Medstudy 2
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
Where are calcifications in toxoplasmosis?
All throughout the brain parenchya, especially in the caudate nucleus and basal ganglion.
Polyostotic fibrous dysplasia seen in what?
McCune-Albright syndrome, which also consists of large café au lait spots and endocrine hyperfunction.
Absence of corpus callosum seen in what?
trisomy 8, trisomy 18, and Aicardi syndrome (X-linked dominant disorder characterized by agenesis of the corpus callosum, infantile spasms, and retinal abnormalities).
Roseola
aka?
aka roseola infantum, exanthema subitum
HHV-6
incidence peaks between 6–15m
pp
High fever and irritability
Rash
Fist seen 12-24h after defervescence
Begins on trunk → face, neck, postauricular area, prox extremities.
Lesions p ersist 1-3d, and are sually eddish-pink, discrete, and slightly papular rathrthan vesicular or petechial.
postauricular and/or occipital lymphadenopathy
edematous eyelids associated with palpebral conjunctivitis (Berliner sign)
macules and/or ulcerations at the junction of the uvula and soft palate (Nagayama spots)
bulging fontanelle
Upper respiratory and gastrointestinal symptoms may also occur
May see febrile seizures
Tx
If toxic appearing and bulging fontanelle → ust get LP to evaluate for meningitis.
Less common parvovirus B19 presentation:
papular purpuric gloves and socks syndrome: tender, pruritic papules, petechiae and purpura of the hands and feet associated with edema.
Treatment for chancroid
It is haemophilus ducreyi
single dose of 1 g of oral azithromycin OR
single intramuscular dose of 250 mg of ceftriaxone
less desirable:
over 18 years of age, ciprofloxacin 500 mg orally twice daily for 3 days is equally effective but less desirable because multiple doses are required.
erythromycin base 500 mg 3×/day for 7 days is also effective, but it is not well tolerated during pregnancy; it, too, is less desirable because multiple doses are required.
Guillan Barree
CSF findings
Symptoms
CSF
Elevated protein
Normal glucose
Normal WBC count
pp
Flacid paralysis
Areflexia
Symmetric sensory and/or motor symptoms, often in association with severe pain.
Typically begin in the lower extremities and may progress to involve the trunk, upper extremities, and in some cases, the cranial nerves
May see respiratory depression and failure
Bradycardia, dysrhythmias, and fluctuations in blood pressure due to autonomic dysfunction can occur
Place what in the ear to remove a live insect?
Lidocaine or Mineral Oil
Maternal meds assoc with gastroschisis?
Other maternal factors assoc with gastroschisis?
Gastroschisis is caused by?
Elevated levels of maternal what are common?
Meds: Cocaine and other vasoactive substances (e.g., nicotine, pseudoephedrine)
Other factors: teen pregnancy, maternal hot tub use, and in utero exposure to alcohol and smoking.
Caused by a vascular accident involving the right umbilical vein or right omphalomesenteric artery that leads to ischemic necrosis of the abdominal wall allowing bowel to enter the amniotic cavity.
Elevated leels of serum α-fetoprotein.
Isotretinoin can cause what in a pregnancy?
Congenital defects inluding
craniofacial, cardiovascular, neurological, and thymic malformations.
30-60% are shown to have neurocognitive impairment, even in absence of physical defects
What associations are there for carbamazepine and pregnancy?
congenital malformations, including spina bifida, craniofacial defects, cardiovascular malformations, and hypospadias.
IVIG given. What about MMRV?
Diminished immunogenicity if it was given within 2w prior, or within 11m after. Hold for ≥11m after giving IVIG.
If at risk, give vac, then give again ≥11m.
Screenings for those with T1DM:
Starts when?
What includes?
Starts 5y after dx of diabetes
Nephropathy: annual spot urine albumin:cr ratio at puberty or age > 10y (whichever is earlier)
Retinopathy: q2y, dilated comprehensive eye exam at puberty or age 11y (whichever is earlier)
Neuropathy: Annual comprehensive foot exam at puberty or age 10y (whichever is earlier)
Annual TSH
Lipid testing: Start when glycemic control is achieved and age is 2y. If initial LDL = 100, subsequent testing done once at 9-11 and repeated q3y thereafter.
vWD
plt function abnormality
PT always normal; PTT usually normal; Platelet function analysis (PFA) prolonged (PFA preferred over bleeding time)
Type 1
most common (90%)
autodom
decreased, but not absent vWF.
Type 2
functional defects in one of several activities (plt binding, factor 8 binding, multimeric asembly)
has several subtypes\
subtype 2n is autorecess
Type 3
Absence of von willebrand antigen.
most severe variant
autorecess
Risk factors for dental caries?
When to see the pediatric dentist?
When to start fluoride varnish?
RFs
Children with special health care needs
Premature birth
Late-order offspring
Primary caregiver or siblings with caries
Children with existing caries, demineralization, and/or staining
Infants sleeping with a bottle
Frequent snacking/excessive use of sippy cups
Breastfeeding after 24 months of age
Bottle use after 12 months of age
Low socioeconomic status
Poor parental dental health
See a dentist:
By 12m for normal risk
If risk factors, as early as 6 months of age and no later than 6 months after 1st tooth eruption or 12 months of age, whichever comes first.
Fluoride
Done q3-6m starting at tooth eruption
When to refer to speech therapy for stuttering
Ss severe or last > 4-8w
stuttering causes anxiety or avoidance
Fam hx of the disorder
Can also do cognitive behavioral therapy
What causes omphalocele?
What causes gastroschisis?
Omphalocele
Failure of central fusion at the umbilical ring due to defective mesodermal growth, followed by herniation of the midgut.
Gastroschisis
LIkely the result of a vascular accident invlving the omphalomesenteric artery or defective mesenchymal development at the junction of the body stalk and abdominal wall, leading to disruption of the abdominal wall and evisceration.
Initial tx of choice for long QT syndrome
b-blocker
Lymphocytic interstitial pneumonitis
What is it?
What on x-ray?
Most commonly seen in who?
one of the rare interstitial lung diseases seen in children
homogenous chronic ground glass opacities
most commonly seen with HIV as well as scleroderma
LIP and HIV is a well-described association
When is measles contagious?
3-5d prior to rash through 4d after its appearance
Which live vaccine is contra in those who live with an immunocompromised person?
LAIV (live attenuated influenza vaccine)
Labs you can see with anabolic steroid use
↓ HDL
↑ LDL
↑ serum transaminases
Is cystic fibrosis a restrictive or obstructive pattern?
Obstructive
Enterovirus aseptic meningitis
pp
dx
tx
morbidities
pp
ha, ↓ activity, malaise, ↑ temp, photophobia, nuchal rigidity. Many have a rash.
Dx
CSF
↑ WBC
Normal glucose
Slightly-to-moderately ↑ protein
Neutrophhils may predominate in the first day or two of illness but transition to a lymphocytic pleocytosis within several days.
Confirmation
Usualy with PCR of spinal fluid for enterovirus RNA.
Tx
Symptomatic and supportive care
Morbidities
Most common are ha and impaired attention which resolve over months.
lead interferes with what process?
Heme biosynthesis
inhibits d-aminolevulinic acid dehydratase (ALAD) and ferrochelatase activity → ↑ free erythrocyte protoporphyrin (FEP) in the blood due to inability to complete the heme syntheis pathway.
FEP elevated in lead and iron def, but is extremely high in lead.
What levels of lead require what levels of treatment?
> 5 µg/dL: confirmation with a venipuncture. ensure adequate intake of iron and calcium, milestone assessment, anticipatory guidance about sources of lead exposure, and follow-up testing
>10 µg/dL: environmental investigation/intervention to remove potential sources of lead is also performed.
≥ 45 µg/dL: chelation
Severe allergy to yeast is a contra for what vaccine?
HPV
7 + 4 rule for teeth
7m → first teeth.
11m (7+4) → 4 teeth
15m (11+4) → 8 teeth
19m (15+4) → 12 teeth
23m (19+4) → 16 teeth
27m (23+4) → 20 teeth
Properdin deficiency
is C5-C9 deficiency
Giving a meningococcal vaccine in someone less than 2 years
Menveo (MenACWY-CRM)
The only one that can be used.
If 7-23m: 2-doses ≥3m apart and 2nd dose must be in 2nd year of life
If ≥2y: 2 doses ≥8w apart
Giving the Menactra vaccine
Must be ≥24m to avoid interference with PCV13 and 15.
2 doses ≥8w apart. 1st dose ≥4w after completion of all PCV-13 or 15 doses.
Giving MenACWY-TT (MenQuadfi)
Must be ≥24m
2 doses ≥8w apart
Transverse myelitis
What is it?
Some common reasons to get it?
pp?
Dx
CSF?
MRI?
Tx?
It is segmental spinal cord inflamation.
sometimes is preceded by an illness associated with nonspecific systemic symptoms
Comon reasons are EBV, rubella, mumps, varicella, influenza, Mycoplasma pneumoniae, and Borrelia burgdorferi; an autoimmune etiology is thought to be likely in many other cases.
pp
Sudden progressive weakness and multimodality sensory disturbances (i.e., pain, temperature, touch) in the lower extremities.
Dx
CSF: Mild lymphocyte pleocytosis, normal or slightly elevated levels of protein
MRI: spinal cord swelling with hyperintensity on T2-weighted imaging
Tx
Corticosteroids
What causes in utero meconium passage
usually results from fetal hypoxic stress
a preductal and postductal oxygen gradient can indicate what?
pulmonary hypertension
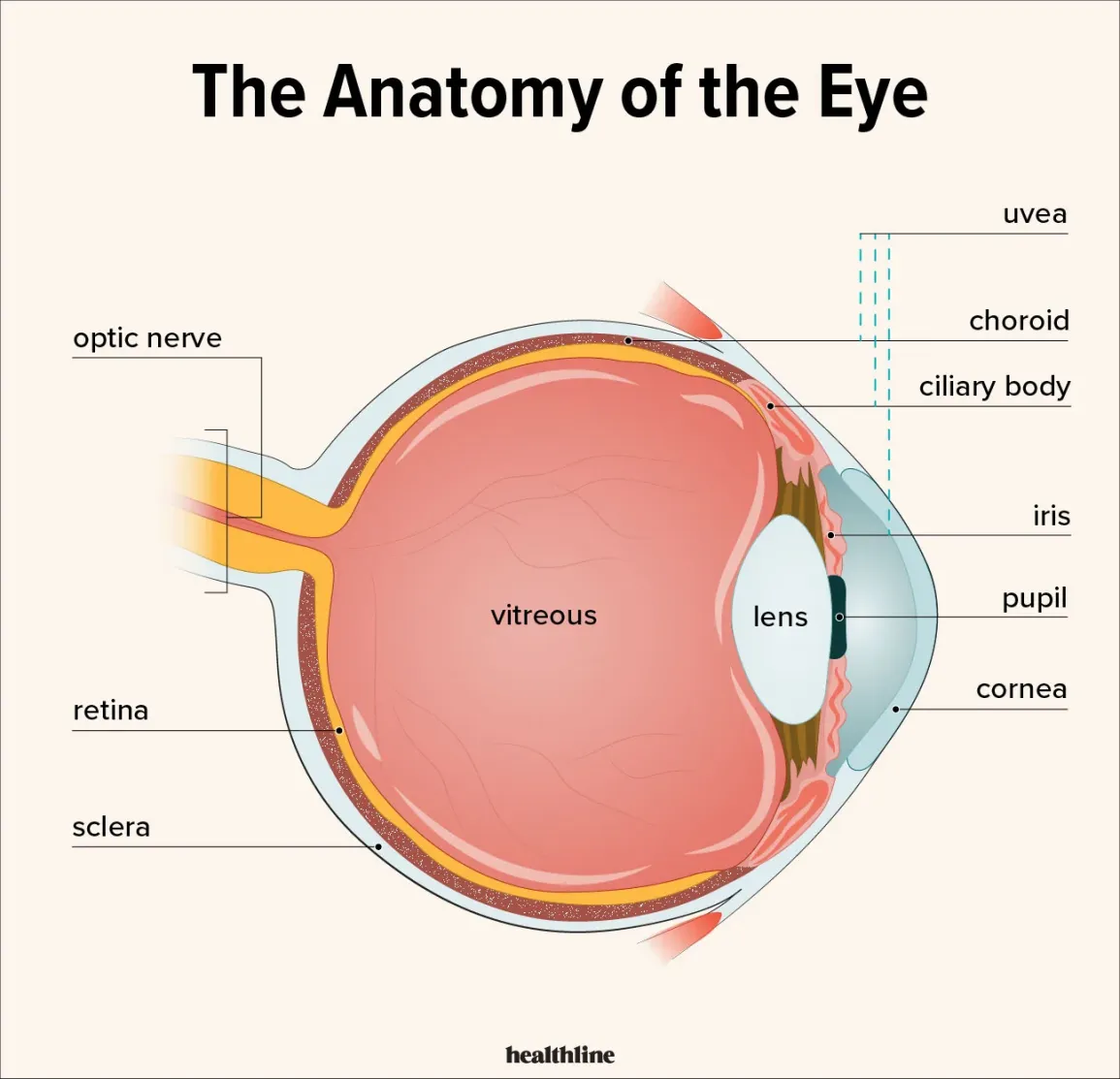
conjunctivitis vs uveitis
Uveitis is inflammation of the structures underneath the sclera which include choroid, ciliary body, and iris.
Conjunctivitis is inflammation of the sclera which is above the uvea.
Enthesitis-related arthritis criteria for dx
Enthesitis and arthritis, or
Either enthesitis or arthritis with ≥ 2 of the following:
History or presence of sacroiliac joint tenderness and/or inflammatory lumbosacral pain
Presence of HLA-B27 antigen
Onset of arthritis in a male > 6 years of age
Acute symptomatic uveitis
A 1st degree relative with ankylosing spondylitis, ERA, sacroiliitis with inflammatory bowel disease, or reactive arthritis
Stickler Syndrome
~20% of Pierre robins have stickler syndrome
Stickler syndrome is a group of several genetic disorders affecting connective tissue, specifically collagen.
stickler also assoc with ophthalmologic (myopia, cataracts, vitreous anomaly, retinal detachment), auditory (sensorineural or conductive hearing loss), and articular (joint hypermobility, early onset osteoarthritis, spondyloepiphyseal dysplasia) abnormalities.
Incontinentia pigmenti
Stages?
Systemic findings?
1: crops of inflammatory vesicles and bullae over the trunk and extremities
Often w/ periph eosinophilia
2. Vesicles clear and are replaced by irregular linearly distributed verrucous (wartyish) lesions on the extremities, hands, and/or feet.
3. thin bands of “swirly” brown, bluish-gray pigmentation that often coalesce and darken further before slowly fading by adolescence
4. As they fade, you get atrophy and hypopigmentation.
Systemics
Dental (delayed dentition, pegged or conical teeth, partial anodontia)
Alopecia
Nail changes
Varying degrees of mental disability and/or seizure dsorders.
Eye problems (strabismus, cataracts, retinal detachment)
What is the rash seen in Langerhans cell histiocytosis?
Erythema and greasy, yellow scales over the trunk and extremities

What is it?
More in males or females?
Associateds?
Is it malignant?
Tx?
Becker nevus
M>F
may be congenital, but more often appears in adolescence
the presence of hypertrichosis is characteristic of a Becker nevus
Hypertrichosis usually develops 12–24 months after changes in pigmentation are first noted.
usually located on the trunk (especially chest, shoulder, or upper back)
Most patients have no additional findings, although some patients do have associated anomalies (the so-called Becker nevus syndrome), including ipsilateral hypoplasia of the chest, breast, and areola; limb shortening; pectus deformities; scoliosis; and spina bifida occulta.
Malignant changes do not occur.
Tx is cosmetic only.
Criteria for Tourettes
At least 2 motor tics and at least 1 vocal (phonic) tic have been present, not necessarily at the same time.
Tics may wax and wane in frequency but have occurred for more than 1 year.
Tics started to appear before the age of 18.
Tics are not caused by the use of a substance or other medical condition.
dermoid cysts vs epidermal cysts
Dermoid cysts
second most common midline neck mass after thyroglossal duct cysts
result from entrapment of skin along lines of embryonic closure
differ from epidermoid cysts in that they contain skin appendages, such as sebaceous glands and hair follicles within the cyst wall.
Epidermal cyst
may occur on any hair-bearing skin
Both do not elevate with swallowing
Branchial cleft cyst
congenital lesions that arise from remnants of a slight cleft or defect during gestation
Located laterall
May change in size and shape
often noticed after an upper respiratory tract infection
Branchial cleft cysts or sinuses may have external openings or pores from which a mucus-like material drains out
Criteria for Lyme ppx?
Meds for ppx?
A single dose of doxycycline prophylaxis (4.4 mg/kg/dose or 200 mg max) to prevent Lyme disease can be offered to nonpregnant adults and children of any age when all the following circumstances are satisfied:
Doxycycline is not contraindicated.
The tick can be identified as an adult or nymphal Ixodes scapularis tick (diagnostic tick testing for expert identification is recommended in 2020 guidelines but not testing the tick for Borrelia).
The time of attachment is ≥ 36 hours based on the degree of tick engorgement or time of exposure to the tick.
Prophylaxis can be started within 72 hours of tick removal.
Lyme disease is common in the location where the patient lives or has recently traveled (high endemicity is when > 20% of nymphal ticks and > 50% of adult ticks are infected).
Ppx
A single dose of doxycycline would be the choice for prophylaxis
Tx
Doxycycline preferred (10d for E migrans) in adults and kids, regardless of age, due to its activity aginst burgdorferi and other oganisms transmitted by ixodes tick like anaplasma or ehrlichhia.
Amoxicillin or cefuroxime for 14 days are alternative options for treatment of erythema migrans (single or multiple) at any age
amoxicillin is not indicated to treat neurologic manifestations of Lyme disease (e.g., facial nerve palsy, meningitis)
Amoxicillin is preferred to doxycycline in children < 8 years of age with Lyme arthritis due to the length of recommended treatment (28 days)
IV ceftriaxone is indicated for treatment of Lyme disease if the patient has severe/complicated neurologic symptoms, early in course of treating Lyme carditis, or for treatment of Lyme arthritis unresponsive to oral agents.
Fetal warfarin syndrome
Happens if there is exposure during 6-9 weeks GA
pp
nasal hypoplasia
stippled epiphyses
Bone findings in congenital syphilis
Osteochondritis and Periostitis, usually involving the metaphysis and diaphysis of 1 or more long bones.
Metaphyseal lesions appear as irregular bands of decreased mineralization or focal circumscribed areas of bony destruction; e.g., destruction of the medial aspect of the proximal tibial metaphysis (Wimberger sign).
infantile cortical hyperostosis
a.k.a. Caffey disease
Radiographic findings of infantile cortical hyperostosis (a.k.a. Caffey disease) include significant cortical thickening (most often of the mandible, clavicle, and ulna) and periosteal reaction in otherwise normally mineralized bone.
When is toilet training usually complete?
The average completion of toilet training is at 30 months of age, with roughly 75% of children attaining daytime continence by 36 months of age.
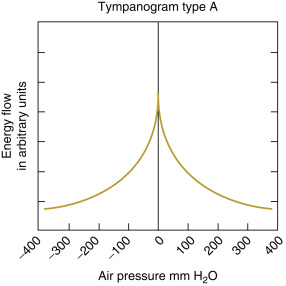
Tympanogram type A
Normal middle ear function
“Normal box values” →
-150 0 +50 daPa (x-axis)
Peak compliance: 0.2-1.8 cc (y-axis)
Thre is absence of middle ear pathology
TM is mobile and intact
Eustachain tub function is normal
If there is hearing loss, it is likely sensorineural.
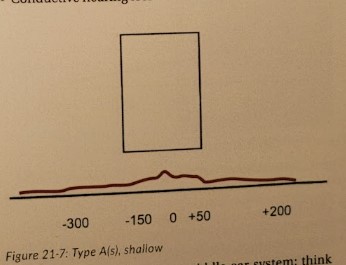
Tympanogram tye A(s)
Shallow; poorly compliant middle ear system.
Think: TM scarring, TM sclerosis, otosclerosis, or ossicular fixation.
Compliance curve is in the normal position (x-axis), but peak compliance is very low (< 0.2 cc)
NOT due to middle ear effusion!
Conductive hearing loss
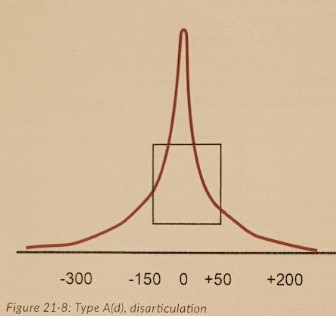
Tympanometry type A(d)
Highly compliant middle ear system.
Think: Ossicular disarticulation or hypermobile TM
Peak compliance occurs between -150-50 (ie normal)
Peak compliance is very high
Conductive hearing loss is possible.
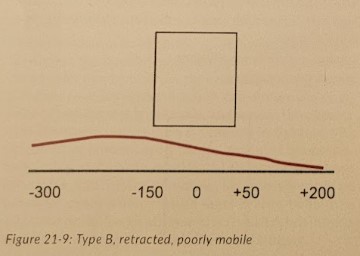
Tympanometry type B
Retracted, poorly mobile.
Think: Middle ear effusion or perforated ear drum
Compliance curve is nearly flat to completely flat and always below normal.
Negative middle ear pressure (Peak compliance is shifted left)
Conductive hearing loss
Tympanometry type C
Normal compliance but negative pressure in the middle ear.
Think: eustachain tube blockage
Clear peak
Peak compliance has normal amplitude
Peak compliance is shifted to the left (negative middle ear pressure)
Conductive hearing loss is likely.
Magnesium exposure for neonates
Mag is given to mothers to treat pre-eclampsia or for tocolytics.
Elevations in neonate serum mag conc (>2.3 meq/L)L
Levels <5 usually don’t result in serous comps but may cause lethargy and difficulty with feeding.
pp
resp depression, apnea, generalized hypotonia.
Additional comps can be GI hypomotility and meconium plug syndrome mimicking intestinal obstruction.
Tx
If kidneys normal, most only need symptomatic care for several days with monitoring of fluid intake and resp status.
In severe cases, tx with IV calcium and diuretics may be needed.
Adrenoleukodystrophy
What causes it?
inheritance?
pp age?
pp?
dx?
tx?
Disorder of peroxisomal degradation of fatty acids → accumulation of very long-chain faty acids in the central and peripheral nervous system and adrenal glands.
X-lnked recessive
Usually presents between 5-15y
pp
Due to associated cortisol deficiency (up to 70% of cases) → ↑ ACTH precursor (proopiomelanocortin) → ↑ melanin synthesis → hyperpigmentation of knees, elbows, palmar creases, axillae, gingival borders.
Seizures
Impaired auditory discrimination
Spatial orientation disturbances
Visual disturbances
Dx
Symmetric periventricular white matter lesions in the posterior parietal and occipital regions of the CNS on CT or MRI are commonly idenified.
Tx
Treat the adrenal insufficiency.
Pts may benefit from a bone marrow transplant.
Tinea capitis
Most often by Trichophyton tonsurans
Is an endothrix infection, meaning the dermatophyte invades the hair shaft and internalizes into the hair cell.
Does not fluoresce with wood lamp
pp
Can have kerion (boggy plaque, inflamed, can have alopecia, pustules, crusting, purulence)
patches of alopecia often asoc with black dots, which are the distal ends of hairs that have broken at the surface of the scalp.
Tx
Oral antifungal (griseofulvin (drug of choice) or terbinafine)
griseofulvin is 6-8w. take with milk or fatty meal
Ketoconazole shampo added to prevent spread to other inds.
some recommend household members use antifungal shampoo to prevent reinfection of a patient.
systemic corticosteroids occasionally added for inflammation and to prevent permanent alopecia. Benefit is unclear.
Infantile glaucoma
associated conditions can be galactosemia, trauma, intraocular hemorrhage, ocular inflamm disease, sturge-weber syndrome, marfan, neurofibromatosis, lowe syndrome congenital rubella, juvenile xanthogranuloma
pp
excessive tearing
photophobia
blepharospasm
corneal edema (and/or cloudy)
corneal and ocular enlargement
conjunctival injection
visual impairment
Tx
Surgery to alleviate intraocular pressure immediately indicated
Congenital varicella syndrome
Hypoplastic limbs, cutaneous scars, cataracts, chorioretinitis, microphthalmos, and cortical atrophy.
Some causes of rectal prolapse
Functional constipation and prolonged straining during defecation = #1
chronic diarrhea caused by enteric and parasitic infections such as Trichuris trichiura = #2
Cystic fibrosis (CF), malnutrition, polyps, and conditions leading to pelvic floor weakness are other common etiologies.
Dx criteria for NF1
By definition, individuals with NF1 must have at least 2 of the following findings:
≥ 6 café au lait macules measuring > 5 mm in greatest diameter in prepubertal individuals and > 15 mm in greatest diameter in postpubertal individuals
≥ 2 neurofibromas of any type or ≥ 1 plexiform neurofibroma
Axillary or inguinal freckling
≥ 2 iris hamartomas (Lisch nodules)
Optic glioma
A distinctive osseous lesion, such as sphenoid dysplasia or thinning (bowing) of the long bone cortex (with or without pseudoarthrosis)
A 1st degree relative with NF1
Charcot-Marie-Tooth (CMT) disease
aka?
aka hereditary motor sensory neuropathy
present in the 1st or 2nd decade
family history is common
pp
progressive distal weakness
mild to moderate sensory loss
depressed or no tendon reflexes
high-arched feet (pes cavus)
Muscle atrophy develops and leads to “stork legs.
Upper extremitieseventually involved in later stages.
Mononeuritis multiplex
An asymmetric pathology of the peripheral nerves, which is typically painful.
Is often associated with other disease states, such as
diabetes mellitus, amyloidosis, rheumatoid arthritis, or systemic lupus erythematosus.
Diagnosis requires involvement in 2 separate nerve areas.
As the disease progresses, muscle weakness and atrophy may develop
What is the most common cause of spinal cord compression in pediatrics?
spinal cord tumors
Most will have some combination of back pain, weakness, gait disturbances, scoliosis, and/or bladder dysfunction
In younger children, motor regression can be a presenting symptom.
Caudal regression syndrome
A group of congenital anomalies that may involve the lower vertebral bodies, sacrum, spinal cord, and lower extremities; or, presents as sirenomelia in extreme cases (sirenomelia = mermaid syndrome = fused legs)
25% of cases assoc with maternal T1DM.
also been linked to env factors like exposure to organic solvents during pregnancy and folate deficiency.
pp
Motor and sensory impaired below the level of the affected vertebrae.
Many have lifelong bowel and/or bladder incontinence, and some lower extremity dysfunction
There are assoc deformities of the hips, legs, and/or feet, in addition to progressive scoliosis, which often complicate the clinical course.
Uncoontrolled hyperthyroidism in pregnancy - probs for baby
↑ risk of preterm and low birth weight. Neonates with high thyrotropin receptor antibody titers are at ↑ risk of developing hyperthyroidism a few days after birth.
Bath salts
Sympthomimetic syndrome with stimulant and hallucinogenic effects
pp
↑ bp, ↑ hr, ↑ rr, ↑ temp, diaphoresis, mydriasis, anxiety, agitation, combativeness, paranoid delusions, and/or seizures
Dx
Clinical
Synthetic cathinone comounds may not be detected on routine urine drug screening
Tx
Psychomotor agitation best treated with IV diazepam or lorazepam.
Treat assoc ele levels and/or hypoglycemia (decreases risk of seizures)
Comps
arrhythmias, extreme hyperthermia, intracerebral hemorrhage, rhabdomyolysis, acute tubular injury (a.k.a. acute tubular necrosis), and electrolyte abnormalities (e.g., hyponatremia, hypokalemia, hypermagnesemia).
Which antiseizure med is assoc with neural tube defects
Valproate
Up to 2% of fetuses exposed to valproate in utero develop neural tube defects (NTDs), a 4× increase when compared to babies born to mothers with epilepsy who used other antiseizure monotherapies
Fetal exposure to valproate may also have adverse effects on cognitive and neurologic function (e.g., lower IQ scores, difficulty with verbal reasoning skills, delay in motor development, increase in the prevalence of autistic spectrum disorders).
Fetal exposure to phenobarbital can cause what?
cardiac, orofacial, and genitourinary anomalies
Contras to oral rehydration can include:
hemodynamic shock, abdominal ileus, persistent emesis, intestinal intussusception, stool output in excess of 10 mL/kg body weight/hour, and monosaccharide intolerance.
25 kg child has a 5% fluid deficit, use holliday-segar to find the fluids for the next 24h:
“100/50/20”
First 10 = 1,000mL, next 10 = 500 mL, remaining 5 = 100 mL. Total 1,600
Deficit in liters = 5% (0.05) * 25 kg = 1.25 L = 1250 mL
Add together = 2850 mL needed for next 24h.
Kwashiorkor
protein-energy malnutrition
low protein caarbohydrate diets (rice, casava, yams)
pp
edematous abdomen
pitting edema
hepatomegaly
brittle hair
reddish-brown scaly rash
pigmentary changes
T-cell function and cell-mediated immunity affected → ↑ risk of infection
Marasmus
protein-enegy malnutrition without edema
severe nutritional deficit in calories
generalized loss of muscle
little or no subcutaneous fat
appear emaciated
loose, wrinkled skin due to the loss of subcutaneous fat
have the appearance of a “wizened old man” due to their loss of temporal and buccal fat pads
frequently hypothermic, bradycardic, and hypotensive due to their chronic energy deficit
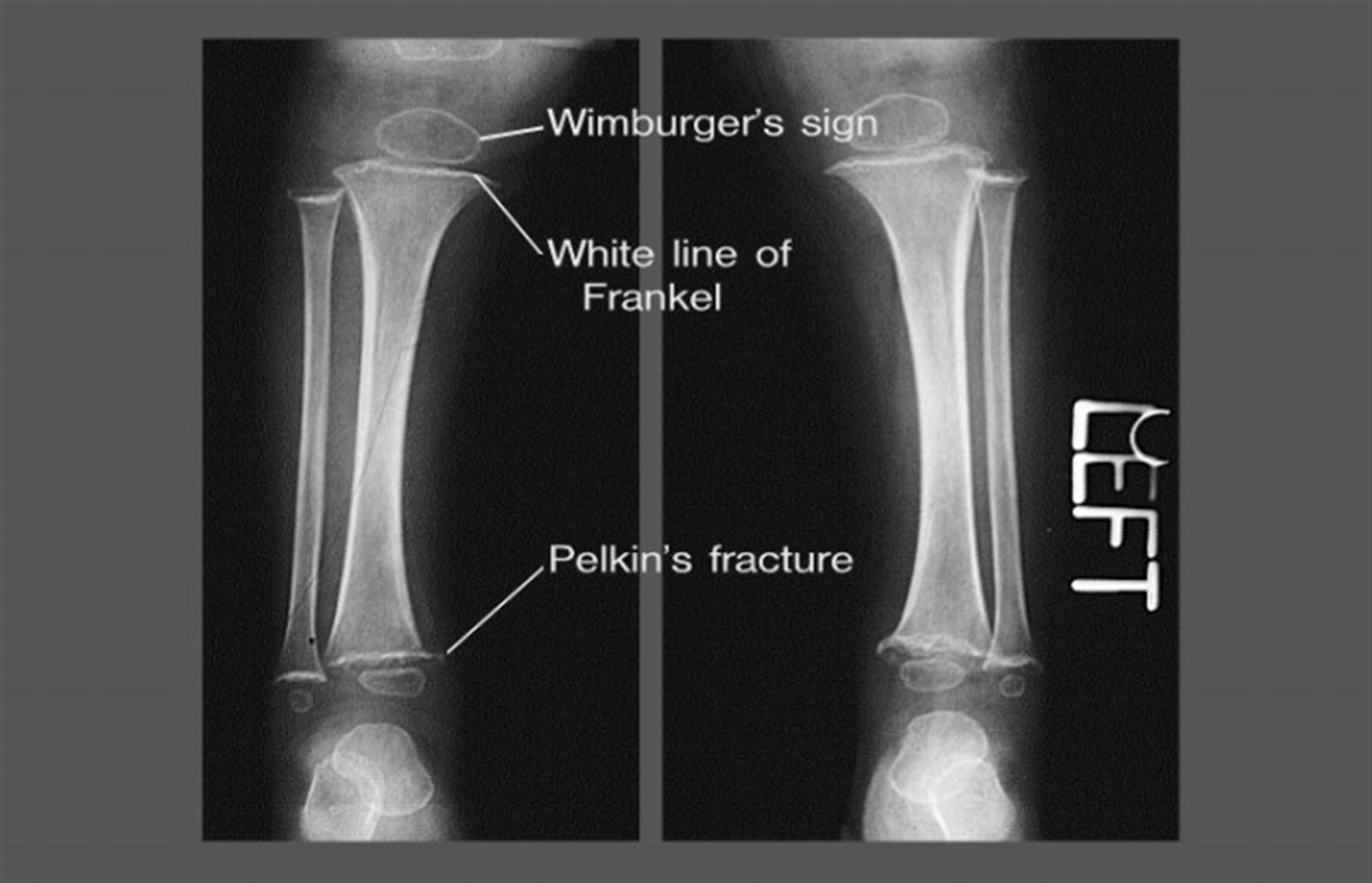
What are white line of Frankel seen in?
Vitamin C deficiency (Scurvy)
Lupus anticoagulant
What is it?
What does it cause?
What about a 1:1 plasma mixing?
It is a prothrombotic, antiphospholipid antibody.
It causes nonspecific inhibition of various clotting factors which leads to prolonged PTT.
Will not correct with mixing of normal plasma
This because the prolonged PTT is caused by an inhibitory factor and not by deficiency of a clotting factor.
It can be the first sign of SLE
Factor V Leiden
An inherited thrombophilia
It is assoc with activated protein C resistance.
Treatment for late lyme disease arthritis
Late lyme
28 days of oral doxy for those ≥8y or
amoxicillin for those < 8y, but amoxicillinis not approved for any neurologic lyme disease.
parenteral ceftriaone is used for lyme arthritis that is unresponsive or worsening desite oral therapy
Early disseminated lyme
oral doxy x14d.
Neuro lyme
No amoxicillin
Use IV ceftriaxone
Cardio lyme
Start with IV, then switch to PO to complete the course (14-21d)
Erythema migrains (single or multiple)
All ages: Oral doxy x10d, or an oral b-lactam (amoxicillin or cefuoxime) x14d.
Burkitt lymphoma endemic form
African
jaw or facial bone tumor that spreads both locally (oral, nasal, and sinus cavities; often associated with inappropriate loosening of the teeth) and to distant sites, including the mesentery, ovary, testis, kidney, bone marrow, and meninges
Linked to EBV
Burkitt lymphoma nonendemic
sporadic type
presents with abdominal distention and ascites due to extensive disease within the abdominal cavity and with distant spread to the bone marrow and/or central nervous system.
originates from relatively mature B cells within Peyer patches and may lead to intussusception.
Linked to EBV
Gianotti-Crosti syndrome
aka papular acrodermatitis of childhood
multiple, slghtly edematous and erythematous papules on the face, but, extensor surface of forearms and legs. spares trunk.
papules (or, less commonly, papulovesicles) may persist for weeks to months and are typically nonumbilicated, monomorphous, and brownish-tan in color, ranging in size from 1 mm to 10 mm
Koebner phenomenon
(lesions that appear or become more prominent at sites of trauma)
Upper respiratory symptoms, fever, diarrhea, hepatosplenomegaly, and/or lymphadenopathy may be noted prior to the appearance of the rash, suggesting an underlying infectious trigger.
EBV most common cause
RSV, hep b, group a strep, myco pneumo, enterviruses, parainfluenza, parvovirus, hhv6, rotavirus, adenovirus.
Urticaria pigmentosa
Urticaria pigmentosa is characterized by brown macules that urticate when stroked (Darier sign).
normal prepubertal estradiol levels are what?
< 10 pg/mL.
Transient neonatal pustular melanosis
benign, self-limited, unknown origin, most common in Black neonates.
present at birth
pp
characterized by superficial 2–5-mm vesiculopustules, which spontaneously rupture within several days, leaving pigmented macules with a fine collarette of scale.
hyperpigmentation fades in 3 weeks to 3 months
Infants may have any combination of pustules, scale, and/or hyperpigmented macules
typical distribution is along the forehead, anterior neck, upper shoulders, lower back, and legs.
Dx
Clinical
Although unnecessary, examination of the contents of the pustules will reveal multiple neutrophils.
Tx
None
ACEIs and fetal health
1st tri
Congenital cardiovascular (e.g., septal defects, patent ductus arteriosus) and CNS (neural tube defects)
2nd & third tri
Renal anomalies including neonatal renal failure
Fetal growth restriction
Oligohydramnios
In utero fetal demise
Pulmonary hypoplasia
Limb anomalies
B-blockers and pregnancy
Propranolol → ↓ growth in utero (may be confoundes)
Propranolol → bradycardia and/or hypoglycemia. Short-lived. Respond to supportive care until drug is metabolized.
Labetalol first line
Toilet training
Introduce the topic at 12m and tell parents it shouldn’t begin until ≥18m and only if kid shows interest in doing so at that time.
Girls go faster than boys
Firstborns often are later
Ma require up to 3m of taining and there are often setbacks.
Readiness signs
sphincter control, regular patterns of elimination, ambulates well, follows 2-step commands, pulls pants up and down, dislikes being wet, imitates behaviors, expresses an interest in the potty, and displays emerging independence.
When is foreskin retractable?
by 3 years of age, over 90% of males have easily retractable foreskin.
Pediatric Type 2 DM management
If not metabolically decompensated at presentation, management depends on HbA1c.
HbA1c < 8.5%
Metformin and lifestyle (diet and exercise) modification.
Hba1c gqu 8.5%
Basal insulin + metformin is considered
After establishing negative pancreatic autoantibodies, insulin should be titrated and liraglutide may be considered.
Salmonella diarrhea and treatment
With uncomplicated Salmonella → no abx; treatment prolonges shedding and increases the risk of resistance.
Exceptions are
older adults
very young (< 3 months old)
immunocompromised
These should be treated with antibiotics because the risk that Salmonella may disseminate or cause more extensive problems is greater than the risk of prolonged shedding.
If antibiotics are to be started, obtain a blood culture before initiating antibiotics.
Complex regional pain syndrome
more common in high-achieving adolescents
pp
Allodynia (pain from light touch)
hyperalgesia (↑ sensitivity to pain) of the region
localized autonomic dysfunction with edema, coolness or excess warmth, mottling, and/or sweatiness.
Tx
Aggressive PT and OT
In many cases, physical therapy includes desensitization to textures, pressure, and temperatures (particularly in those with allodynia)
Mental health support
do not immobilize the area. Pain will diminish as extremity function improves with physical therapy and range-of-motion exercises.
Comps
CRPS can result in long-term disability and atrophic changes leading to permanent damage in the involved extremity.
Rosacea treatment
If a papulopustular component → topical metronidazole.
Alt: azelaic acid, sufacetamide/sulphur, benzoyl peroxide (with or without a topical antibiotic), and retinoids.
Oral tetracyclines are often beneficial in a more severe disease and may be combined with a topical agent.
Alternative oral agents: erythromycin, azithromycin, and metronidazole.
Oral retinoids: may lead to improvement in patients not responding to initial therapies.