Cardio pulm Heart Rhythms and ECG
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced |
|---|
No study sessions yet.
27 Terms
What is the ECG?
measurement of cardiac depolarization
Why and when would a picture of the electrical activity of the heart be useful?
MI indicator
How do doctors use the ECG to diagnose MI?
ST segment elevated or depressed or the T wave is inverted
Limb leads
I, II, III
Augmented leads
AVR, AVF, AVL
Gives you a 180 degree view within the FRONTAL plane of the heart
Precordial leads
V1- V6
Gives 180 degree view TRANSVERSLY through the heart
Negative deflection
Depolarization move away from + electrode and towards - electrode
Positive Deflection
Depolarization moves towards + electrode and away from - electrode
Infarction area with 12 lead EKG
I, aVL, V5, V6= lateral
II, III, AVF= Inferior
V1, V2= septal
V3, V4= anterior
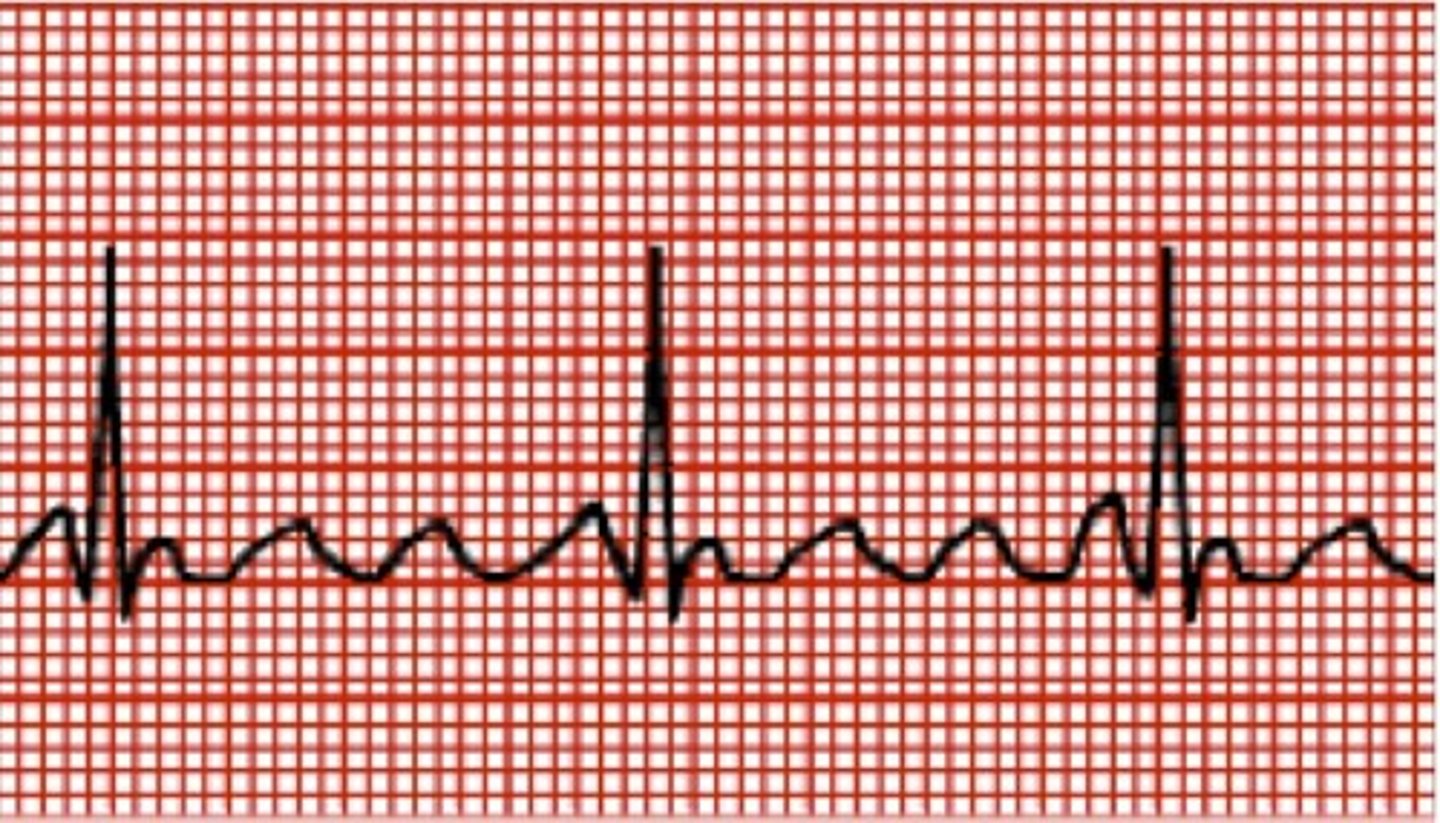
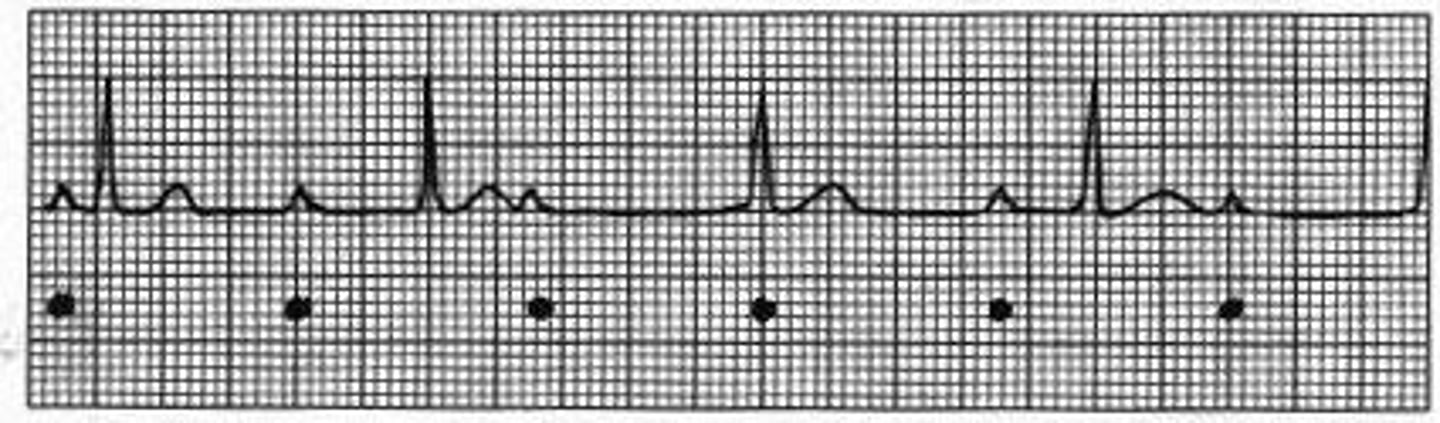
Normal EKG
PR interval duration: .12-.20 s
Q wave: duration- <.04 s amplitude- <25% of R wave
ST segment Amplitude: should be 0
Determining rate of EKG
300/ # of boxes from R to R
Atrial rhythms
if QRS complex looks normal in form- dysrhythmia is typically atrial in origin
Ventricular rhythms
if QRS complex looks abnormal and you lack a P wave- dysrhythmia is typically ventricular in origin
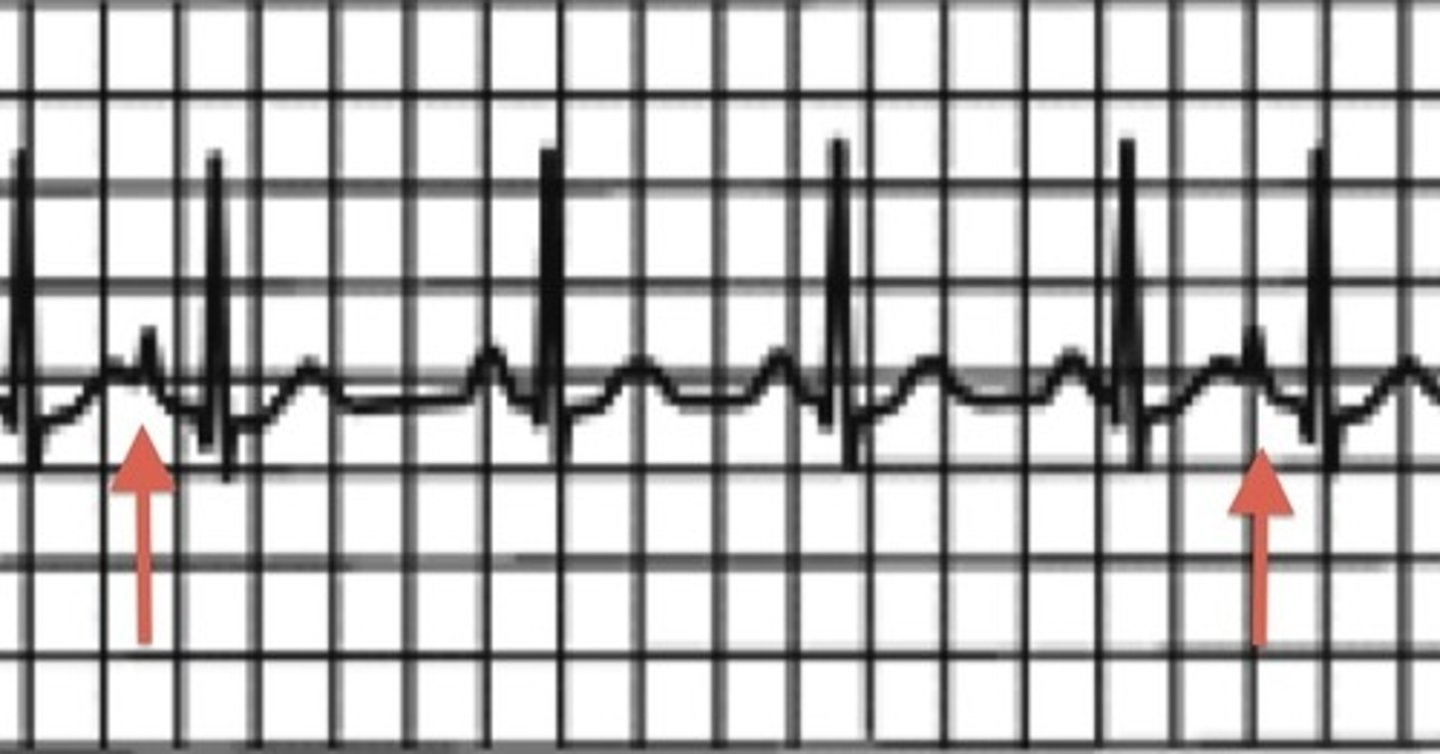
Premature Atrial contraction (PAC)
R to R wave not symmetrical
early beat that comes before P wave or looks odd
Atrial rate 60-100 bpm
Clinical implications: nothing HR usually normal
Little clinical significance
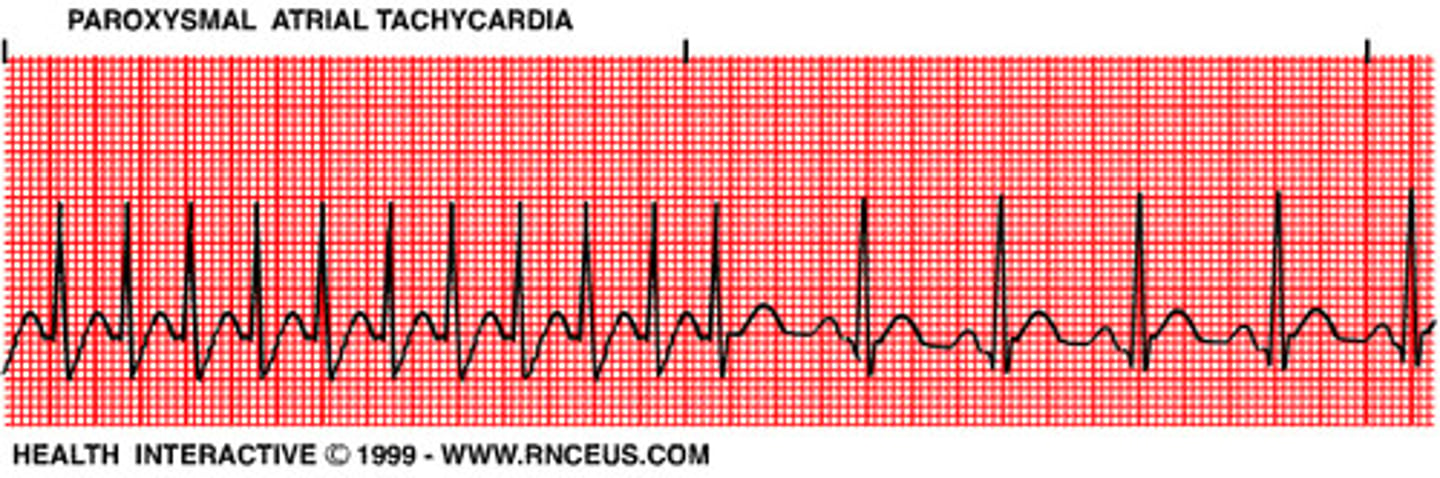
Supraventricular Tachycardia (SVT)
Single irritable atrial pacemaker in the atria begins to fire rapidly
Ventricles contract for each impulse from atria
Atrial rate 150-250 bpm
Clinical implications: ventricles moving so fast they can't fill
Atrial flutter
Saw tooth F waves with QRS complex
AV node becomes primary pacemaker
Atrial rate 250-350 bpm
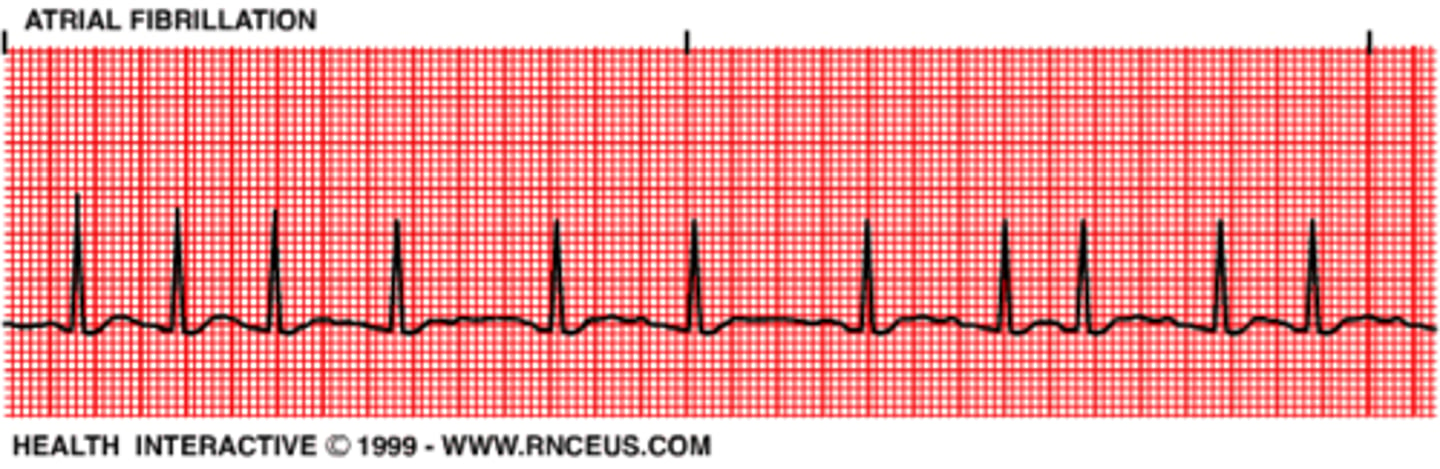
Atrial Fibrillation
No p wave
Uneven R-R interval
Need anticoagulants
Atrial rate 350-450 bpm
Produces fibrillations of the atria
AV node primary pacemaker
Clinical implication: people don't realize they have it
Find when taking pulse
Premature Ventricular Contractions (PVCs)
A depolarization that arises in either on the ventricles prior to the subsequent beat
Shortening R-R interval
Wide QRS
>6 PVCs per min considered pathological
Coupling and tripling PVCs very dangerous
Clinical implications: delay therapy till PVCs stop or calm down

Ventricular Tachycardia
150-250 bpm
Resemble PVCs
very irritable ventricular focus paces rapidly
Clinical implications: if develops stop treatment and lay pt down
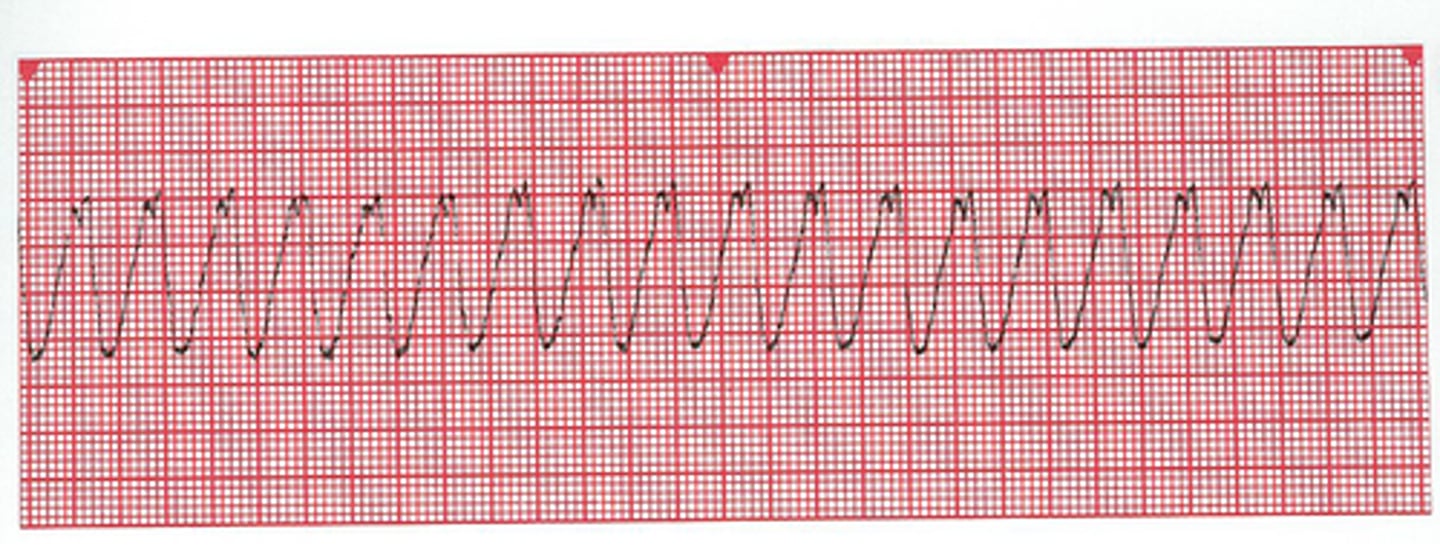
Ventricular flutter
250-300 bpm
Single ventricular automaticity focus
Ventricles don't have enough time to fill

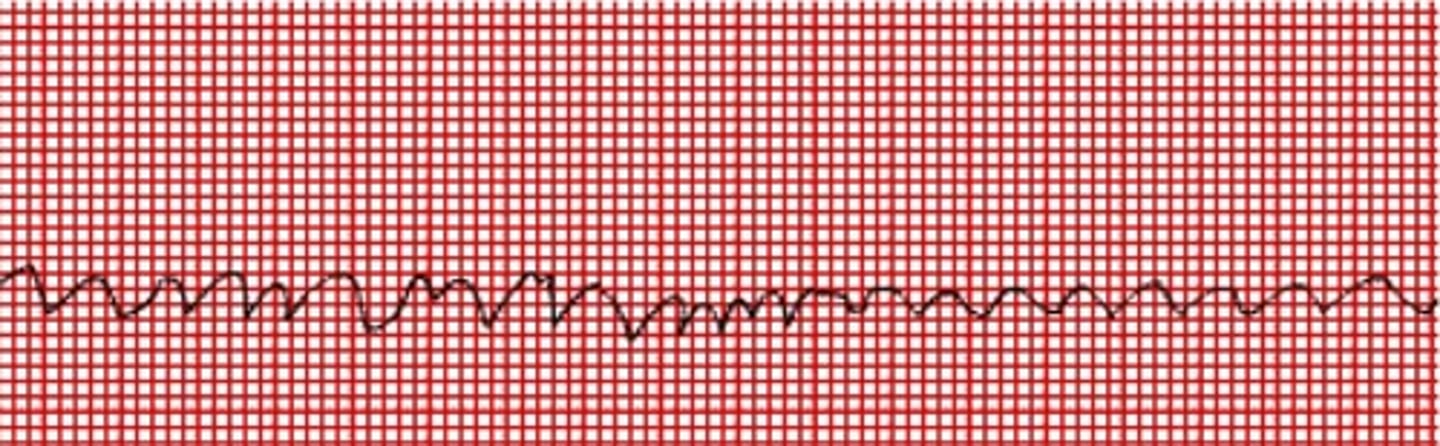
Ventricular Fibrillation
Hypoxia of coronary arteries
Lethal rhythm
Unorganized unidentifiable wave forms
pulseless
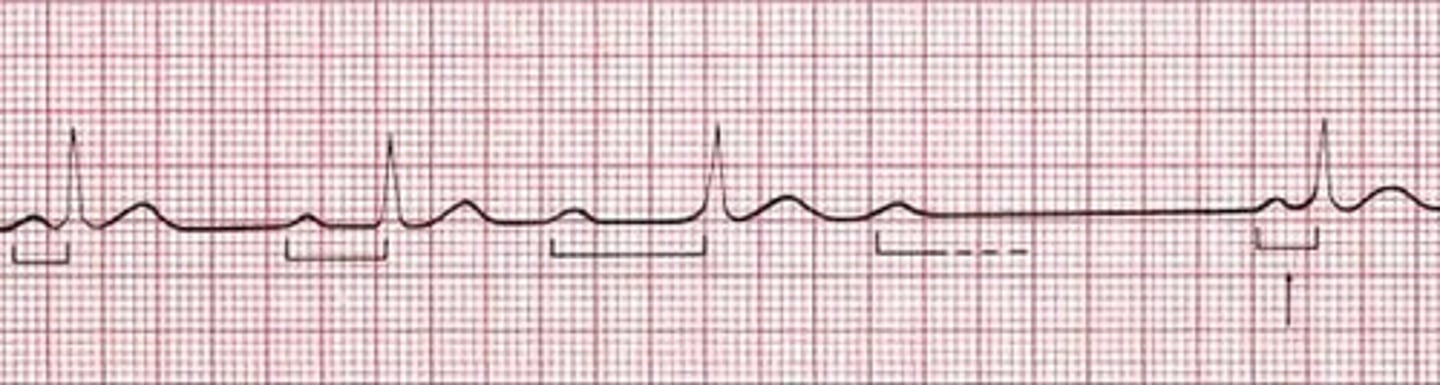
First degree heart block
Prolonged PR interval- normal is less than 1 box
everything else normal, except prolonged PR interval

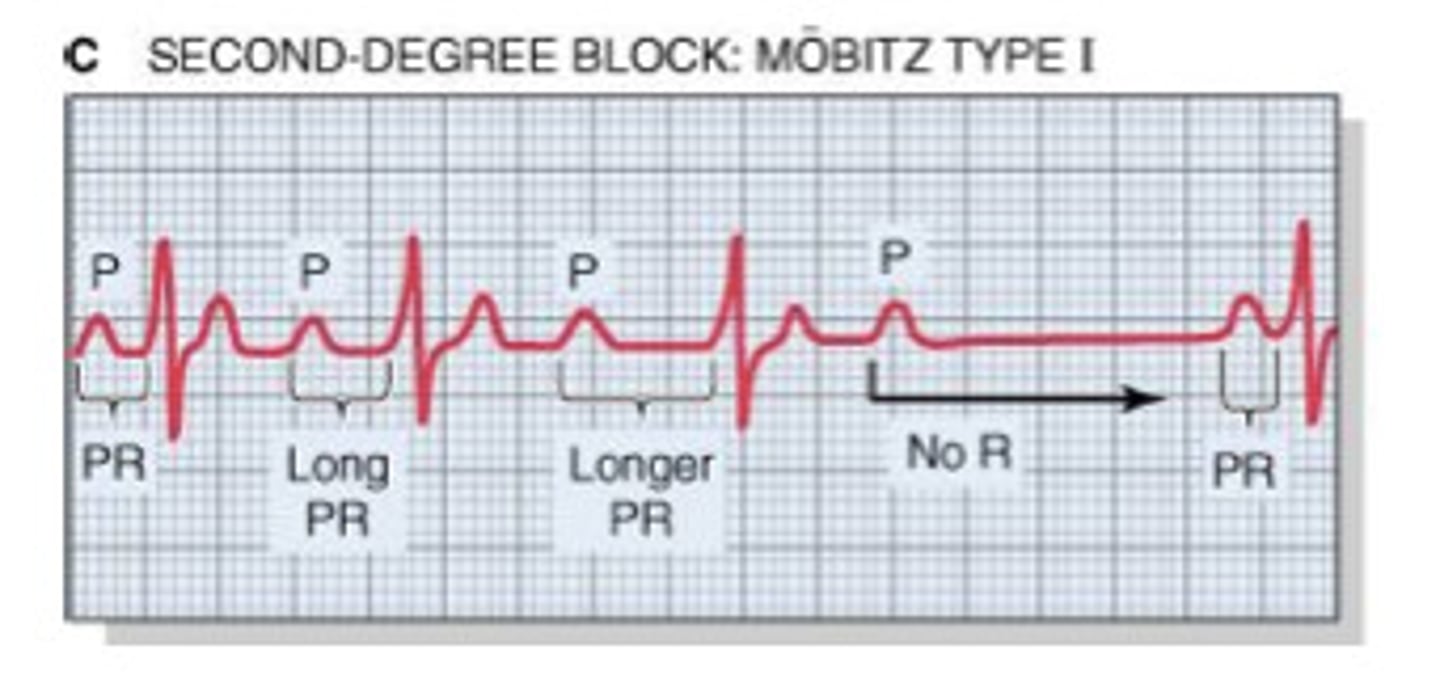
Second degree heart block type 1
1) Progressive increase of the PR interval
2) Progressive shortening of the R-R interval
3) Dropped QRS
Common with acute inferior wall MI
Second degree heart block type 2
No QRS complex
P waves followed by no QRS
no pattern
Third degree AV block
No communication between atria and ventricles
DANGEROUS
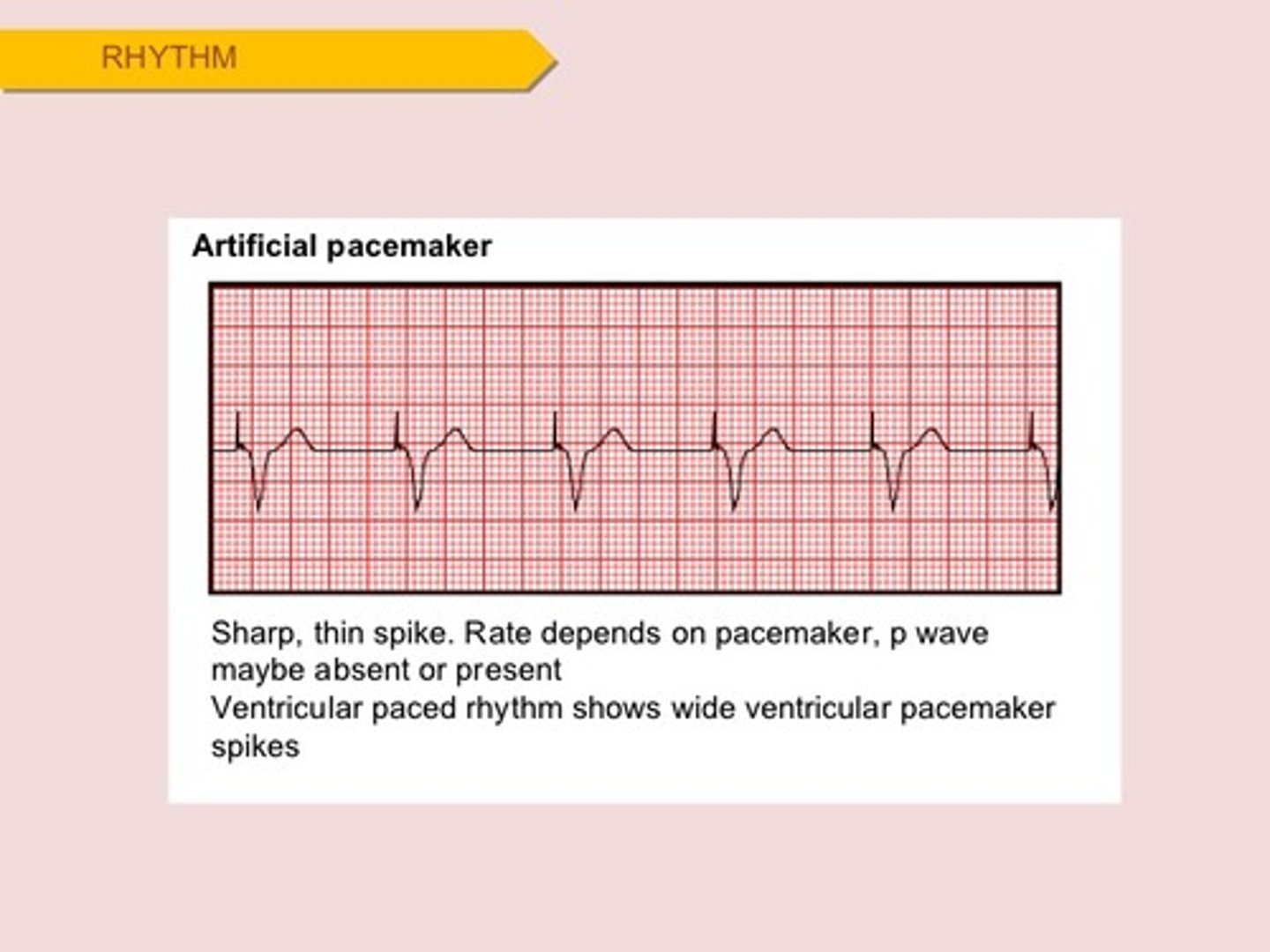
Pacemaker rhythms
sharp spike
Bundle branch block
depolarization of ventricles does not happen at the same time because of block in the bundle branches
Widened QRS
Double spike- the mountains in the grinch
