WCF exam 2
1/350
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
351 Terms
What are some fetal assessments for before and during labor?
Intermittent auscultation (IA) and electronic fetal monitoring
What is intermittent auscultation?
Listening to the fetal heart sounds at periodic intervals to assess FHR
What is electronic fetal monitoring?
Visualize FHR patterns; monitor screen or printed tracking; more sensitive than auscultation in predicting fetal compromise
What are the goals of FHR monitoring?
Looking for fetal response; identify reassuring and non-reassuring patterns
What are some factors affecting oxygenation and perfusion?
Maternal HTN or hypotension, hypovolemia, and umbilical cord compression; ALL lead to decreased O2 and perfusion
What are some external fetal monitoring devices?
For FHR, ultrasound transducer; for uterine contraction (UCS), tocotransducer
What are some ways to do internal fetal monitoring?
Can be continuous and invasive; fetal spiral electrode (FSE) and intrauterine pressure catheter (IUPC)
When looking at the display for fetal monitoring, what do the vertical red lines represent?
One minute
On the display, there are two different lines being monitored. What is the top monitoring and what is the bottom monitoring?
Top is monitoring fetal heart tracing, and the bottom is monitoring uterine activity
What is the baseline in fetal heart monitoring?
Where the tracing lies (on or between two lines); average FHR over 10 minutes (round to nearest 5 BPM)
What are some abnormal baselines?
Tachycardia and bradycardia
What is tachycardia in fetal heart monitoring?
Baseline more than 160BPM for duration of 10 minutes or longer
What is bradycardia in fetal heart monitoring?
Baseline less than 110BPM for duration of 10 minutes or longer (check maternal HR)
What is the minimal baselines FHR variability?
2-5 BPM
What is a moderate FHR variability?
5-25 BPM
What is a marked FHR variability?
Greater than 25 BPM
What is an absent amplitude range?
Undetectable
What are the most concerning variabilities?
Absent and marked variability
What are accelerations for full terms?
Greater than 15bpm rise for at least 15 seconds, less than 10 minutes with fetal movement; means mature autonomic system
What happens to the fetal heart rate during contractions?
A drop in O2 signals sympathetic stimulation, increasing HR
What are the four types of decelerations?
Early, late, variable, and prolonged
Which type of decelerations are considered normal or anticipated?
Early and variable
What are early decelerations caused by?
Head compression, vagal response, sign of progress; no need to intervene
What constitutes an early deceleration?
Decel less than 2 minutes, more than 30 seconds from start to finish; gradual decrease with onset of contraction; resolves before contraction has ended
What causes a variable deceleration?
Cord can be compressed in a variety of ways, can be persistent after rupture of membranes; first intervention is to reposition patient
What constitutes a variable deceleration?
Less than 30 seconds from start to finish, abrupt decrease in FHR below the baseline is 15bpm or more, lasts at least 15 seconds; returns to baseline in less than 2 minutes from the time of onset
What causes late decelerations?
Uterus, placenta and maternal circulation; insufficient delivery of oxygen to fetus
What constitues a late deceleration?
Decel less than 2 minutes, more than 30 seconds from start to finish; gradual decrease with LATE onset and begins after the peak of the contraction; doesn’t resolve until after the contraction has ended
What constitutes a prolonged deceleration?
Decel more than 2 minutes but less than 10 minutes
What are some interventions with late and prolonged decelerations?
Reposition, IV fluids, and oxygen
FHR changes and causes mneumonic
VEAL CHOP
What does VEAL CHOP stand for?
V: variable C: Cord compression (Caution)
E: Early H: Head compression (good sign!)
A: accelerations O: Oxygenation (Good sign)
L: Late P: Placenta (poor perfusion)
What are some interventions for variable FHR changes?
Reposition, amnio infusion
What are some interventions with early FHR changes?
Document, check progress, continue to monitor
What is considered a normal FHR interpretation?
Baseline FHR 110-160 BPM, moderate variability, accelerations, NO late or variable decelerations, may have early decelerations
What is considered an indeterminate FHR interpretation?
Tachycardia, bradycardia, minimal variability, absent variability without recurring decelerations, marked variability, absence of accelerations after stimulation, recurrent variable decelerations with minimal/moderate variability, prolonged decelerations less than or equal to 2 minutes but less than 10 minutes, recurrent late decelerations with moderate variability, and variable decelerations with other characteristics such as slow return to baseline
What is considered an abnormal FHR interpretation?
Sinusoidal pattern OR absent variability with one or more: recurrent late decelerations, recurrent variable decelerations, and bradycardia
What are three components that can affect FHR?
Frequency, duration and intensity of contractions
What is tachysystole?
Greater than 5 contractions in 10 minutes, leading to fetal distress
What is the 6 week phase postpartum called?
Puerperium or 4th trimester
How often should vitals be checked for a patient who had a vaginal birth?
Every 15 minutes for 2 hours, every 4 hours for 8 hours, and then every 8 hours until discharge
How often should vitals be checked for a patient who had a c-section birth?
Every 30 minutes for 4 hours, then every hour for 3 hours, then every 4-8 hours
What is the postpartum maternal assessment mnemonic?
BUBBLE-HE(B) or BUBBLE-LE(B)
What does BUBBLE-H/L E(B) stand for?
Breasts, uterus, bladder, bowel, lochia, episiotomy, Homan’s Sign/Legs, emotional support, and bonding
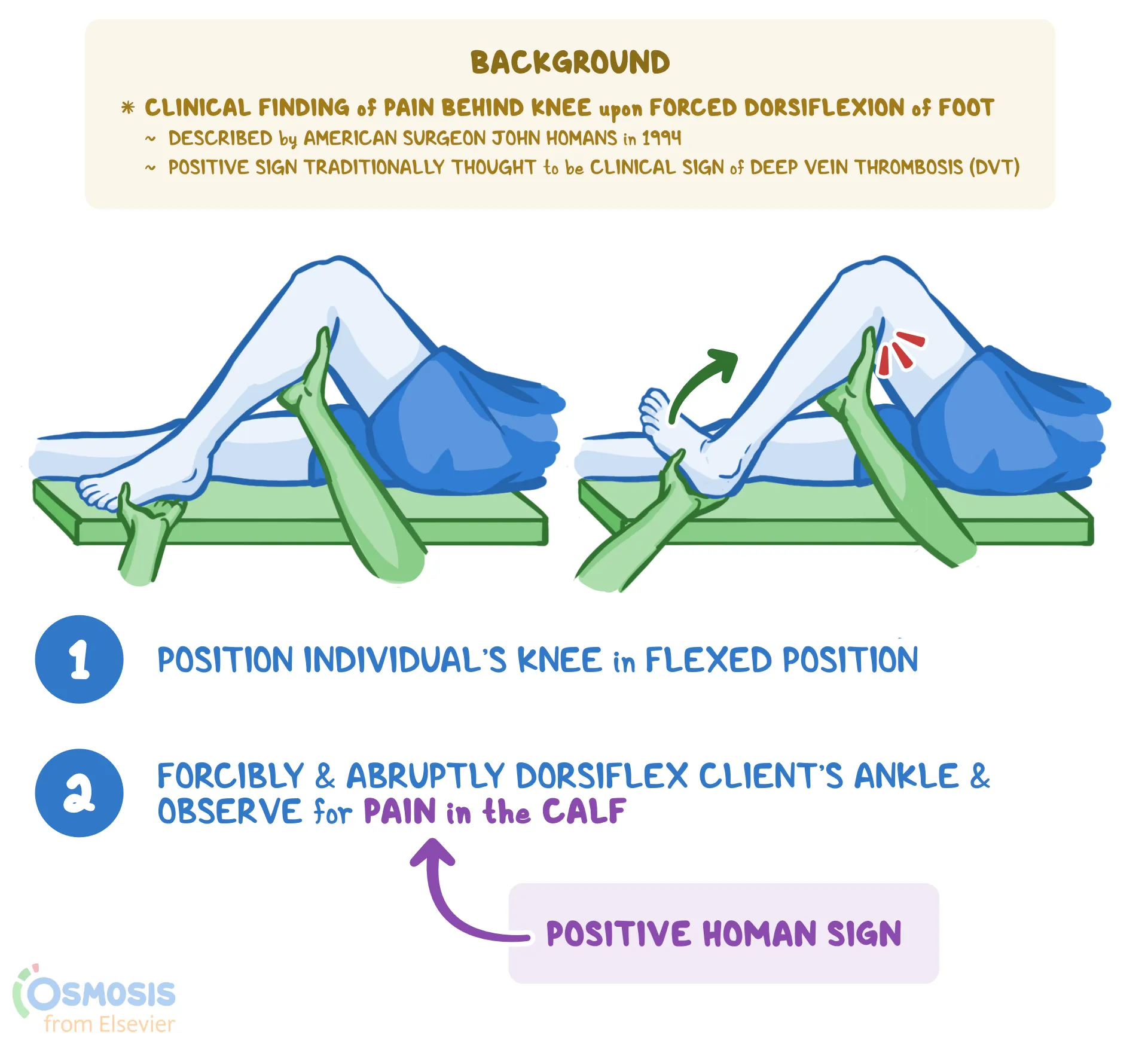
What is Homan’s sign?
A test for DVT; Considered positive for DVT when flexing the ankle and pain is felt in the calf
What is colostrum?
Yellowish/gold fluid from nipples, usually heavily recommended for newborns to have this when first born
General education for breastfeeding patients
Tenderness can be expected, lanolin cream or milk for dry/cracked nipples, use minimal soap/water on nipples, air dry after feedings, should NOT be painful,
General education for non-breastfeeding patients
Wear a supportive bra, get ice packs to axillary area, ibuprofen or acetaminophen can be taken for discomfort; educate, use safe water source, mix according to directions
What are some interventions for engorgement for breastfeeding parents?
Massage breasts before and during feedings, cold compresses after the swelling; starts within 48-72 hours and resolves within 4-5 days
What are some interventions for engorgement for non-breast feeding parents?
Resolves spontaneously, discomfort decreases within 24-36 hours, breast binder or tight bra, ice pack, mild analgesics for pain, avoid stimulation, cool washcloths, and cabbage leave
What is mastitis?
Blocked milk duct/bacteria, unilateral breast involvement; fever usually occurs; rarely occurs in first two weeks postpartum; treatment is moist heat, increased fluid intake, tylenol/motrin; continue to breastfeed
What is involution?
Normal; Return to non-pregnant state following birth
What is subinvolution?
Abnormal; uterus is not decreasing in size, retained placental fragment can produce progesterone; pelvic infection; must have follow up appointment to monitor
What are the S/S of subinvolution?
Prolonged lochial discharge, irregular to excessive bleeding, sometimes hemorrhage; give Methergine PO
What is some patient education regarding afterpains from delivery?
Most severe 2-3 days after delivery, similar to menstrual cramps; multiparas and patients with larger uterine distention experience more vigorous contractions; ibuprofen or naproxen
What is the leading cause of maternal morbidity and mortality?
Postpartum hemorrhage (PPH)
Early vs late PPH
Early is first 24 hours after delivery, late is 24 hours to 12 weeks after delivery
What are the PPH estimated blood loss (EBL) of vaginal deliveries?
More than 500 mL
What are the PPH EBL of Cesarean deliveries?
More than 1000 mL
How much do HCT levels need to drop for PPH dx?
10%
What is one way to treat PPH?
RBC transfusion
What are the four T’s of PPH?
Tone, trauma, tissue, and thrombin
What is uterine atony?
Uterus does not contract after childbirth; caused by pitocin use during induction or augmentation of labor, over distended uterus, obesity, prolonged labor, previous history, trauma during birth, manual placental removal, and use of anesthesia
What does uterine atony look like?
Intermittent/continuous dark red blood cells with clots, uterus soft and boggy
What areas can have trauma that causes a PPH?
Uterus, perineum, vagina, and cervix
How do you identify a PPH caused by trauma?
Steady, bright red blood - no clots, uterus contracted
What should be done with the placenta after delivery?
Carefuly examine, ensure that it is not fragmented; might need manual removal; more common with late post partum
What are hematomas?
Collection of blood that has pooled outside of a blood vessel; may fill with 250-500mL of blood rapidly
What is thrombocytopenia?
Reduced thrombin, leading to delayed blood clotting
What is some management and care interventions for PPH?
Palpate fundus for location, tone and lochia and massage if boggy; express clots, not elength of time to saturate pad; assess perineum for hematoma, unrepaired lacerations; empty bladder (bedpan, straight cath or foley)
What are some medications given for PPH?
IV large bore 18G rapid infusion of 1L of fluids (NS or LR), oxytocin 20-40 units/1L, restore blood volume, O2 10-12 L/min for compromised perfusion
What are some medications that increase uterine tone?
Pitocin IV (bolus rapidly), cytotec PR (use lubricating jelly), methergine IM (DO NOT give to hypertensives), hemabate IM (DO NOT give to asthmatics)
What does oxytocin (pitocin) do?
Stimulates contractions (uterine smooth muscle); first line for PPH; bolus can lead to hypotension and cardiac arrythmias
What does methylergoovine maleate do (methergine)?
Stimulates contractions (uterine and vascular smooth muscles); do not mix with other meds, and don’t administer if there’s a hx of HTN or current high BP
What does carboprost tromethamine (hemabate) do?
Stimulates contractions (myometrium); VERY expensive; do not administer if patient demonstrating S/S of shock; DO NOT ADMINISTER IF ASTHMA
What does misoprostol (cytotec) do?
Stimulates powerful contractions (myometrium); rectal is much slower than IV; do NOT administer if sensitive to prostaglandins
What does dinoprostone (prostin E2) do?
Stimulates powerful contractions (myometrium); if vaginal bleeding, vaginal suppository likely ineffective; fever is common; do NOT administer if sensitive to prostaglandins and/or has severe HTN
What are some rapid interventions to prevent hypovolemic shock?
Restore blood volume and treat cause of hemorrahge?
What are the classic signs of hypovolemic shock caused by PPH?
Maternal dyspnea, tachycardia, thready pulse; dropping BP, increasing HR
What are some nursing interventions for shock?
Summon help, especially anesthesia; MASSAGE FUNDUS; assess patient’s risk factors; rapid infusion of crystalloids (NS/RBCs); check airway (O2) and monitor status
What are some ways to increase comfort for postpartum bowel movements?
Increase water intake, take sitz baths, use stool softeners, take walks, eat healthy, and don’t ignore the urge!
What is lochia?
Discharge
What are the colors lochia can be?
Rubra (dark red, lasts 3-4 days), serosa (pink/brown, lasts 4-10 days), and alba (whitish-yellow, lasts 10-28 days)
What do you check for when a patient has an episiotomy, vaginal tearing, and/or hemorrhoids?
REEDA: redness, edema, ecchymosis, discharge, and approximation
How long does it take for vaginal tears to heal?
6 weeks (vag)
How long does it take for an episiotomy to heal?
2-3 weeks
How long does it take for hemorrhoids to heal?
6 weeks (hem)
What are some nursing interventions for perineal discomfort?
Assess perineum for hematoma, bleeding, S/S of infection; ice packs, ice filled glove wrapped in wash cloth, peri bottle, sitz baths to start after first 24 hours; instruct patient nothing in vagina for a minimum of 6 weeks; kegel exercises
What are some risk factors for postpartum depression (PPD)?
Chronic/prenatal depression, low self-esteem, stress of childcare, prenatal anxiety, life stress, lack of social support, hx of depression, multiple births/fatigue
What is postpartum psychosis?
Abnormal depression, delusions, thoughts of harming infant or self, usually evident in first 8 weeks; psychiatric emergency, hospitalization and medical management necessary; most improve with treatment
What are the signs/symptoms of postpartum psychosis?
Hallucinations, delusions, agitation, confusion, disorientation, sleep disturbances, loss of touch with reality, possible suicide and/or infanticide
What is the treatment for postpartum psychosis?
Antidepressants, antipsychotics, anti-anxiety meds and long term therapy
What is phase 1 of the mothering role?
Taking in; 1-2 days; recovering from immediate exhaustion of labor, relatively dependent on others to meet physical needs
What is phase 2 of the mothering role?
Taking hold; day 2-3; starts to initiate action and to begin some tasks of motherhood
What is phase 3 of the mothering role?
Letting go; weeks 2-6; mother is redefining her new role, able to focus on partner, other children, and family issues
How is the endocrine system affected postpartum?
70% menstruate within 12 weeks, may ovulate before first menstrual cycle
How is the cardiovascular system affected postpartum?
Delivery of the baby, expulsion of the placenta, and loss of amniotic fluid can create cardiovascular instability; cardiac output generally returns to normal within 2-4 weeks after birth; BP after birth could be due to hemorrhage
What are two vaccines recommended for mothers?
Rubella vaccination, either before or after pregnancy, and Rh isoimmunization given within 72 hours for Rh-negative patients who deliver Rh-positive infants
What should discharge teaching include?
Infant feeding and bathing, breastfeeding, perineal hygiene, physical activity/rest, and emotional changes
When preparing for birth, what are things needed to prepare?
Radiant warmer, resuscitation equipment, medications, and prenatal hx/complications and labor course