymphocyte precursors
Monocytes
B lymphocytes
T lymphocytes
Homeostatic Imbalances of Leukocytes
Leukemia
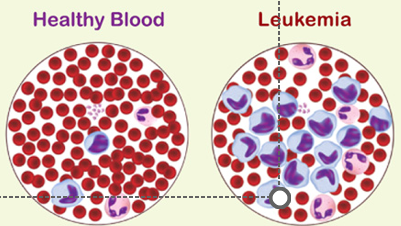
Leukemia
cancer resulting in over-production of abnormal leukocytes
“Extra cells originate from single abnormal cell
Abnormal leukocytes remain unspecialized, proliferate extensively
Cancerous leukocytes crowd red marrow & immature leukocytes flood bloodstream
Other blood cell types are crowded out of blood, resulting in anemia & bleeding problems
Do not defend the body as they shouldinfection & hemorrhage occurs
Way Leukemia is named
according to how fast cells proliferate and the type of cell involved
Rate of proliferation:
Acute leukemia: derived from stem cells
Primarily affects children
Severe and progresses quickly
Chronic leukemia: derived from later cell stages
Primarily affects the elderly
Takes longer to progress
Type of cell involved:
Myeloid leukemia: involves myeloid stem cell descendants
Lymphocyte leukemia: involves lymphocyte
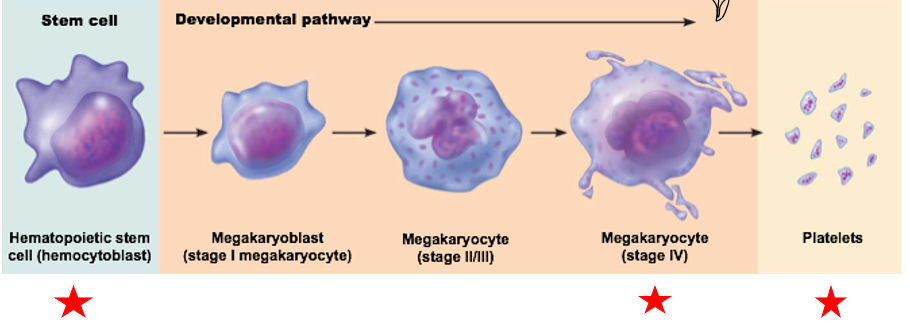
Thrombocytes
Fragments of large cells (megakaryocytes)
Megakaryocyte is fragmented into smaller platelet “cells”released to blood
Average lifespan: about 10 days if unused (shorter if used)
Function: Initiate blood clot formation after damage to blood vessel wall
When blood vessel wall is damaged/torn → platelets stick to each other & to injury site
With no damage → prostacyclin and nitric oxide prevent platelets from sticking together
Prevents unnecessary and unwanted blood clots
Platelet formation regulated by
Hormone thrombopoietin
Steps of platelet formation
Start with stem cell - Hematopoietic stem cell (hemocytoblast)
Developmental pathway results in Megakaryocyte (stage IV)
Bits and pieces breakoff - Platelets
Hemostasis
blood clotting
the process by which bleeding is stopped after blood vessel rupture occurs
very very highly localized response that progresses very quickly
Steps of Hemostasis
vascular spasm
platelet plug formation
coagulation
Vascular Spasm
first step of hemostasis
rapid constriction of a damaged blood vessel
Triggered by:
injured smooth muscle tissue
chemicals released by damaged cells in vessel wall (inflammation)
reflexes from local pain receptors (pain indicates damage)
Platelet Plug Formation
second step of hemostasis
platelets stick to each other & to fibers in blood vessel wall to form a plug in a damaged blood vessel
Platelets release the following in response to injury:
ADP: causes more platelets to stick to site of injury
Serotonin & thromboxane A2: increase vascular spasm & platelet aggregation
Platelet plugs are only good for general wear & tear and small injuries
Not particularly strong
Larger injuries require more severe mechanism to stop bleeding (i.e., coagulation)
Coagulation
third step of hemostasis
formation of a true blood clot
The Process:
Clotting factors (I-XIII) form prothrombin activator
Clotting factors produced by liver
All clotting factors needed for coagulation!
Prothrombin activator catalyzes conversion of plasma protein prothrombin into active enzyme thrombin
Thrombin catalyzes transformation of soluble clotting factor fibrinogen (soluble) into fibrin (insoluble) molecules
Fibrin molecules link together to form long, insoluble strands that stick together
Factor XIII: enzyme that binds fibrin strands to one another (making very strong mesh work)
Fibrin strands also trap platelets & RBCs → forming a blood clot
Blood Clot Retraction
the process of pulling damaged edges of blood vessel close together
Platelets in blood clot have contractile ability (much less than muscle tissue)
Contraction pulls fibrin strands together & pulls edges of injury closer together
easier to repair small area
Platelet-derived growth factor
causes increase in number of fibroblasts and smooth muscle cells in damaged area
Forms connective tissue that will eventually form new blood vessel wall where damaged occurred
Fibrinolysis
the removal of blood clot after healing is complete
prevents blood clots form on top of old blood clots
Plasmin: enzyme that digests fibrin
Typically begins within 2 days of clot formation
Depends on extent of damage
Homeostatic Imbalances of Blood Clotting
Thromboembolic Disorder
Thrombus
Embolus
Bleeding disorders
Thrombocytopenia
Hemophilia
Thromboembolic Disorders
formation of undesired/unnecessary blood clots
Thrombus (stationary)
Embolus (circulates)
Thrombus
Thromboembolic Disorder
formation of blood clot in unbroken vessel (*remains stuck to vessel wall*)
Effect: blocks circulation
How bad depend on size of thrombus
Embolus
Thromboembolic Disorders
thrombus that breaks free & enters circulation
Effect:
If small, embolus is generally not a problem
If large, can obstruct smaller blood vessels & block circulation
Examples:
Pulmonary (lung): very bad, decreased oxygen supplied to body
Cerebral (brain): ischemic stroke
Bleeding disorders
absence of desirable blood clots, leading to excessive bleeding
Thrombocytopenia
Hemophilia
Thrombocytopenia
Bleeding disorder
low number of platelets in circulation
Limited ability of body to form platelet plugs → even “small breaks” can cause massive hemorrhage
Caused by: anything that decreases red bone marrow will usually decrease platelet count
Hemophilia
Bleeding disorder
hereditary bleeding disorders
Deficiency or absence of certain clotting factors causes extreme bleeding from small cuts/injuries
Symptoms: prolonged bleeding into tissues, painful/disabled joints
Types:
Hemophilia A: deficiency of clotting factor VIII (sex linked on x chromosome, most dangerous)
Hemophilia B: deficiency of factor IX (sex linked on x chromosome)
Hemophilia C: lack of factor XI (least dangerous)
Treatment:
all very expensive
Plasma transfusions
Injections of absent/deficient clotting factor
Prefix for heart
“cardio-”
Function of the heart overview
movement of blood
Multichambered
Tissue: Cardiac Muscle Tissue
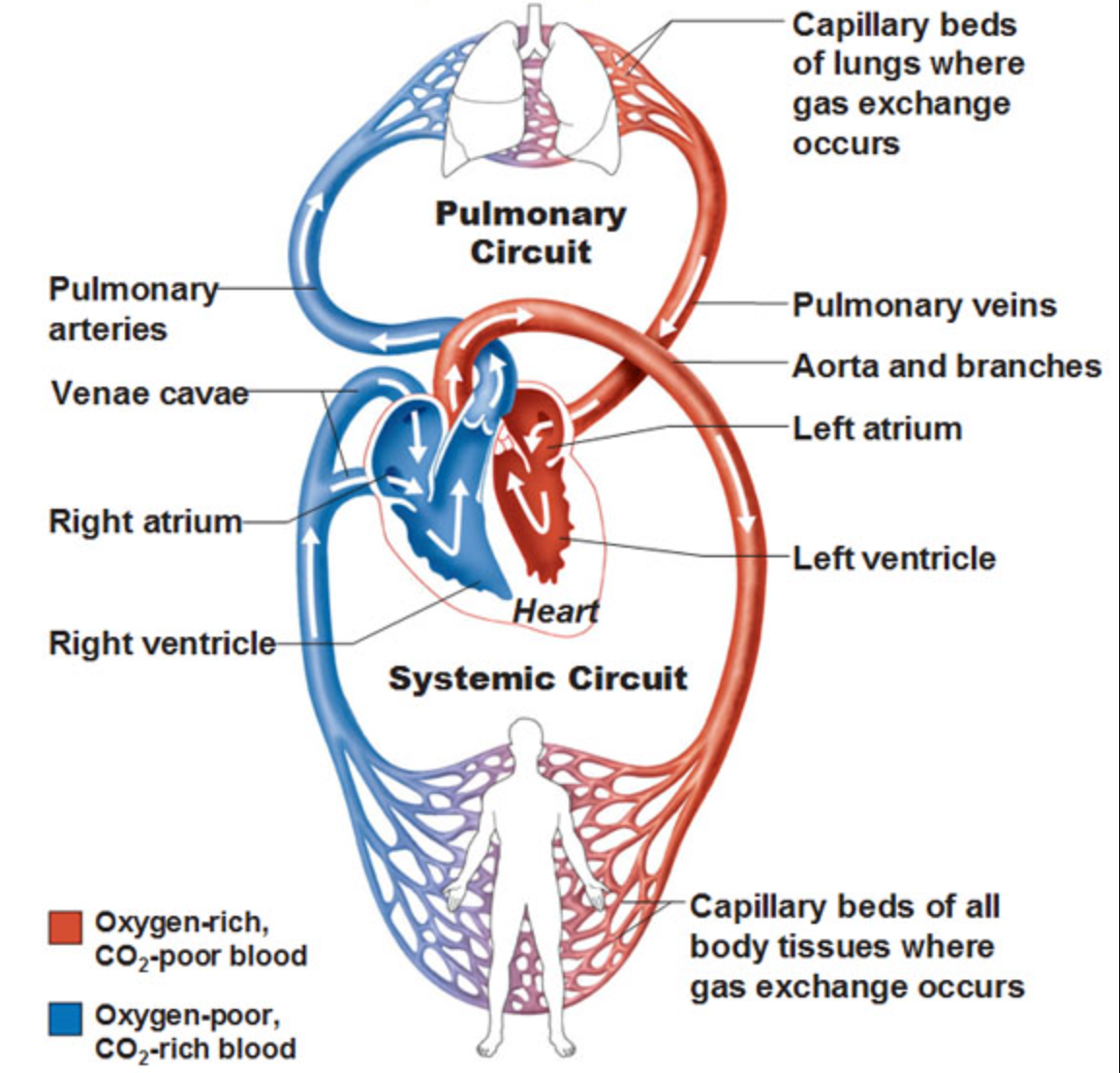
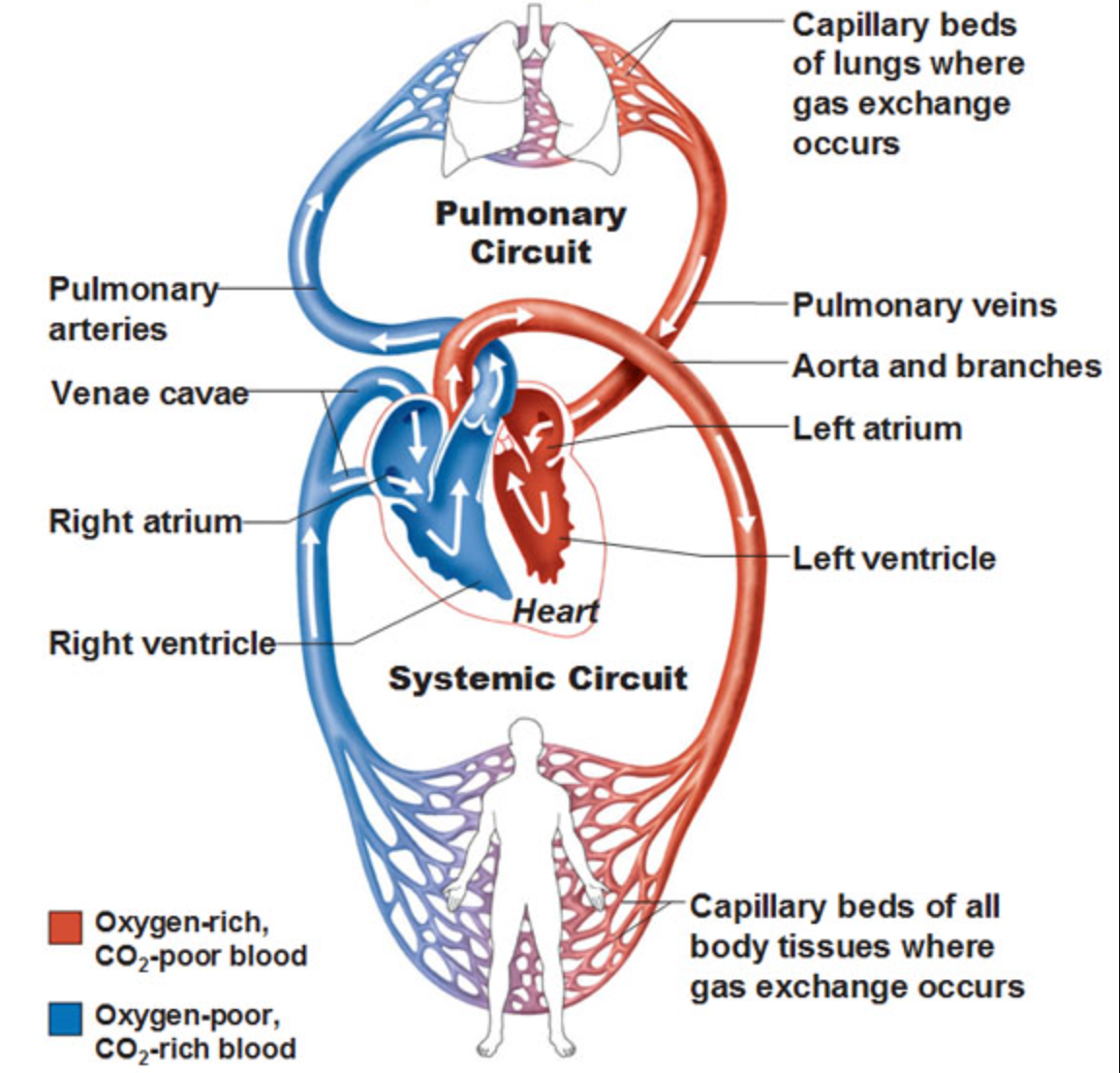
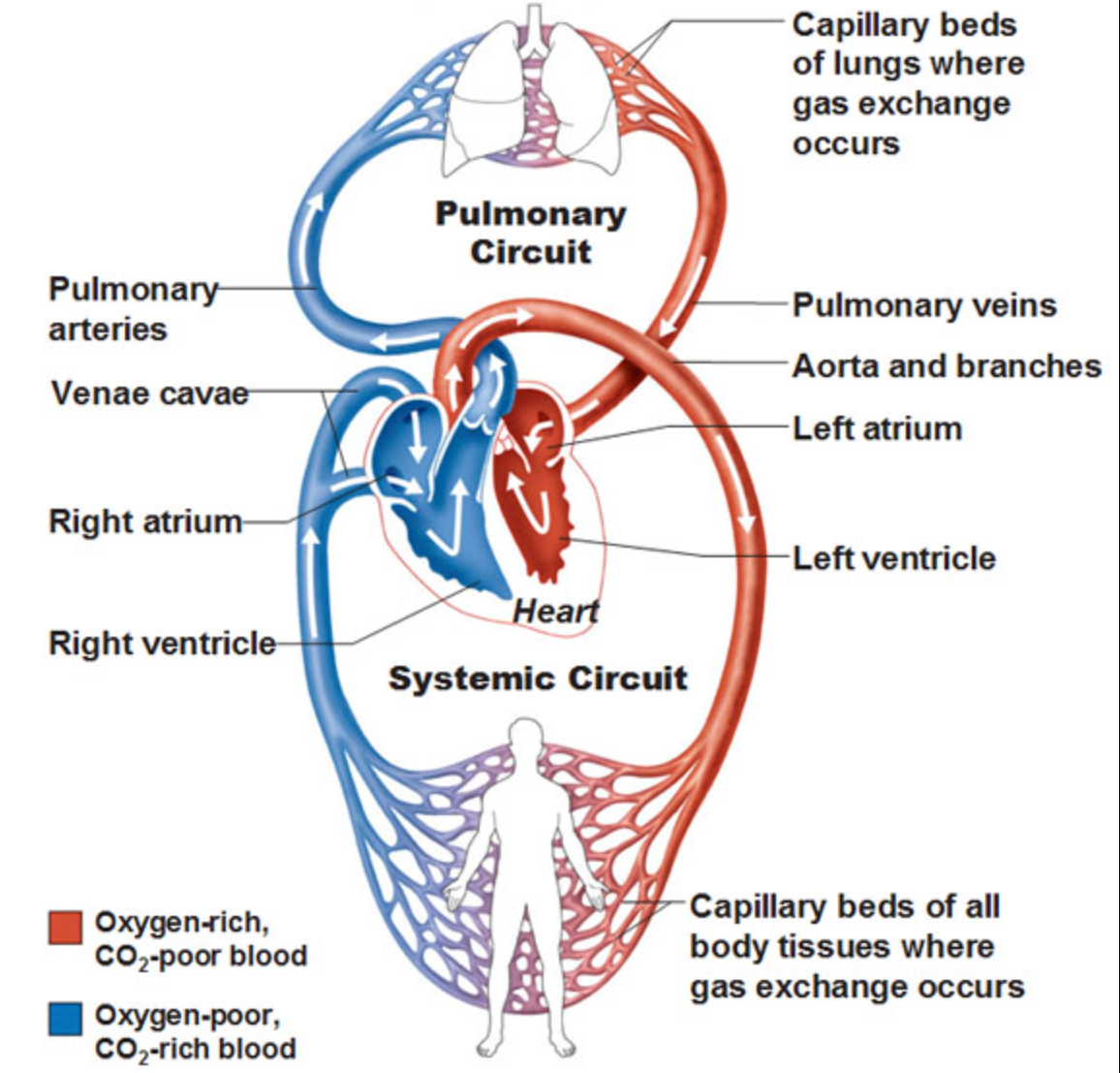
Circuits that move blood through the body
Pulmonary Circuit
Systemic Circuit
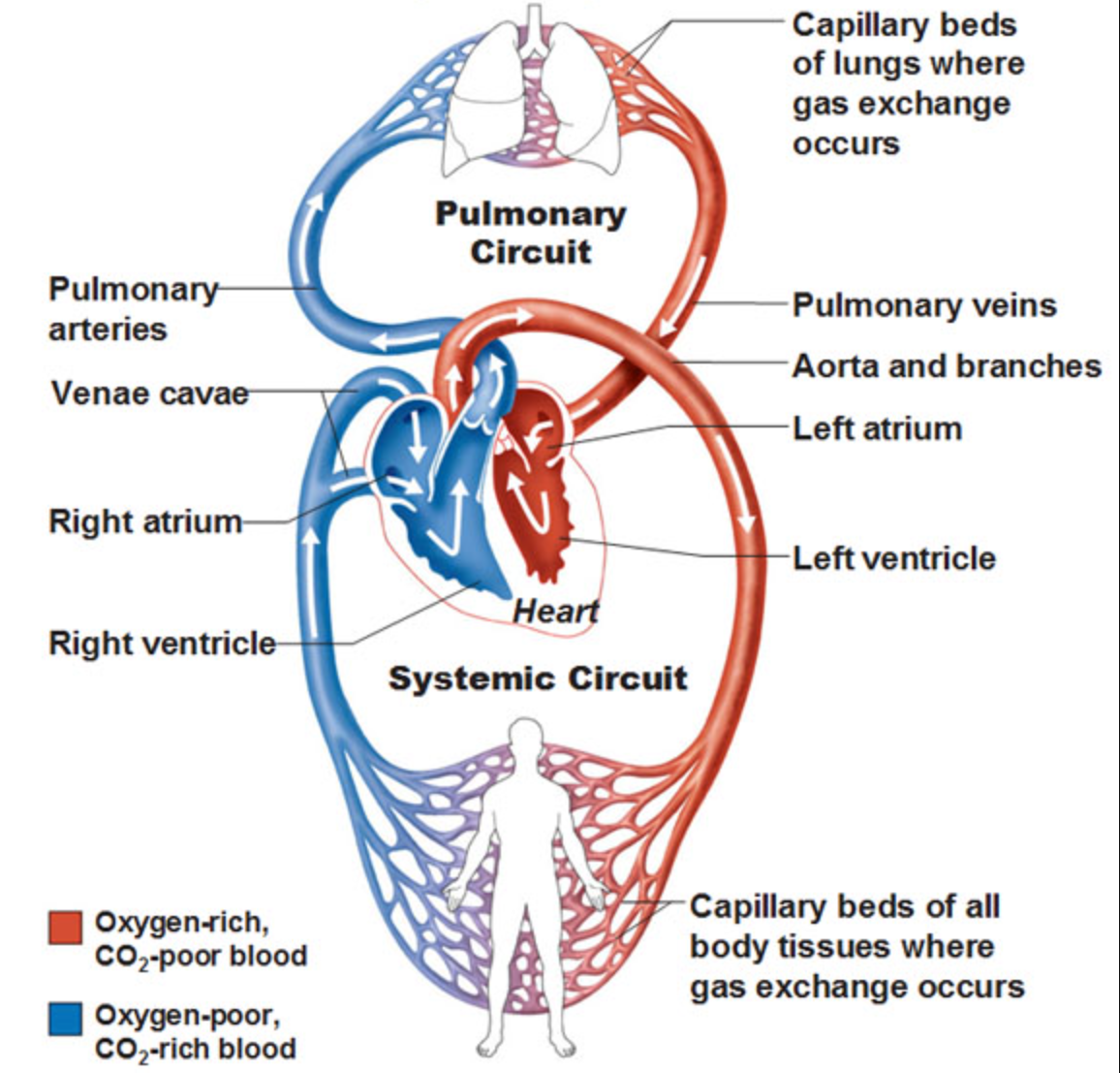
Pulmonary Circuit
any of the blood vessels that carry blood to and from the lungs
to lungs supplies blood with O2 and disposed of CO2
away from lungs supplies the body tissues with O2
made up of
Pulmonary arteries
Pulmonary veins

Pulmonary arteries
pump oxygen poor blood from right side of the heart to the lungs

Pulmonary veins
pump oxygenated blood from the lungs to the left side of the heart
What side of the heart is part of the pulmonary circuit?
Right

Systemic circuit
any of the blood vessels that carry blood to and from the tissues
oxygenated blood leaves heart through aorta (and its branches) to body tissues
oxygen poor blood returns to heart via superior vena cava & inferior vena cava
What side of the heart is part of the systemic circuit?
Left side
The right & left side of the heart pump roughly the __ volume of blood per minute, BUT:
The right & left side of the heart pump roughly the _SAME_ volume of blood per minute, BUT:
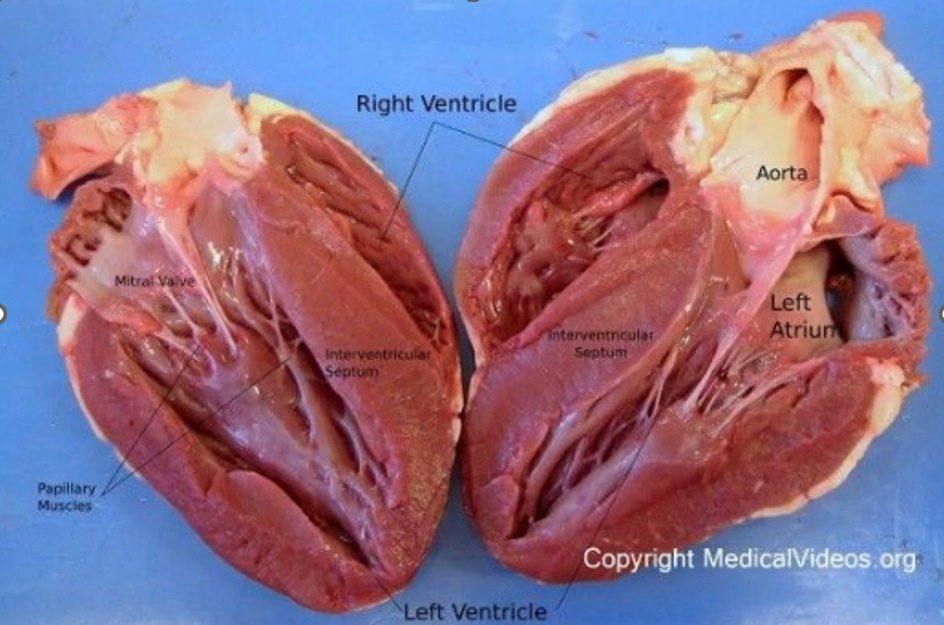
wall that immediately surrounds empty space is muscles
The right side (pulmonic) is relatively low-pressure
smaller than left
thinner walls, less muscle, less force
The left side (systemic) is high pressure
The walls of the left side of the heart (especially the ventricle) are very thick, more muscle, more force
Why?
Right side delivers blood to in the same cavity, needs to travel shorter difference
Left side delivers blood to rest of body, head to toes, needs to travel farther
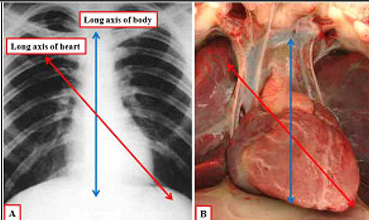
Gross Anatomy of the Heart
Heart slightly on left side
The heart is tipped in the thoracic cavity
Apex (inferior “tip” of the heart) points to left hip
Ensures blood vessels stay open and are not crushed