Obstetrics and Neonatal Care 2.0
1/69
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
70 Terms
Placenta
●The placenta is a disk-shaped structure attached to the uterine wall that provides nourishment to the fetus.
●Keeps the circulation of the woman and fetus separated but allows substances to pass between them
●After delivery, the placenta separates from the uterus and delivers
●Anything ingested by a pregnant woman has the potential to affect the fetus.
●The umbilical cord connects the woman and fetus through the placenta
Umbilical Cord
●Bundle of blood vessels
●2 umbilical arteries
●1 umbilical vein
●Umbilical arteries (2) carry deoxygenated blood from the fetus to the placenta
●Umbilical vein (1) carries oxygenated blood from the placenta (maternal) to the fetus
●Passage for nourishment, oxygen, nutrients & waste products to & from the fetus
●22 – 24 inches long
LIFELINE OF THE FETUS
Amniotic Sac
●Fluid-filled, baglike membrane
●Contains about 500 to 1,000 mL of fluid
●Helps insulate and protect the fetus
●Fluid is released in a gush when the sac ruptures
●Usually at the beginning of labor
Normal Changes to the body during pregnancy
Respiratory
•Diaphragm get displaced
•Respiratory rate increases
•Minute volume decrease
Changes in cardiovascular system
•Blood volume increases up to 50% by the end of pregnancy
•Heart rate increases up to 20%
•Cardiac output is significantly increased
•Number of red blood cells increase
•Speed of clotting increases
Musculoskeletal system changes
•Joints becomes loose or unstable
•Center of gravity changes increasing the risk of falls
Stages of delivery
Contractions
Childbirth
Afterbirth
Stage 1
●Begins with the onset of contractions and ends when the cervix is fully dilated
●Usually the longest stage, lasting an average of 16 hours
●Uterine contractions become more regular and last about 30 to 60 seconds each.
●Frequency and intensity increase.
●A woman may experience preterm or false labor, or Braxton-Hicks contractions.
●*Labor is generally longer in a first pregnancy*
Stage 2
Begins when the fetus begins to encounter the birth canal
Ends when the newborn is born
●Uterine contractions are usually closer together and last longer.
●The perineum will bulge significantly, and the top of the fetus’s head will appear at the vaginal opening (crowning)
If your patient is crowning, go get the OB kit and your catchers mitt, you stay on scene and deliver the baby
Stage 3
The third stage of labor begins with the birth of the newborn and ends with the delivery of the placenta.
●During this stage, the placenta must completely separate from the uterine wall.
●This may take up to 30 minutes
Stay on scene if:
●Delivery is imminent will occur within a few minutes
●A natural disaster, inclement weather, or other environmental factor makes it impossible to reach the hospital
To determine if delivery is imminent, ask the patient:
●How long have you been pregnant?
●When are you due?
●Is this your first baby?
●Are you having contractions?
●How far apart?
●How long do they last?
●Have you had spotting or bleeding?
●Has your water broken?
●Do you feel as though you need to have a bowel movement?
●Do you feel the need to push?
Once labor has begun, it cannot be slowed or stopped…
●Never attempt to hold the patient’s legs together.
●Do not let her go to the bathroom.
●Instead, reassure her that the sensation of needing to move her bowels is normal and that it means she is about to deliver.
●If your decision is to deliver at the scene, remember that you are only assisting the woman with the delivery.
●Your part is to help, guide, and support the baby as it is born
Indication that delivery imminent
●Contractions every 2 minutes,
●Lasting about 45 seconds
●Urge to push or move her bowels
●If amniotic sac is still intact
●Tear the sac
●Move away from face
Field Delivery
●Place towels or sheets on the floor around the delivery area.
●Open the OB kit carefully
●Put on sterile gloves. ( from the OB kit)
●Use the sterile sheets and drapes from the OB kit to make a sterile delivery field
Delivery Prep… Patient Position
●The patient’s clothing should be removed or pushed up to her waist, and pants and undergarments should be removed.
●Preserve the patient’s privacy as much as possible.
●Place the patient on a firm surface that is padded with blankets, folded sheets, or towels.
●Elevate the hips about 2 to 4 inches with a pillow or blankets.
●Support the head, neck, and upper back with pillows and blankets.
●Have her keep her legs and hips flexed, with her feet flat on the surface beneath her and her knees spread apart
Delivering the head
●Continually check for crowning.
●Some patients experience precipitous labor and birth.
●Position yourself so that you can see the perineal area at all times
●Observe the head as it begins to exit the vagina so you can provide support as it emerges.
●Place your sterile gloved hand over the emerging bony parts of the head to control the delivery of the head.
●Continue to support the head as it rotates
Delivering the body
●The head is the largest part of the fetus.
●Once it is born, the body usually delivers easily.
●Support the head and upper body as the shoulders deliver.
●Do not pull the fetus from the birth canal.
●The newborn will be slippery and may be covered with a white, cheesy substance, called vernix caseosa
Normal Delivery steps
Crowning
2 support head - Body & head rotate naturally
3.Check for nuchal cord once head delivers
4.Upper shoulders - guide head downward
5.Body delivers Lower shoulders - deliver guide head upward
6 place on mother’s abdomen if appropriate w/cord intact
7.If not - keep at the same level as vagina until cord it cut
8.Prior to cutting cord – assess for distress
9.Gurgling / Respiratory distress = SUCTION (Mouth then Nose)
10.Cut between the clamps ( 3 inches)
Post Delivery care
●Wipe the mouth with a sterile gauze pad as needed.
●Clamp and cut the umbilical cord after approximately 60 seconds.
●Obtain the 1-minute Apgar score
●You can help to slow bleeding by gently massaging the woman’s abdomen with a firm, circular, “kneading” motion.
●Record the time of birth in your patient care report.
●The following are emergency situations:
●More than 30 minutes elapse and the placenta has not delivered
●There is more than 500 mL of bleeding before delivery of the placenta.
●There is significant bleeding after the delivery of the placenta
Bleeding in postpartum
●Bleeding that exceeds approximately 1,000 mL is considered excessive
●Continue to massage the uterus.
●Check your technique and hand placement if bleeding continues.
●Excessive bleeding is usually caused by the uterine muscles not fully contracting
Postpartum Embolism
●Most commonly a pulmonary embolism
●Results from a clot that travels through the bloodstream and becomes lodged in the pulmonary circulation
●Consider when a woman complains of sudden difficulty breathing or shortness of breath following delivery
Gestational Diabetes
●Diabetes develops during the second half of pregnancy in many women who have not had diabetes previously.
●Gestational diabetes, resolves in most women after delivery.
●The treatment is the same as for any other patient with diabetes
Hypertensive Emergencies
●Gestational hypertension is the presence of high blood pressure in the absence of other systemic effects.
●Defined as a systolic blood pressure higher than 140 mm Hg and a diastolic blood pressure higher than 90 mm Hg.
●Considered severe when the systolic blood pressure is higher than 160 mm Hg and/or the diastolic pressure is higher than 110 mm Hg
Preeclampsia
What is it…
●Preeclampsia is pregnancy-induced hypertension.
●Can develop after the 20th week of gestation
●Signs and symptoms include severe hypertension, severe or persistent headache, visual abnormalities, swelling in the hands and feet, and anxiety
Preeclampsia signs and symptoms
●Severe hypertension
●Severe or persistent headache
●Visual abnormalities such as seeing spots, blurred vision, or sensitivity to light
●Swelling in the hands and feet (edema)
●Upper abdominal or epigastric pain.
●Dyspnea and/or retrosternal chest pain
●Anxiety
●Altered mental status
Eclampsia
●Eclampsia is characterized by seizures that occur as a result of hypertension.
●To treat seizures:
●Lay the patient on her left side.
●Maintain her airway.
●Administer supplemental oxygen if necessary.
●If vomiting occurs, suction the airway.
●Provide rapid transport.
●Call for an ALS intercept, if available
Supine Hypotension Syndrome
What is it?
●Caused by compression of the descending aorta and the inferior vena cava by the pregnant uterus when the patient lies supine
Supine Hypotension Syndrome What do I do?
Transport the patient on her left side.

Bleeding in Pregnancy
Bleeding prior to 20 weeks gestation
●Hemorrhage from the vagina that occurs before labor begins may be very serious.
●May be a sign of spontaneous abortion, or miscarriage
Bleeding in Pregnancy
Bleeding after 20 weeks Gestation
●Placenta Previa
●Abruptio Placenta
●Uterine Rupture
●Uterine Inversion
Abuse
Pregnant women have an increased chance of being victims of domestic violence and abuse.
●Abuse increases the chance of:
●Spontaneous abortion
●Premature delivery
●Low birth weight
●The woman is at risk from bleeding, infection, and uterine rupture.
●Pay attention to the environment for any signs of abuse.
●Pregnant patients who are abused are often scared and may not be honest as to how their injuries may have occurred.
●Talk to the patient in a private area, away from the potential abuser if possible
Substance Abuse
●Effects of addiction on the fetus include:
●Prematurity
●Low birth weight
●Severe respiratory distress
●Death
●Fetal alcohol syndrome describes the condition of infants born to women who have abused alcohol.
●Newborn will probably need immediate resuscitation
Ectopic Pregnancy
●Embryo develops outside the uterus
●Usually in the fallopian tubes
●Sudden onset
●Severe abdominal pain
●Unilateral lower abdominal pain
●1st trimester vaginal bleeding
●Signs of shock if ruptured
At Risk:
●PID
●Tubal ligation
●Previous ectopic pregnancies
●Suspect in women who have missed a menstrual cycle
●Suspect if sudden onset of severe abdominal pain and vaginal bleeding in 1st trimester
SPONTANEOUS OR INDUCED ABORTION
●Bleeding
●Infection
●Treat for shock if indicated
●Bring any tissue that passes to the hospital
●Never pull anything out of the vagina
●Never pack anything in vagina
Spontaneous abortion
●Prior to 20 weeks
●Miscarriage
Induced abortion
Elective termination of pregnancy, not always elective, some complications for mother’s safety and life, may be required
Placenta Previa
Placenta develops over the Cervix
Cervix dilates
Patient may have heavy vaginal bleeding
Often without significant pain
Abruptio Placenta Signs
In abruptio placenta, the placenta separates prematurely from the wall of the uterus, most commonly caused by hypertension or trauma
•Severe pain
•Bleeding not always visible
•Signs of Shock
Treatment for Placenta previa and abruptio Placenta Treatment
●Same for both
●Requires immediate transport
●Signs of shock
●Place on left side
●High flow O2
●Sterile pad over vagina
●Do not pack
Uterine Rupture
●Rare
●Occurs during vaginal delivery
●Uterus tears
●Baby slips into the abdomen
Women at risk:
●Previous cesarean deliveries
●Uterine surgeries
●Risk increases with every c-section
Uterine Rupture Signs, Symptoms, and Causes
Signs and Symptoms
●Excessive vaginal bleeding
●Sudden pain between contractions
●Contractions slow down
●Contractions become less intense
●Baby’s head recedes back into birth canal
Causes
●Labors lasting more than 24 hrs
●Weakened uterus
●Placenta embedded to deeply into the uterine wall
●Placenta implants in the fundal portion (very top) of the uterus
●Pulling on the umbilical cord to speed delivery of the placenta
Uterine Inversion
●Uterus inverts (flips inside out)
●Rare
●Caused by pulling on the umbilical cord or baby
Signs
●Abdominal pain
●Excessive bleeding
●Signs of shock, like very low blood pressure
●In a complete inversion, the uterus will be visible in the vagina
Unruptured amniotic sac
●If the amniotic sac does not rupture by the time the head is crowning, it will appear as a fluid-filled sac emerging from the vagina.
●It will suffocate the fetus if not removed.
●You may puncture the sac with a clamp or tear it by twisting it between your fingers.
●Clear the newborn’s mouth and nose immediately
Nuchal Cord
●Umbilical cord around the neck
●As soon as the head is delivered, use one finger to feel whether the umbilical cord is wrapped around the neck (nuchal cord).
●Usually, you can slip the cord gently over the delivered head.
●If not, you must cut it, on cut, put your fingers under the cord and cut over your fingers so you do not cut baby
Breech Delivery
The presentation is the position in which an infant is born or buttocks first
●Most infants are born headfirst, called a vertex presentation.
●The fetus is at great risk for trauma from the delivery.
●Prolapsed cords are more common in a breech delivery
Breech Delivery Preparation
same as a normal delivery
•Allow the buttocks & legs to deliver spontaneously
•Support them to avoid rapid expulsion
•legs to dangle on either side of your arm
•Support the trunk & chest
•The head is almost always face down
•Allow to deliver spontaneously
•Keep the walls of the vagina off the newborn’s face
•Make a “V” with your gloved fingers
•position them in the vagina
•Keep walls of vagina off the fetus’s airway
Prolapsed Cord
What is it?
●Umbilical cord comes out first
●Fetus’s head compresses cord
●Cuts off circulation
●Deprives fetus of oxygenated blood
Prolapsed Cord What To Do
Method of relieving cord pressure
●Insert sterile gloved hand into the vagina
●Gently push the fetus’s head off the cord
●If supine (Raise foot of stretcher)
●If knee-chest position (Preferred)
●Relieve pressure from cord
●Keep fetus’s head off the cord
●Wrap cord in moist, sterile dressing (if it belongs in the body warm and wet, it needs moist sterile dressing)
●High flow O2
●Rapid transport
Limb Presentation
●Life threat- both to mom and baby
Cannot successfully deliver in the field
●Rapid transport & notification
●needs to be delivered surgically
●If limb’s protruding, cover with a sterile towel
Do not attempt to reposition the limb or push anything that comes out the vagina back
●Position on her back, head down & pelvis elevated
●Administer high flow O2
Precipitous Delivery
●Rapid delivery
●less that 3 hours start to finish
Explosive delivery
●Possible Complications:
●Maternal hemorrhage
●Fetal trauma
●Fetal hypoxia
Meconium
●First Bowel movement in utero
●Can be caused by fetal distress prior to delivery
●Green tint in amniotic fluid
●suction prior to ventilating
Risk Factors
●Maternal age
●Preeclampsia
●Prolonged labor
●Post term (42 weeks)
When treating pregnant trauma patient
●The uterus is especially vulnerable to penetrating trauma and blunt injuries.
●A trauma injury to the pregnant uterus can be life threatening to the woman and fetus because the uterus has a rich blood supply.
●In most cases, the only chance to save the fetus is to adequately resuscitate the woman
●Trauma is one of the leading causes of abruptio placenta
Follow these guidelines when treating a pregnant trauma patient:
●Maintain an open airway.
●Administer high-flow oxygen.
●Ensure adequate ventilation.
●Assess circulation.
●Transport the patient on her left side
●May experience a significant amount of blood loss before you will see signs of shock
●Fetus may be in trouble before signs of shock appear
Cultural Values…
●Cultural sensitivity is important when you are assessing and treating a pregnant patient.
●Women of some cultures may have a value system that will affect:
●The choice of how they care for themselves during pregnancy
●How they have planned the childbirth process
●Some cultures may not permit a male health care provider to assess or examine a female patient.
●Respect these differences and honor requests from the patient
Teenage Pregnancy
●The United States has one of the highest teenage pregnancy rates among developed countries.
●Pregnant teenagers may not know they are pregnant or may be in denial about it.
●As you begin to assess all female teenagers, remember that pregnancy is a possibility.
●Respect the teenager’s privacy and need for independence
Physical Examination
●If the patient is in labor, the physical examination should be focused on contractions and possible delivery.
●If at any point you suspect that delivery is imminent, you should check for crowning.
●If you do not suspect an imminent delivery and the patient reports other problems unrelated to delivery, you should not visually inspect the vaginal area
Post Delivery Care:
●Keeping them warm & dry, facilitating effective breathing.
●Further treatment is based on assessment of the newborns:
●Respiratory effort / heart rate / skin color
“ The Golden Minute”
1st minute after birth
●Many newborns require some form of stimulation that will encourage them to breathe air and begin circulating blood through the lungs, including:
●Position the airway in a neutral or sniffing position
●If necessary, then suction the mouth and then the nose
●Vigorously dry the head, body, and back
●Rub the newborn’s back and gently flick or slap the soles of his or her feet
●Tactile stimulation
Normally the newborn will begin breathing within 30 seconds after birth, and the heart rate will be 100 beats/min or higher.
●If not, positive pressure ventilation may be needed
●Leading cause of neonatal arrest is respiratory
●Observe the newborn for spontaneous respirations, skin color, and movement of the extremities.
●Evaluate the heart rate at the base of the umbilical cord or brachial artery or by listening to the newborn’s chest with a stethoscope.
●The heart rate is the most important measure in determining the need for further resuscitation
Spontaneous Breathing…
If spontaneous breathing or a heart rate above 100 bpm is not observed within 30 sec.
●Ventilate on room air (21% O2) with BVM
●40-60 breaths per minute
●Reassess every 30 seconds
●SpO2 doesn’t usually reach 85%-95% until about 10 minutes after birth
●Blow-by oxygen if central cyanosis or low SpO2 but breathing is adequate (5L/min
Opening the newborn airway
Place padding under the baby’s shoulders so the head falls back into the “sniffing position”
If newborn heart rate is 60-100bpm…
IF THE HEART RATE IS MORE THAN 100 BEATS / MINUTE
●Keep warm ~ Transport ~ Continuously reassess
IF THE HEART RATE IS 60 to 100 BEATS / MINUTE
●Ventilations ~ 40-60 breath / minute
●BVM & room air
●Reassess after 30 seconds
●If heart rate and respirations do not improve
●Ventilate with BVM and 100% oxygen
●Continue to reassess ~ Call for ALS ~ Keep newborn warm
Neonate Resuscitation
Heart rate less than 60 bpm
●Begin assisted ventilations with BVM & 100% oxygen
●Reassess newborn every 30 seconds
HR below 60 after 30 seconds of ventilation with O2
●Begin chest compressions
●Compression to Ventilation Ration
●3:1
●120 actions
●30 ventilations
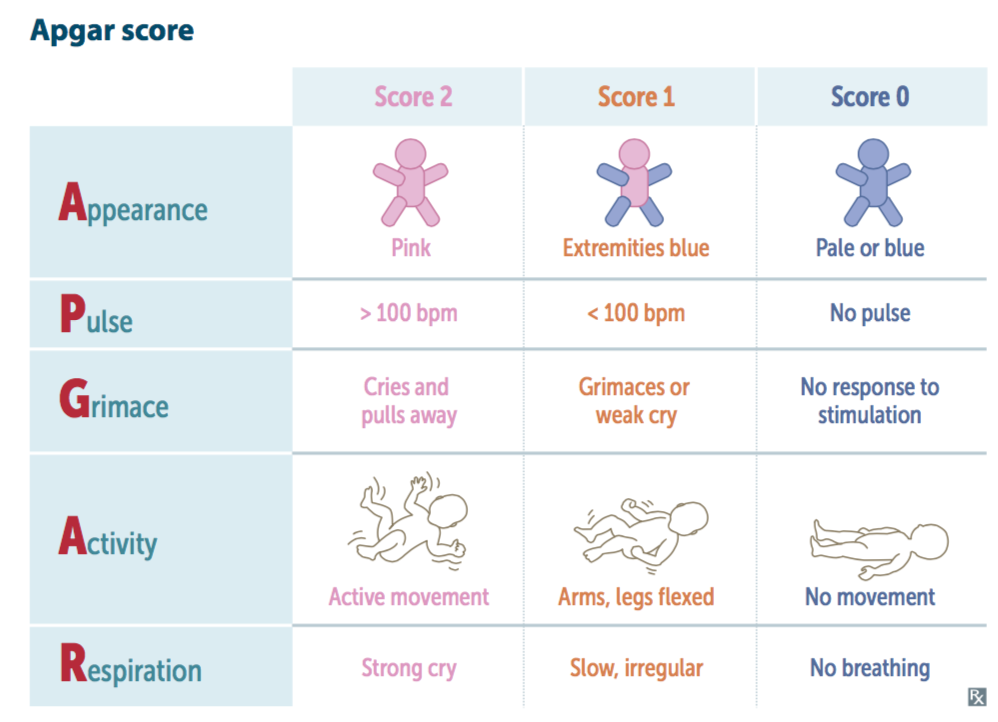
APGAR Score
The Apgar score is the standard scoring system used to assess the status of a newborn.
●It assigns a number value (0, 1, or 2) to five areas of activity.
●Appearance
●Pulse
●Grimace or irritability
●Activity or muscle tone
●Respirations
●Calculate the Apgar score at 1 minute and 5 minutes after birth.
●The highest possible Apgar score is 10
Fetal Demise
●The onset of labor may be premature, but labor will otherwise progress normally in most cases.
●If an intrauterine infection has caused the demise, you may note an extremely foul odor.
●The delivered fetus may have skin blisters, skin sloughing, and a dark discoloration.
●The head will be soft and perhaps grossly deformed.
●Do not attempt to resuscitate an obviously dead neonate.
Assessment 1
Scene Size up
●Take standard precautions.
●Gloves and eye and face protection are a minimum if delivery is already begun or is complete.
●If time allows, a gown should also be used.
●Consider calling for additional resources
●Determine the MOI or NOI.
●Do not develop tunnel vision during a call.
●Falls and necessity for spinal immobilization must be considered
Form a general Impression
●Should tell you whether the patient is in active labor or whether you have time to assess and address other possible life threats
●Perform a rapid examination.
●When trauma or other medical problems present, evaluate these first.
Assessment 2 airway breathing circulation
Airway and Breathing
●Life-threatening conditions with the woman’s airway and breathing are usually not an issue during a birth.
●A motor vehicle crash, assault, or a medical condition may cause a life threat.
●Assess the airway and breathing to ensure they are adequate
●Treat breathing problems like any other patient and provide oxygen
Circulation
●Blood loss after delivery is expected, but significant bleeding is not.
●Quickly assess for any potential life-threatening bleeding and begin treatment immediately.
●If signs of shock are present, control the bleeding if possible do not pack the vagina, give oxygen, and keep the patient warm
Assessment 3 transport decision
Transport Decision
●Transport decision
●If delivery is imminent, prepare to deliver at the scene.
●Ideal place to deliver is in the ambulance or the woman’s home.
●If delivery is not imminent, prepare the patient for transport
Rapid Transport for Pts who:
●Have significant bleeding and pain
●Are hypertensive
●Are having a seizure
●Have an altered mental status
Assessment 4 History
History
●Her expected due date
●Any complications that she is aware of
●If she has been receiving prenatal care
●A complete medical history
Obtain SAMPLE and:
●Determine the due date, frequency of contractions, a history of previous pregnancies and deliveries, the possibility of multiples, and if she has taken any drugs or medications.
Assessment 5 Vitals
Vitals
●Obtain a complete set of vital signs and pulse oximetry.
●Be especially alert for tachycardia and hypo- or hypertension.
●Hypertension, even mild, may indicate more serious problems
Reassessment
●Repeat the primary assessment with a focus on the patient’s ABCs and vaginal bleeding, particularly after delivery.
●Obtain another set of vital signs and compare with those obtained earlier.
●Recheck interventions and treatments to see whether they were effective.
Assessment 6 Communication
●If delivery is imminent, notify staff at the receiving hospital.
●Provide an update on the status of the woman and the newborn after delivery.
●If delivery does not occur within 30 minutes, provide rapid transport