Case 6: Devi Gopal - V/Q Mismatch
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
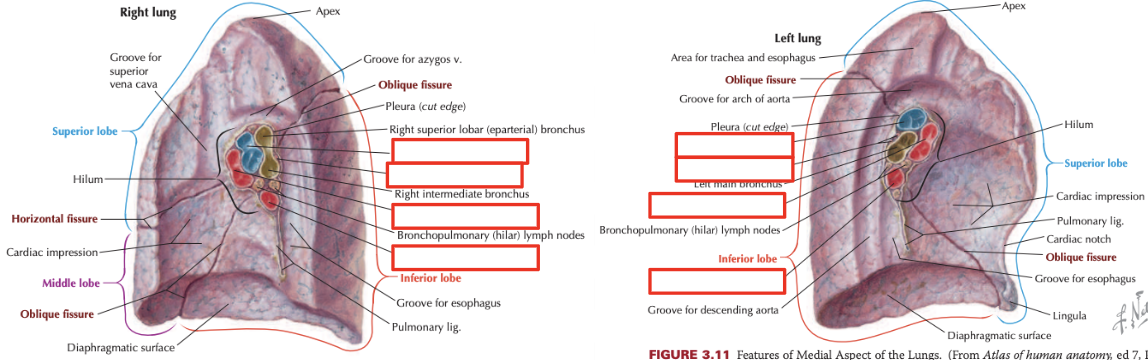
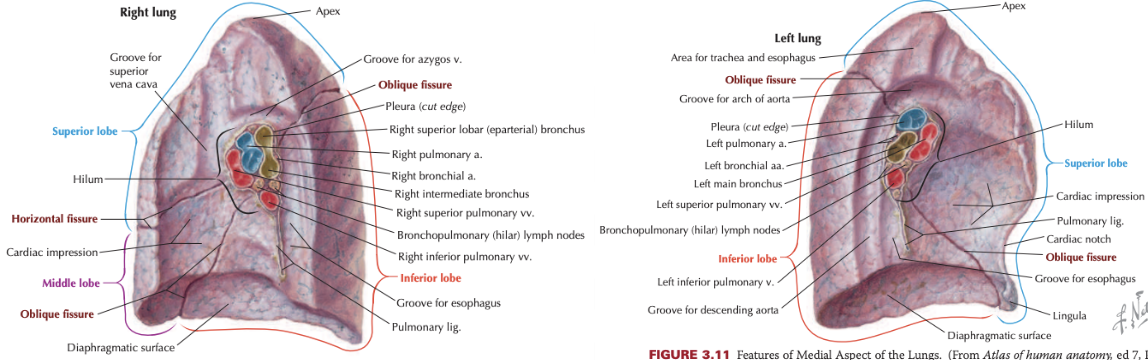
Bronchial Arteries
Supply lung parenchyma
Main bronchi has:
1 right artery
2 left arteries (superior and inferior)
Pulmonary Arteries
Thin and distensible walls
Large compliance
Accommodate large stroke volume
Deliver deoxygenated blood from systemic circulation to alveolar capillaries (gas exchange)
Pulmonary Veins
Deliver oxygenated blood from alveolar capillaries to heart (gas exchange)
Pump through systemic circulation
Blood leaves lungs (to heart) through pulmonary veins (most) and bronchial veins (some)
Pulmonary vs Systemic Circulation
Systemic: High-pressure, low-flow
Include bronchial arteries
Pulmonary: Low-pressure, high-flow
Pulmonary arteries and veins
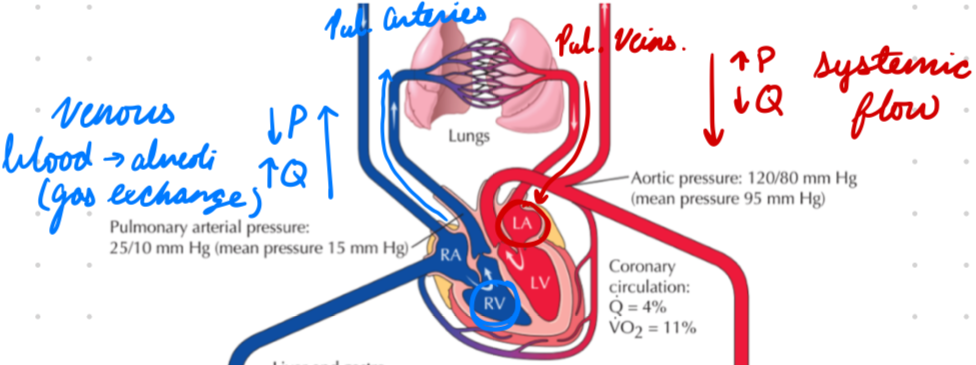
Pulmonary Capillary Pressure
Low for gas exchange
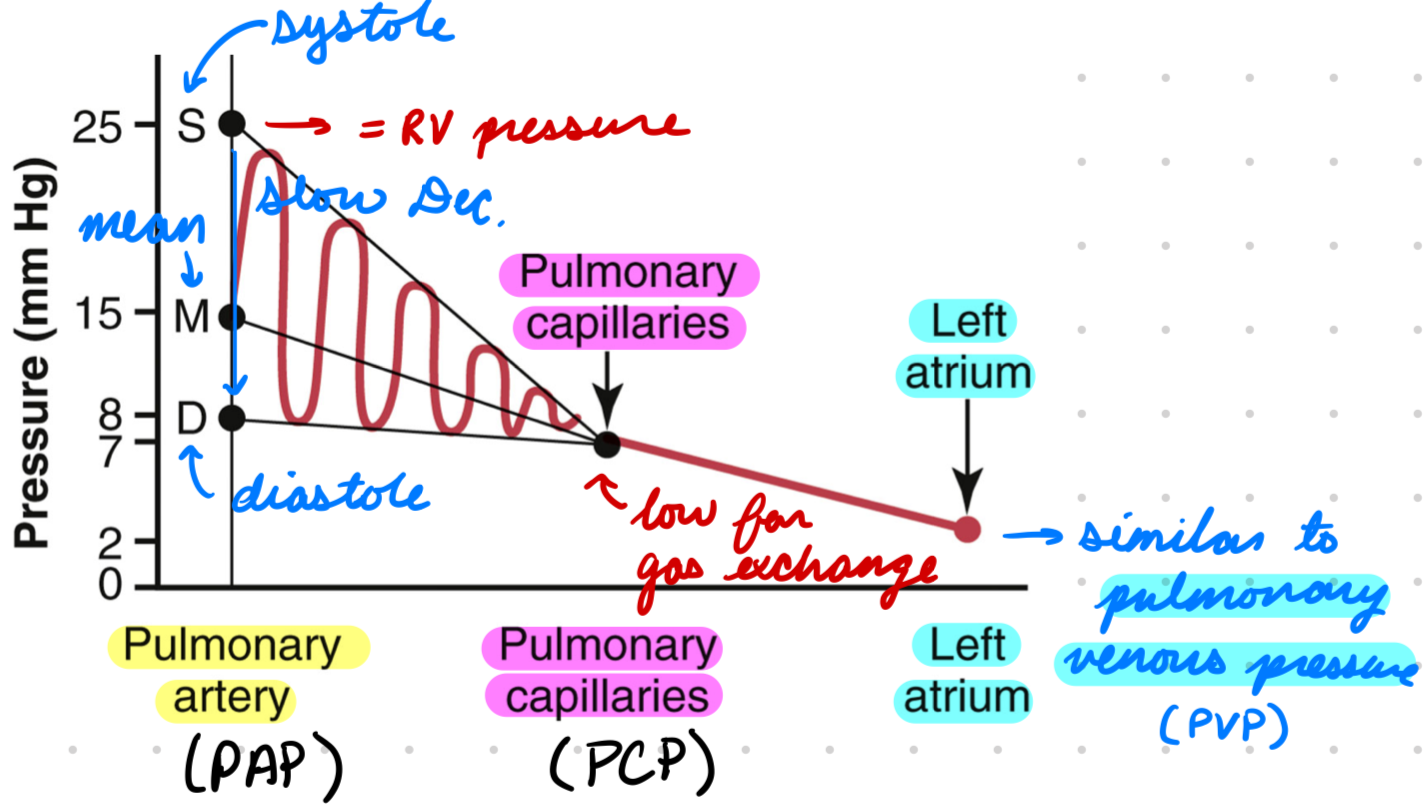
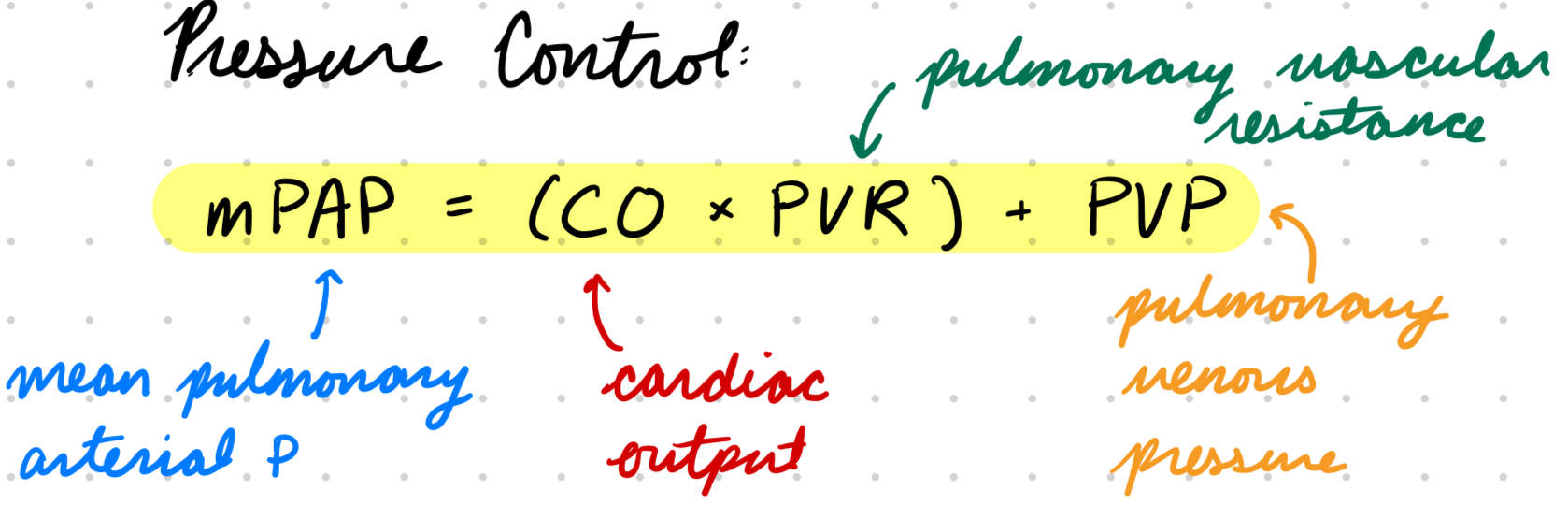
Pulmonary Pressure Control
Mean Pulmonary Arterial Pressure (mPAP) = Cardiac Output (CO) x Pulmonary Vascular Resistance (PVR) + Pulmonary Venous Pressure (PVP)
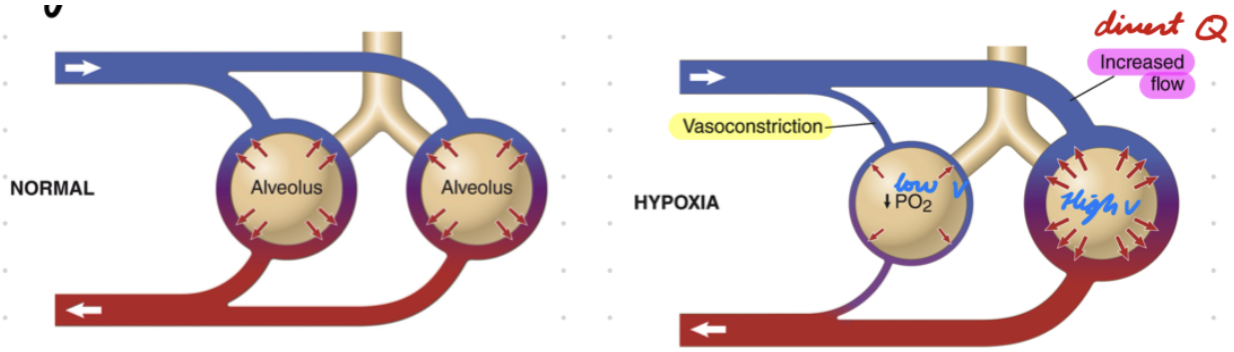
Hypoxic Pulmonary Vasoconstriction
Low PO2 (ventilation) = Alveolar vasoconstriction
Divert blood flow (Q) to well-ventilated (V) alveoli
Ventilation (V)
Air moving in and out of lungs
Dead Space Ventilation: Air entering conducting airways not in gas exchange
Alveolar Ventilation: Air entering alveolus
Perfusion (Q)
Blood flow through alveolus (gas exchange)
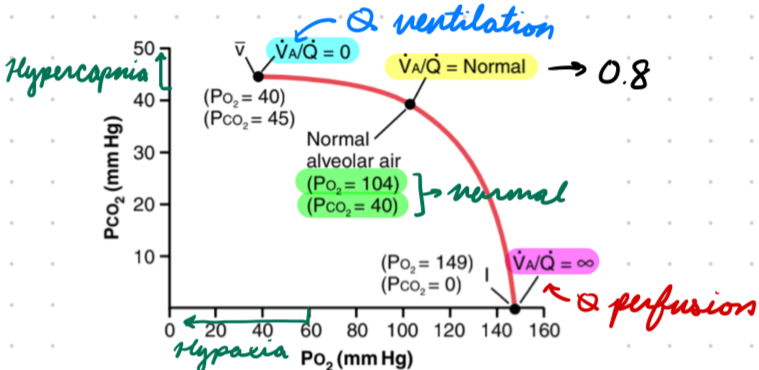
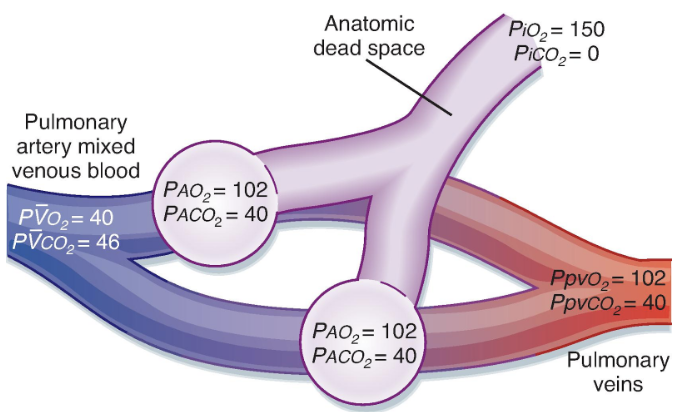
V/Q Ratio
Normal = 0.80
PO2: 104 mmHg
PCO2: 40 mmHg
Measuring V/Q
Nuclear medicine imaging techniques (V/Q scan, PET, CT)
A-a gradient
Measuring V/Q: A-a Gradient
Difference between PO2 in alveoli (PAO2) and PO2 in arteries (PaO2)
Normal Range: 5-10 mmHg (increase with exercise)
V/Q Mismatch: Increase A-a gradient
V/Q Mismatch
V/Q > or < 0.80
Decreased/no gas exchange
Low V/Q (< 0.80)
Low ventilation
Normal perfusion
Air in alveolus = Blood O2 and CO2 (no air supply)
High V/Q (> 0.80)
Normal ventilation
Low perfusion
Air in alveolus = Inspired air O2 and CO2 (no blood flow)
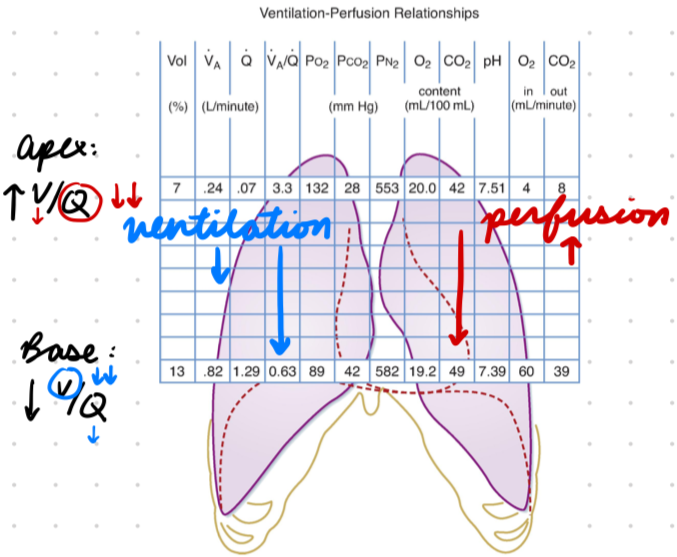
Normal Lungs
Apex → Base = Ventilation decrease and perfusion increase (relative)
V and Q low in apex
V and Q high in base
Apex:
Low Q (High V/Q)
Base:
Low V (Low V/Q)
V/Q Mismatch: Clinical Features
Hypoxemia
Increased A-a gradient
Supine position improve V/Q match
Severe:
Dyspnea
Resp distress
V/Q Mismatch: Effects on Blood Gas
Hypoxia:
Causes
Shunt
Hypoventilation (decrease alveolar ventilation = decrease PO2 and increase PCO2)
Hypercapnia:
Causes
Increase dead space ventilation
Hypoventilation
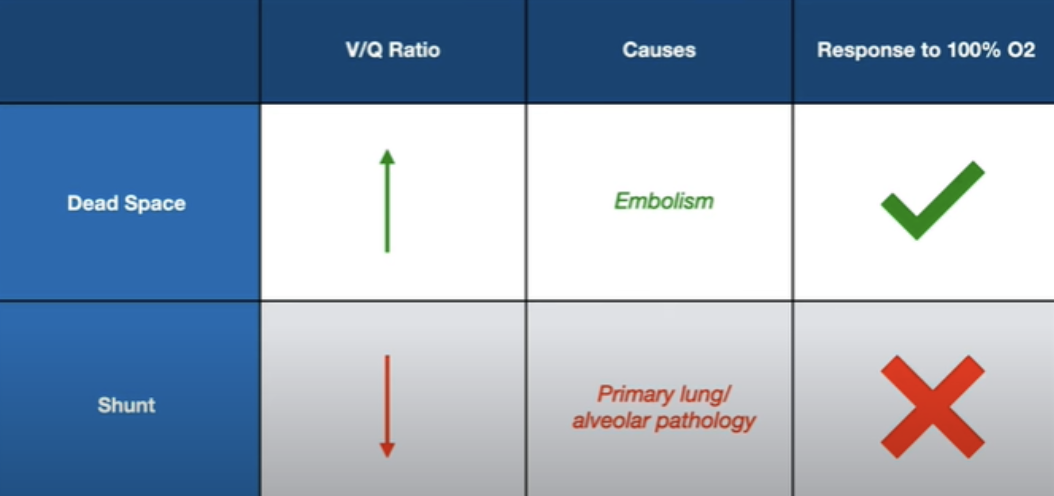
Dead Space Ventilation
Obstruction prevent perfusion to ventilated alveoli
Ventilation with no pay off
Ex: Pulmonary embolism
High V/Q
Redistribute to regions with blood flow (decrease V/Q)
Give O2 = Increase saturation
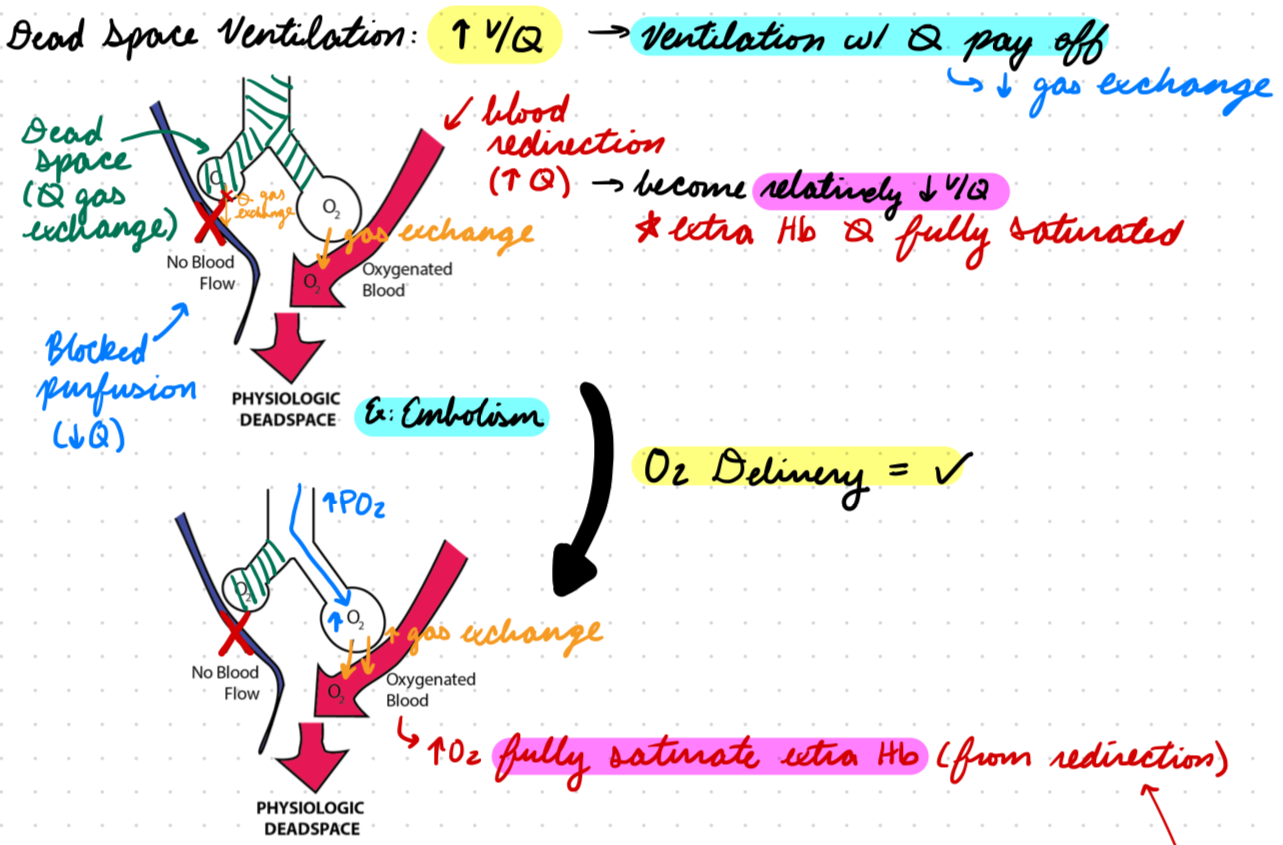
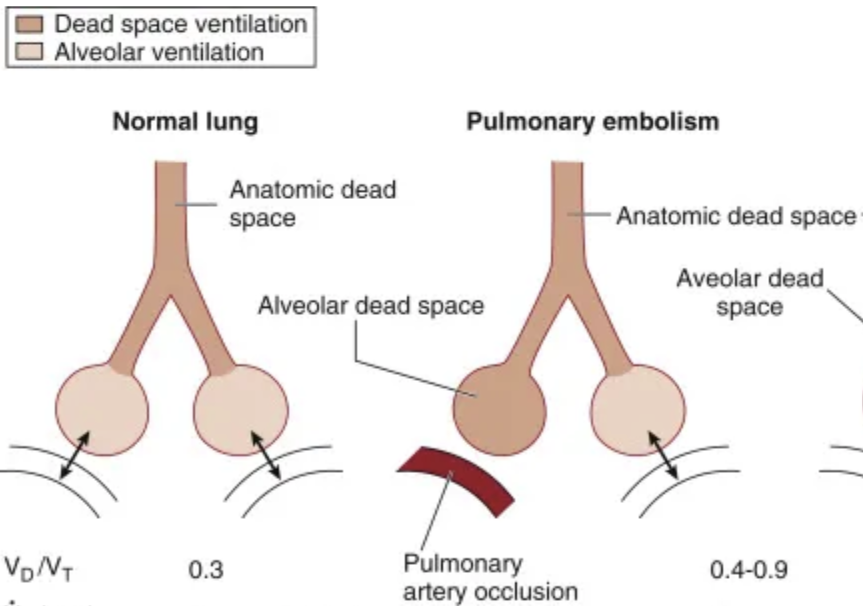
Dead Space Ventilation: Pulmonary Embolism
Blood flow obstruction in pulmonary circulation
No perfusion to ventilated area = Physiological dead space
Normal V, low Q
V/Q > 0.80
Increase CO2 retention
Shunting
Blood flow diversion prevent ventilation to perfused alveoli
Perfusion with no benefit
Low V/Q
Give O2 = Small saturation increase (shunted blood not exposed to increased O2)
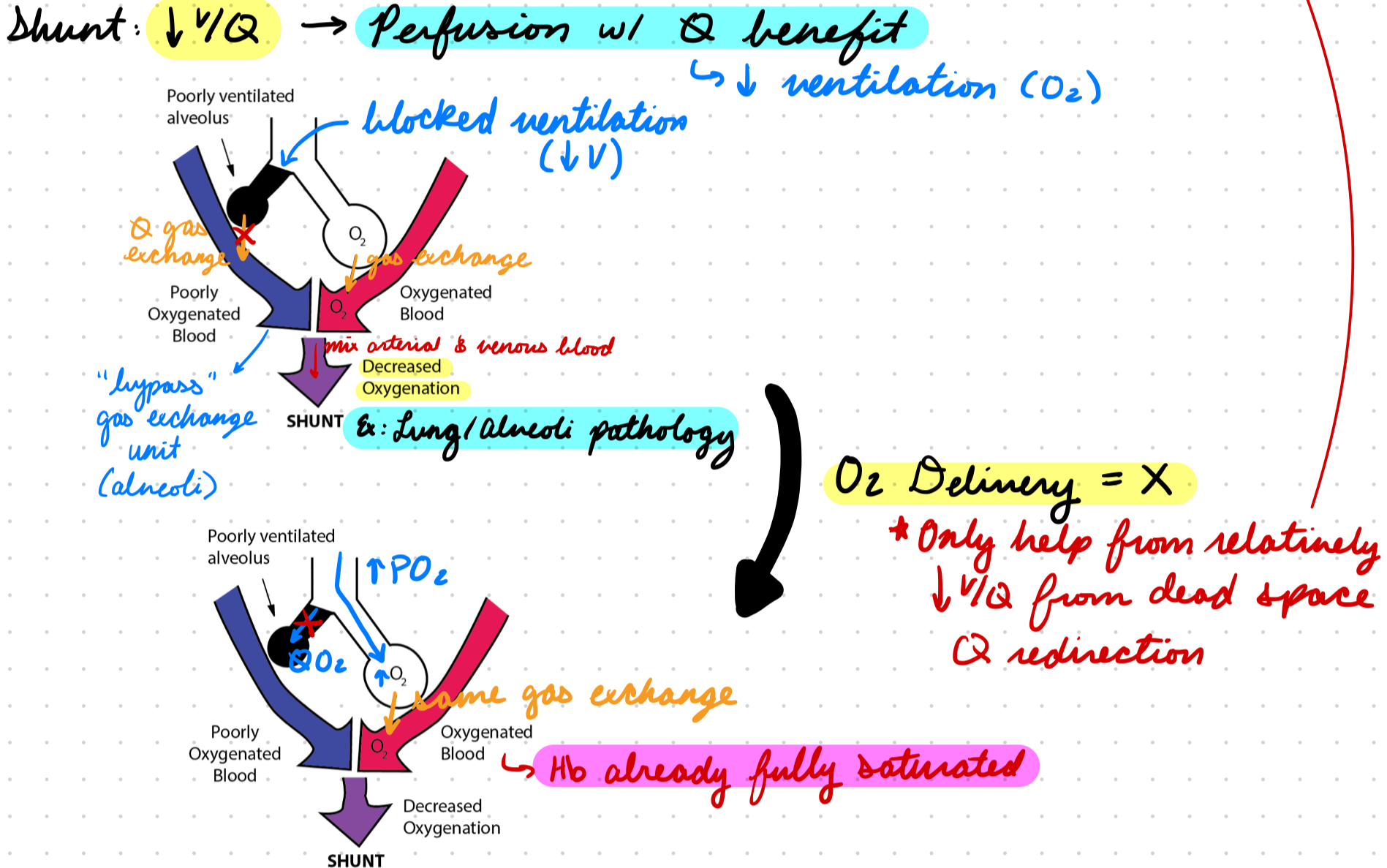
Shunting: Normal Lung Unit
Normal V and Q to both lungs (gas exchange units)
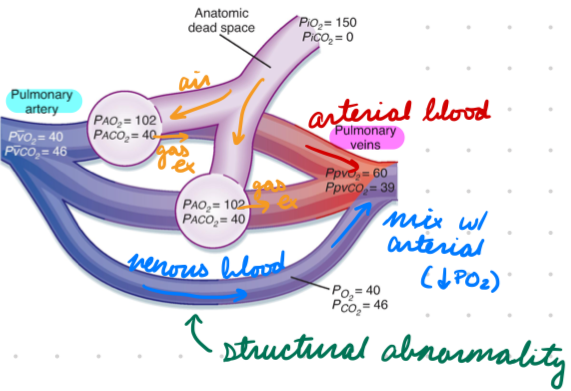
Shunting: Anatomical Shunt
From structural abnormalities
Venous blood bypass gas-exchange unit to mix with arterial blood
Low V, normal Q
V/Q < 0.80
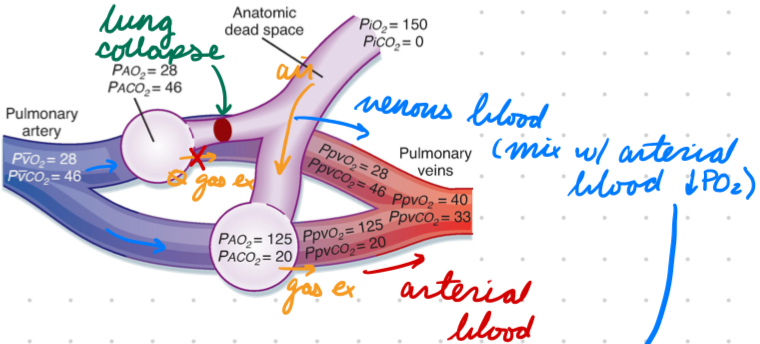
Shunting: Physiological Shunt
From ventilation blockage (lung collapse in atelectasis)
Venous blood bypass one gas-exchange unit to mix with arterial
Low V, normal Q
V/Q < 0.80
O2 Saturation
% of O2-saturated hemoglobin in blood
Arterial: 95-100%
Venous: Variable based on tissue metabolic activity
O2 Sat Measurement
Pulse oximetry (SpO2)
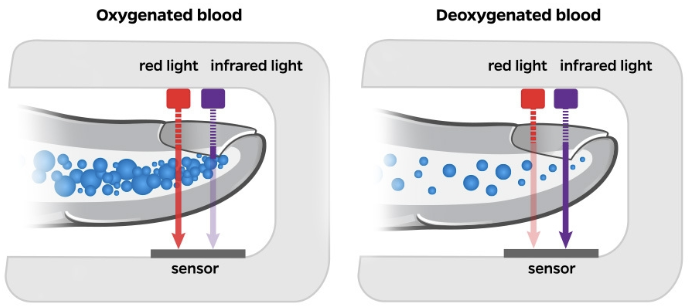
SpO2
Red/infrared light absorption determine oxygenated (O2Hb) vs deoxygenated (HHb) hemoglobin
O2Hb: Absorb infrared, red pass through
HHb: Absorb red, infrared pass through
SpO2: Inaccurate Measurements
Nail polish
Poor perfusion
CO poisoning
CO-hemoglobin indistinguishable from O2-hemoglobin
Darker skin
Overestimate at <85% (false negative for hypoxemia)