Evaluation of Sodium and Water Disorders
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
What is Tonicity?
Tonicity refers to the ability of surrounding solution to cause a cell to gain or lose water
→ Tonicity specifically measures the concentration of effective osmoles that cannot freely cross the cell membrane, rather than things that can which are termed ineffective osmoles
→ So tonicity then is osmolality minus the ineffective osmoles across the cell membrane
What do Laboratory abnormalities represent?
Lab abnormality values represent a new equilibrium
→ this indicates that an abnormal value must mean that a regulator of that value is either not working or overwhelmed
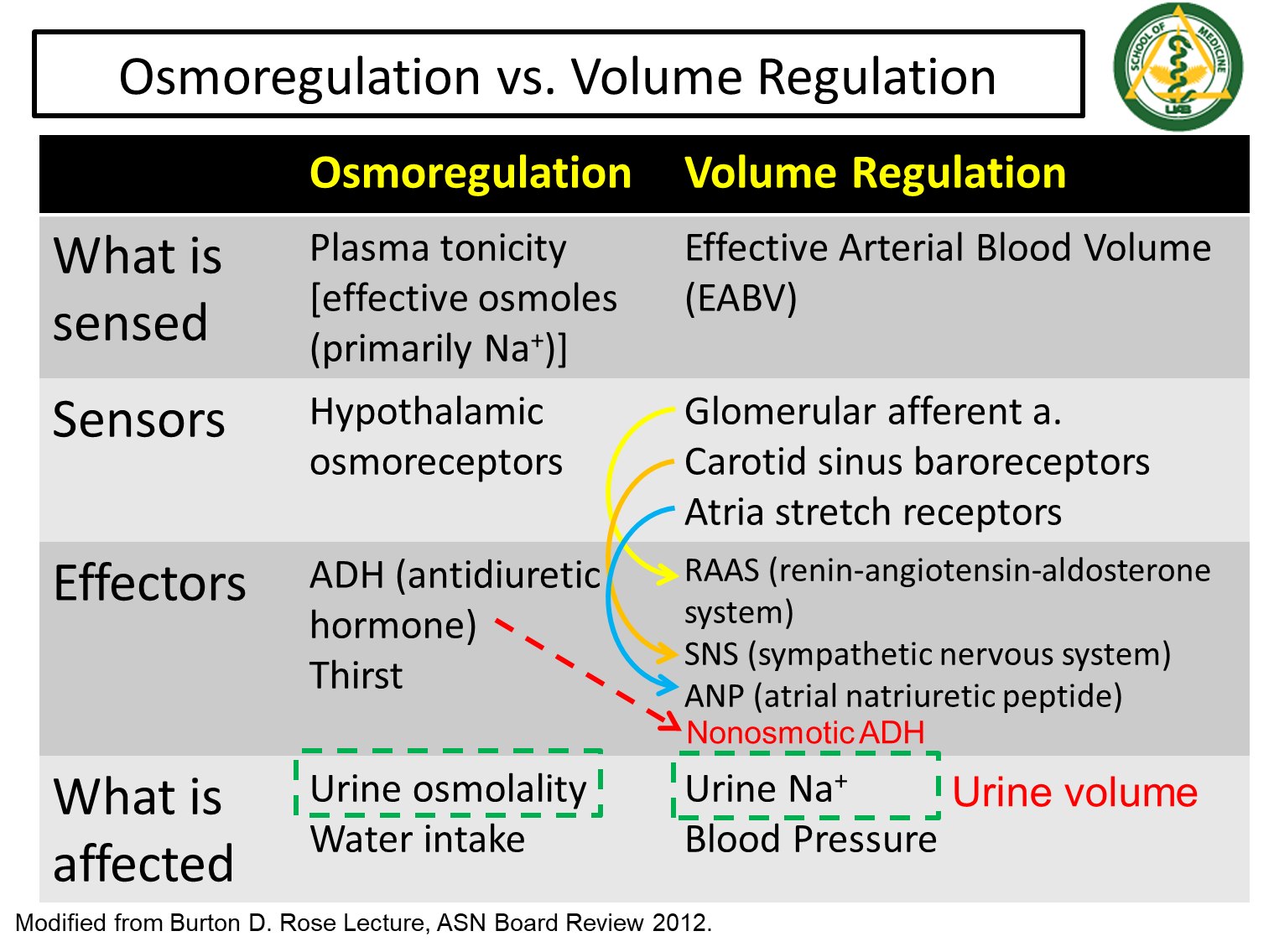
What is the difference between volume regulation and osmoregulation

Osmoregulation
1) Osmoregulation begins by sensing changes in plasma tonicity via the hypothalamic osmoreceptors
→ high tonicity would cause our osmoreceptors to trigger ADH secretion as well as thirst sensation
→ this results in a high urine osmolality due to increased ADH and water reabsorption
Volume Regulation
1) Volume regulation begins by sensing the effective arterial blood volume in the baroreceptors
→ will activate the RAAS, SNS, and ANP systems leading to low sodium levels in the urine because of sodium reabsorption
When is ADH released apart from changes in tonicity?
ADH, while primarily released in times of high tonicity, can also be released during a volume contracted state
→ in cases of emergency where volume is low in the body, despite activation of RAAS and SNS, you can recruit ADH in order to reduce urine volume
→ this only occurs in severe drops in arterial blood volume
How do you calculate plasma sodium concentration?

1) You cannot divide sodium concentration in ECF over ECF due to the corrective mechanisms that will draw water into the ECF when salt levels increase
→ you can also not divide sodium content by total body water because it doesn’t account for the movement of sodium between the ICF and ECF
2) Instead we use exchangeable sodium and exchangeable potassium in order to account for ICF and ECF movement over total body water
What is the Plasma Osmolality Equation? Why does the equation calculating for plasma osmolality multiply sodium concentration by 2?

In the plasma osmolality equation sodium is multiplied by 2 in order to reflect that its the largest factor determining osmolality
→ In the extracellular space, sodium is the largest positive charge which will draw negative solutes along with it
→ this is why we multiply it by 2, in order to account for the negative solutes that follow sodium
What are the three steps to a basic approach to sodium disorders?
1) Confirm that plasma sodium abnormality matches the plasma osmolality abnormality
→ When plasma sodium is decreased, then plasma osmolality should also be decreased and vice versa
2) If they are the same direction, determine the patient’s extracellular fluid volume status based on physical exam
→ hypovolemic, euvolemia, hypervolemia
3) Think about homeostasis
→ what is the expected urine sodium and urine osmolality in order to meet their clinical picture and extracellular volume status
What does a low versus high sodium urine concentration indicate?
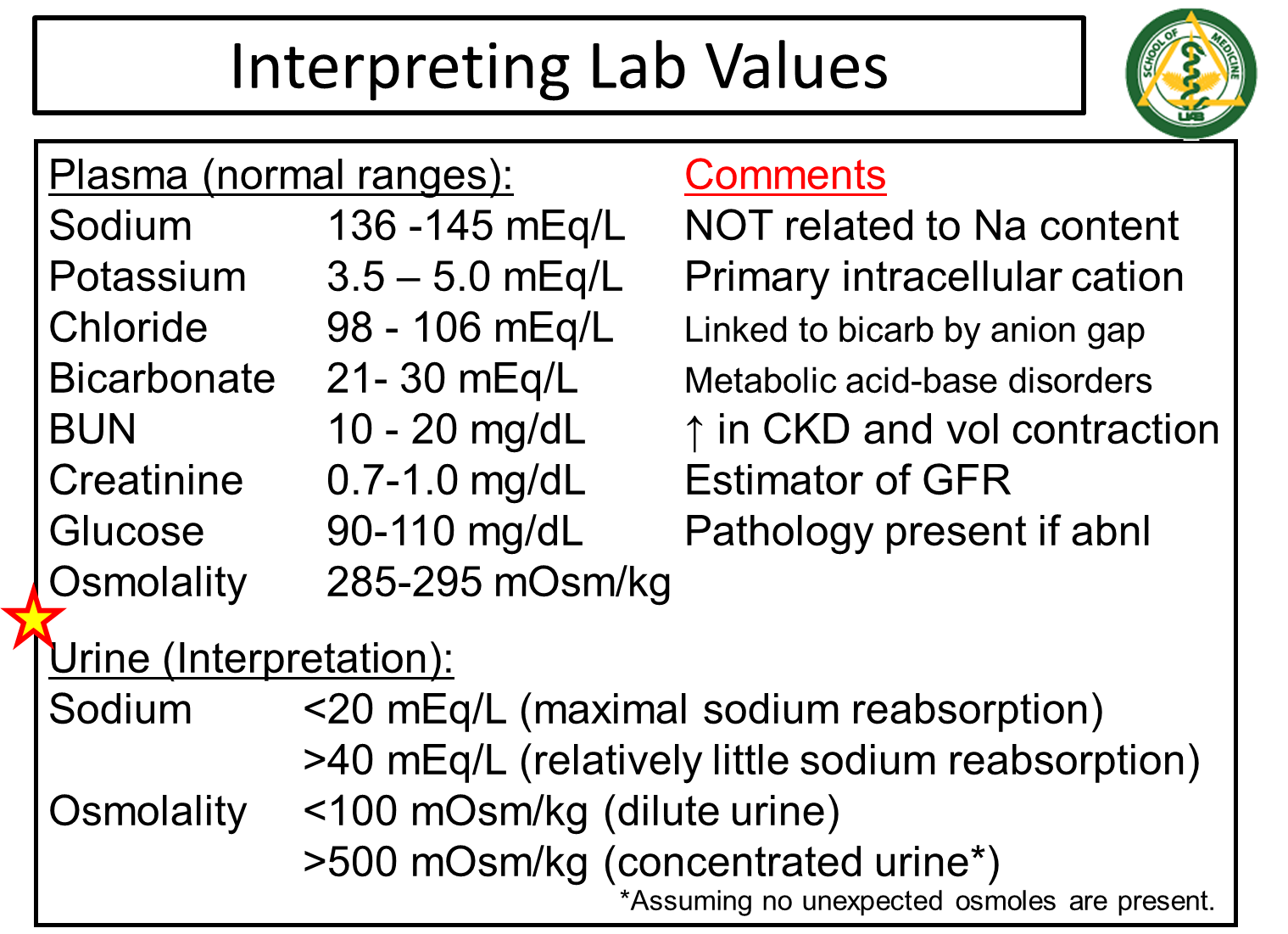
Low Sodium in the Urine < 20 mEq/L indicates RAAS activation and maximal sodium reabsorption
High sodium in the Urine > 40 mEq/L indicates little sodium reabsorption
What does high and low urine osmolality indicate?
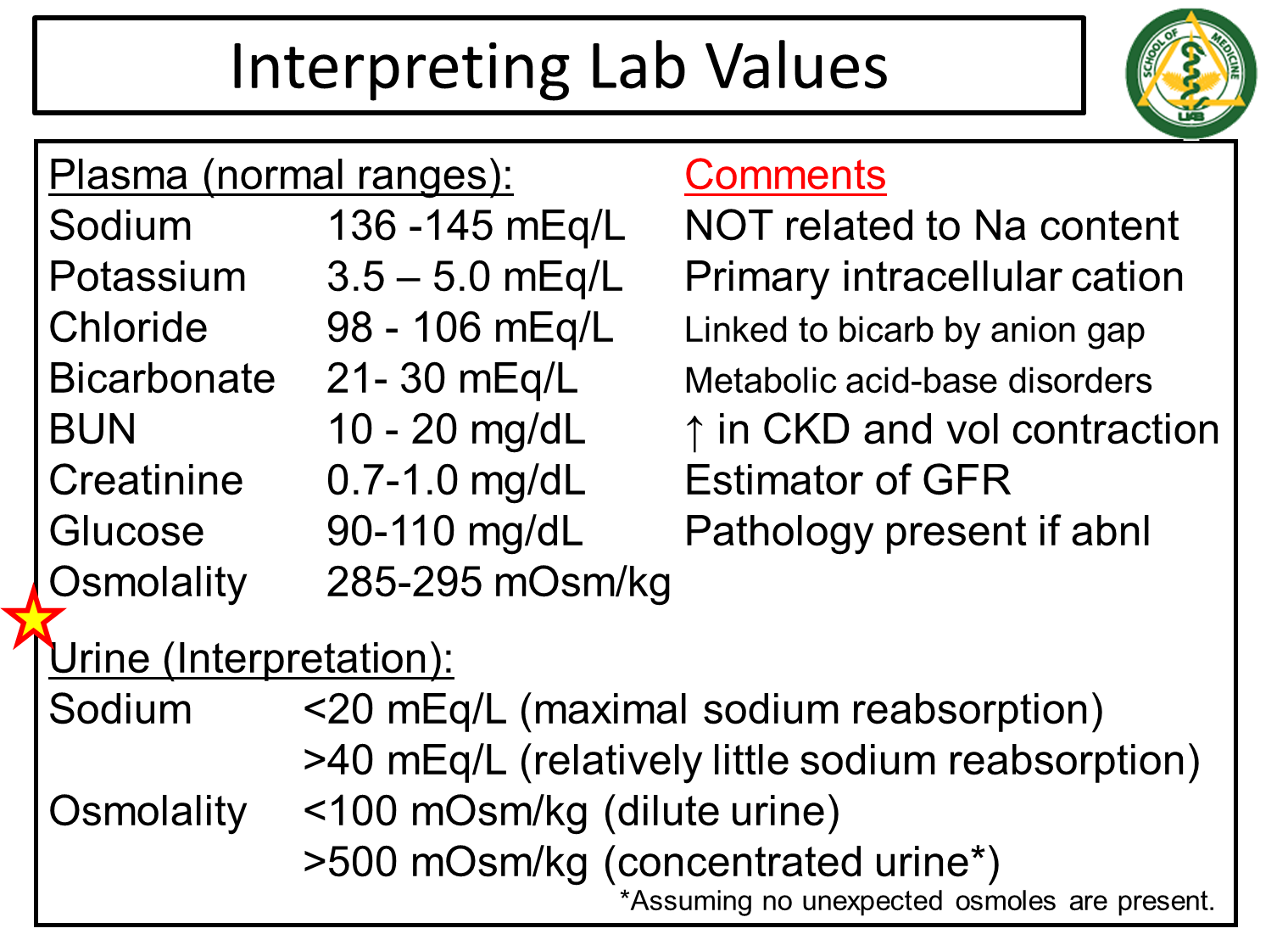
Low Urine Osmolality < 100 mOsm/kg - dilute urine and no ADH activity
→ when this number is lower than plasma osmolality it means we are losing more water in the urine than we have in the plasma
High Urine Osmolality > 500 mOsm/kg - concentrated urine and high ADH activity
What is Diabetes Insipidus?
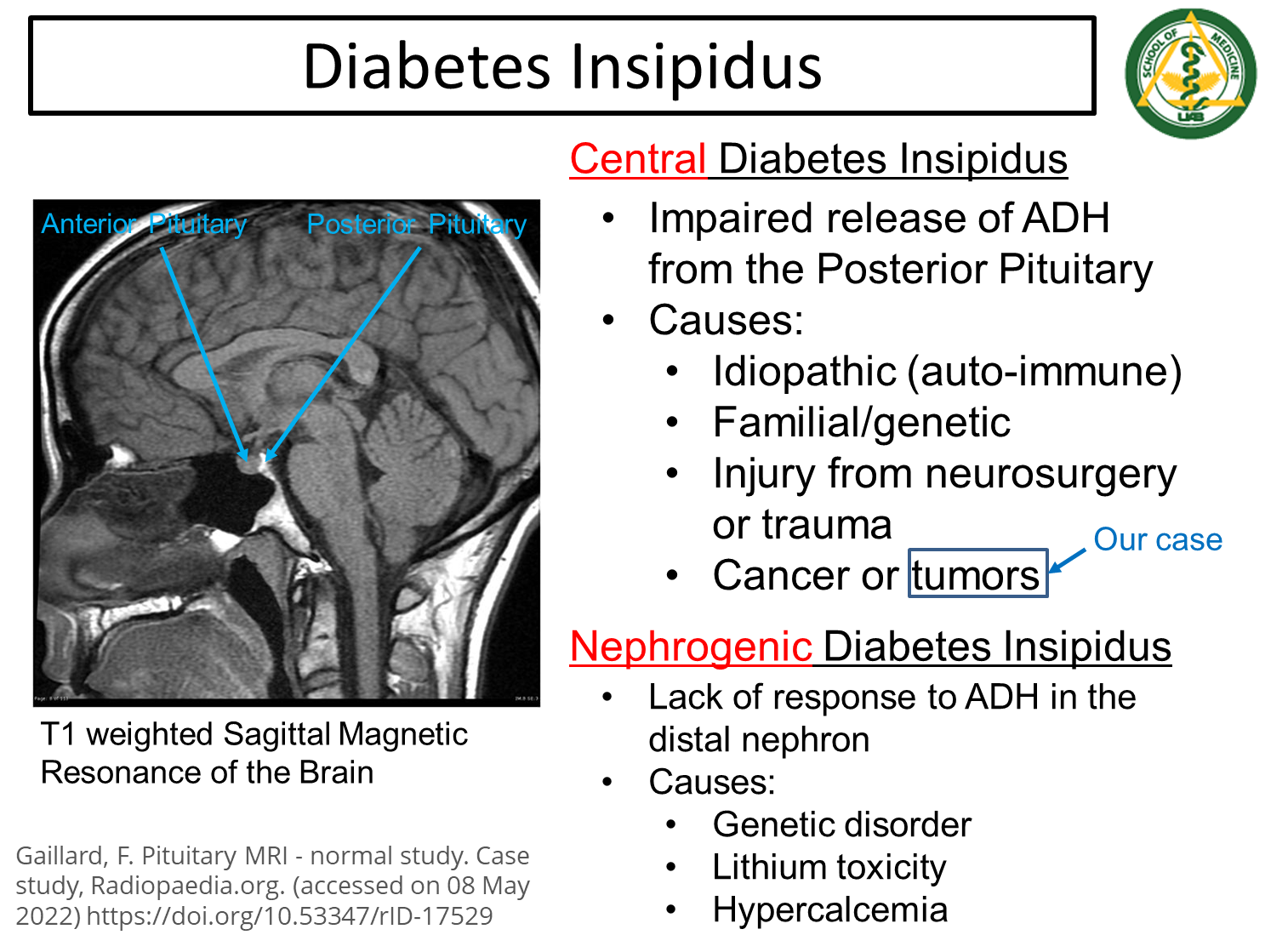
Diabetes Insipidus is a condition where ADH is not secreted or ADH is nonfunctional. Subdivided into Central and Neurogenic
→ results in a low urine osmolality even in a patient that should be expected to have high ADH levels and increased sodium reabsorption from the urine
1) Central
→ impaired release of ADH from the posterior pituitary gland and can be caused by a variety of issues
2) Nephrogenic
→ lack of response to ADH in the distal nephron
What is the Osmotic Regulation of ADH?
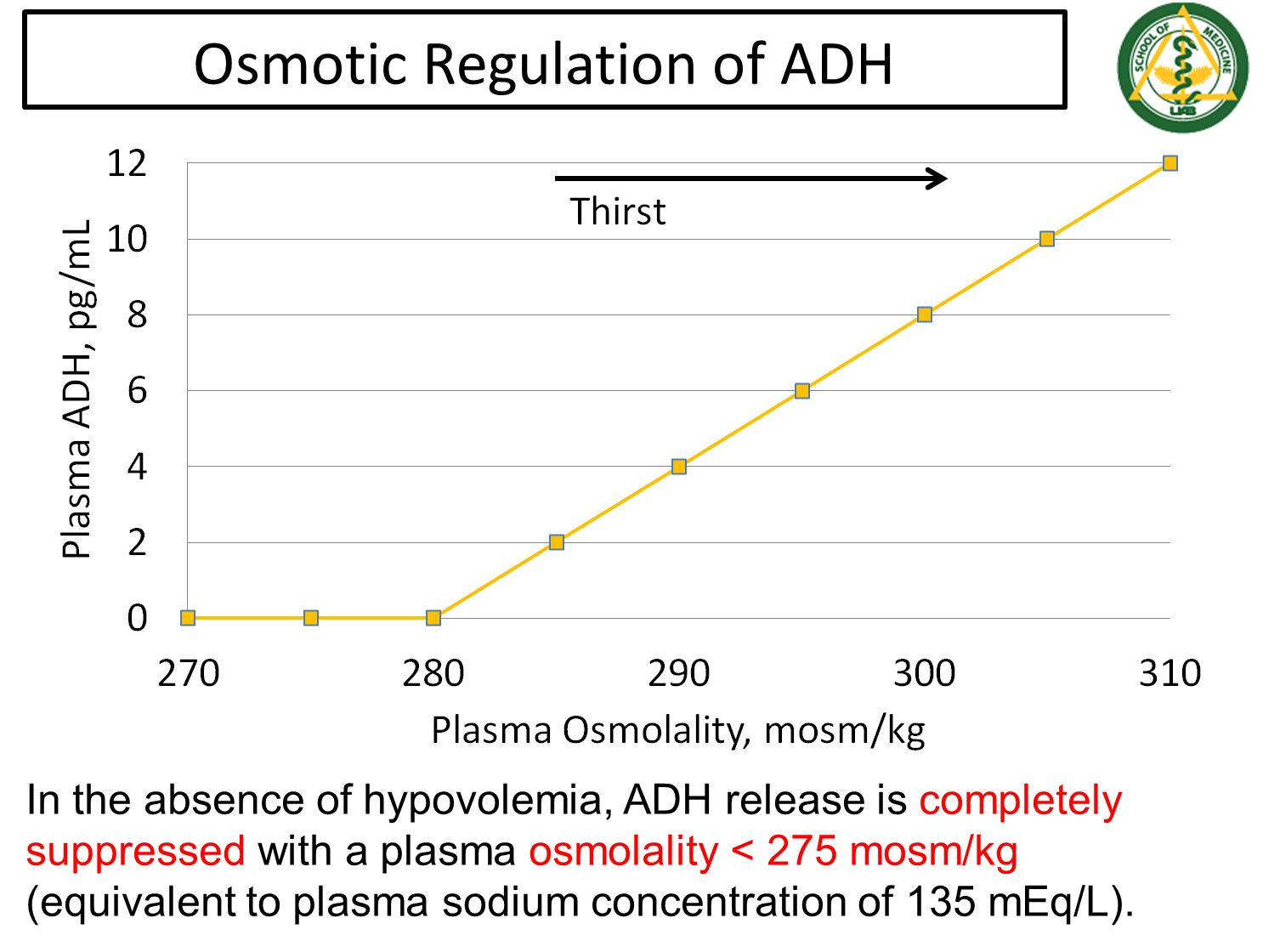
ADH release is completely suppressed with a plasma osmolality of less than 275 mOsm/kg in the absence of hypovolemia
→ or a plasma sodium concentration of 135 mEq/L
What is Syndrome of Inappropriate ADH?
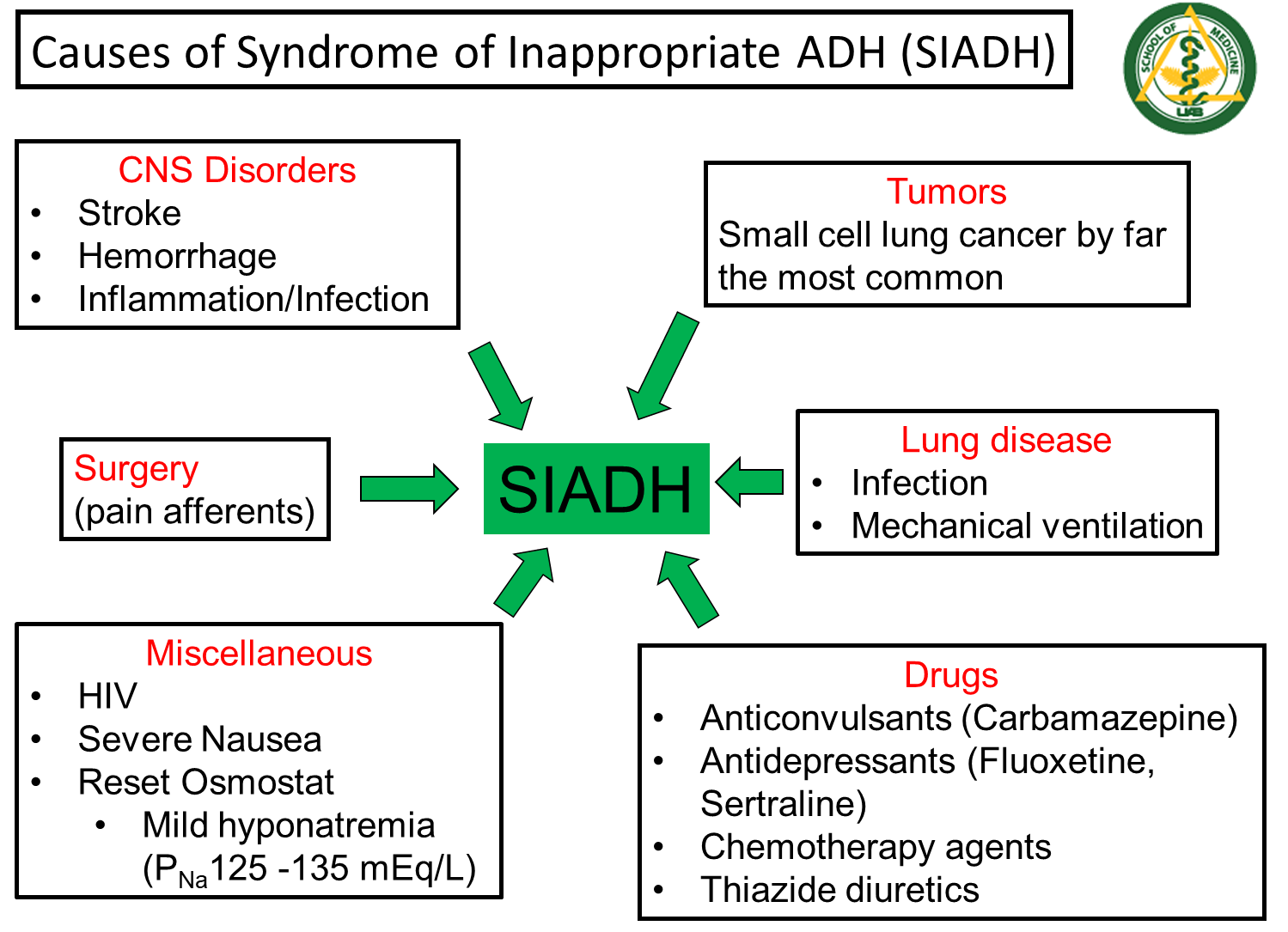
SIADH or Syndrome of Inappropriate ADH is a syndrome where ADH is released when it should not be
→ Can be caused by CNS issues, Surgery, Tumors, and other miscellaneous conditions
→ most likely indicated in a patient that has low plasma osmolality and low sodium levels, but their urine osmolality is abnormally high indicating that ADH is being secreted when unnecessary
What is acute hyponatremia?
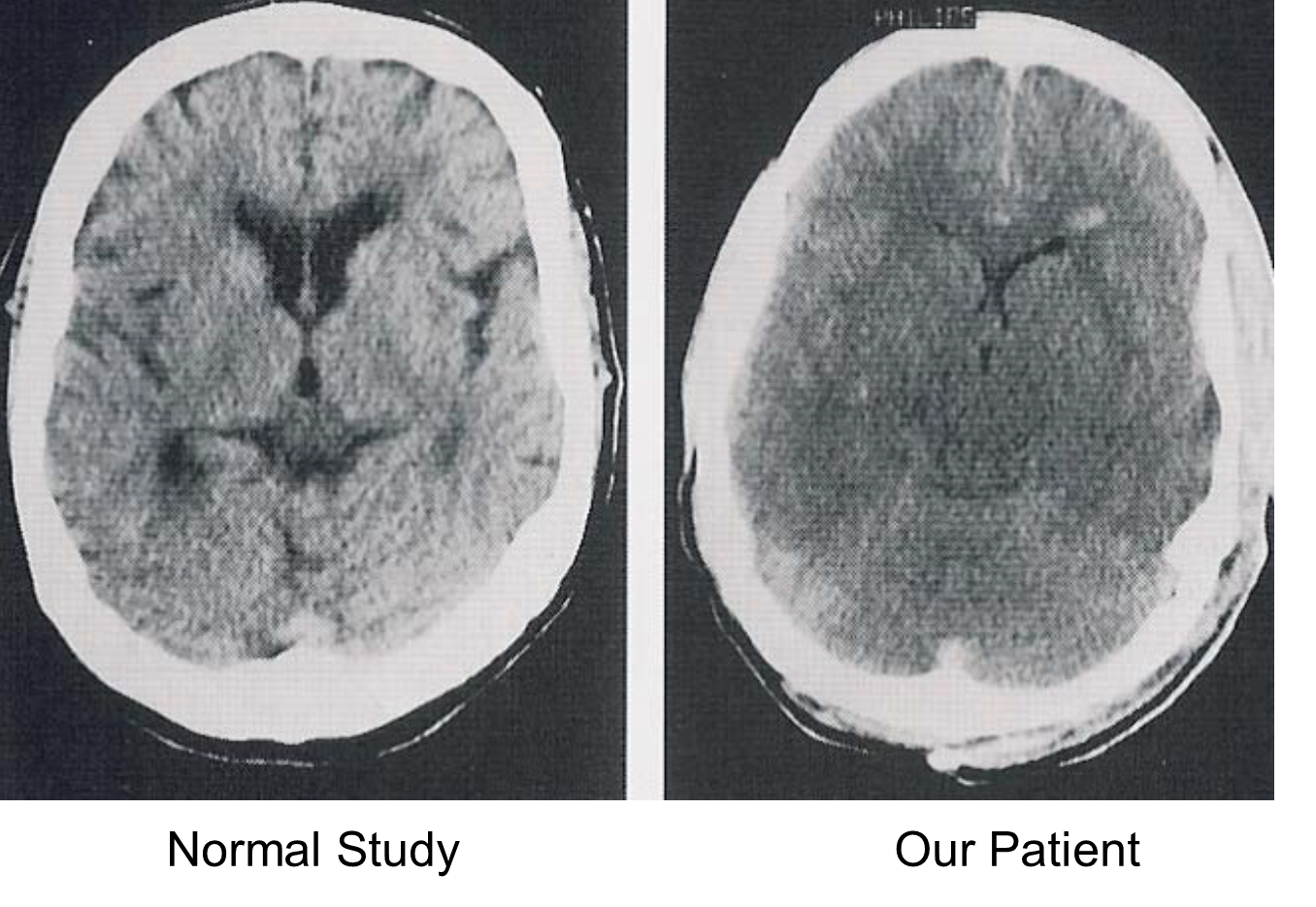
Acute Hyponatremia is a rapid drop in serum sodium concentration over a short period of time
→ this sudden decline causes a dangerous shift of water into the brain due to the plasma becoming hypotonic relative to brain tissue causing cerebral edema and seizures
→ Can occur in patients with high urine osmolality, due to being volume contracted and secreting ADH, but is blowing off large amounts of sodium in some form (low sodium urine)
→ treated with hypertonic saline
What is the brains response to chronic hyponatremia?
Following 48 hours, in response to cerebral edema caused by hyponatremia
→ brain will place taurine and myoinositol on the cell surface that pumps out organic osmoles allowing for the brain to shrink back to normal size
What is Seizure First Aid?
Call 911 and lay the person on their side while padding their head
→ do not restrain or put anything into their mouth
What is Osmotic Demyelination?
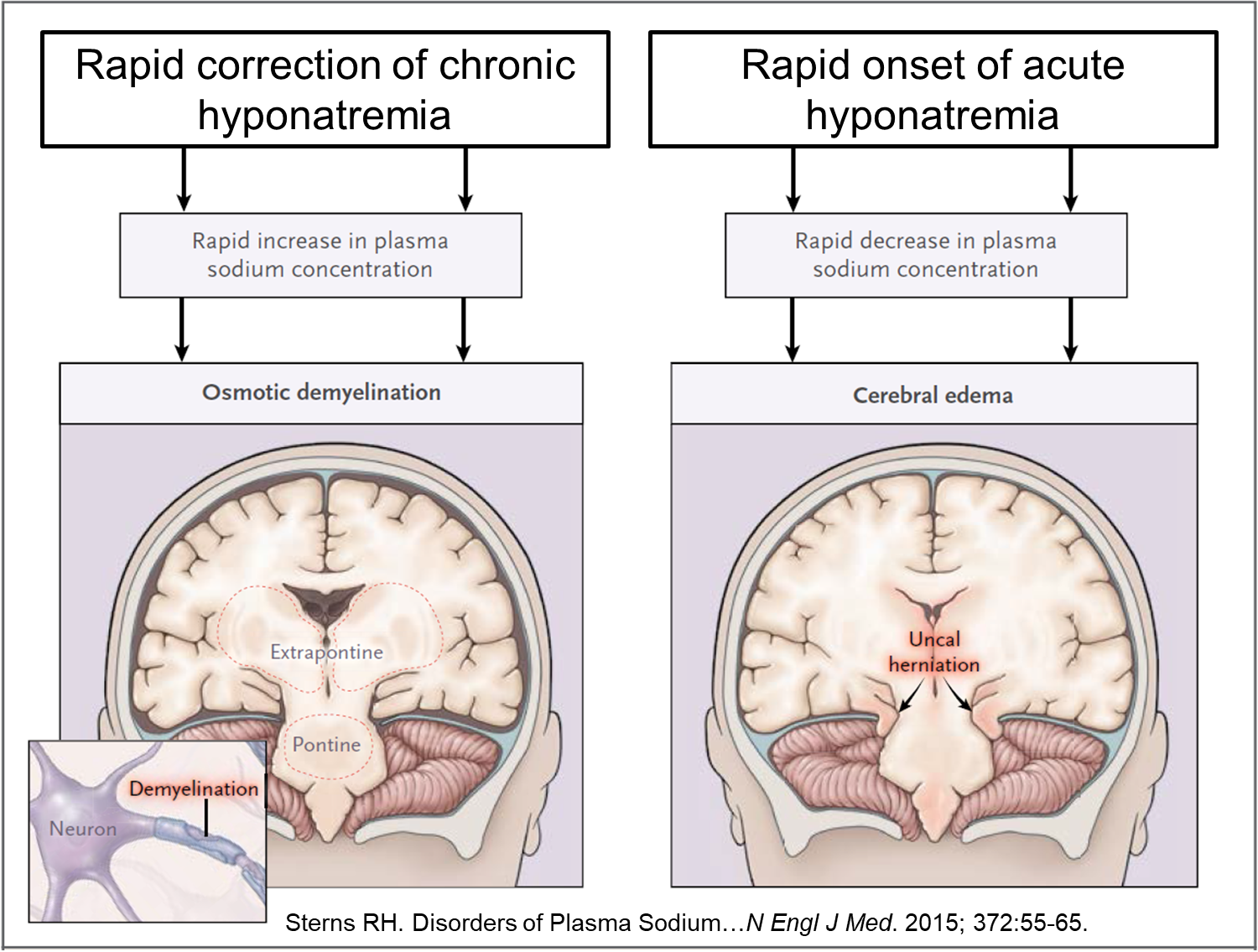
During rapid correction of chronic hyponatremia the patient can be susceptible to osmotic demyelination
→ When you rapidly raise the plasma sodium concentration too quickly you risk causing demyelination of the neurons causing locked in syndrome
→ patients can also become paralyzed
What are the three different sodiums?
Exchangeable Sodium
→ sodium available to move across the cell membrane
→ sodium that is not trapped in bone or connective tissue
Total Body Sodium
→ Amount of sodium in the body which is directly proportional to the ECF volume and weight
Plasma Sodium Concentration
→ Representation of the relative amount of water to solute in the body