Fluorescein Staining Patterns
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
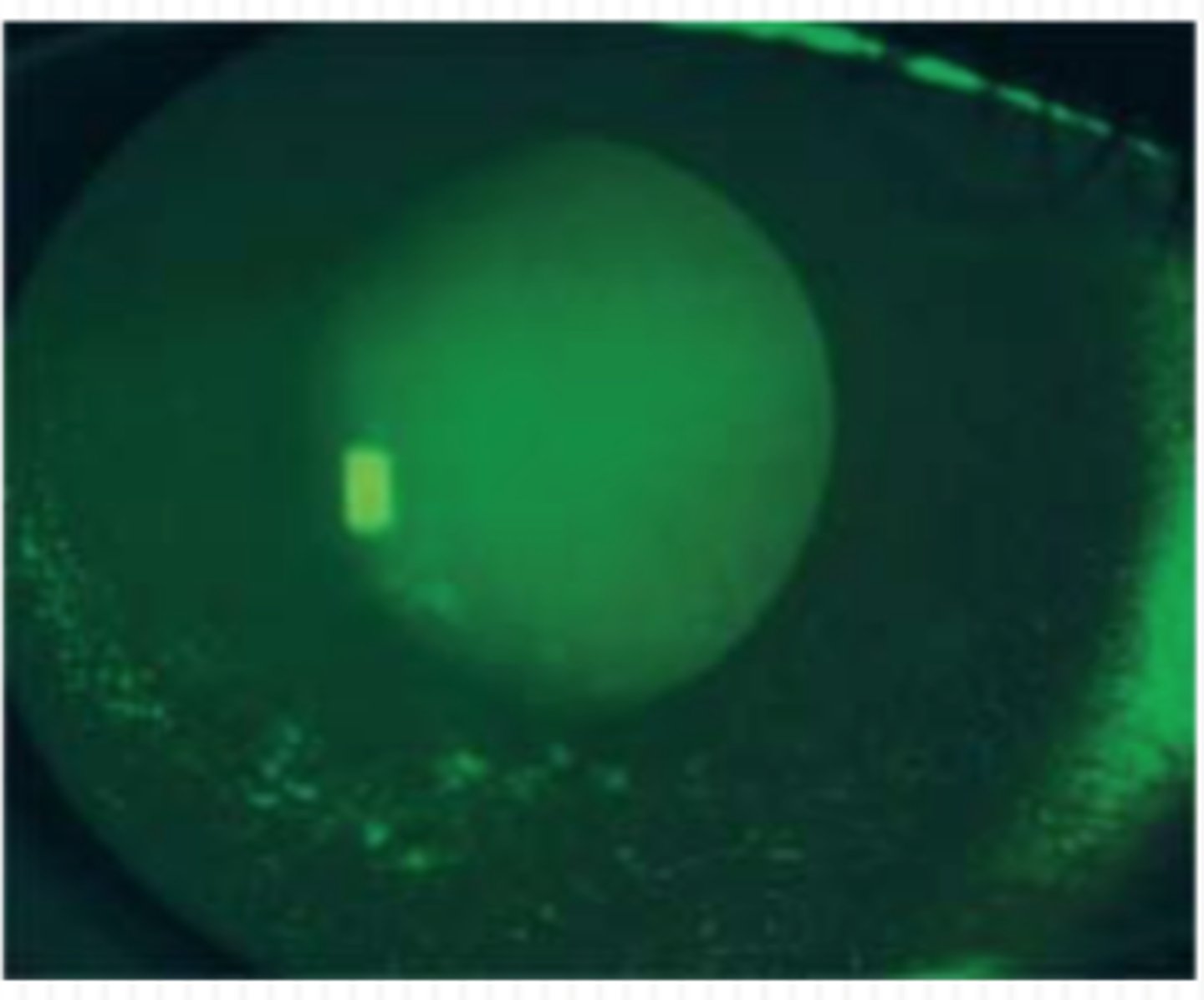
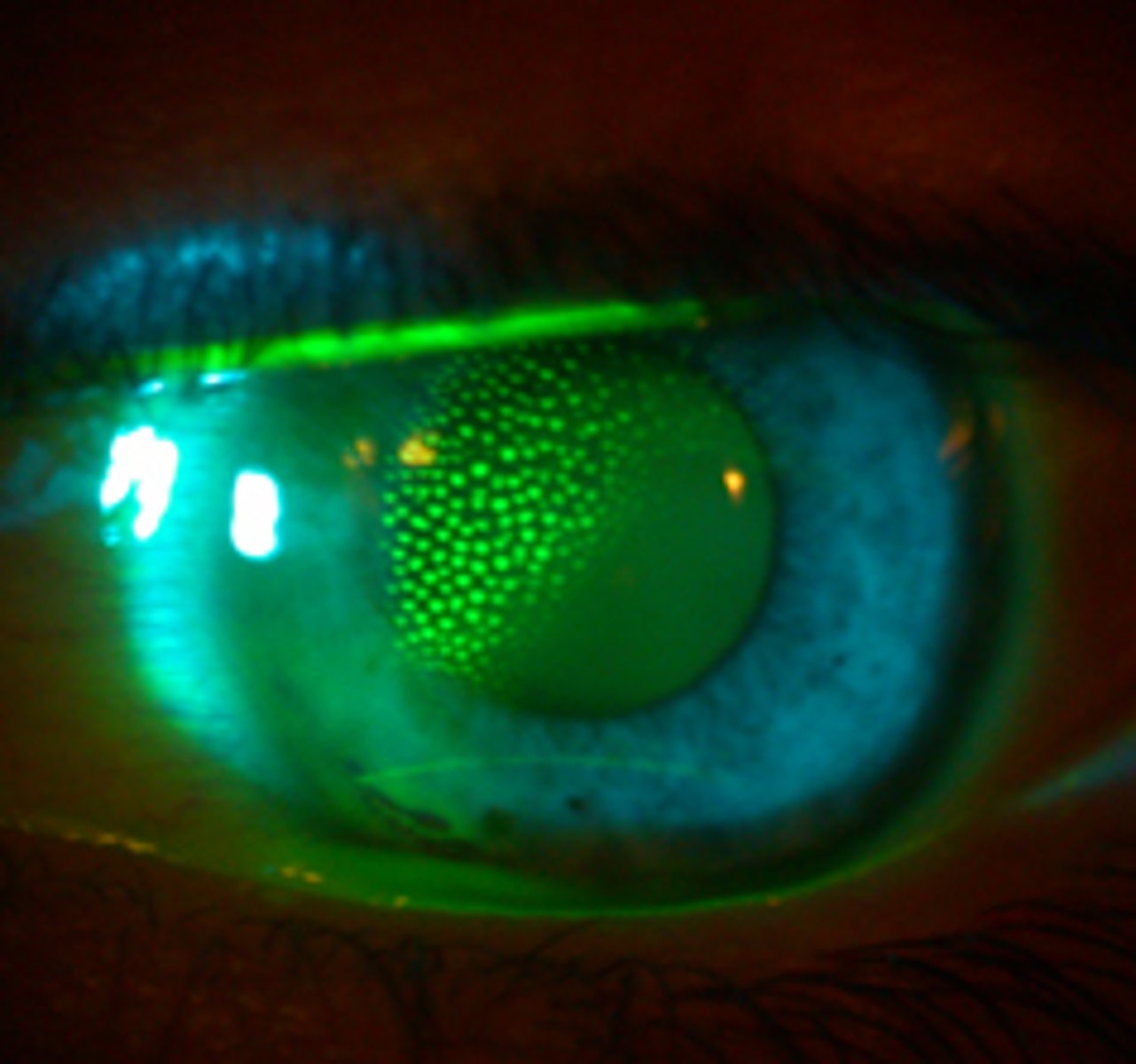
Superficial Punctate Keratitis (SPK)
Isolated or diffuse dots across a larger area of the cornea. An isolated pattern may be due to a poor contact lens fit or infection, while a diffuse pattern may indicate solution toxicity or an interaction between certain lens/solution combinations or dry eye syndrome.
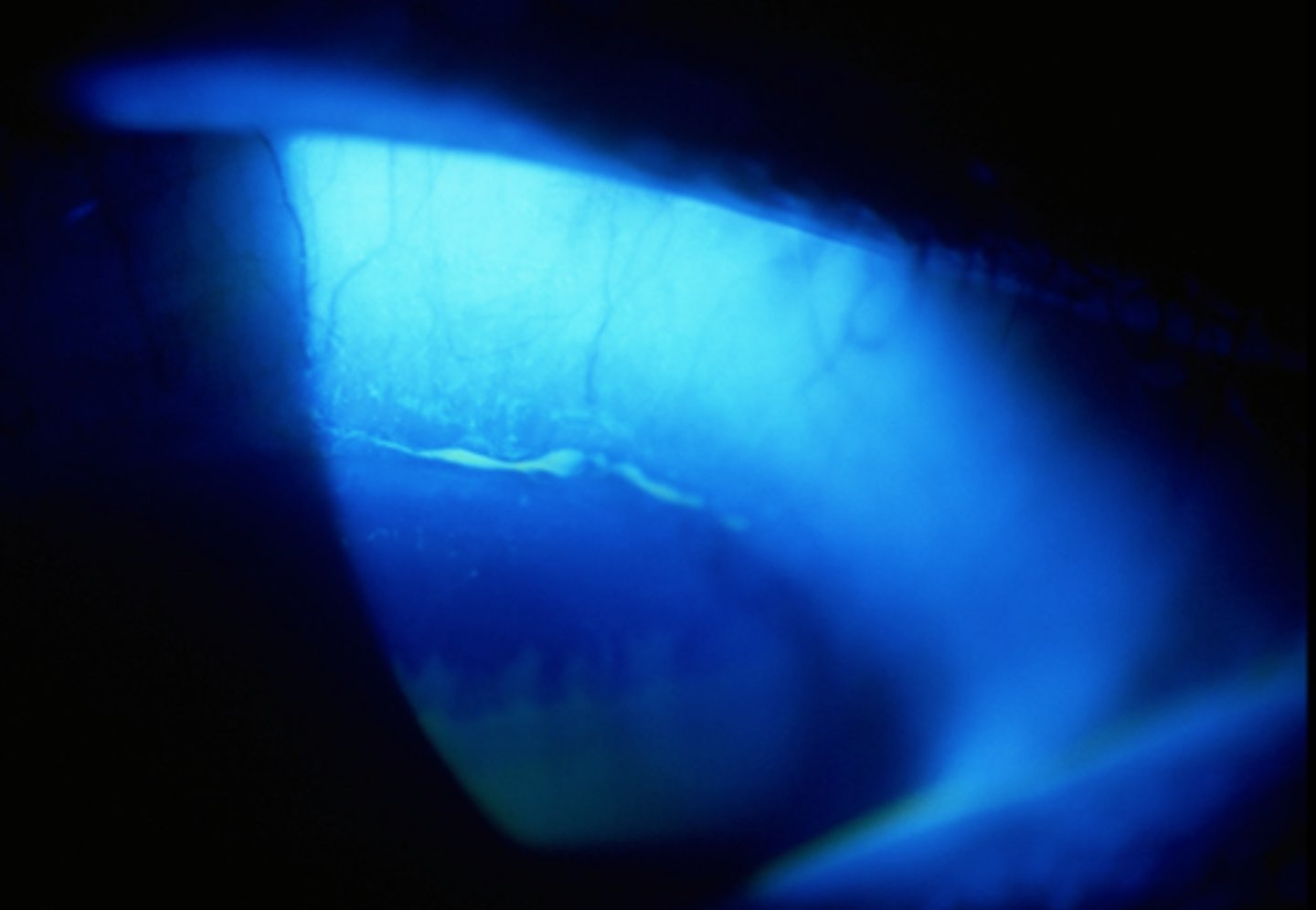
Superior epithelial arcuate lesion (SEAL)
present parallel to the superior limbus and are due to mechanical chaffing by a contact lens on the superior cornea. The patient is usually asymptomatic.
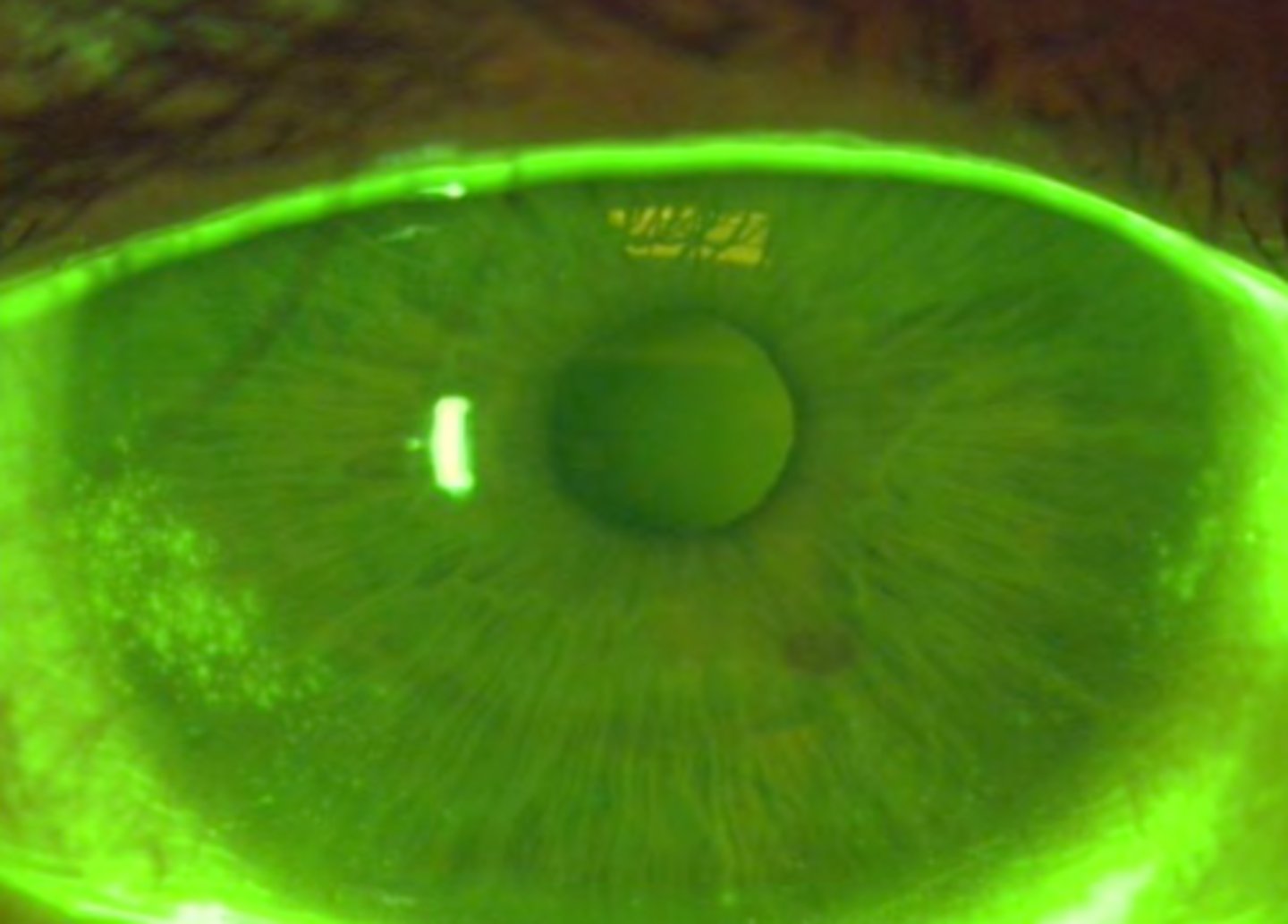
Inferior arcuate staining
presents parallel to the inferior limbus and is due to dehydrated contact lenses associated with insufficient post-lens tear film. Patients may have complaints of mild discomfort.
Three and nine o'clock staining
presents parallel to the nasal and temporal limbus and is due to contact lens associated dry eye. Patients may experience mild discomfort.
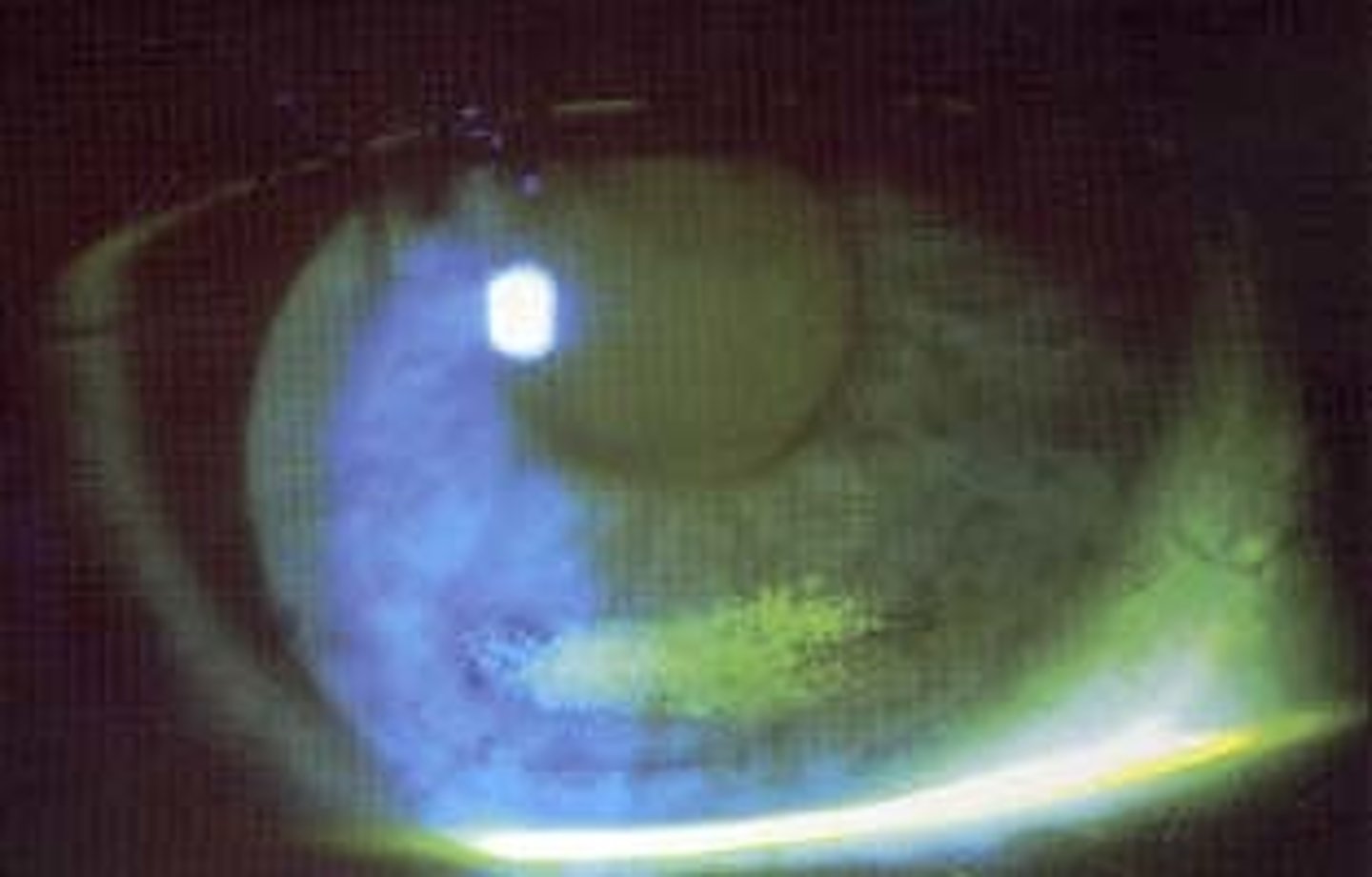
Dimple veil staining
not true staining, but rather pooling of the dye into corneal indention caused by trapped air bubbles under a poorly fitting rigid gas permeable contact lens. It presents as sharply demarcated, circular patterns of stain on the cornea.
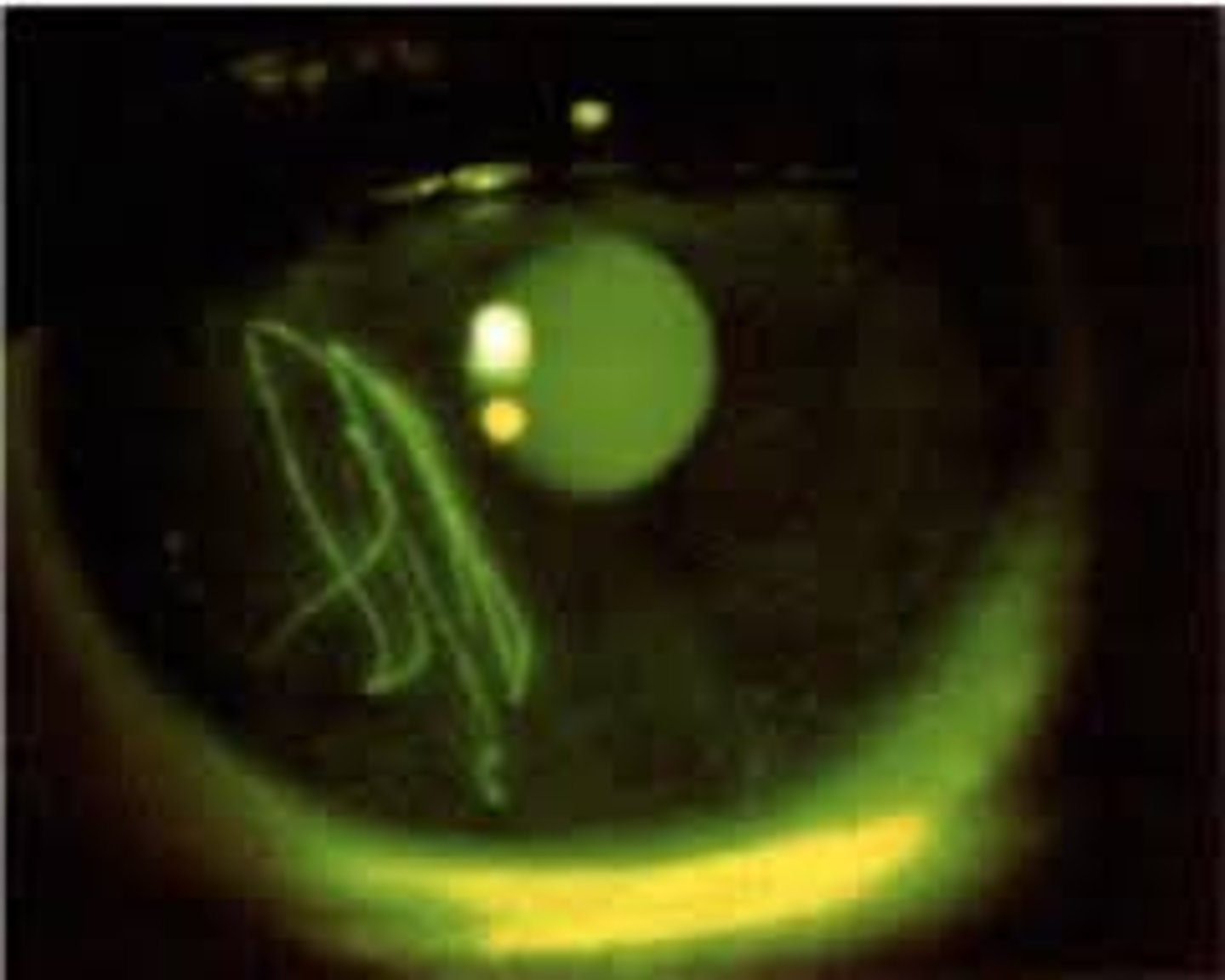
Foreign body staining
or mechanical trauma can present in various ways, such as a zigzag-shaped abrasion or as the outline shape of an embedded foreign body.
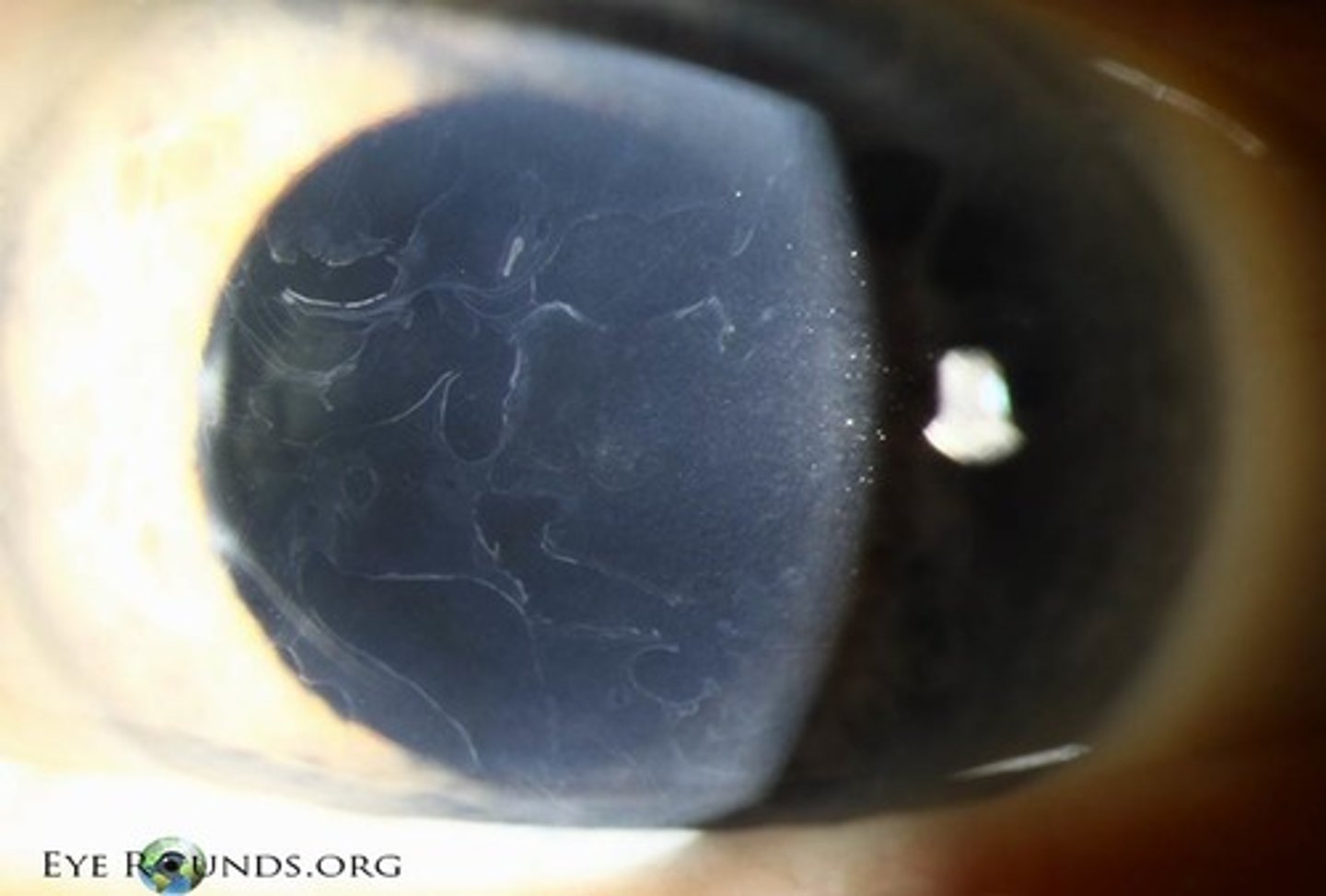
Epithelial Basement Membrane Dystrophy (EBMD)
raised dots, maps and fingerprints and results in negative staining. The elevations of the ocular surface, result in an immediate tear film break-up over the corresponding area. Patients are usually asymptomatic unless the dots, maps and fingerprints erupt, at which time they will stain positively and become symptomatic
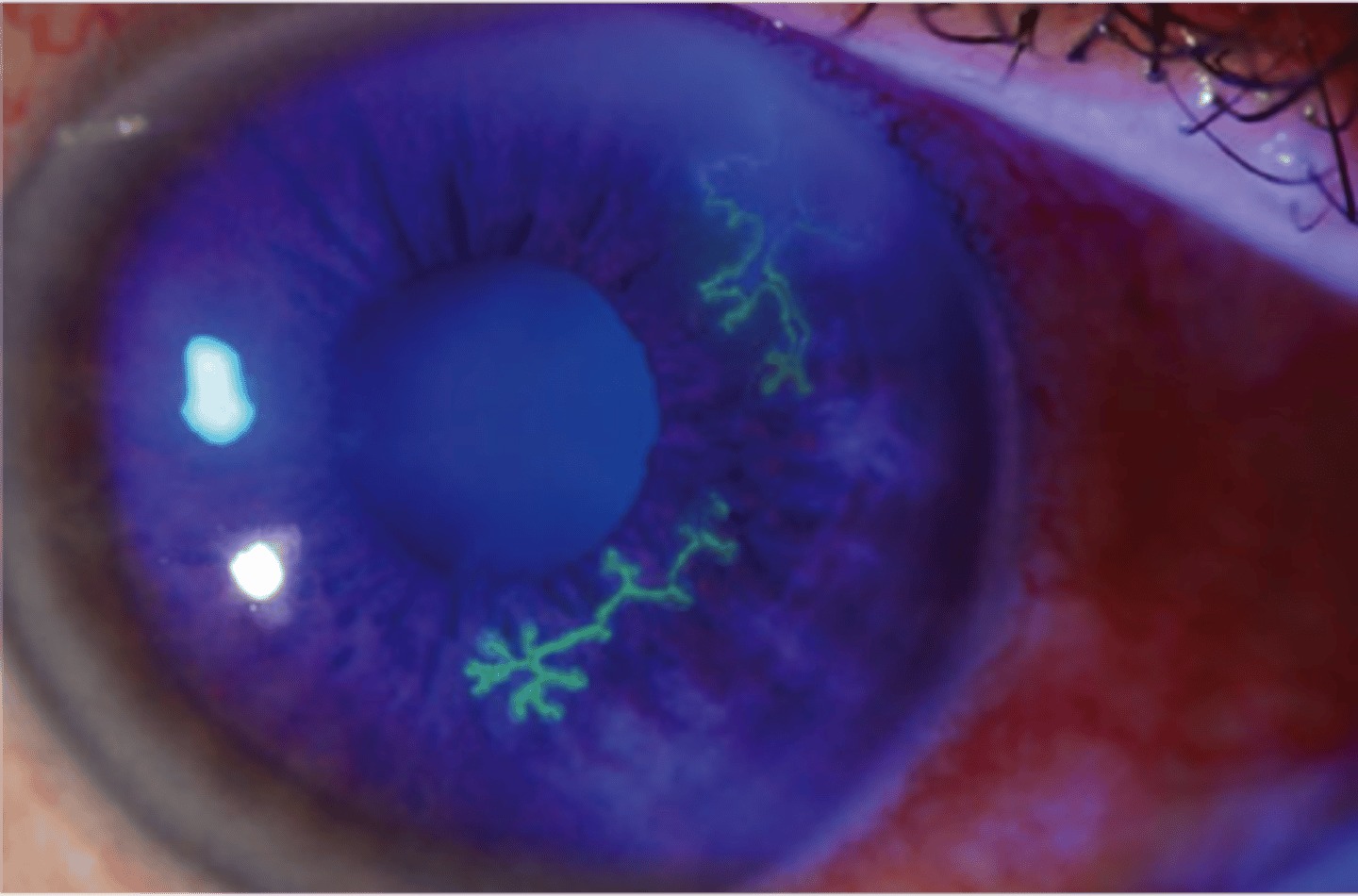
Herpetic Keratitis
Dendritic ulcers are associated with the herpes simplex virus (HSV). The edges may be slightly elevated due to swollen epithelial cells.
Use fluorescein to stain the:
cornea
Use lissamine green to stain the:
conjunctiva, even in your asymptomatic patients.
Alignment fit
Back surface of lens matches the curvature of the cornea
Clearance
(STEEP) There is space between the lens and the cornea
Touch
(FLAT) The lens is close to the cornea, compared to another part of the lens
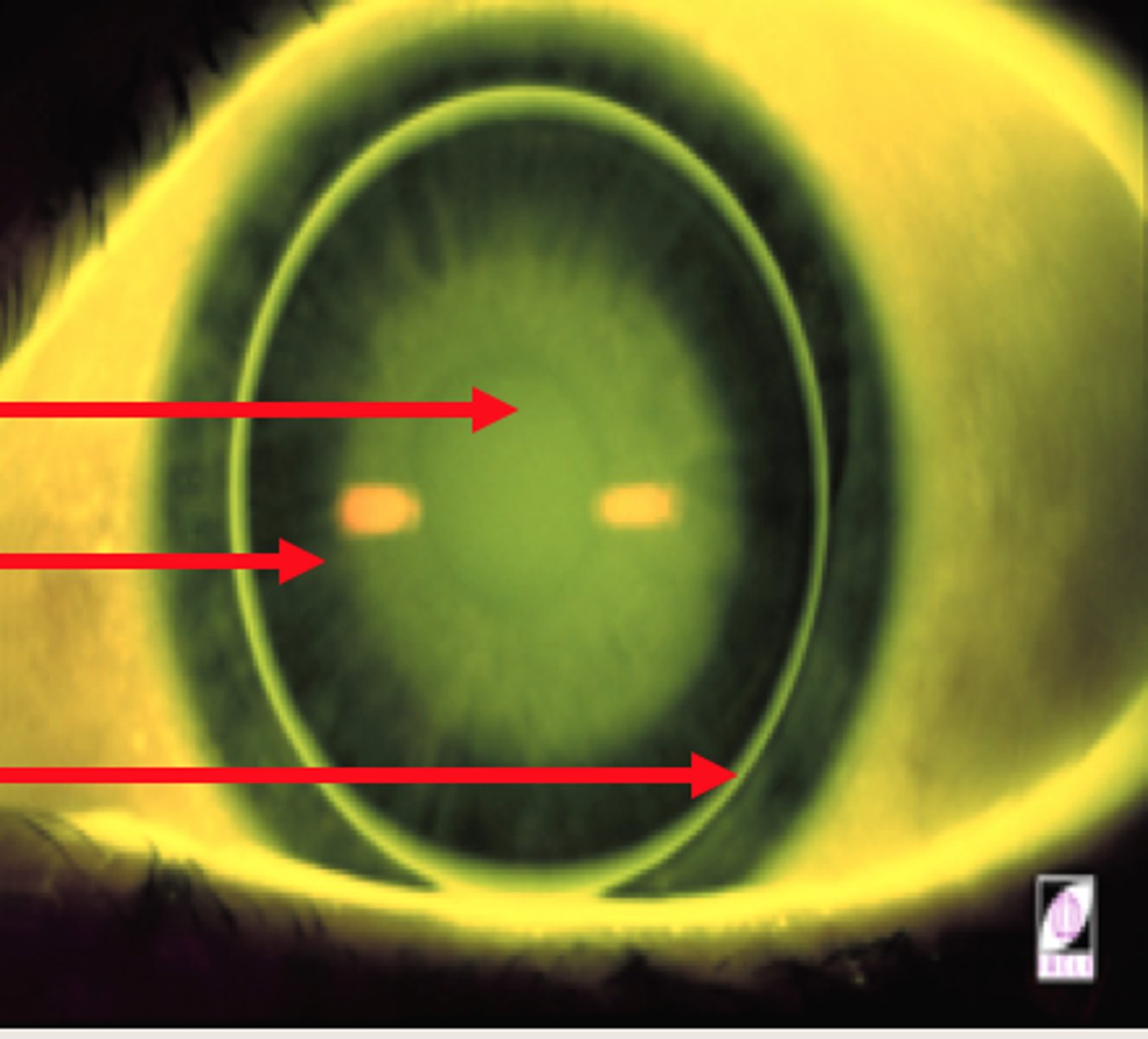
Apical
-Central portion of FP
-Area under optic zone
Mid-peripheral
-Area under the intermediate curves
-Determines lens positioning and movement patterns
Peripheral
-Area under peripheral curves
-Determines tear exchange
Static pattern
-FP when lens is centered on the cornea
-If lens de-centers, use PT lids to manually center
-Gives true apical relationship
Dynamic pattern
-FP when lens is in normal resting position
-May be different than static pattern
-pattern not as flat as when centered because peripheral cornea is flatter.
Apical Alignment (AA)
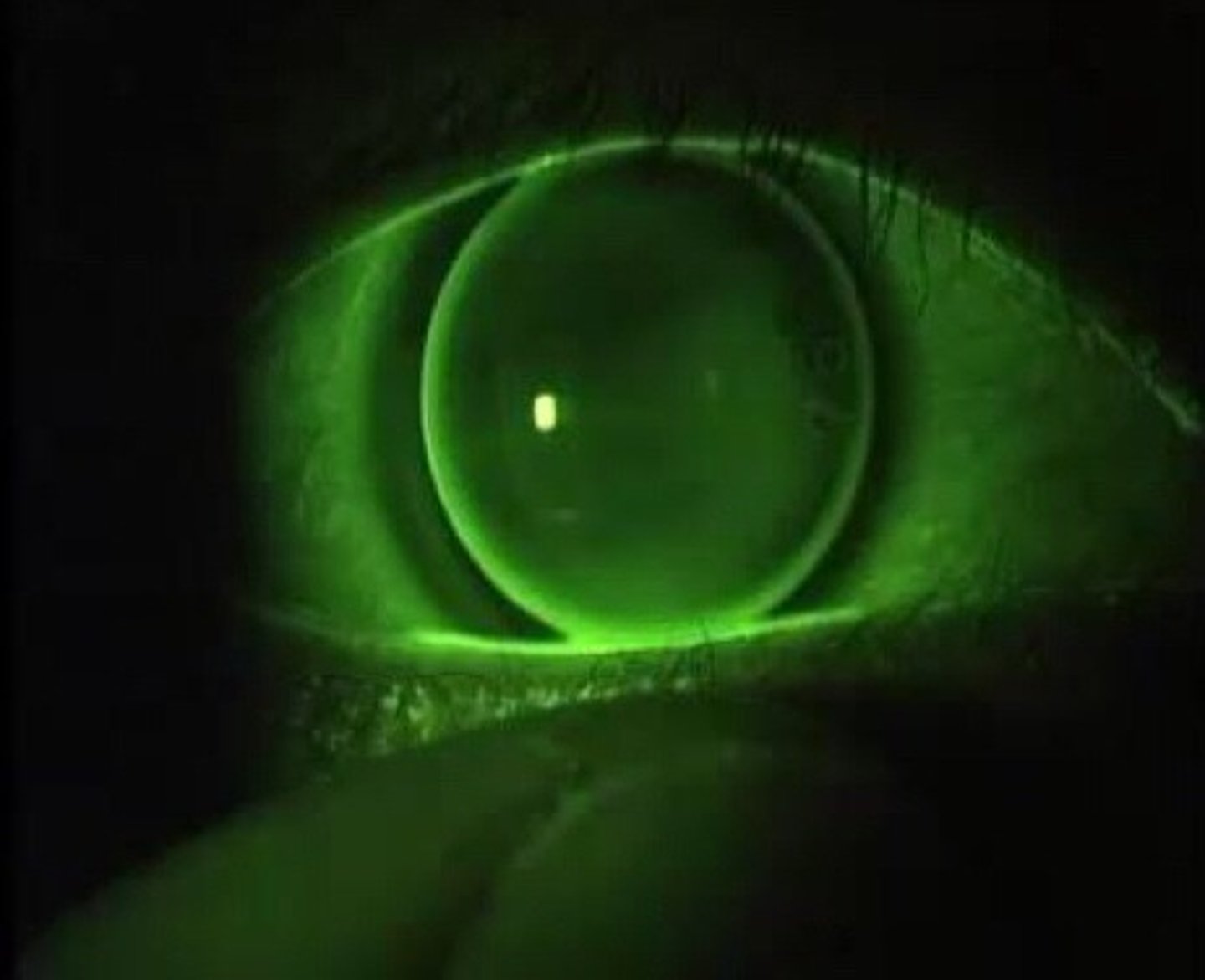
Apical Clearance
Steep fit

Apical Touch
Flat fit
mid-peripheral alignment

mid-peripheral touch
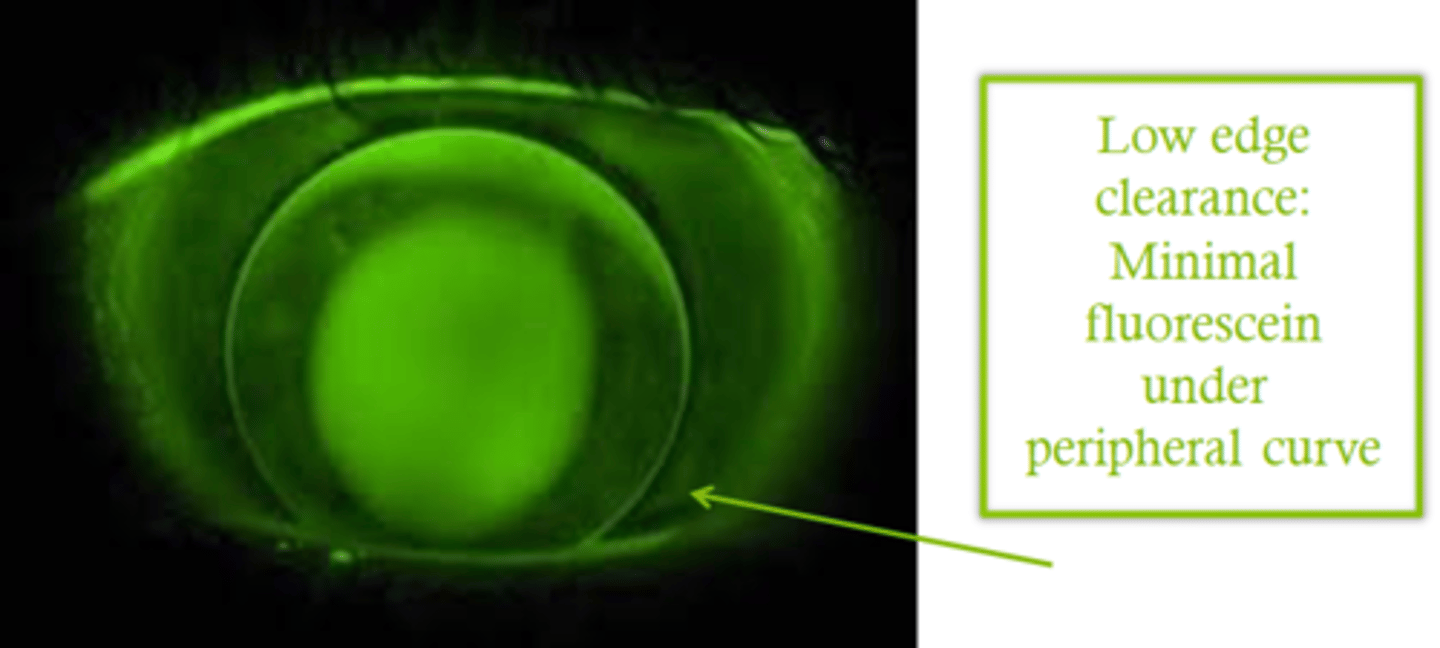
peripheral clearance- minimal/none
peripheral clearance- moderate/medium

peripheral clearance- High/excessive
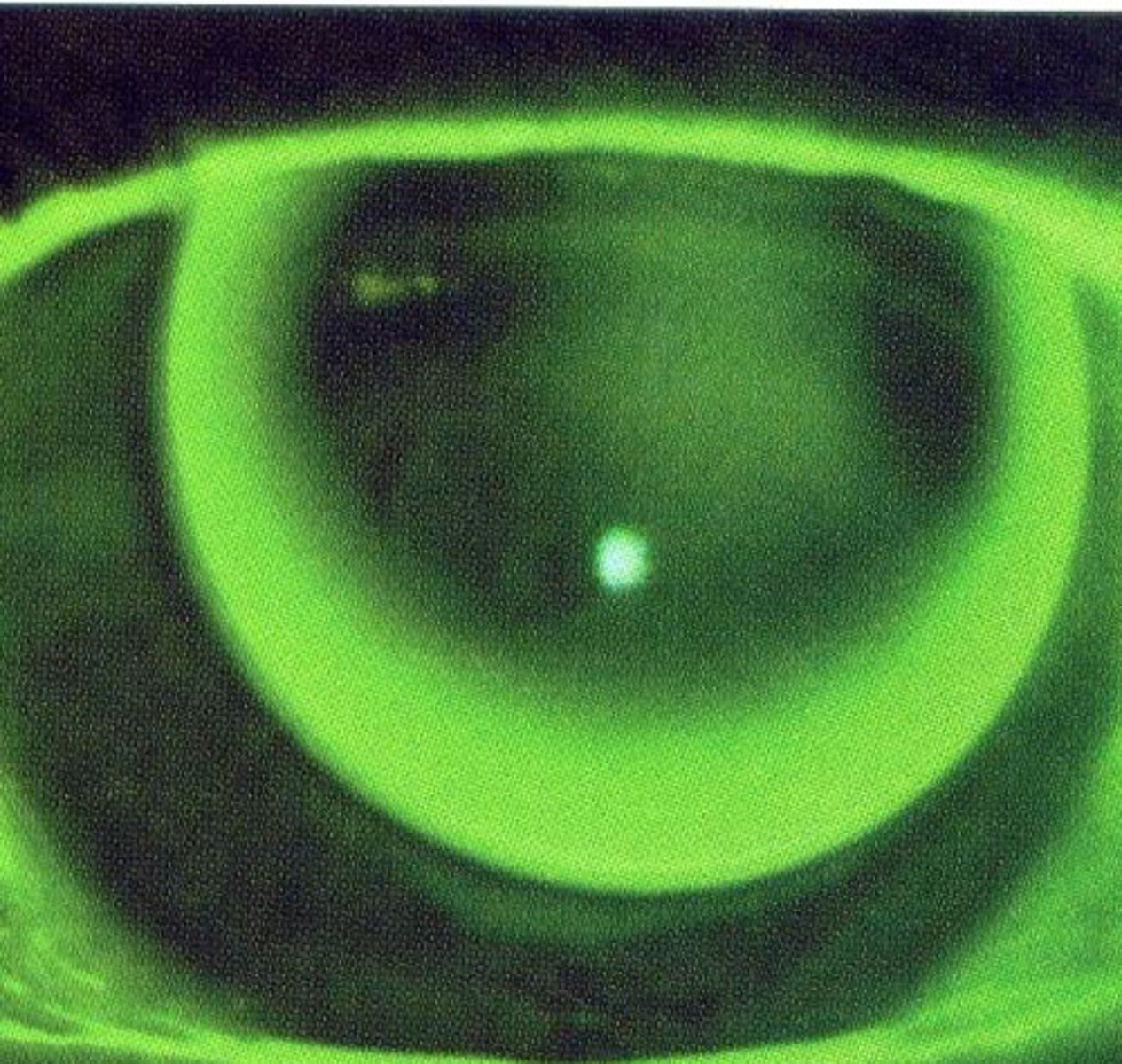
With the rule (WTR)

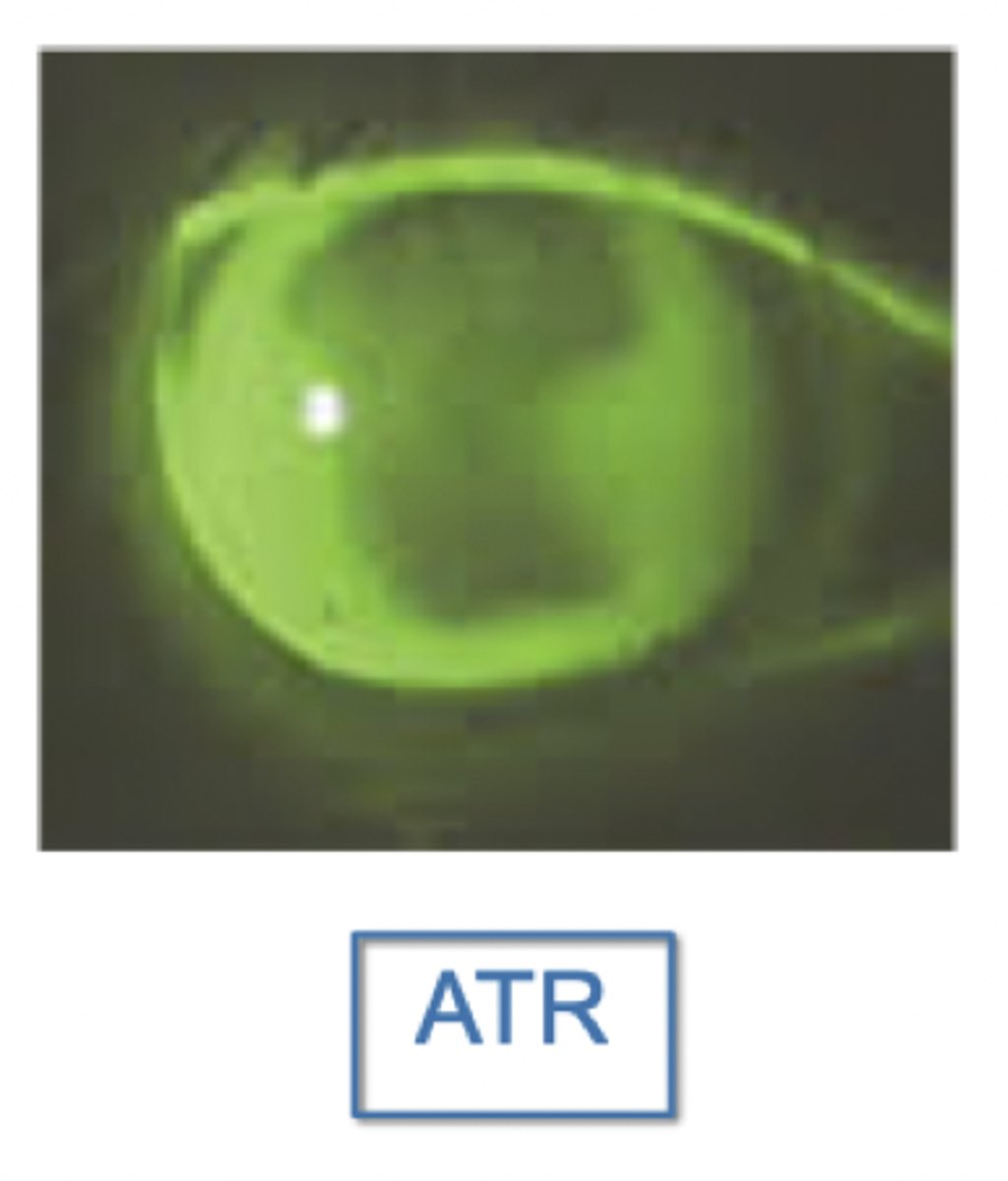
Against the rule (ATR)
With the rule corneas:
-Superior or inferior position
-good for lens alignment, but poor for inferior
-Steeper fits tend to center better
Against the rule corneas:
-Temporal or nasal position
-poor comfort when de-centered laterally
-Steeper fits tend to center better
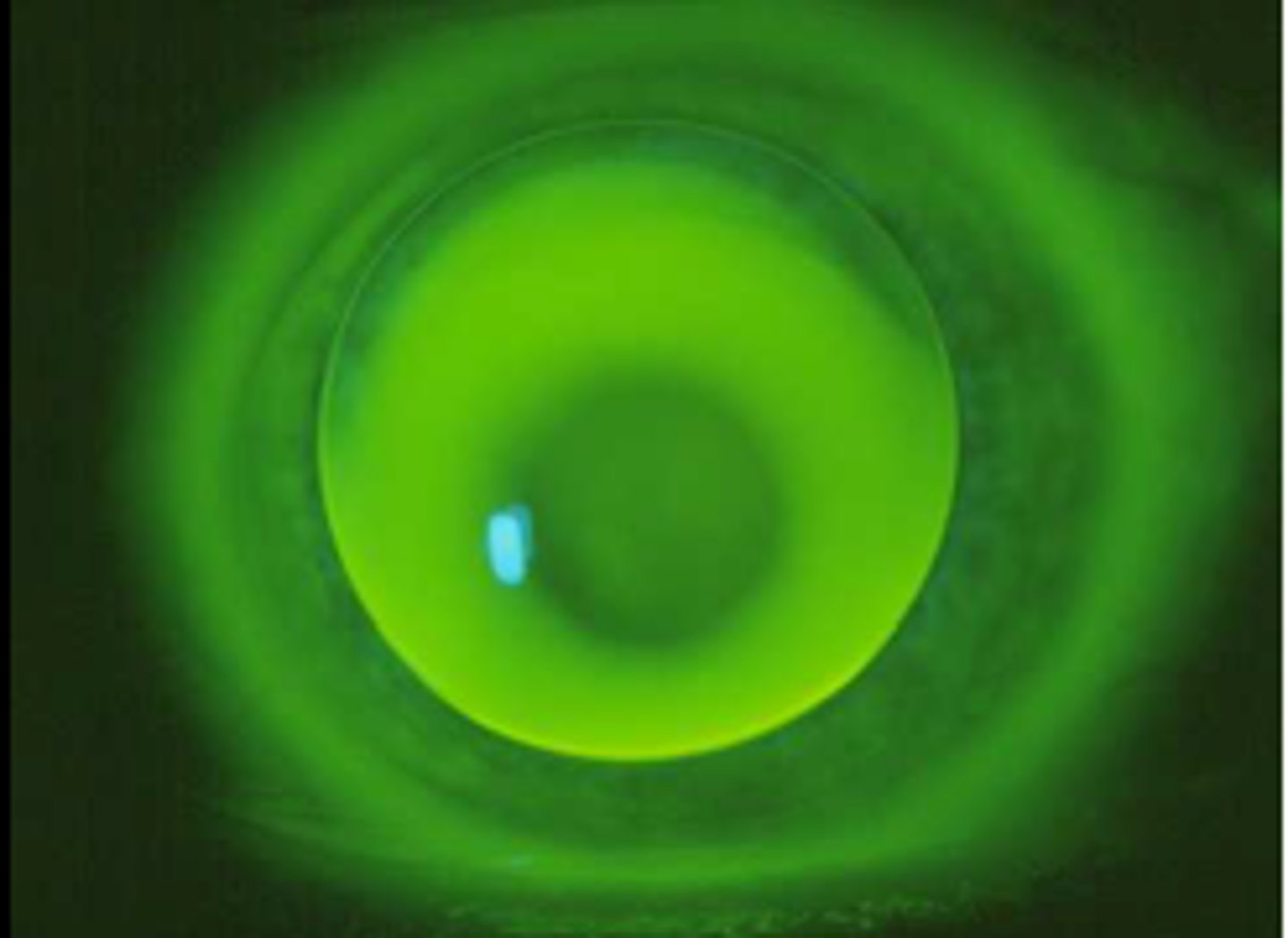
Base curve radius: too steep
Green appearance centrally
Base curve radius: too flat
Black appearance centrally