Multiple Sclerosis (Khan)
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Cause of MS?
unknown→ but genetic/viral links
Symptoms of MS?
dysarthria (speech problems)
optic neuritis
fatigue
spasms
incontinence
depression
Pathogenesis of MS:
What do white blood cells do in MS?
How do MS lesions arise?
What happens to the BBB?
WBCs (B and T lymphocytes) involved in adaptative immunity attack the CNS
MS lesions arise from destruction of oligodendrocytes (what makes the myelin) or direct myelin destruction
BBB is destroyed as well (allows WBCs to easily get in and attack)
Steroids used for acute attacks of MS are used _____ dose for _____ duration.
a. high dose, short duration
b. high dose, long duration
c. low dose, short duration
d. low dose, long duration
a.
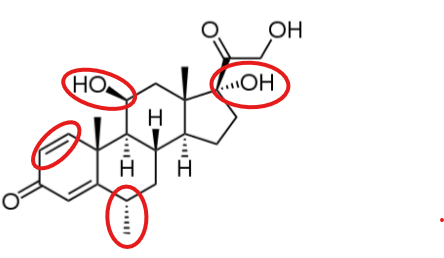
What group on methylprednisolone is required for activity?
unsaturated system (C4-5)
What groups on methylprednisolone increase GC activity?
double bond on C1-2 (increases GC activity, decreases MC activity)
a-hydroxyl at C17 (increases GC activity)
b-hydroxyl at C11 (increases GC activity)
methyl group at C6 (increases GC/MC ratio)
MOA of glucocorticoids:
steroid in circulation bound to CBG (aka protein bound in blood)
enters cell and binds to CYTOPLASMIC RECEPTOR
receptor changes conformation
steroid-receptor complex translocates to nucleus
receptor dimerizes, binds to GRE (DNA)
results: increase/decrease in transcription
(note: BINDS in the cytoplasm, ACTS in the nucleus)
ADRs of glucocorticoids:
mood disturbances
hyperglycemia
GI
infection risk
metallic taste
What ADR is associated with long term systemic steroid use?
HPA suppression (basically when natural cortisol production is shut down)
What drugs are ONLY used for tx of acute attacks with MS?
glucocorticoids (methylprednisolone, prednisone)
ACTH (corticotropin)
ACTH is part of a precursor molecule to what? which is the precursor to what hormone?
ACTH→ POMC→ MSH hormone
MOA of ACTH:
acts on what receptors?
what type of receptor? G protein? ionotropic?
activates or inhibits AC?
increases or decreases cAMP?
stimulates production of what?
results?
acts on melanocortin receptor (MC2)
which is a GPCR
activates AC → increases cAMP
stimulates: cortisol, androgen, and mineralocorticoid secretion
results: immunosuppression, adrenal suppression?
ADRs of ACTH:
electrolyte and psych disturbances
MOA of Interferon B (IFN-β):
results?
DIMERIZATION: IFN-β binds to receptor, dimerization occurs
PHOSPHORYLATION: receptor phosphorylated, activates mobile tyrosine kinase JAK
STAT PHOSPHORYLATION: JAK phosphorylates STAT molecules
TRANSLOCATION: STAT-P dimerization occurs→ translocation to nucleus
gene expression effected
RESULTS:
decrease immune cell BBB adhesion/penetration
reduces inflammation
increase neurotrophic factors
ADRs of Interferon B (IFN-β):
Flu-like symptoms
Severe depression
Injection site necrosis
Elevated liver enzymes
Thyroid dysfunction
Others: leukopenia, pain
Which fumerates are prodrugs? which is the actual drug?
prodrugs: dimethyl fumarate and diroximel fumerate
actual drug/active metabolite: monomethyl fumarate
MOA of Fumerates:
activates what?
results?
activate Nrf-2 transcription pathway
results: increased expression of antioxidative enzymes and increase GSH (glutathione) biosynthesis
(FYI: oxidative stress is bad in MS bc it produces free radicals that further MS… here this drug increases antioxidants that will neutralize these free radicals)
In addition to the antioxidative effects, what else occurs as a result of Nrf-2 pathway activation with fumerates? leads to what side effect?
nACh agonist→ leads to ADR of cutaneous flushing
ADRs of Fumerates:
cutaneous flushing
hepatotoxicity
neutropenia
What is the PREFERRED MS drug in PREGNANCY?
glatiramer acetate
MOA of Glatiramer acetate:
mimics antigenic properties of myelin basic protein (MBP) (part of the myelin sheath)
acts as decoy for immune attack on MBP
BASICALLY: mimics a protein that makes up myelin and tricks the immune system into attacking it INSTEAD of myelin
ADRs of Glatiramer acetate:
injection site rxns
post infusion rxns (flush, diaphoresis, dypsnea)
chest pain
flu-like symptoms
List the Spingosine1P modulators:
Fingolimod
Ozanimod
Siponimod
Ponesimod
What is the ONLY Spingosine1P modulator that is a PRODRUG and needs phosphorylated?
Fingolimod
MOA of Spingosine1P modulators?
bind to S1P1R receptor→ causes irreversible downregulation, internalization, and degradation of S1P1R
results: blocks lymphocytes egress from lymph nodes
basically: traps lymphocytes (B and T cells) in the lymph nodes so they can’t attack the CNS
ADRs of Spingosine1P modulators?
bradycardia
macular edema
increased LFTs
What drug is contraindicated in pts. homozygous with CYP2C9*3/*3 genotype?
Siponimod
What drug is contraindicated with MAOIs?
Ozanimod (bc Ozanimod metabolite inhibits MAO)
What are the contraindications with Spingosine1P modulators?
cardiac issues→ arrhythmias, MI, stroke/TIA, HF
What facilitates the rapid removal of Teriflunomide?
activated charcoal and cholestyramine
MOA of Teriflunomide:
inhibits synthesis of orotate (pyrimidine precursor)
inhibits the enzyme dihydrooorotate dehydrogenase
results: decreased # of activated lymphocytes in CNS
BBW AND C/I of TERIFLUNOMIDE:
PREGNANCY (cat X)
HEPATOTOXICITY
MOA of Cladribine:
prodrug activation?
requires phosphorylation to its triphosphate (deoxyadenosine derivative)
incorporates into DNA and causes DNA strand break→ apoptosis
For Cladribine:
ADRs
BBW
C/I
ADRs: infections, liver injury, heart failure
BBW: malignancy, teratogenicity (must use contraception)
C/I: malignancy, HIV, chronic infection
MOA of Mitoxantrone:
intercalation with DNA (affects transcription / translation / replication)
radical induced damage
inhibits Top II
ADRs and BBW of Mitoxantrone:
ADRs: cardiotoxicity, BMS, GI/cutaneous disturbances, alopecia
BBW: cardiotoxicity, BMS, malignancy
MOA of Natalizumab (TYSABRI):
results?
binds to alpha-4 integrins and prevents interactions with VCAM-1 receptors on CNS vessel walls
results: lymphocytes can’t get in the BBB
ADRs and BBW of Natalizumab:
ADRs: infusion rxns, HA, fatigue
BBW: progress multifocal leukoencephalopathy
viral infection of white matter in brain
MOA of Alemtuzumab:
HUMANIZED mAb that binds to CD52 abs on B cells
results: increases antibody-dependent cell mediated cytolysis →
B-cell depletion
BBW and C/I of Alemtuzumab:
BBW:
infusion rxns
autoimmune conditions
stroke
malignancies
C/I: HIV
What was the first drug approved for PPMS? (progressive primary MS)
Ocrelizumab
What drugs are CD20 targeting antibodies?
Ocrelizumab
Ofatumumab
Ublituximab
What CD20 targeting antibody is C/I in active Hep B?
Ublituximab
MOA and ADRs of Dalfampridine:
lowkey khan said not really even used anymore
MOA: K+ channel blocker → increases conduction in damaged nerves
ADRs: seizure
REVIEW
For each of the following mAb, what is their target?
Natalizumab
Alemtuzumab
Ocrelizumab
Ofatumumab
Ublituximab
Natalizumab- alpha-4 integrins
Alemtuzumab- CD52
Ocrelizumab- CD20
Ofatumumab- CD20
Ublituximab- CD20